
Abstract
Study Design:
Retrospective cohort study
Objective:
The aim of this study is to determine if there is a correlation between the amount of facet distraction and postoperative patient-reported outcomes after ACDF.
Methods:
A retrospective cohort analysis of patients undergoing 1 to 3 level ACDF for degenerative pathologies at a single academic center was performed. Each patient received upright, lateral cervical spine x-rays at the immediate postoperative time point from which interfacet distance (facet distraction) was measured. Patient-reported outcome measures including NDI, PCS-12, MCS-12, VAS Neck, and VAS Arm pain scores were obtained preoperatively and at short-term (<3 months) and long-term (>1 year) follow-up. Receiver operating curves were generated to evaluate the possibility of a critical interfacet distraction distance. Univariate and multivariate analysis were performed to compare outcomes between groups based on the degree of facet distraction.
Results:
A total of 229 patients met the inclusion criteria. Receiver operating curves failed to yield a critical interfacet distraction distance associated with worse post-operative outcomes. Patients were instead grouped based on facet distraction distance below and above the third quartile (0.8mm-2.0 mm, 2.0mm-3.7 mm), with 173 and 56 patients in each respective group. Univariate analysis did not detect any statistically significant differences in outcome measures, recovery ratio, or % MCID achievement at short- and long-term follow-up between groups. Multivariate analysis also failed to demonstrate any significant differences between the facet distraction groups.
Conclusion:
Increased interfacet distance did not correlate with increased neck pain or disability after an ACDF.
Keywords
Introduction
Cervical radiculopathy and myelopathy are common cervical spine degenerative pathologies, with an annual incidence of 83.2 and 4.1 per 100,000, respectively.1,2 The sequelae of cervical degeneration represent an important cause of neck pain, disability, and diminished quality of life. Although the cause of neck pain is multifactorial, the facet joint and its capsular ligaments are known to be a source of pain with a high density of mechanoreceptors and nociceptive fibers.3-6 Fifty-five percent of chronic neck pain patients experience pain originating from the facet joint. 7 Anterior cervical discectomy and fusion (ACDF) has proven to be the gold standard surgical treatment for patients requiring decompression and stabilization for both radicular and myelopathic conditions.8,9 The procedure itself, however, has the potential to increase facet mediated pain through over-distraction and abnormal tensile loading of the facet joint.3-6,10
When performing an ACDF, intervertebral distraction is necessary to optimize visualization, facilitate graft insertion, and provide indirect nerve decompression.11-16 Currently there is limited evidence defining the optimal intervertebral graft height to accomplish such goals.17-19 Distraction of the intervertebral disc space leads to direct increases in foraminal space and maximizes cervical canal diameter.16,17,20,21 Likewise, under-distraction risks poor outcomes through insufficient decompression, graft dislodgement, and pseudoarthrosis.14,15,17 However, evidence suggests that there may be a limit to the amount of intervertebral distraction tolerated by patients.12,14 When this limit is surpassed, excessive distraction can lead to adverse outcomes. During initial vertebral distraction, the facet joints and posterior elements first experience compression. 14 However, as the distraction force increases, the load sharing disproportionately favors the anterior elements resulting in tensile stress across the facet joint.14,21 Consequently, over-distraction has been associated with risk of endplate subsidence, muscle spasm, and painful distraction of the facet joint capsule.14,15,17
Oversized graft insertion is known to cause strain of the facet joint and capsule. 5 However, controversy ensues in the literature on what represents a clinically relevant degree of cervical facet over-distraction.15,17-19 The purpose of the present study is to determine if a correlation exists between the degree of facet distraction and postoperative axial neck pain or disability following ACDF.
Materials and Methods
Upon obtaining Institutional Review Board (IRB#19D.508) approval, all patients over age 18 who underwent 1 to 3 level ACDF for cervical spondylosis with associated radiculopathy and/or myelopathy at a single academic institution between 2010-2015 were retrospectively identified. Waiver was granted for patient informed consent as a minimal risk research study. Additional inclusion criteria required complete patient demographic profiles, surgical characteristics, immediate postoperative imaging, and preoperative and postoperative patient-reported outcomes measures (PROMs) with minimum 1-year follow-up. Patients with a traumatic injury, infection, malignancy, or revision procedures were excluded. Patients were also excluded if their medical records or outcome measures were incomplete.
Patient demographic data including age, sex, smoking status (never, former, current), body mass index (BMI), and duration of follow-up was recorded via chart review. Surgical factors including the preoperative diagnosis (radiculopathy, myelopathy, myeloradiculopathy) and number of levels fused were noted. Immediate postoperative upright, lateral cervical spine x-rays were used to measure the interfacet distraction distance at the midpoint of the facet joint (Figure 1). For patients receiving multilevel fusion, the spinal level corresponding with the greatest facet distraction distance was referenced. The primary result was preoperative and postoperative health-related quality of life outcomes including the Neck Disability Index (NDI), Short Form-12 (SF-12) with embedded Physical and Mental Component Scores (PCS and MCS), VAS Neck pain, and VAS Arm pain scores. Outcomes scores were extracted at short- and long-term postoperative follow-up times defined as less than 3 months and greater than 1 year, respectively. Individual patient delta (▵) outcome scores were calculated by subtracting their preoperative score from postoperative score upon which a recovery ratio (RR) was calculated (▵score/ optimal score—preoperative score). 22 Achievement of Minimum Clinically Important Differences (MCID) was determined according to established values for the PROMs studied. 23

Image demonstrating the distance between facet joints measured at the midpoint.
Statistical Methods
Descriptive statistics were used to represent and compare patient demographics and outcomes in terms of mean and standard deviation. Continuous and categorical variables were analyzed with a non-parametric Mann Whitney U test and Chi-squared test, respectively. Area under the curve analysis was performed in attempt to identify a critical distance of interfacet distraction. Additionally, patients were grouped into 2 cohorts based upon interfacet distances. Given the apparent left skewed distribution of patient interfacet distance, groups were designated such that the bottom 75% of interfacet distances resembled normalcy and the top 25% represented the right tail. A multivariate linear regression model was developed with preoperative demographics and surgical factors as independent variables to isolate potential predictors of each ▵ PROM at short- and long-term follow-up. All statistical analysis was performed with R studio software (R Foundation for Statical Computing, Version 3.6.3, Vienna, Austria). A P-value < .05 was considered statistically significant.
Results
A total of 229 patients were included in the final patient cohort with 108 (47.2%) males and 121 (52.8%) females. The average patient age was 52.4 years and average BMI was 29.3. With regard to smoking status, there were 134 (58.5%) nonsmokers, 39 (17.0%) smokers, and 56 (24.5%) former smokers. The preoperative surgical indication was radiculopathy in 111 (48.5%) patients, myelopathy in 54 (23.6%) patients, and myeloradiculopathy in 64 (27.9%) patients. The number of levels fused included 54 (23.6%) single level, 112 (48.9%) 2 level, and 63 (27.5%) 3 level fusions. The average follow-up time was 19.0 (15.1; 22.2) months (Table 1). Short-term outcomes were available for 128 (55.9%) patients with an average follow-up of 51 days. Receiver operating curves (ROC) with interfacet distance as a predictor variable for short- and long-term PROM MCID failed to yield a critical interfacet distraction distance (Table 2). Accordingly, groups were designed with a cutoff interfacet distance corresponding to the upper quartile to maximize the odds of detecting an outcome difference. Group one contained 173 patients with an interfacet distraction below the third quartile (0.8-2.0 mm) whereas group 2 had 56 patients in the upper quartile (2.0-3.7 mm). There were no statistically significant differences for patient demographic or surgical factors between groups (Table 1).
Comparison of Patient Demographics by Degree of Facet Distraction.
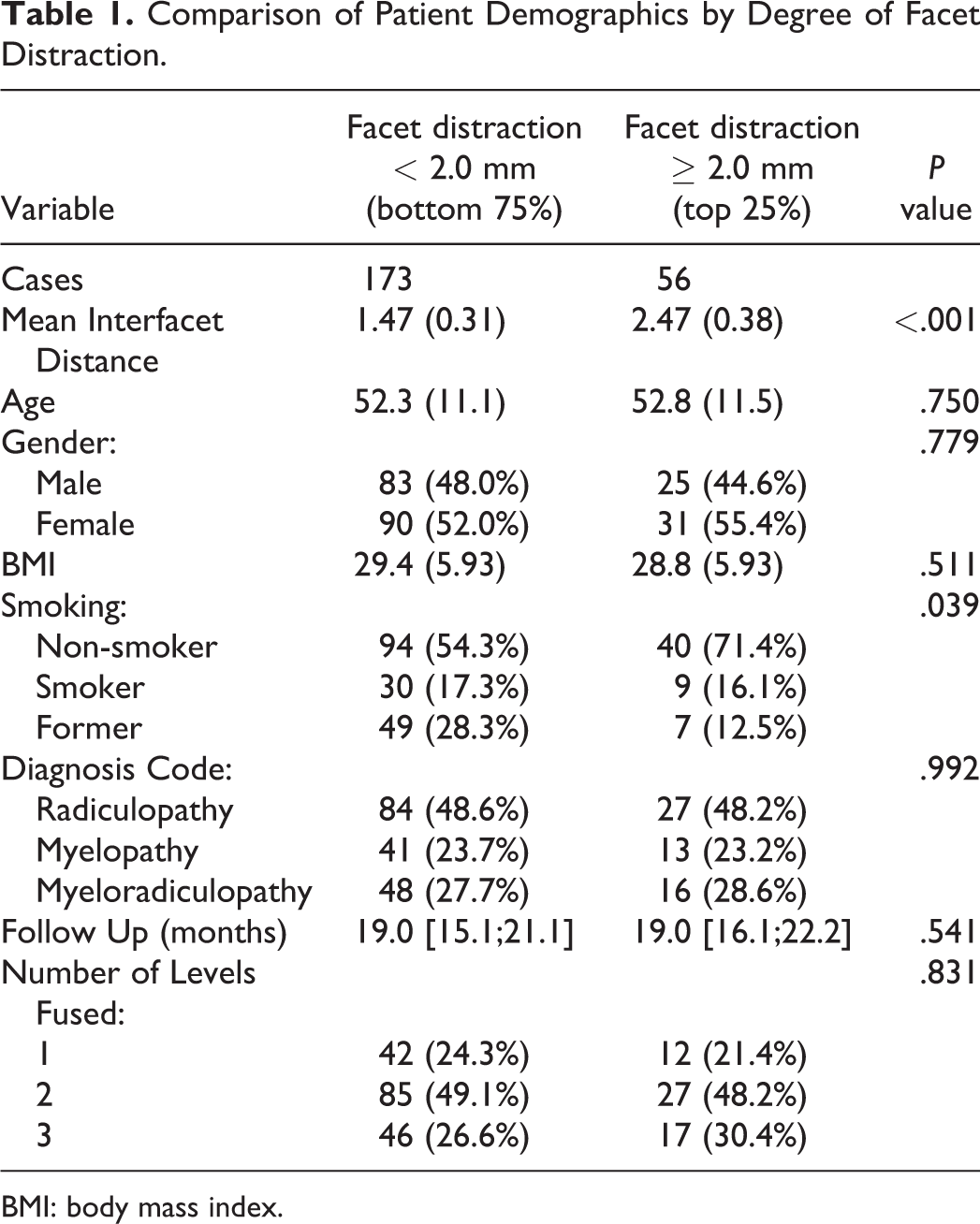
BMI: body mass index.
AUC Analysis Using Interfacet Distance as a Predictor Variable for Outcomes.
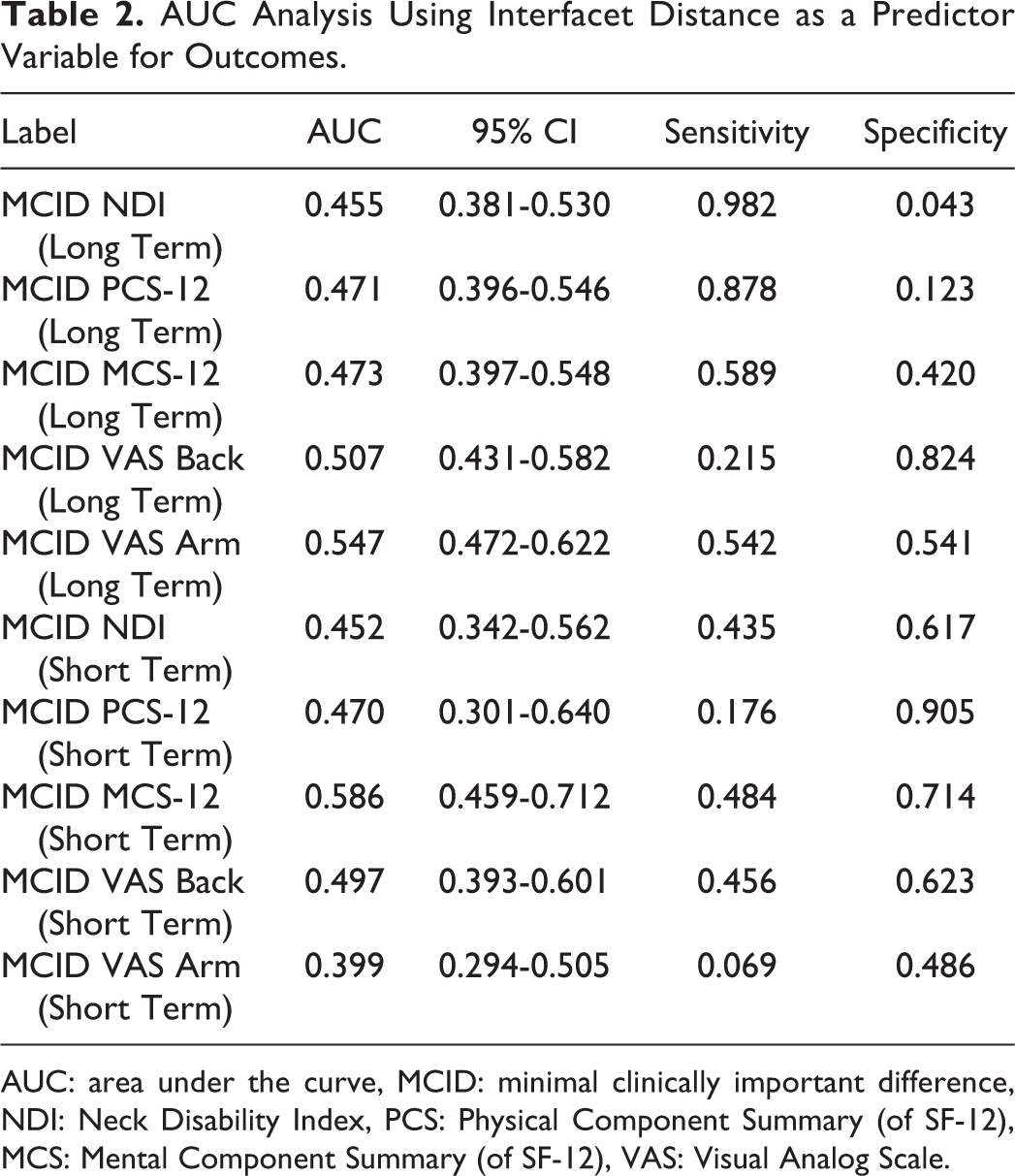
AUC: area under the curve, MCID: minimal clinically important difference, NDI: Neck Disability Index, PCS: Physical Component Summary (of SF-12), MCS: Mental Component Summary (of SF-12), VAS: Visual Analog Scale.
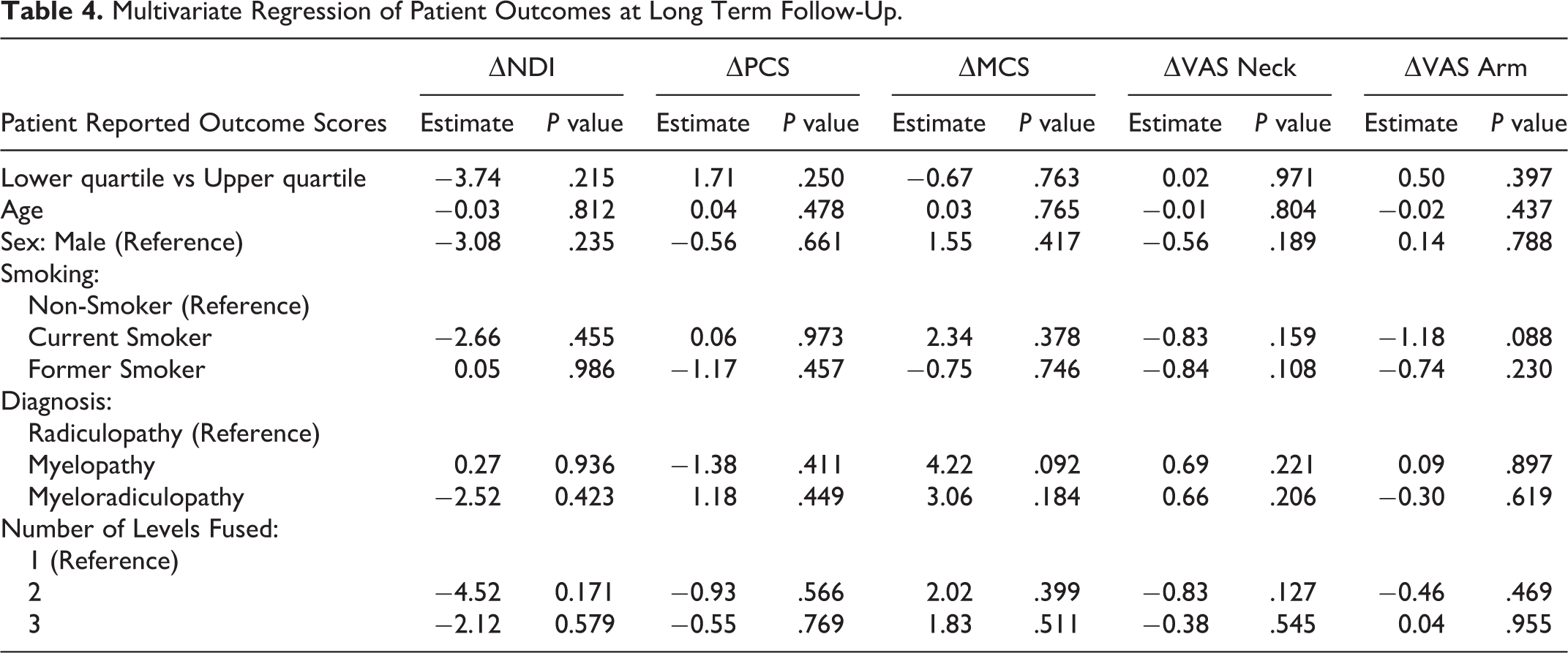
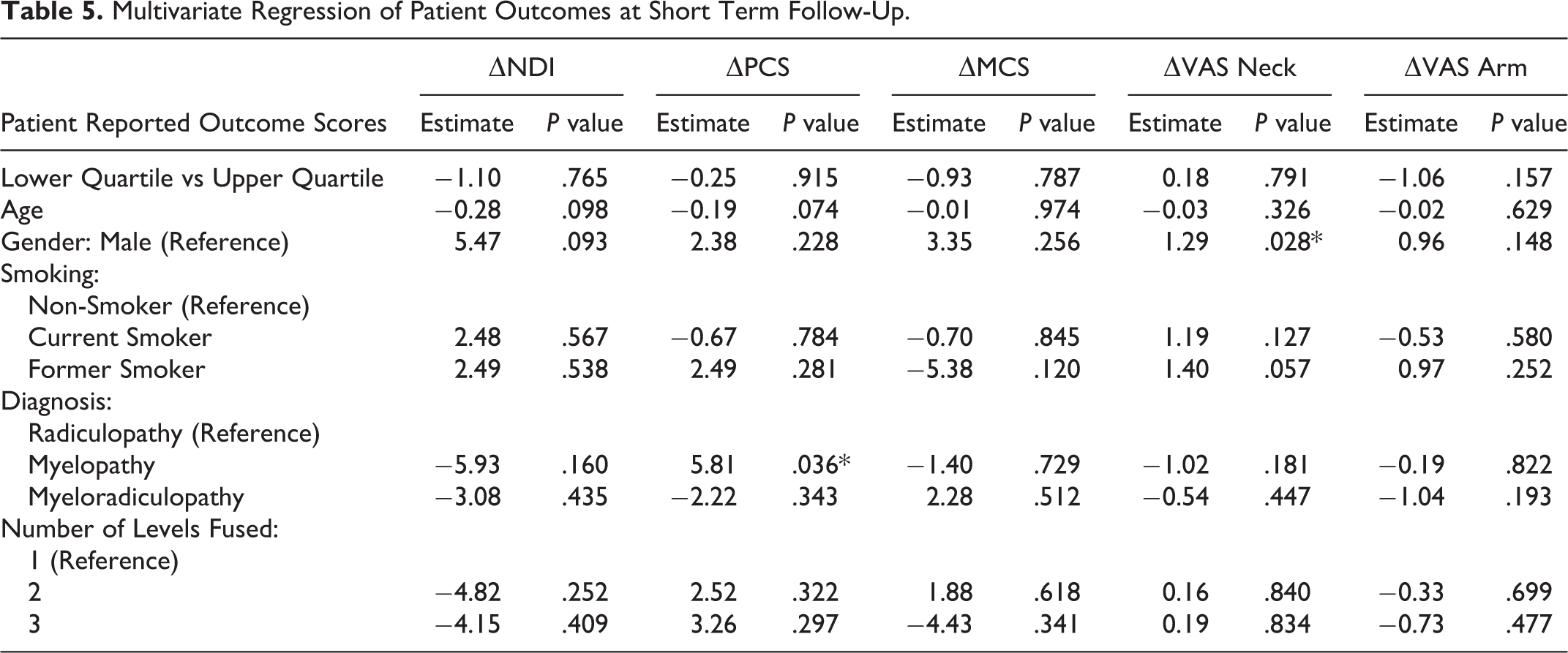
Univariate analysis failed to detect any statistically significant differences between the 2 groups in all PROMs as measured through ▵, RR, and % MCID achievement at both short- and long-term follow-up (Table 3). A trend toward statical significance favoring the lower interfacet distance group was only seen in short-term VAS Arm MCID achievement (P = .053). Multivariate analysis failed to demonstrate any significant differences between interfacet distraction and ▵PROM at short- and long-term follow-up (Tables 4 and 5). In the long-term regression models, preoperative demographics and surgical factors were not able to reliably predict ▵PROM score (Table 4). There was, however, a trend toward significant association between current smoking status and long-term increase in arm pain (P = .088). In the short-term regression models, the independent variables of myelopathy diagnosis and female sex served as positive predictors for ▵PCS (P = .036) and ▵VAS Arm (P = .028), respectively (Table 5). Nonetheless, the aforementioned variables were not statistically meaningful determinants for any other short-term ▵PROM score.
Comparison of Patient Short- and Long-Term Outcomes by Facet Distraction Group.
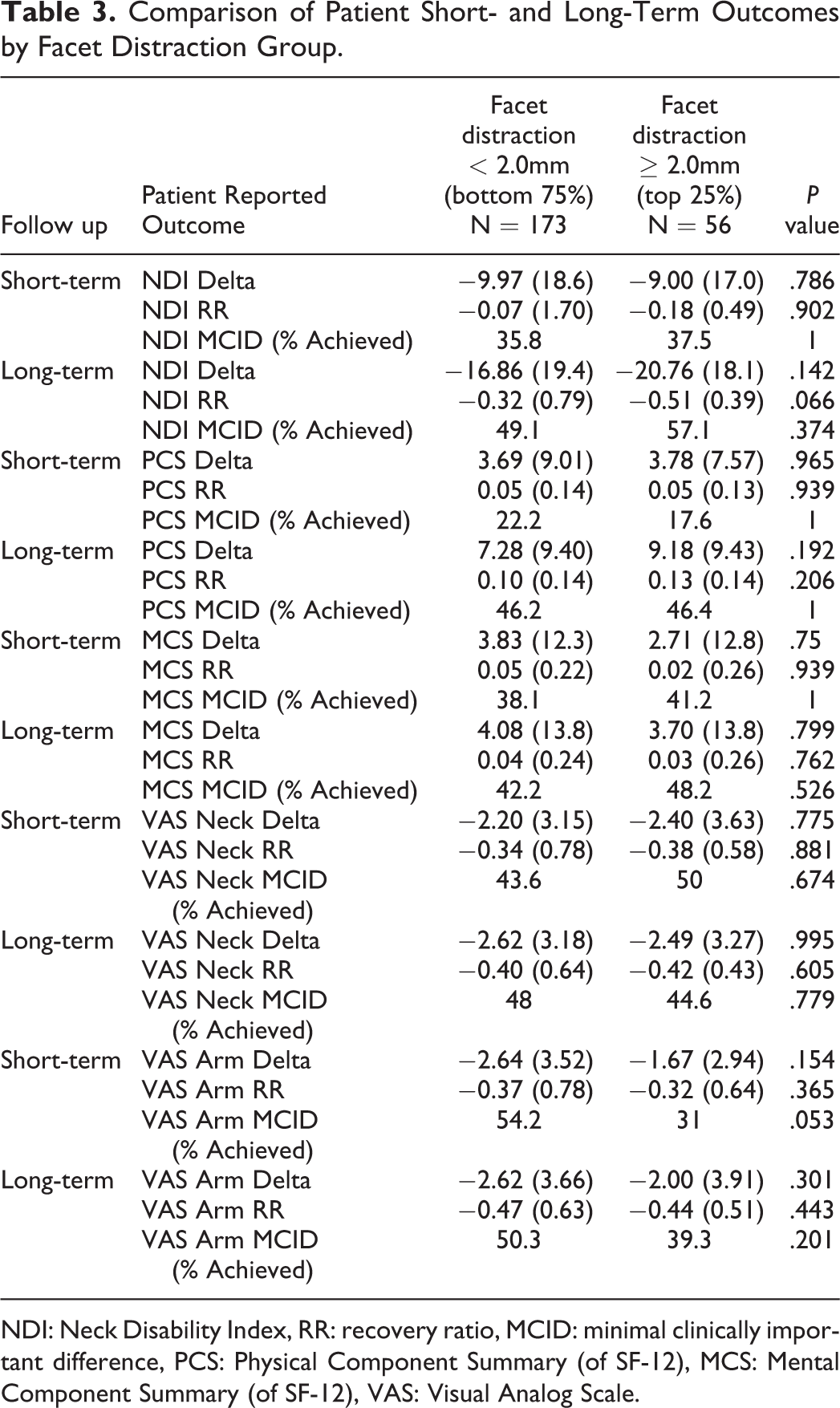
NDI: Neck Disability Index, RR: recovery ratio, MCID: minimal clinically important difference, PCS: Physical Component Summary (of SF-12), MCS: Mental Component Summary (of SF-12), VAS: Visual Analog Scale.
Multivariate Regression of Patient Outcomes at Long Term Follow-Up.
Multivariate Regression of Patient Outcomes at Short Term Follow-Up.
Discussion
ACDF is the gold standard surgical procedure for degenerative cervical pathologies. 8 The optimal graft height and corresponding degree of intervertebral distraction, however, remains unknown. Under-distraction and over-distraction are both associated with their respective risks and complications. Without a thorough direct decompression, under-distraction may lead to persistent nerve compression; conversely, while a taller graft affords better indirect decompression, it risks distracting the facet joint and capsule, a known cervical pain generator, and can lead to subsidence into the endplate with recurrent compression.3,5,6,15 The results of our study suggest in increased facet distraction does not significantly affect changes in patient clinical outcomes in the short- or long-term.
Posterior neck pain, though multifactorial in origin, frequently originates from the facet joint.5,24 Anesthetic injections to the cervical facet commonly relieve axial neck pain.3,4,24 The cervical facet synovium and capsule contain a high density of neuropeptides, nociceptive pain fibers, and inflammatory cytokines.6,25,26 Calcitonin gene-related peptide and Substance-P sensory neuropeptides are mediators thought to be involved in mechanical and nociceptive pain pathways by creating a neuroinflammatory state resulting in increased levels of IL-1ß and IL-6.25,27 Pain pathways in the facet joint may be triggered by joint impingement, synovial fold pinching, or capsular strain. 6 It is postulated that cervical facet joints have a tensile strain threshold that when surpassed generate pain only if the capsular ligament remains intact.3-5,15 In a rodent model, the critical degree of facet capsular strain occurs between 11-42%. 4 However, the capsular distraction threshold in human cervical facets joints has not yet been elucidated.
When evaluating the degree of facet distraction in relation to neck pain, there is conflicting evidence in the literature. Increased interfacet distance has been shown to correlate with improvement in VAS Arm pain scores in patients who underwent 1-2 level ACDF for degenerative conditions.16,17 However, in the present study increased interfacet distraction was not meaningful associated with VAS Arm or VAS Neck pain reduction. Increased facet distraction, to a certain degree, may be beneficial to enable greater indirect decompression resulting from a taller interbody graft. 15 However, all surgeons in our paper routinely performed a thorough direct decompression prior to graft placement and did not rely on graft height for indirect decompression. The heterogeneity in extent of direct and indirect decompression through surgical technique and graft selection, respectively, may explain this disparity in pain reduction. No available evidence reliably predicts how graft footprint and geometry affect facet distraction.15,16 Given the multitude of cage manufacturers, materials, and geometries used by the various surgeons included in our study, facet distraction was analyzed independent of graft choice in order to determine if direct association exists between facet distraction and clinical outcomes.
Previous studies investigating ACDF have sought to determine if there exists a critical facet strain that leads to adverse postoperative outcomes when surpassed. Specifically, in patients undergoing ACDF for traumatic injury, a significant change in NDI and VAS was noted at greater than 3.0 mm of facet distraction. 18 However, a separate investigation examining a small cohort of single-level ACDFs for radiculopathy determined a critical distraction distance relative to ▵VAS occurred at a lower threshold of 0.7 mm but did not show significant outcomes difference in groups above and below the critical distraction value on univariate analysis. 19
Our study aims to clarify the disparate outcomes presented in the aforementioned literature through examining a larger degenerative patient cohort with additional outcome metrics. Though our study’s interfacet distraction distances were consistent with the previously published ACDF facet distraction ranges, variation in interfacet distance was not meaningfully associated with arm or neck pain. ROC analysis failed to demonstrate a critical value of interfacet distance when referencing MCID achievement in PROMs. This underscores the lack of a discernable transition point between acceptable range of distraction and over-distraction as presented in previous studies.18,19 Additionally, univariate analysis demonstrated no significant differences in ▵outcomes, RR, and MCID achievement across interfacet groups designed to maximize the odds of detecting an outcome difference. Lastly, no association between interfacet distance and outcomes was found even after controlling for potential confounders in multivariate analysis. The trend associating long-term increase in arm pain with current smoking status is consistent with previous reporting of outcomes after ACDF. 28 Nonetheless, our results suggest that a patient’s ability to clinically improve after ACDF, in both the short- and long-term, does not depend on the extent of facet joint distraction.
There are many potential reasons why intraoperative facet distraction was not associated worse clinical outcomes. The first explanation is that the critical threshold of capsular strain was not surpassed.3,5 However, when taking into consideration previously reported thresholds of 0.7 mm and 3.0 mm, patients included in our study were found to have distraction of up to 3.7 mm.18,19 Another possibility is that the capsular ligament was torn as a result of over-distraction and was no longer intact to serve as a pain generator. 5 However, the approach and technique for ACDF remains relatively standardized despite variation in instrumentation. 29 It therefore appears unlikely that a majority of 229 patients undergoing ACDF in our study would sustain painless torn capsular ligaments as compared to prior ACDF studies.17-19 Nonetheless, intervertebral distraction during ACDF was not associated with harmful facet over-distraction.
This study is not without limitations. Our study design is subject to the limitations inherent to a retrospective study. Although patients were included in this study by a systematic method, potentially relevant cases were identified based on follow-up parameters, introducing a selection bias. However, previous literature suggests that patients lost to follow-up after spine surgery are often young, working patients who did not seek care after symptom resolution. 30 Although all patients underwent surgery at an academic tertiary care hospital, they were seen at offices across the region. Nevertheless, this cohort may be representative of more complex degenerative pathologies as noted by the number of multi-level ACDFs in the study. Furthermore, advanced imaging including postoperative computed tomography (CT) may have provided a more accurate assessment of interfacet distance. However, such imaging is outside of the normal institutional imaging protocol and would have subjected patients to radiation otherwise unnecessary for routine postoperative care. Moreover, the interbody graft selected was subject to physician practice preferences and may have had variable impact on facet distraction. For this reason, facet distraction was analyzed independent of graft characteristics. Finally, a greater percentage of short-term follow-up outcomes would be helpful in confirming that facet distraction does not contribute to pain in the immediate postoperative period.
Conclusion
Overall, this study did not find a correlation between the degree of facet distraction and postoperative neck pain or disability after ACDF. Intervertebral distraction necessary for taller graft insertion was not associated with facet distraction-mediated pain in the short- or long-term.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.