
Abstract
Study Design:
Systematic literature review.
Objectives:
The impact of thromboembolic disease on the morbidity and mortality of patients with acute spinal cord injury is well documented, with rates as high as 67%-100% among untreated patients. The efficacy of mechanical prophylaxis as a stand-alone measure has been questioned, so we sought to determine a safe perioperative window for chemical anticoagulation use after spine surgery. Many surgeons have concerns anticoagulants may cause post-operative hematoma.
Methods:
A systematic literature review was performed, ultimately yielding 13 articles. Based on the existing literature and input from our multidisciplinary institutional trauma committee, a Spine Trauma DVT Prophylaxis Protocol was developed.
Results:
Effort was placed to identify cases within our institution in which patients suffered vertebral column fractures and/or spinal cord injuries. Of these 466 vertebral column fractures and/or spinal cord injuries, 4 patients were identified and diagnosed with DVTs while admitted.
Conclusions:
Of these patients, there is a clear dilemma with regard to safety of chemoprophylaxis use versus risk of developing a DVT. Though none of the patients developed a PE, utilizing the protocol would have led to earlier IVC filter placement or initiation of a VTE surveillance protocol in 2 of the patients. Initiation of enoxaparin before surgery in one patient (despite delay of surgical timing) may have avoided his subsequent LUE DVT. Though not appropriate for all clinical scenarios, we are confident that our treatment algorithm will prove beneficial for patient care in avoiding DVTs and helping trauma surgeons with evidence-based clinical decision making.
Background
Thromboembolic disease after spine surgery significantly increases hospital length of stay, hospital costs, and mortality rates. Even though the majority of patients with acute spinal cord injuries are young, the impact of thromboembolic disease on the morbidity and mortality of these patients is well documented, with rates as high as 67%-100% among untreated patients. 1 Within this patient profile, pulmonary embolism is the 3 rd most common cause of death. 1 The risk of venous thromboembolism is greatest during the first 12 weeks after the injury, when flaccidity, paralysis, or immobilization of the extremities allow the “stasis” component of Virchow’s triad to predominate. Additionally, spinal cord injuries may also lead to autonomic dysregulation, ultimately increasing coagulability through changes in the hemostatic and fibrinolytic cascades.1,2
Anticoagulation therapy is known to reduce thrombotic events, yet the safety and timing of initiating deep vein thrombosis (DVT) chemical prophylaxis in spine trauma patients remains controversial. 2 Should one be found, a standardized approach to VTE prophylaxis in the post-traumatic and perioperative period would streamline systems-based processes and may decrease the risk of adverse outcomes. To assist providers at our institution with patient care we aim to provide such an instrument. The purpose of our study is to first perform a systematic literature review of current practices and accepted applications of DVT prophylaxis among spine trauma patients. Then, guided by the evidence, a multidisciplinary team intends to develop a DVT prophylaxis protocol for those patients presenting to our institution with spine trauma. Finally, we will retrospectively apply the protocol to spine trauma patients who have had VTE events at our institution to assess the impact that an intervention may have had on outcomes.
Methods
Systematic Review—Search Details
This project began within Baylor University Medical Center’s Trauma Operations Committee, a multi-disciplinary team consisting of general surgery traumatologists, orthopaedic surgery traumatologists, neurosurgeons, pharmacists, emergency department doctors, and critical care specialists. One of the authors (SJBN) was tasked with performing a systematic literature review. This was performed utilizing PubMed, CIHAHL Complete database, the Cochrane Central Register of Systematic Reviews, the Cochrane Central Register of Controlled Trials, and the Ovid MEDLINE databases.
Studies were considered relevant if they pertained to the diagnosis of spine trauma (with no limitation placed on anatomic region), the diagnosis of thromboembolic (TE) disease in spine trauma patients, or subsequent administration of prophylactic measures to address the risk of thromboembolic disease in this patient population. A work that did not specifically mention prophylactic protocols or guidelines was expressly scrutinized, and was deemed irrelevant unless it discussed surgeon preferences on the topic; introduced basic science research related to TE disease; presented standards of screening/diagnostic techniques of thromboembolic disease; or outcome data related to spine trauma patients and thromboembolic disease. In this systematic fashion, we sought works that advanced our understanding of the topic in a way that could readily translate into an evidence-based protocol for our institution.
Inclusion criteria for this systematic review were: Articles presenting patients with spine trauma Clinical intervention with mechanical or chemical DVT prophylaxis Presentation of outcomes, complications, and adverse events English language reports, and
Exclusion criteria for this systematic review were: Animal studies Articles published more than 10 years ago No mention of operative management of the spine or involvement of spine surgery consultant in patient care, and Absence of DVT prophylaxis protocol, or recommendation regarding thromboembolic chemical prophylaxis
Two authors independently used the same selection criteria to screen titles, abstracts, and full papers of the relevant articles. A study that did not meet the inclusion criteria was removed. The following data was extracted: authorship, year of publication, study design, relevant patient population characteristics, intervention, duration of trial period, outcomes/complications, and time frame of study. In an effort to generate a more favorable yield, we imposed no restriction on publication status or study design. We made no efforts to assess the scientific quality of each study. In the case of an eligible article, the full text of the original article was studied, and the appendices were evaluated and applied to this review as applicable.
Development of the Protocol
Once the existing literature was reviewed and consolidated, the protocol was created. The final product was the result of multiple revisions based on the efforts of the authors and the input of the multidisciplinary committee. This project was undertaken as a quality improvement initiative at Baylor University Medical Center (BUMC), and as such was not formally supervised by the Institutional Review Board. We did not intend to supersede sound clinical decision-making but rather aimed to design and implement a protocol that would lead to safe, consistent, and timely administration of thromboembolic prophylaxis for those eligible spine trauma patients.
One important detail that frequently arose during discussion was the appropriate dosing of enoxaparin. The associated FDA label for enoxaparin states that DVT prophylaxis dosing is either 40 milligrams once daily or 30 milligrams every 12 hours. However, some recent studies in the trauma surgery literature have suggested that Anti Factor Xa-dosing or weight-based dosing regimens may be more effective in achieving therapeutic levels of anti-factor Xa.3-8 We elected to adopt subcutaneous administration of 30 milligrams twice daily dosing for the purposes of our quality improvement project to avoid questions of “off-label” use.
Retrospective Application
To simulate the potential impact that our established protocol may have had on previous thromboembolic events, we identified past cases of vertebral column fractures and/or spinal cord injuries within the institutional trauma database, the “Baylor Trauma Registry,” based on ICD10 codes. There were 3987 total trauma arrivals at the BUMC ED in 2017, the year selected for review. We then screened for ICD-10 categories S12, S14, S22, S24, S32, and/or S34, which represent diagnoses of vertebral column fractures and/or spinal cord injuries. There were 929 patients classified into these categories. After removing trauma patients with isolated pelvic fractures, there were 466 patients identified that met inclusion criteria. Of those 466 patients with vertebral column fractures and/or spinal cord injuries, 4 patients were diagnosed with DVTs while admitted. The details of their hospital course were carefully reviewed, and retrospective application of the protocol was applied to theorize what impact, if any, our protocol may have had on DVT prophylactic techniques in each instance.
Results
Systematic Review—Search
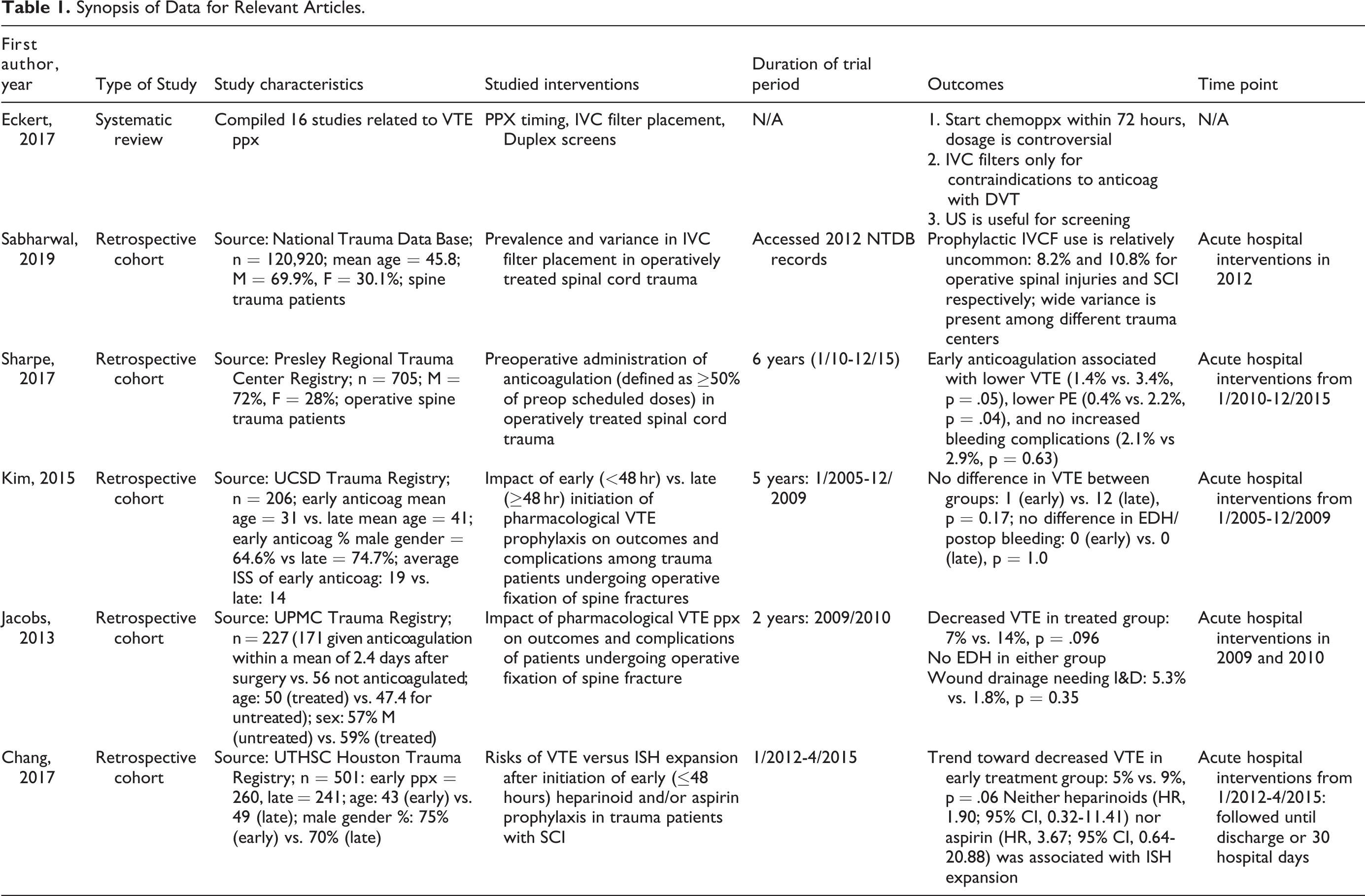
On June 16th, 2020, a PubMed database search with the initial algorithm: “spine surgery” + “trauma” was performed. This use of MeSH terms yielded 15,835 articles. By limiting the publication date to the past decade, 6,522 articles remained. The addition of MeSH term, “thromboembolism,” significantly limited the relevant yield to 18 articles and represented the point at which each text was fully reviewed. The addition of the MeSH term “prevention” provided 16 more articles, of which 10 were excluded for reasons outlined in Figure 1. This ultimately provided 6 articles that became the foundation of our literature review (Table 1). Addition of terms “prophylaxis” and “anticoagulants” provided 12 and 5 articles, respectively, but these were duplicates of those found previously. Careful review of the 6 articles and extraction of relevant articles from their bibliographies provided another 7 articles, for a total yield of 13.
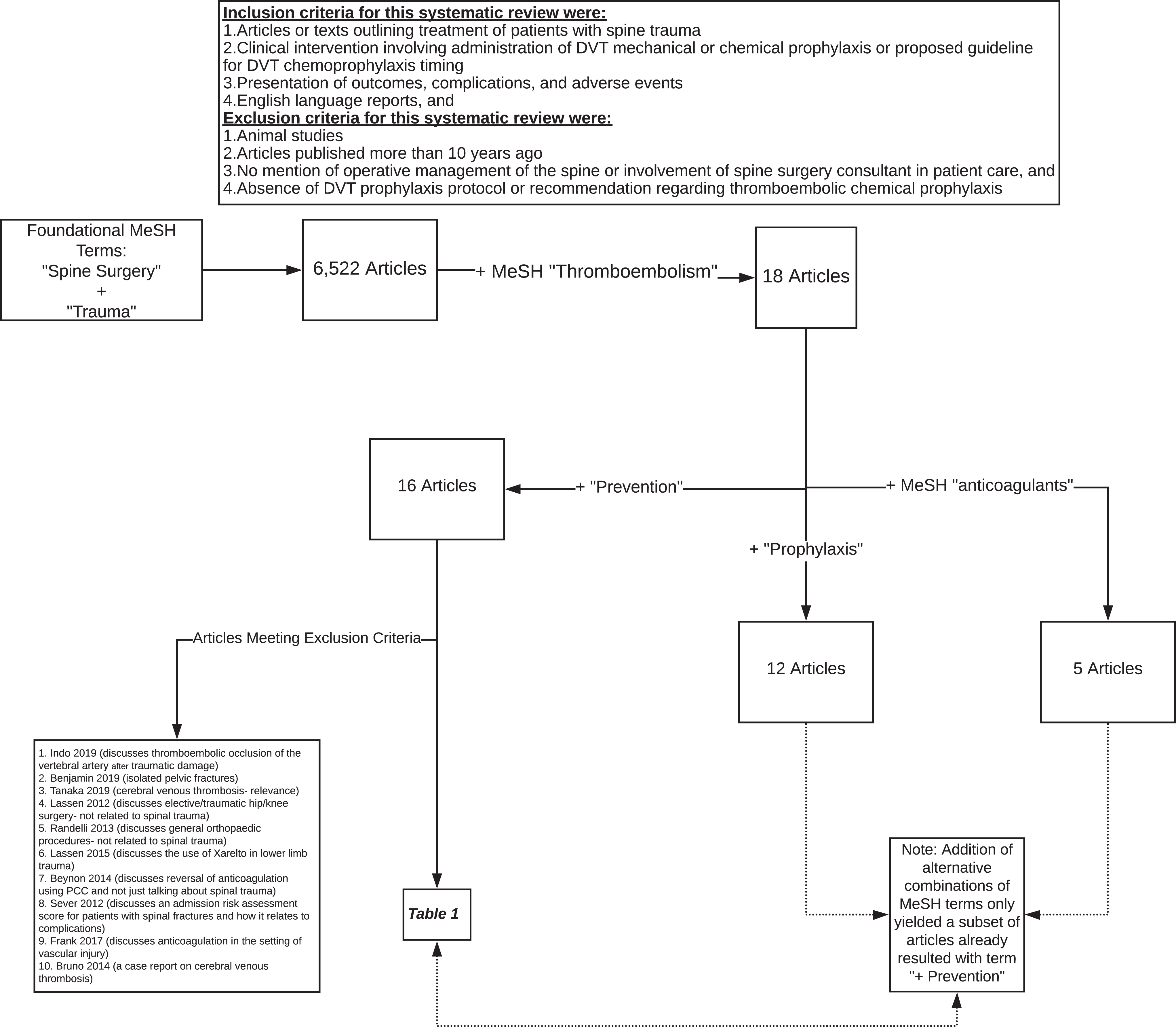
Literature review methodology flowchart.
Synopsis of Data for Relevant Articles.
Systematic Review—Summary of Evidence
As mentioned beforehand, the risk of VTE in an inadequately anti-coagulated spinal trauma patient approaches 100%. Therefore, it is essential to address options for chemical prophylaxis, including vitamin K antagonists, unfractionated heparin, low-molecular-weight heparin, and anti-platelet therapy.1,9 In their systematic review, Ploumis et al. determined that the prevalence of DVT thrombosis was significantly lower in patients without spinal cord injury (P < 0.00001), but there was no difference in the prevalence of pulmonary embolism between patients with and without an associated spinal cord injury (along with the spinal trauma) (p = 0.73). 1 Based on this finding, the authors conclude that the indications for prophylaxis may need to be stratified in the setting of spinal trauma based on the presence or absence of spinal cord injury. In their systematic review, Cheng et al. similarly determined that the only identifiable risk factor for thromboembolic disease in spine surgery patients was traumatic etiology of their condition. 10 In terms of specific implementation, Ploumis et al. recommended that prophylactic treatment should begin as soon after injury as possible, ideally within 72 hours. Even in cases where chemoprophylaxis may be contraindicated (intracranial bleeding, hemothorax, intra-abdominal bleeding, etc.), mechanical prophylaxis should be initiated immediately, with pharmacological prophylaxis started as soon as the patient is hemodynamically and neurologically stable. The authors did not find conclusive evidence on the optimum duration of treatment, though they report that a minimum of 2 weeks appeared to be “sufficient time” for most patients with spine trauma, though this can be extended as long as 3 months for patients with a complete motor spinal cord injury. 1 Both standard dose and adjusted-dose LMWH achieved similarly successful results.
Seeking to establish the safety of early chemical prophylaxis administration (<48 hours) in the setting of traumatic spinal cord injuries, Chang et al. performed a risk analysis of venous thromboembolic events and intraspinal hematoma (EDH, SDH, SAH, or intramedullary hemorrhage). While their institution had no set protocol, it did follow guidelines that allowed for the onset of VTE prophylaxis in patients with SCI or spine fractures immediately after the consultant surgeon has determined there is no need for emergent intervention. 11 In those instances where an intervention was warranted, chemoprophylaxis was held the night prior to surgery and for 24 hours post-operatively.
Within their cohort of 501 patients with SCI, while not statistically significant, there was a trend for decreased incidence of thromboembolic events in the early prophylaxis group (5% vs. 9%, p = 0.06). From this data, the authors concluded that early heparinoids (but not early aspirin) was associated with reduced VTE risk and reduced PE risk. 11 With respect to ISH expansion risk, only 7 patients were diagnosed with intraspinal hemorrhage for an overall incidence of 1.4%. Through statistical analysis, Chang et al. determined that neither heparinoids nor aspirin was significantly associated with ISH expansion, even in cases where patients had ISH upon admission. 11 In another study also comparing early (<48 hours) with late initiation (≥48 hours) of pharmacologic thromboembolic prophylaxis (with LMWH alone), but specifically in operatively treated traumatic spine fractures, Kim et al. found rates of VTE among the early group at 2.1% and 7.6% for the late group. 12 This reflects an overall VTE rate of 6.2%, which is consistent with published data. They similarly did not find any evidence that early initiation of VTE prophylaxis was associated with increased risk of bleeding, progression of neurological insult, or postoperative complications. Interestingly, one variable from their study that seemed to be related to delayed initiation of VTE prophylaxis was injury severity, reflected in statistically significant higher ISS, Glasgow Coma Scale, and AIS >3. 12 Other studies have also reached similar conclusions.13,14 In one performed by Nathens et al., VTE was twice as likely to be held beyond 4 days in patients with more severe injury profiles, despite the fact that this delay was associated with a 3-times greater risk of VTE than the early group.13,14
Seemingly unsatisfied with the lack of specific recommendations on which to base treatment decisions, several surgeons established a protocol for mechanical prophylaxis and early initiation of pharmacological thromboembolic prophylaxis for all patients undergoing spinal surgery at their institution. With this analysis of the treatment algorithm, Cox et al. compared the “safety and efficacy” of a multimodal thromboembolic prophylaxis protocol for 2 years after implementation with non-standardized management in the 2 years preceding implementation. 2 The protocol itself involved both chemical and mechanical prophylaxis and was developed with contributions from a multidisciplinary team of neurosurgeons, hematologists, critical care physicians, and pharmacists.
With the implementation of this protocol, the authors found a statistically significant reduction in DVTs (p = 0.009), but no difference between the pre-protocol or post-protocol groups with respect to rates of pulmonary embolism (p = 0.767) or epidural hemorrhage (p = 0.583). 2 Furthermore, patients treated in the prophylaxis protocol had significantly lower rates of DVT than those of patients treated without prophylaxis (p = 0.001), with compressive stockings alone (p = 0.016), or SCDs alone (p < 0.001) in the published literature. 2 Established rates of postoperative epidural hemorrhage are slightly higher with chemoprophylaxis (0.314%) than without chemoprophylaxis (0.180%), a difference that is statistically significant (p = 0.021). Yet, when the rate of epidural hemorrhage within the protocol group (0.4%) was compared to the published rates of epidural hemorrhage with and without chemoprophylaxis, neither was significant (p = 0.770 and p = 0.135, respectively). 2 Based on this data, Cox et al. conclude that the early initiation of an anticoagulation protocol can significantly decrease venous thromboembolic events, especially DVTs, and at least with the dosing regimen outlined within the study, can be considered safe for those concerned about symptomatic epidural hemorrhage. Other studies, while retrospective in nature, have affirmed that early chemoprophylaxis is both safe and efficacious in at risk patients after spinal surgery, with some even reporting no cases of epidural hematomas. 14
Unfortunately, the most effective screening method for venous thromboembolism remains elusive despite the Centers for Medicare and Medicaid Services considering DVT in trauma patients a “never event.” At institutions that routinely screen trauma patients, surveillance bias may lead to increased prevalence of occult DVT without an associated decrease of pulmonary embolism incidence. 15 While the rate of DVT in a hospital may reflect screening practice rather than quality of care, consensus guidelines from the Eastern Association for the Surgery of Trauma and the American College of Chest Physicians affirm that early detection of DVT with venous ultrasound in selectively-screened, high-risk patients can allow for timely therapeutic intervention.16,17 One study initiated by Allen et al. aimed to reduce the risk of pulmonary embolism among high-risk trauma patients through one such venous duplex ultrasound DVT surveillance protocol. The research team identified patients that were at high risk for VTE using a scoring system and recommended weekly bilateral venous duplex ultrasound examinations on these patients to the treating physician (Figure 2). At their institution, all examinations were performed by certified ultrasound technologists and involved the deep venous systems of both lower extremities from the ankle to the inguinal ligaments using B-mode compression, color augmentation, and spectral Doppler ultrasound. 18 Additional duplex ultrasound exams were ordered in the surveillance cohort or in the non-surveillance cohort if symptoms such as leg edema or pain raised clinical suspicion for VTE. High-risk trauma patients who underwent DVT surveillance in this manner were able to receive early therapy for the thrombotic disease and had a decreased rate of PE.
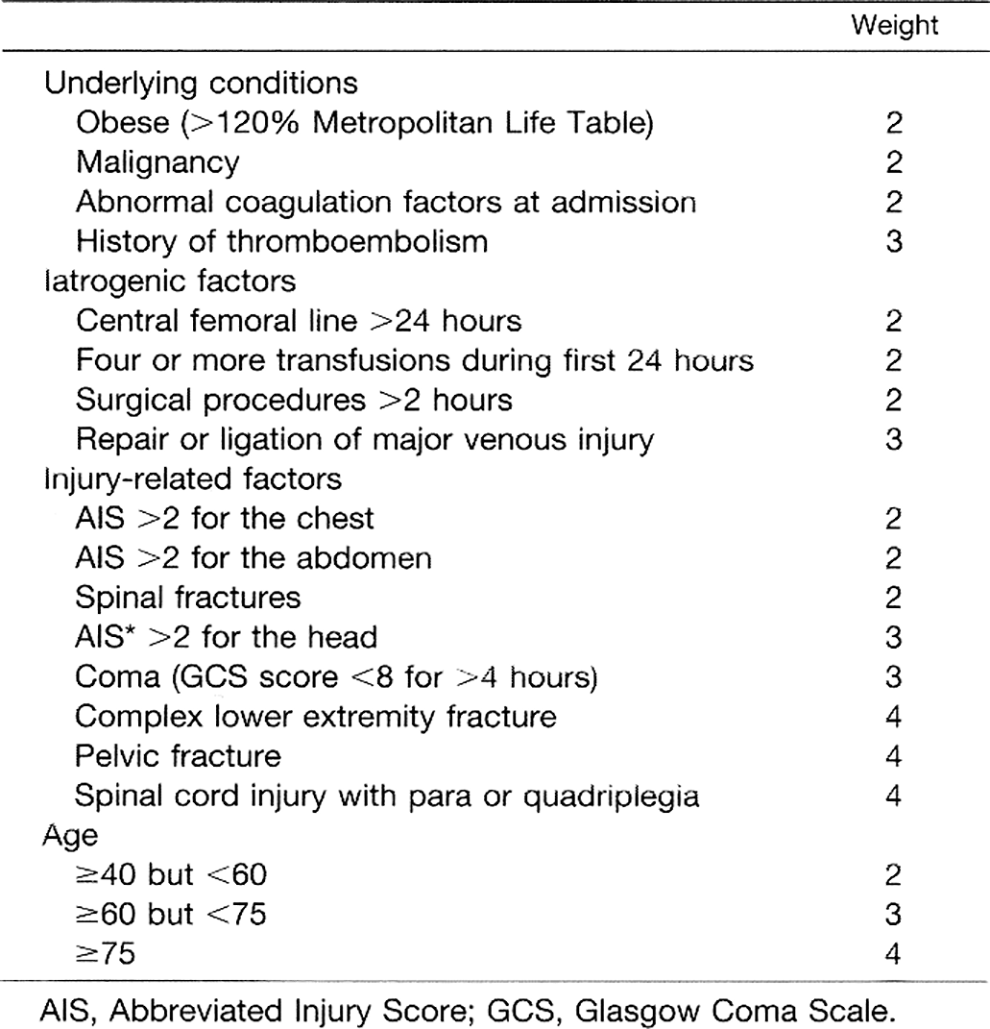
Greenfield’s risk assessment profile thromboembolism (RAPT) score.
The insertion of inferior vena cava filters is another intervention utilized by clinicians to manage patients at high risk for VTE. Many trauma patients, including a number of those with ongoing bleeding, recent brain injury, recent spinal cord injury, or medical comorbidities, have definite or relative contraindications to chemical thromboembolic prophylaxis due to the increased risk of hemorrhage. There is wide variability among trauma centers in the rates of IVC filter placement, largely due to the risk of thrombotic complications (i.e. caval thrombosis) and mechanical complications (i.e. strut fracture, filter migration, or filter embolization) and inability to reliably identify the “high-risk” patient in whom the benefits of IVC filter placement outweigh the risk. A recent meta-analysis by Haut et al. attempted to evaluate and better quantify the effectiveness of prophylactic IVC filter placement in trauma patients, particularly in preventing PE, fatal PE, and mortality. The authors concluded that there is low-strength evidence that prophylactic IVC filter placement leads to a lower incidence of PE and a lower incidence of fatal PE among hospitalized trauma patients when compared to those patients who did not have an IVC filter placed. 19 Filter placement had little impact on overall patient mortality. Therefore, even among those high-risk spinal trauma without a documented occurrence of a DVT or PE and in whom anticoagulation is contraindicated, IVC filter insertion should be considered. 17 Chemical thromboembolic prophylaxis should be commenced as soon as the contraindication resolves. 16
Development of Protocol
Based on the literature review and multidisciplinary discussions with the Trauma Ops committee, we present our Baylor University Medical Center Spine Trauma Thromboembolic Disease Prophylaxis protocol here (Figure 3).
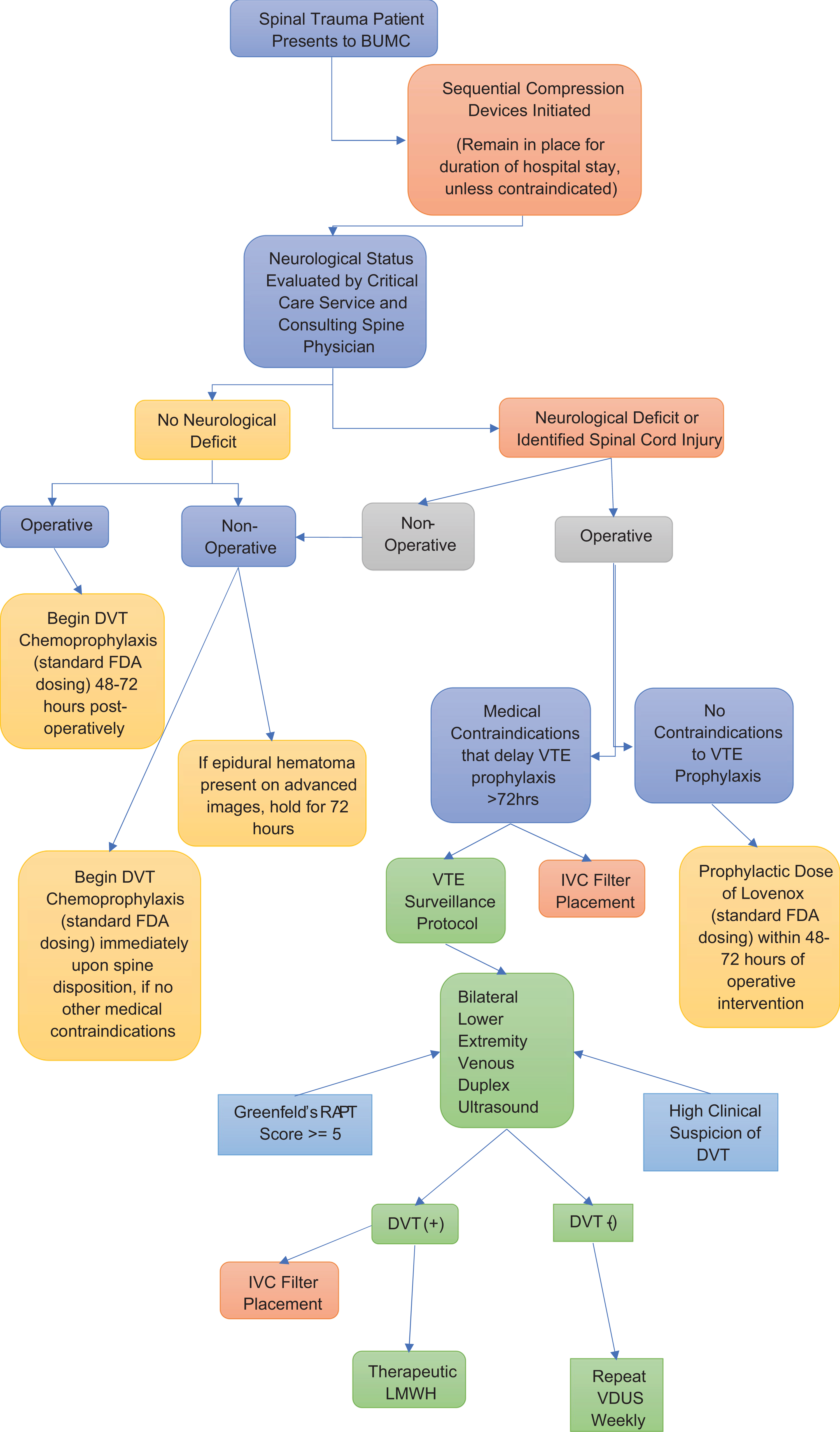
BUMC spine trauma thromboembolic disease prophylaxis protocol.
For our purposes, traumatic etiology of the injury is a significant factor when considering appropriate treatment and thus serves as the gateway into our protocol and subsequent evaluation by the trauma service and consultant spine surgeon. In accordance with the Ploumis and Cheng articles, the first stratification point of our protocol distinguished those patients presenting to our institution with spinal cord injuries/neurological deficits or without. As early in the evaluation process as possible, sequential compression devices are applied.
Similar to the works outlined previously, we used a threshold of 48-72 hours for administration of chemical prophylaxis post-operatively. This also served as the general window for holding the lovenox in situations of contraindication, such as brain or spine epidural hematoma before later reevaluation of the clinical picture. Although it can be a source of contention in practice, there are multiple studies that demonstrate that resumption of anticoagulation after this window can be done without increased risk of bleeding, progression of neurological insults, or symptomatic epidural hematoma, even in a patient previously excluded for medical reasons or diagnosed hemorrhage.10,11
In those scenarios in which medical contraindications precluded starting lovenox for more than 72 hours, our protocol relied on the work of Allen et al. and others in their description of ultrasound screening to develop our VTE surveillance protocol, as well as introduce the option for IVC filter placement. We believe that patients with a neurological deficit or identified spinal cord injury qualify as one group that merit such selective screening.
Finally, those patients who ultimately develop DVTs are to receive therapeutic levels of lovenox according to our protocol, though Shui et al. underscore the importance of avoiding such dosing levels due to increased rates of reoperation.
Retrospective Application
Patient #1:
29-year-old male was in a head-on motor vehicle accident, suffering significant trauma to the hands, face, brain, and spine. He was found to have an unstable C1 ring fracture and was placed in halo immobilization on HD #1. Notably, he was found to have small EDH, SDH and intraparenchymal hemorrhages that were stable on repeat CT. However, given the patient’s worsening neurologic status, he underwent a craniotomy for evacuation on HD #10. Patient remained neurologically tenuous and was deemed inappropriate for chemoprophylaxis. He was later diagnosed with RLE DVT on HD #20. An IVC filter was placed that same day. He never received chemical DVT prophylaxis and was ultimately discharged to a nursing home.
Patient #2:
39-year-old male who was a pedestrian hit by a vehicle traveling approximately 40 mph. Among multiple injuries, the patient suffered a T6-T7 Chance fracture, T6-T7 epidural hematoma, and a stable SAH. He was taken to the operating room on HD #3 for laminectomies and T4-T9 posterior spinal fusion and instrumentation. The spinal surgery team had deemed the patient inappropriate for DVT prophylaxis and the patient was found to have right popliteal DVT on HD #19. An IVC filter was placed the next day. He never received chemical DVT prophylaxis while an inpatient and was ultimately discharged to SNF.
Patient #3:
Patient is a 43-year-old male who was in a motor vehicle collision. Among other injuries, that patient suffered T1-T3 spinous process fractures as well as a stable SAH. Per Neurosurgery recommendations, the patient was to remain off chemical DVT prophylaxis for 1 month. On HD #9 he was found to have left cephalic vein thrombophlebitis. The patient had the affected vein removed and never received DVT prophylaxis while an inpatient.
Patient #4:
Patient is an 80-year-old male with severe spinal stenosis who developed central cord syndrome after a fall. On HD #3 he was found to have a LUE DVT. Lovenox was started on HD #4. Per neurosurgery consult, Lovenox was cleared for use, but would just need to be held on the day of surgery. He had C3-C6 laminectomies on HD #7. He did not resume chemical DVT prophylaxis after that. He was discharged to inpatient rehab.
Discussion
Within the framework of accepted quality standards and by means of this protocol, we aimed to consolidate existing science and experience to design and present a spine trauma VTE prophylaxis protocol that improves the delivery of care within our institution. We believe we have accomplished that goal.
Admittedly, the literature review was somewhat limited in the quantity of relevant articles based on our search terms, but our clinical question was similarly finite. Rather than make inferences, we sought to concentrate on literature that would allow us to create meaningful branchpoints on the algorithm. For example, though excluded from the onset of our study based on our foundational terms (“spine trauma”), manual searching of the databases yielded relatively more works describing safe and efficacious anticoagulation in elective spine cases and other orthopaedic procedures. The unique risks of thromboembolism to spine trauma patients (and the potential consequences of overly aggressive anticoagulation) demanded our strict exclusion criteria. Even so, the quality of articles provided a consistent base of knowledge upon which to design our project. Especially useful was the reverse indexing of the 6 primary articles, leading to the subsequent inclusion of the systematic reviews and institutional protocols highlighted previously.1,2,10
Based on the data acquired from the systematic review, a protocol was designed and presented to our institutional Trauma Operations Committee. This body benefits from its multidisciplinary composition. The focus on lovenox dosing standardization and inclusion of surveillance protocols serve as 2 examples of how a distinctive, specialist-specific foci may have been overlooked had spine surgeons alone been asked to compose this work. However, the patient-related interests of providers are so siloed at times that providing guidance on each possible clinical iteration renders the design-phase impractical. Simply put, we soon realized that the protocol could not replace sound medical decision-making across all specialties (particularly those beyond the customary scope of an orthopaedic surgeon’s practice) nor could it anticipate all possible iterations of a patient’s clinical course.
One limitation of this review was the inconsistent dosing and selection of chemical anticoagulation agent across the 4 patients presented through our retrospective application. This prevented us from meaningfully commenting on either variable. However, this lack of constancy does once again underscore one critical reason we undertook this work.
Though not ideal for all clinical scenarios, we are confident that the treatment algorithm above will prove beneficial for patient care, leading to more timely, safe, and consistent administration of DVT prophylaxis among spine trauma patients presenting to Baylor University Medical Center. In the future, we hope to perform a prospective, observational application of this standardized protocol and report on its safety and efficacy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.