
Abstract
Study Design
Retrospective database analysis.
Objective
Polytraumatized patients with spinal injuries require tailor-made treatment plans. Severity of both spinal and concomitant injuries determine timing of spinal surgery. Aim of this study was to evaluate the role of spinal injury localization, severity and concurrent injury patterns on timing of surgery and subsequent outcome.
Methods
The TraumaRegister DGU® was utilized and patients, aged ≥16 years, with an Injury Severity Score (ISS) ≥16 and diagnosed with relevant spinal injuries (abbreviated injury scale, AIS ≥ 3) were selected. Concurrent spinal and non-spinal injuries were analysed and the relation between injury severity, concurrent injury patterns and timing of spinal surgery was determined.
Results
12.596 patients with a mean age of 50.8 years were included. 7.2% of patients had relevant multisegmental spinal injuries. Furthermore, 50% of patients with spine injuries AIS ≥3 had a more severe non-spinal injury to another body part. ICU and hospital stay were superior in patients treated within 48 hrs for lumbar and thoracic spinal injuries. In cervical injuries early intervention (<48 hrs) was associated with increased mortality rates (9.7 vs 6.3%).
Conclusions
The current multicentre study demonstrates that polytrauma patients frequently sustain multiple spinal injuries, and those with an index spine injury may therefore benefit from standardized whole-spine imaging. Moreover, timing of surgical spinal surgery and outcome appear to depend on the severity of concomitant injuries and spinal injury localization. Future prospective studies are needed to identify trauma characteristics that are associated with improved outcome upon early or late spinal surgery.
Introduction
Multiple spine injuries occur frequently in severely injured patients.1,2 Therefore, it is strongly recommended by the ATLS-guidelines, to actively search for additional spinal injuries in the case of diagnosed spinal fractures. 3 In addition to the frequent occurrence of multiple spinal injuries in polytrauma, high energy trauma is also associated with severe non-spinal injuries.4-7 Specific patterns of concurrent injuries are to be expected for specific spinal segments. For example, patients with an injury to the cervical spine frequently also sustain traumatic brain injury (TBI) 8 among close anatomic linkage. 9 Due to biomechanical conditions of the rigid rib thorax, a fracture of the thoracic spine requires high traumatic energy, 10 which explains the frequent occurrence of concurrent non-vertebral thoracic injuries.5,6 In this context, accompanying injuries such as lung contusions, rib fractures and hemopneumothoraces have a negative impact on the respiratory system and likely also affect timing of spinal surgery.5,6,11 Moreover, lumbar spine injuries have been linked with intra-abdominal and pelvic injuries.12-15 In some cases, the spinal injury is the primary treatment-determining diagnosis, whereas in other cases, concurrent non-spinal injuries dictate treatment strategy. Due to inconclusive findings in literature, there is still much debate regarding appropriate timing of surgical treatment of spine injuries in polytrauma.2,16-22 Improved outcome has been described in spine patients operated within 72 hours after admission,2,7,17,18,23-25 another study however did not encounter relevant difference between prompt (<24 hours) and later surgery. 22 Patients’ factors,26,27 as well as injury characteristics and systemic homeostasis should all be considered in clearing patients for spinal surgery. 28
The aim of the current multicenter study was to analyse concurrent injuries in polytrauma patients with spinal injuries. Furthermore, the interplay between spinal injury localization, concurrent injuries and timing of surgery was investigated.
Materials and Methods
TraumaRegister DGU®
The TraumaRegister DGU® (TR-DGU) of the German Trauma Society (Deutsche Gesellschaft für Unfallchirurgie, DGU) was founded in 1993. The purpose of this multi-center database is the pseudonymised and standardised documentation of severely injured patients.
Data are prospectively collected in four consecutive time phases from the site of the accident until discharge from hospital: (A) pre-hospital phase; (B) emergency room and initial surgery; (C) intensive care unit (ICU), and (D) discharge. The documentation includes detailed information on demographics, injury pattern, comorbidities, pre- and in-hospital management, course of ICU, relevant laboratory findings including data about transfusion, and outcome of each individual. The inclusion criterion is being admitted to hospital via emergency room with a subsequent ICU care or reaching the hospital with vital signs and dying before admission to ICU.
The infrastructure for documentation, data management, and data analysis is provided by AUC - Academy for Trauma Surgery (AUC - Akademie der Unfallchirurgie GmbH), a company affiliated with the German Trauma Society. Scientific leadership is provided by the Committee on Emergency Medicine, Intensive Care and Trauma Management (Sektion NIS) of the German Trauma Society. Participating hospitals pseudonymize their data and submit them into a central database via a web-based application. Scientific data analysis is approved according to a peer review procedure laid down in the publication guideline of TR-DGU.
The participating hospitals are primarily located in Germany (90%), but a rising number of hospitals of other countries contribute their data as well (currently, these include Austria, Belgium, Finland, Luxembourg, Slovenia, Switzerland, The Netherlands and The United Arab Emirates). At present, over 35 000 cases from nearly 700 hospitals are entered into the database annually.
Participation in TR-DGU is voluntary. However, for hospitals associated with TraumaNetzwerk DGU®, the entry of at least a basic data set is obligatory for quality assurance reasons. This study has followed the publication guidelines of the TR-DGU and is registered as TR-DGU project ID 2019-016.
This study has been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. Ethical approval was not needed due to retrospective use of routine medical records.
Definitions
Severely injured patients were defined as Injury Severity Score (ISS) ≥16. The ISS is an anatomical scoring system that provides an overall score for multiple injured patients. Each injury is assigned to an abbreviated injury scale (AIS) score and is allocated to one of six body regions. The AIS Code is on a scale of one to six, one being a minor injury and six being maximal (AIS 1 = minor, AIS 2 = moderate, AIS 3 = serious, AIS 4 = severe, AIS 5 = critical, AIS 6 = fatal/currently untreatable). 29 The highest AIS score in each body region is used. The three most severely injured body regions have their score squared and added together to produce the ISS score. 30 The ISS score takes values from 0 to 75. If an injury is assigned an AIS of 6, the ISS score is automatically assigned to 75. Major trauma is considered to be present if the ISS is >15. Bolorunduro et al categorised and validated the ISS as follows 31 : <9 mild, 9-15 moderate, 16-24 severe, ≥25 profound. Relevant spine injury was defined as an injury with an AIS ≥3. A fall from great heights was defined as more than 3 meters. Early stabilization of the spine was defined as surgery within the first 48 hours after admission, while late stabilization was defined as surgical treatment afterwards. Outcome parameters were defined as LOS, ICU LOS, and in-hospital mortality. Complications were defined as sepsis, respiratory failure, and multiple organ failure (MOF).
Inclusion and Exclusion Criteria
Patient and Trauma Characteristics per Spinal Segment.
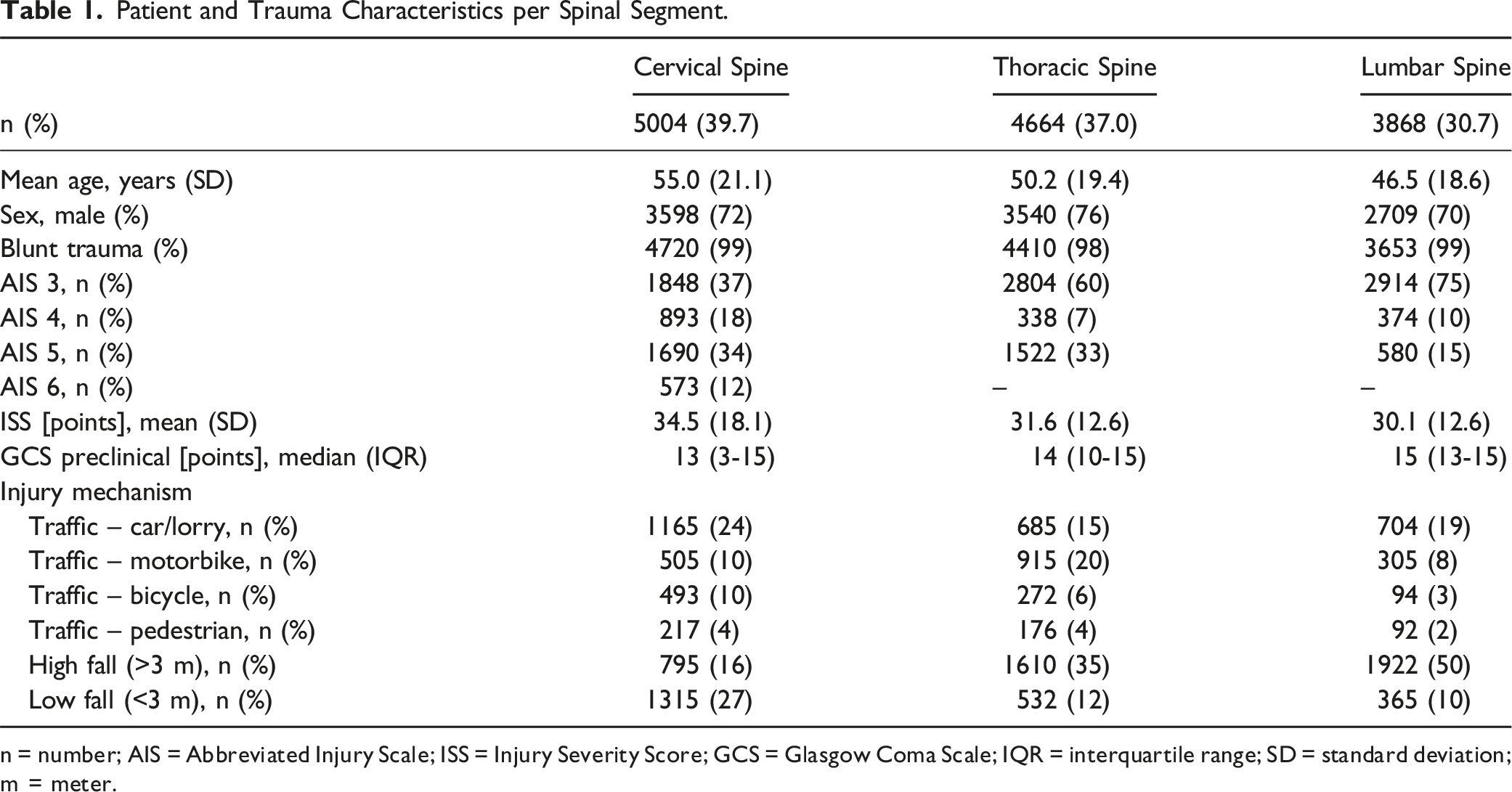
n = number; AIS = Abbreviated Injury Scale; ISS = Injury Severity Score; GCS = Glasgow Coma Scale; IQR = interquartile range; SD = standard deviation; m = meter.
Outcome Parameters.
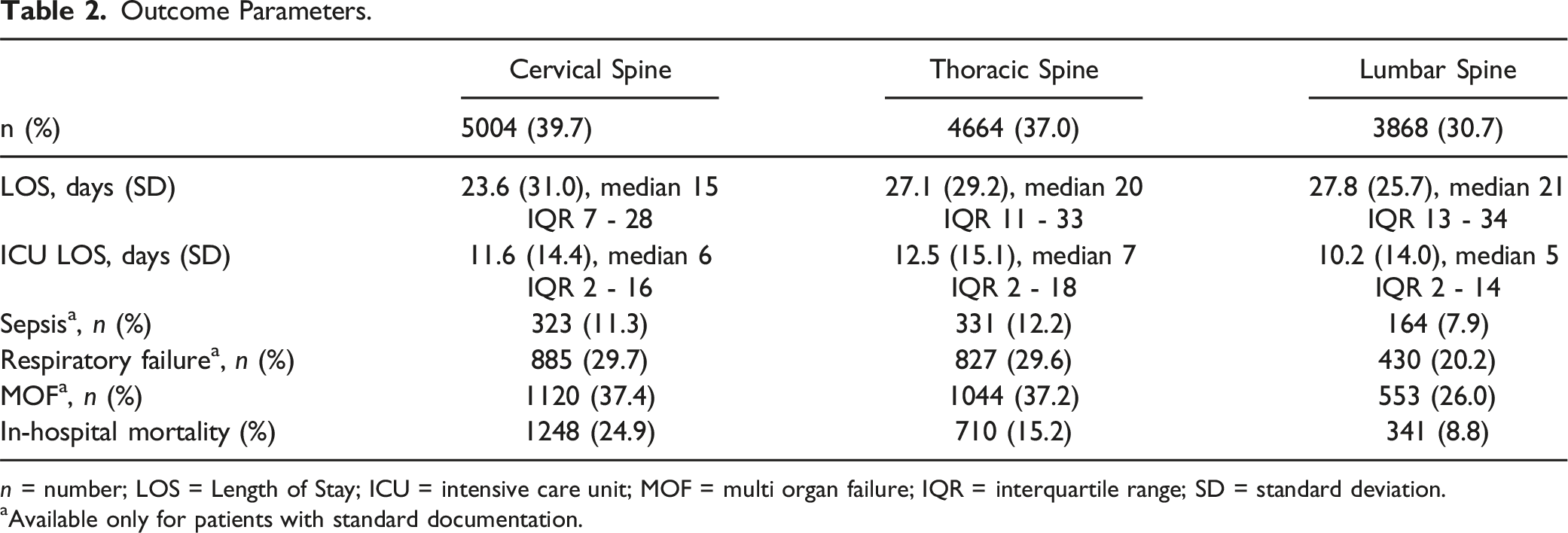
n = number; LOS = Length of Stay; ICU = intensive care unit; MOF = multi organ failure; IQR = interquartile range; SD = standard deviation.
aAvailable only for patients with standard documentation.
For the purpose of the study, patient and trauma characteristics as well as outcome were compared. Patients were initially grouped based on involved spinal segment (cervical-thoracic-lumbar). We further grouped patients based on timing of surgery. Group early consisted of individuals treated with spinal surgery within 48 hours after admission. Patients receiving spinal surgery later than 48 hours after admission were selected for Gr. Late. For the latter analysis we excluded patients with a spinal AIS of 6.
Statistical Analysis
A descriptive data analysis was performed to investigate the prevalence of concomitant injuries in spine injuries. Categorical variables are presented with counts and percentages, and continuous values are shown as mean, median and standard deviation (SD). In case of skewed data, median and inter-quartile range were presented instead. Due to the large number of patients included here, statistical testing was avoided since even minor and non-relevant differences would turn out to be formally significant. The statistical analysis was performed using Statistical Package for the Social Sciences (version 24, IBM Inc., Armonk, NY, USA).
Results
12 596 patients polytraumatized adult patients with a mean age of 50.8 ± 20.2 years were identified. An overview of patient in- and exclusion is displayed as a flowchart in Figure 1. An overall male predominance of 72.7% was encountered. The most common mechanism of injury was a fall from great heights (31.1%), and this mechanism of injury was most frequently encountered in patients diagnosed with lumbar injuries, namely in up to 50.0% of cases. Most patients suffered from injuries of the cervical spine (39.7%), followed by thoracic injuries (37.0%) and lumbar spinal injuries (30.7%). Multisegmental injuries were encountered in 909 cases (representing 7.2% of all included patients). In .2% of the entire cohort (n = 31), all spinal segments were involved. Severe injuries (AIS ≥4) were most frequently diagnosed in the cervical spine group. Furthermore, patients with cervical spinal injuries had the highest mean ISS (34.5 ± 18.1), and the most profound impaired (1-2 points) Glasgow Coma Scale (GCS)-score compared with thoracic or lumbar spine injuries. Patient and trauma characteristics are shown in Table 1. Patient inclusion flowchart.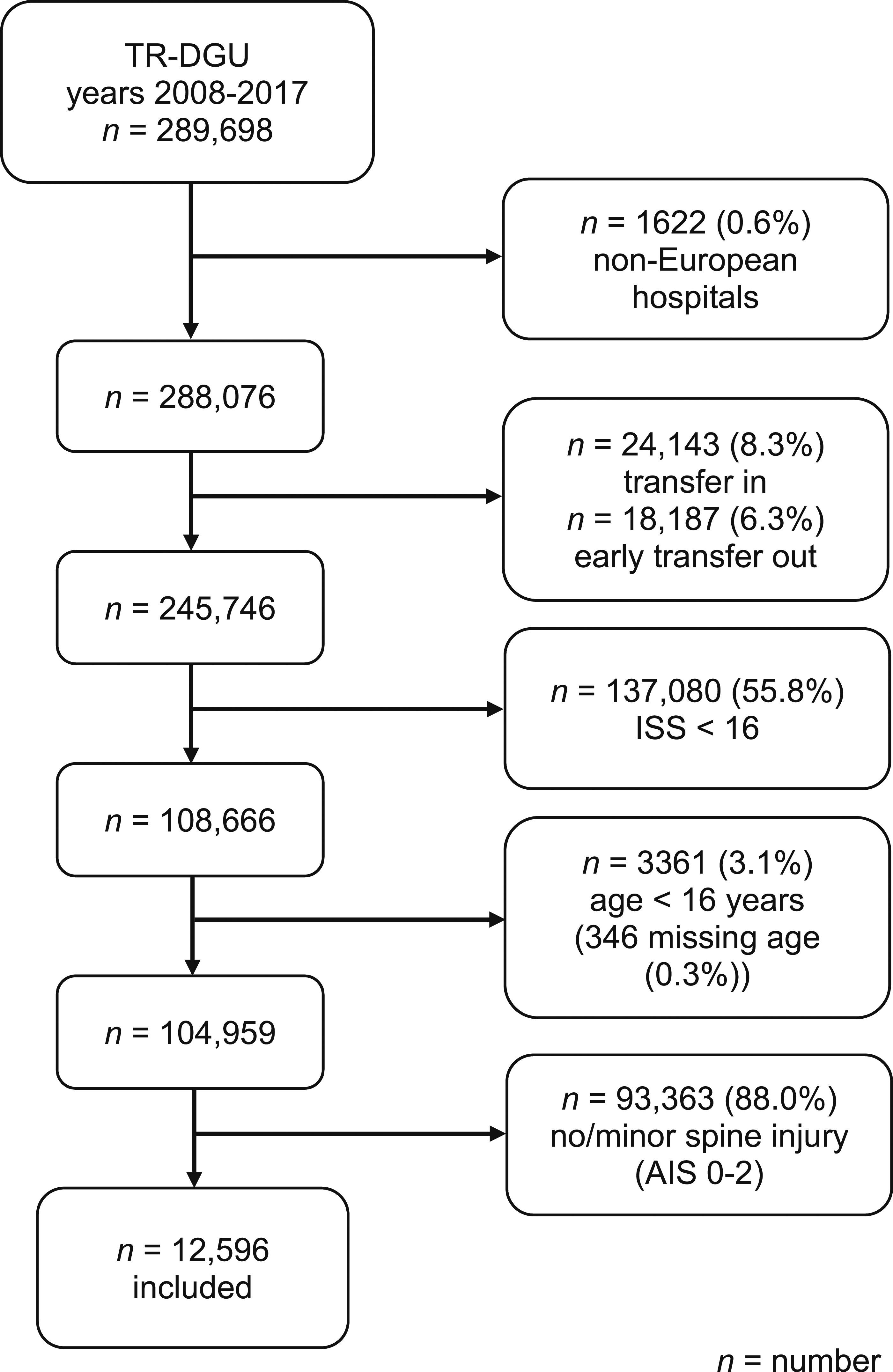
Patients with cervical injuries had shorter mean LOS than individuals with thoracic or lumbar injuries. Spinal segmentation was not markedly linked with aberrant durations of ICU-stay. Although, in-hospital mortality almost doubles per spinal segment from caudal to cranial and peaks in patients with a cervical spine injury (24.9%). Complication rates were highest in both patients with cervical or thoracic spinal injuries. Outcome per group is displayed in Table 2.
The Occurrence of Concurrent Injuries and Spinal Segmentation
Concomitant Non-spinal Injuries (AIS ≥2) per Spinal Segment.
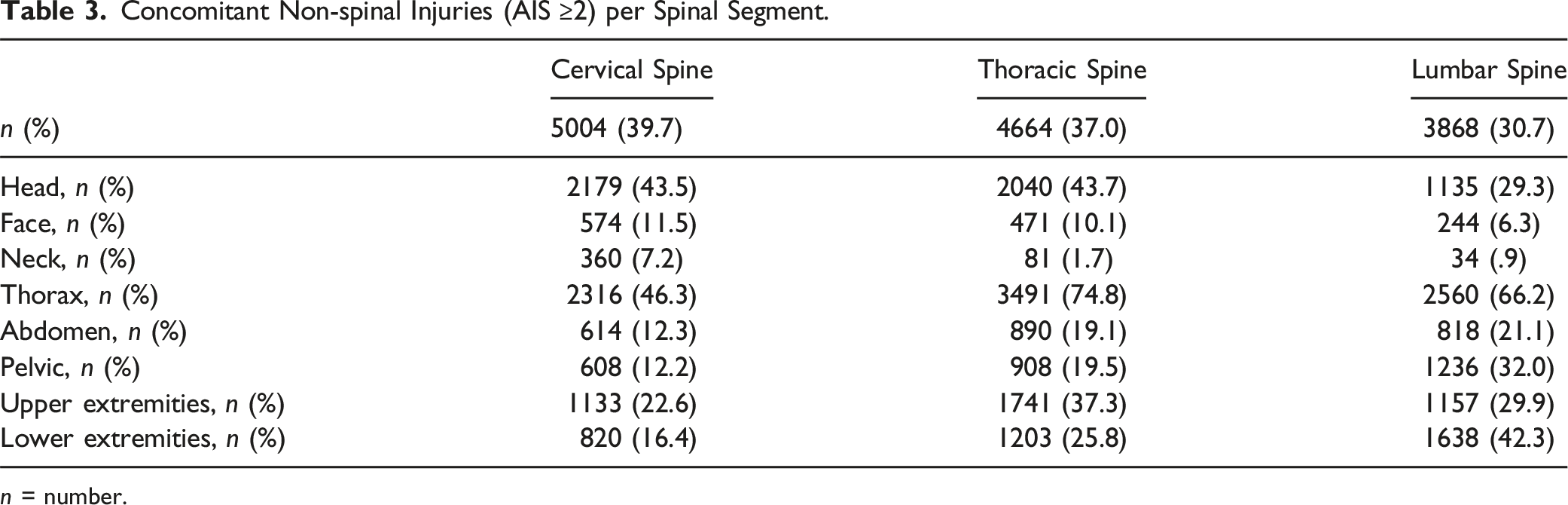
n = number.
Timing of Spinal Surgery and Outcome in Polytrauma
Polytrauma patients with spinal injuries mainly underwent early (<48 h) surgical treatment, irrespective of the spinal segment. Comparable numbers of patients with an injury severity of AIS 3 in the cervical (24.9% early vs 22.3% late) or thoracic (35.5% early vs 31.2% late) spine are treated surgically early or late (>48 h), with a tendency towards early treatment. With an increasing AIS, there is a tendency towards surgery at an early stage (<48 h), regardless of the spinal segment (Figure 2). Of note, in order to avoid distortion of the statistics in Figure 2, patients who died in the first 24 hours were not included in this calculation. Time of surgery related to AIS.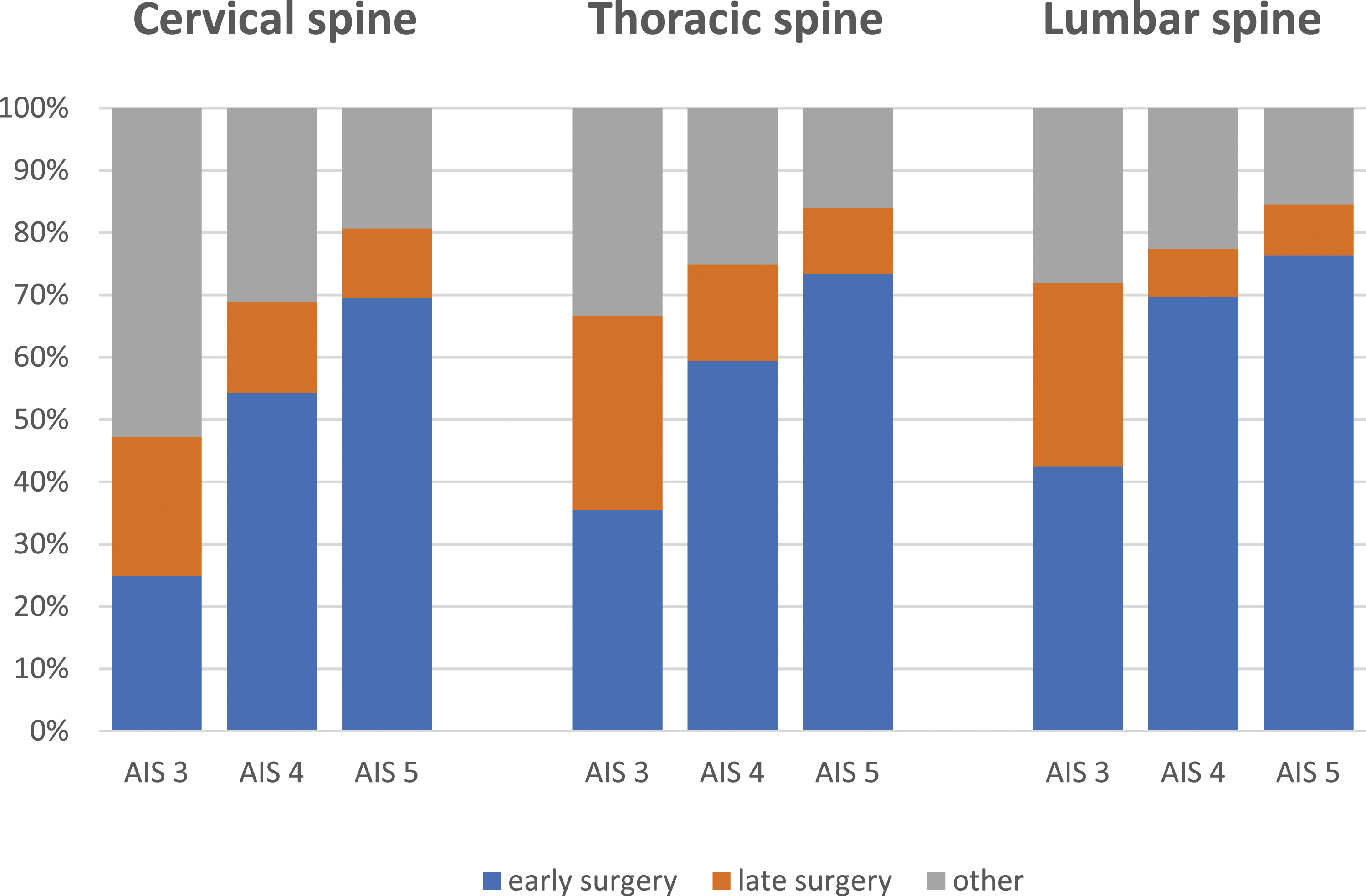
Outcome of Early (<48 hrs) and Late Spinal Surgery in Polytrauma per Spinal Region.
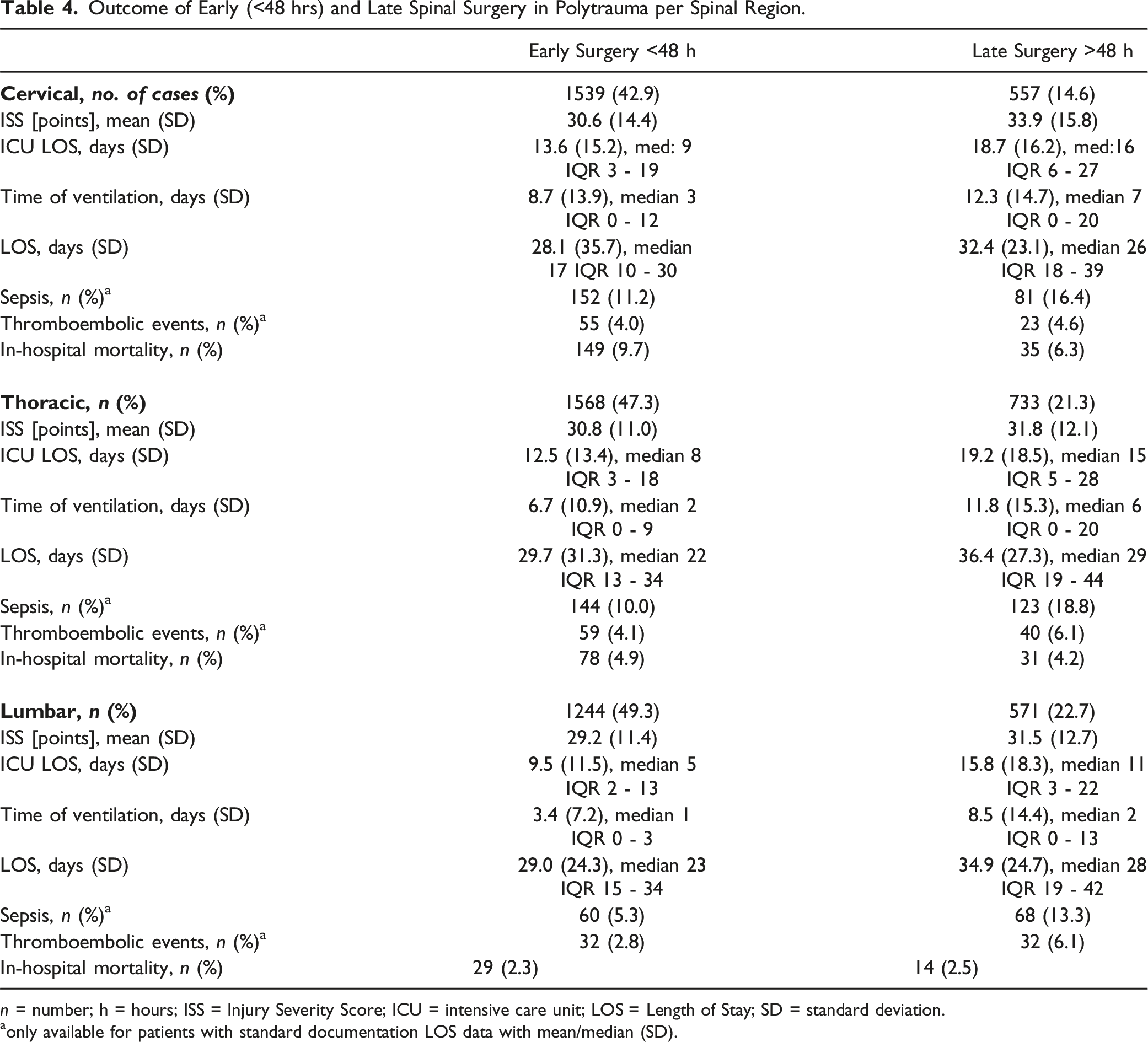
n = number; h = hours; ISS = Injury Severity Score; ICU = intensive care unit; LOS = Length of Stay; SD = standard deviation.
aonly available for patients with standard documentation LOS data with mean/median (SD).
Discussion
The key findings of this multicenter study on 12.596 polytrauma patients with spinal injuries may be summarized as follows: 1. In polytrauma patients 7.2% of patients suffer from relevant multisegmental spinal injuries. Furthermore, high incidences of non-spinal (mainly thoracic) injuries occur in patients with serious spinal injuries, regardless of spinal injury localization. 2. Similar incidences of relevant concurrent head injuries are diagnosed in polytrauma patients with cervical spinal injuries as in patients with thoracic spinal injuries. 3. Outcome of polytrauma patients with lumbar and thoracic spinal injuries seems to be superior upon early spinal surgery (<48 hrs), although differences in in-hospital mortality were not identified. 4. In-hospital mortality of polytrauma patients with spinal injuries is highest in individuals with cervical injuries and mortality rates are markedly higher in patients undergoing early spinal surgery.
These findings underline the importance of the ATLS´s recommendation to execute a full-spinal examination in trauma patients diagnosed with spinal injuries. Given the overrepresentation of associated thoracic injuries in this collective, severely injured trauma patients with spinal injuries may benefit from standardized imaging of the thorax as well. Moreover, the findings of this large-database study suggest that polytrauma patients with either thoracic or cervical spinal injuries might qualify for standardized cerebral imaging. The outcome data of the current investigation demonstrate that cranialization of spinal injuries is linked with increased mortality. Early spinal surgery seems to be beneficial for both lumbar and thoracic spinal injury patients, although mortality-rates do not differ between groups. In these injuries a spine-first approach seems appropriate. In the specific case of polytrauma patients with cervical spinal injuries, optimal timing of surgery is still under debate. Based on the findings of the current study however, it is tempting to hypothesize that delayed surgical spinal interventions are beneficial in specific patients. The authors like to speculate on the background of these observations and believe that delayed surgery in polytraumatized patients with cervical spine injuries, allows for restoration of systemic homeostasis first. This may prevent life-threating systemic complications upon polytrauma such as ARDS, organ failure and multiorgan dysfunction syndrome. Hypothesis-driven prospective multicenter studies are highly indicated to further confirm the findings of the current study. This may lead to the development of novel, selection criteria for early intervention in the polytraumatized patients.
In the total collective of polytrauma patients, about 12% of the severely injured patients had a relevant spine injury. Concomitant non-spinal injuries are common and impact clinical outcome, as well as timing of surgical intervention of the spine injury, and thereby secondary neurological and long-term outcome. This large database study is the first to validate historical assumptions on spinal and non-spinal combinational injury patterns. These findings may affect diagnostics in polytrauma patients. Looking at the frequent occurrence of a concomitant head injury in our collective of spine patients (about 43%), this injury pattern is well justified, and has been described in literature on high-impact trauma cases before. 9 A recent systemic review demonstrated corresponding findings. 8 The current study, however, was the first to demonstrate that thoracic spinal injuries in polytrauma are as predictive for head injuries as cervical spine injuries are. Therefore, both thoracic and cervical injuries should be considered as an indicator injury for TBI and vice versa. Nevertheless, a TBI is often not detected during diagnostics and acute care of patients with severe spine injuries. 32 Another clinically relevant aspect in the group of cervical spine injuries is the lower preclinical GCS identified in our data, which may have an impact on long-term outcome. 33 Because of the high clinical relevance, we included injuries of the cervical spine with their concomitant injuries to this analysis, in contrast to the analysis of Bliemel et al 2 Common other concomitant injuries of the thoracic spine are mainly injuries to the thorax in our collective. In particular, an accumulation of critical concomitant thorax injuries (AIS 5) has been found in this group, compared to patients with cervical or lumbar spine injuries. It is already known that traumatic chest injuries usually occur with rib fractures and lung contusions.4,34 The occurrence of these concomitant injuries can lead to respiratory impairment and pneumonia with subsequent increased morbidity and mortality in the clinical course.5,6 Cotton et al 6 showed in a large study that the risk of pneumonia and respiratory complications with subsequent intubation or tracheotomy was increased in patients with injury to the thoracic spine compared to those with injury to lumbar spine. This effect is also seen in our clinical outcome parameters, with an increased incidence of respiratory failure (29.6%) and sepsis (12.2%) in thoracic spine injuries (Table 2). Concomitant injuries of the thorax were also frequently seen in injuries to the lumbar spine (Table 3). This may be related to the fact that such injuries are often located at the thoracolumbar junction.4,35,36 And given the overall incidences of concurrent relevant thoracic injuries in polytrauma cases with spinal injuries may suggest the need of routine thoracic imaging in these patients. More focussed prospective studies on this issue are required in order to determine the impact of this alteration to standard trauma diagnostics on outcome.
In addition to previous studies, we managed to evaluate the role of timing of surgery on outcome per involved spinal segment in an overpowered dataset, rather than in a small patient collective.2,17,23,37 For this study we analysed the timing of the first spinal surgical intervention. Basically, our analysis indicates that patients undergo early surgical treatment (<48 h) more frequently with increasing severity of spine injury (Figure 2). This is in line with the analysis of Bliemel et al 2 In addition, our data show that 35.1% of patients with a leading spinal injury received early surgical treatment. However, if the patients had a more severe concomitant non-spinal injury (AIS 4-6), only 15.2% received early surgical treatment. Management was more often conservative in these cases. Only a small number of patients were treated surgically at a later time point.
Most studies on timing of spinal surgery report that early surgical treatment of spine injuries is beneficial, while defining different time points. McLain and Benson 22 compared immediate (<24 h) surgical treatment of the spine with a treatment between 24 and 72 hours in a group of severely injured patients (ISS >26). There was no difference in complication rates and mortality. Another study concluded that early surgical treatment of the spine allows earlier mobilisation, thus reducing the incidence of pressure ulcers and pulmonary complications. 5 Other advantages of early surgical treatment were a decreased length of stay on ICU, a decreased duration of mechanical ventilation as well as a decreased time of hospitalisation.18,19 Our data provide fairly similar results. All groups were comparable in terms of injury severity as defined by the ISS. Reduction of ventilator days was particularly notable in patients with thoracic or lumbar spine injuries in the early care group. In line with previous studies,24,34 we found a reduction of LOS in hospital and a reduction of LOS on ICU regardless of spinal segment. Interestingly, however, injuries to the cervical spine showed a significant increase of in-hospital mortality in the early care group. The chosen cut-off timepoint of 48 hours thus seems to be beneficial especially in injuries to the thoracic and lumbar spine. For injuries to the cervical spine, the ideal timepoint of surgery still needs to be evaluated and our findings warrant more in-depth evaluation of this matter.
Study Limitations
Due to register analysis, this study has some limitations. First, detailed information on indications (such as neurological status) for surgical intervention and clearing for surgery have not been reported. Although, no profound differences in baseline characteristics were found between study conditions in our comparative analyses. Secondly, a polytrauma database was used and as a consequence neurological outcome and long-term patient reported outcome was not collected. Third, specific AIS scores of the spinal injuries are not available in this polytrauma register. The ISS is the sum of the squares of the highest AIS code in each of the three most severely injured ISS body regions. The spine is not considered as a specific body region and spinal injuries can be added to the calculation as part of the following body regions: head or neck, chest or abdomen. However, in the case more severe injuries in the same domain are present the AIS of the specific spinal injury is not available.
Conclusions
The current multicentre study demonstrates that polytrauma patients frequently sustain spinal injuries. Spinal segmentation relates to specific patterns of associated injuries and this requires specific protocols for additional imaging. Given the high incidence of concurrent multiple spinal injuries in severely injured patients, whole spine imaging is suggested in the case of a diagnosed spinal index fracture. Timing of surgical management of the spine appears to depend on the severity of the concomitant injuries as well as on the affected segment of the spine. The findings of the current retrospective analysis suggest that early surgical management (<48 h) seems to be beneficial in thoracic and lumbar spine injuries. Caution is required for early surgical management of patients with cervical spine injuries, because it may lead to a greater mortality rate as seen in this retrospective, large cohort study. However, the retrospective analysis subjects it to potential confounding factors and our study is not suggesting surgical delay for cervical spinal cord injuries in patients medically fit for surgery as this can greatly improve their quality of life. More prospective studies on timing of surgery for specific spinal injuries in polytrauma patients is highly mandated.
Footnotes
Acknowledgments
Author Contributions
Conceptualization, K.S.; Formal analysis, J.H., M.T., S.H., K.O.J., R.L. and K.S.; Investigation, J.H., S.H., K.O.J., T.B., H.-C.P. and K.S.; Resources, J.H.; Supervision, K.S.; Writing—original draft, J.H., M.T.; Writing—review & editing, T.B., J.S., H.-C.P. and K.S. All authors have read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors state that this work has not been previously published in whole or in part or submitted elsewhere for review. R. L. declares that his institution receives ongoing support from AUC GmbH, the data holder of the TR-DGU. This support includes statistical analyses of the registry data.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Institutional Review Board Statement
This study has been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. Ethical approval was not needed due to retrospective use of medical records.
Data Availability Statement
The authors state that the sensitive data presented in this study is available from a third party, which is the AUC - Academy for Trauma Surgery (“Akademie der Unfallchirurgie GmbH”), which is the owner of the data of the TR-DGU. The data underlying the results presented in the study are available under consideration of the publication guideline from: AUC - Akademie der Unfallchirurgie GmbH, Emil-Riedel-Straße 5, 80538 München, Deutschland.