
Abstract
Study Design:
Retrospective cohort study.
Objective:
To assess the impact of fondaparinux on venous thromboembolism (VTE) following elective lumbar spine surgery in high-risk patients.
Methods:
Matched patient cohorts who did or did not receive inpatient fondaparinux starting postoperative day 2 following elective lumbar spine surgery were compared. All patients received 1 month of acetyl salicylic acid 325 mg following discharge. The primary outcome was a symptomatic DVT (deep vein thrombosis) or PE (pulmonary embolus) within 30 days of surgery. Secondary outcomes included prolonged wound drainage, epidural hematoma, and transfusion.
Results:
A significantly higher number of DVTs were diagnosed in the group that did not receive inpatient VTE prophylaxis (3/102, 2.9%) compared with the fondaparinux group (0/275, 0%, P = .02). Increased wound drainage was seen in 18.5% of patients administered fondaparinux, compared with 25.5% of untreated patients (P = .15). Deep infections were equivalent (2.2% with fondaparinux vs 4.9% control, P = .18). No epidural hematomas were noted, and the number of transfusions after postoperative day 2 and 90-day return to operating room rates were equivalent.
Conclusions:
Patients receiving fondaparinux had lower rates of symptomatic DVT and PE and a favorable complication profile when compared with matched controls. The retrospective nature of this work limits the safety and efficacy claims that can be made about the use of fondaparinux to prevent VTE in elective lumbar spine surgery patients. Importantly, this work highlights the potential safety of this regimen, permitting future high-quality trials.
Keywords
Introduction
The prevention of venous thromboembolism (VTE) following orthopedic procedures has largely focused on the trauma and adult reconstruction populations. 1 -6 However, the incidence of pulmonary embolus (PE) and deep venous thrombosis (DVT) following spine surgery has been reported to be as high as 18% and 19%, respectively 7,8 Hohl et al 9 in their multi-institutional study of patients who underwent elective thoracolumbar surgery reported an overall VTE prevalence of 1.5%, of symptomatic PE 0.88%, and of DVT 0.66%. They also reported that while patients >65 years old at the time of surgery had a 2.196 times higher prevalence of DVT and PE, sex, instrumentation, and revision surgery were not risk factors for VTE. A National Surgical Quality Improvement Program (NSQIP) study by Schoenfeld et al 10 found a 1% incidence of VTE after spine surgery at any level, with a significantly increased risk of DVT seen in patients with a body mass index ≥40 kg/m2, age ≥80 years, operative time >261 minutes, and American Society of Anesthesiologists classification of ≥3.
There is currently no gold standard for the administration of VTE prophylaxis following elective spine surgery. Current recommendations are based on limited evidence, and proposed algorithms remain controversial. Recent work suggests that the risk of bleeding complications after elective spine surgery is negligible when weight-based subcutaneous heparin or low-molecular-weight heparin is started 24 hours after surgery. 11,12 Fondaparinux, a once-a-day injectable, has been found to have an equivalent benefit, risk reduction, and complication rate after total joint surgery compared with multidose enoxaparin. 13 However, its utility as chemoprophylaxis after spine surgery has not been established.
The purpose of the present study was to assess the impact of fondaparinux on VTE following elective lumbar spine surgery in high-risk patients. We hypothesized that fewer VTEs would occur in patients administered fondaparinux compared with matched peers, without an increased risk of postoperative complications.
Methods
Study Population and Patient Selection
In a University of Pittsburgh Institutional Review Board-approved protocol (#PRO14090068), a retrospective analysis of 6 years (January 2009 to December 2015) of patients who underwent elective lumbar (including thoracolumbar junction and lumbosacral) spine procedures was performed. Patients who received any other VTE prophylaxis during their inpatient stay (ie, warfarin, heparin, etc) were excluded from this analysis. Both primary and revision procedures were included. All patients had 7-French drains placed intraoperatively, with the number of drains dependent on intraoperative bleeding.
Venous Thromboembolic Prophylaxis
All patients received mechanoprophylaxis with pneumatic compression devices postoperatively and were prescribed 30 days of acetyl salicylic acid (ASA) 325 mg following discharge. Patients who were at a higher medical risk of developing a postoperative VTE were identified according to criteria listed in Figure 1. In those patients, fondaparinux 2.5 mg subcutaneous daily was started on postoperative day 2 and continued throughout admission. The selection of fondaparinux was due to its once-a-day dosing and equivalent safety profile in arthroplasty patients. 14,15 Drains were maintained for at least 24 hours after the start of fondaparinux, then removed based on output.
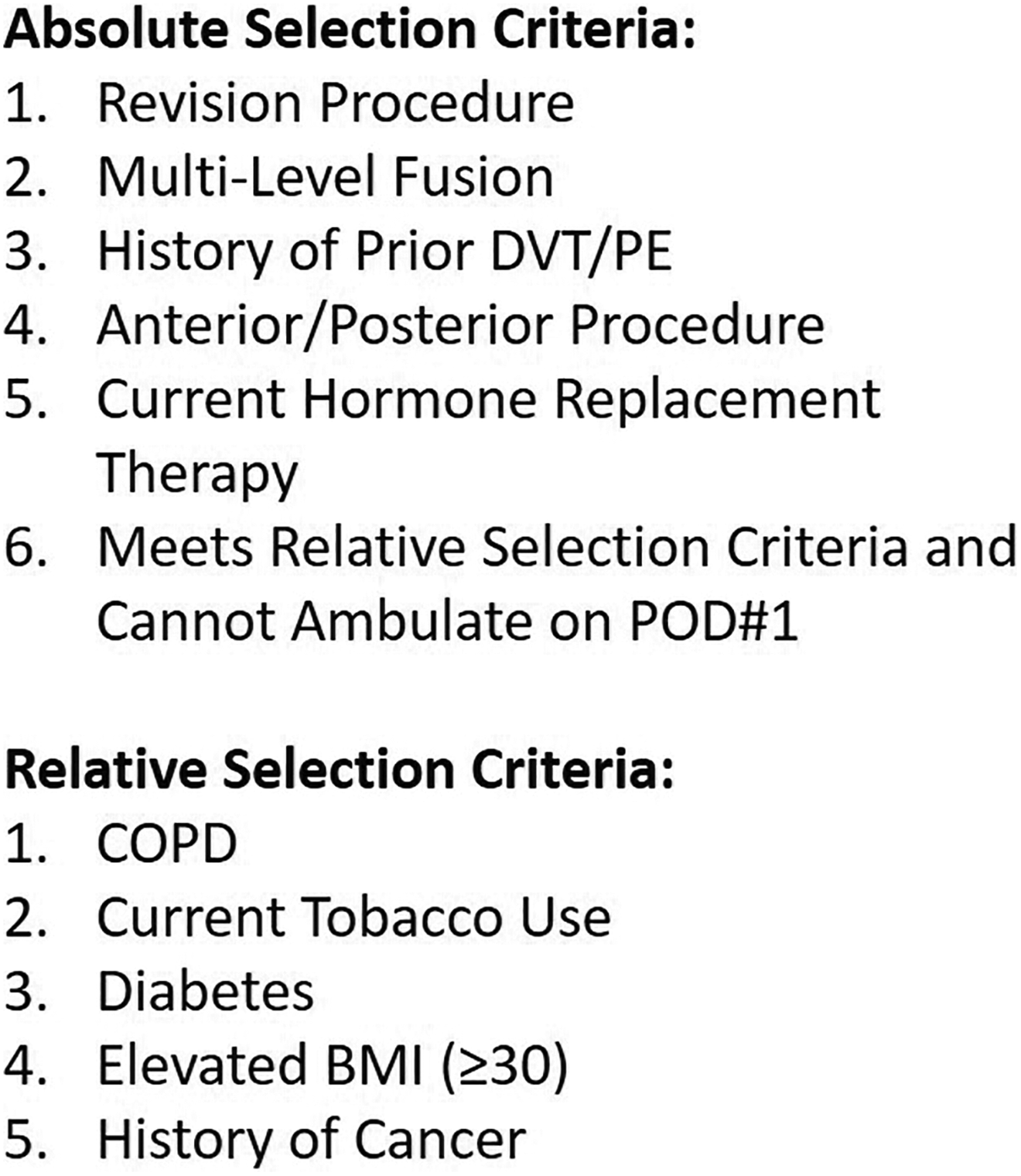
Absolute and relative selection criteria for the use of fondaparinux starting on postoperative day 2.
Data Collection
In addition to the high-risk criteria used to indicate fondaparinux prophylaxis, patient characteristics used to establish a matched cohort included age on the date of surgery, gender, and Age-Adjusted Charlson Comorbidity Index (AACCI). 16
The primary outcome measure was the incidence of a symptomatic DVT within 30 days of surgical intervention. Secondary outcomes included pulmonary embolism, epidural hematoma, minor wound complications that resolved without operative intervention, and major wound complications that required a return to the operating room. All recorded thromboembolic diagnoses were confirmed using venous duplex ultrasound for DVT and chest computed tomography (CTPE) for PE.
Statistical Analysis
Data are reported as mean ± standard deviation for continuous variables, and as percentages for categorical variables. Continuous variables were compared using the Student’s t test, while dichotomous variables were compared using Fisher’s exact test. Statistical analyses were performed by the investigators using GraphPad Prism 7.0 (La Jolla, CA), with significance defined as P < .05.
Results
A total of 724 patients underwent elective spine surgery during the study period. Of these, 377 met high-risk patient criteria (Figure 2); 275 received fondaparinux followed by 30 days of ASA following discharge, while 102 received outpatient ASA alone. Matched cohorts based on absolute risk factors were established (Table 1). An equivalent proportion of patients met each criterion in the ASA-only and the fondaparinux + ASA groups, except for those who underwent multilevel fusions (63/102, 61.8% in ASA-only group vs 227/275, 82.5% in the fondaparinux + ASA group, P < .0001). The mean number of absolute risk factors was also significantly greater in the fondaparinux + ASA group (2.3 ± 1.0 vs 1.5 ± 0.6 in the ASA-only group, P = .01). Patient characteristics in each cohort are shown in Table 2.
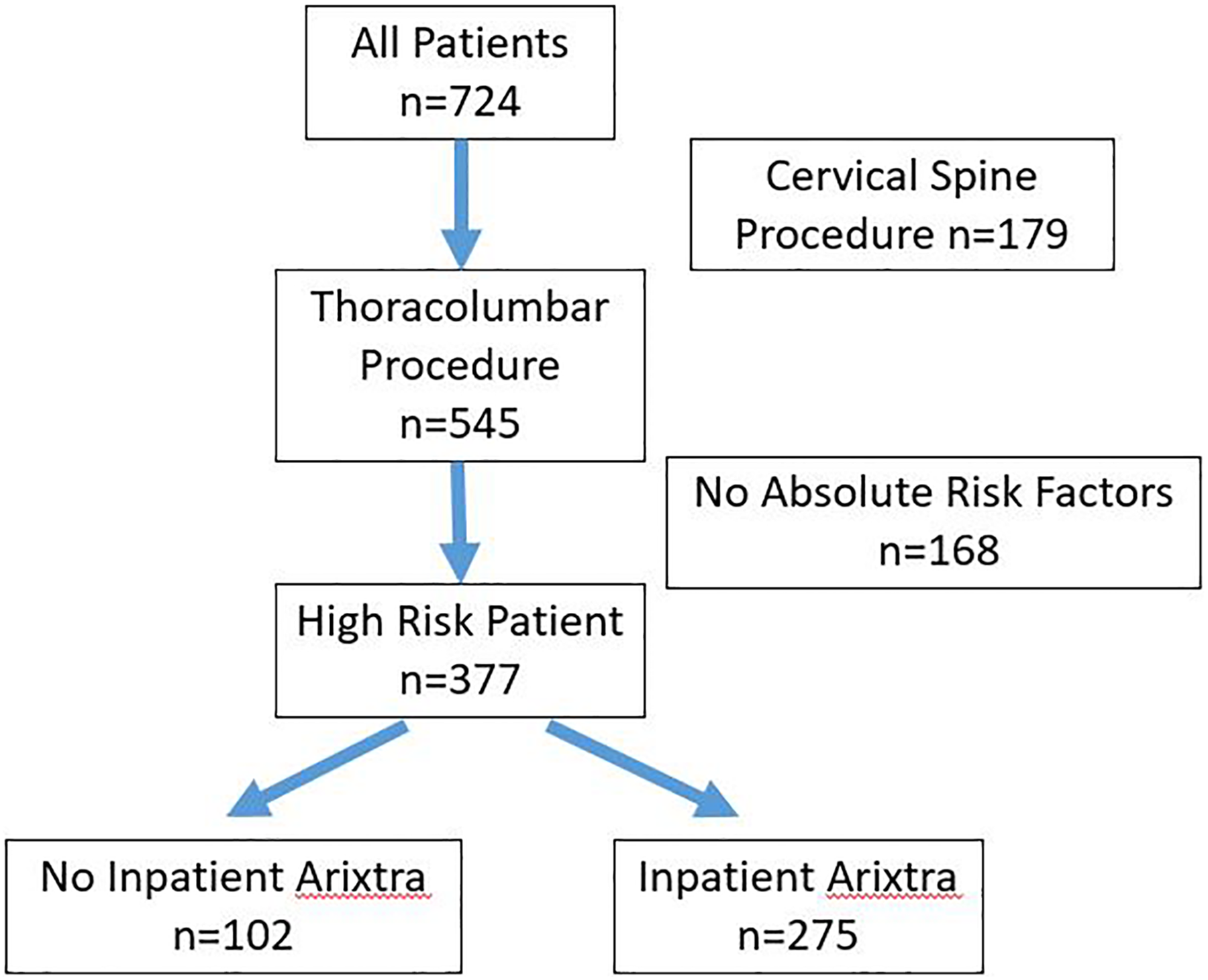
Patient selection flowchart.
Patient Inclusion by Absolute Risk Factor.
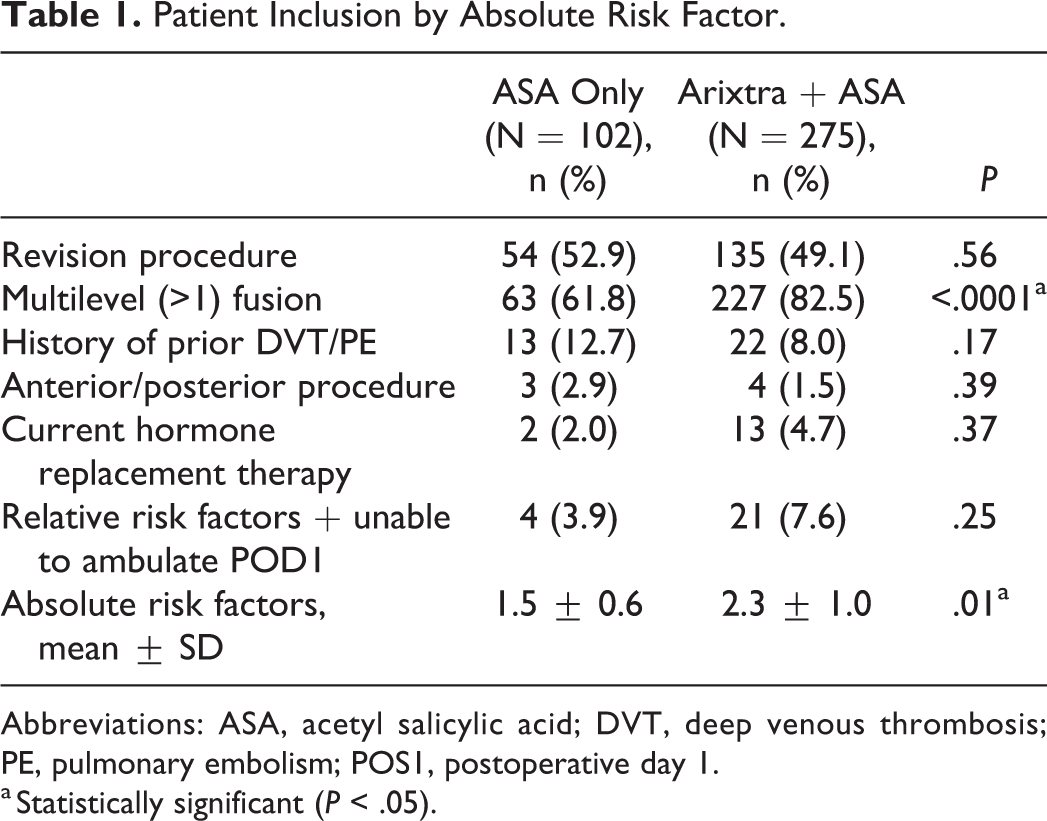
Abbreviations: ASA, acetyl salicylic acid; DVT, deep venous thrombosis; PE, pulmonary embolism; POS1, postoperative day 1.
a Statistically significant (P < .05).
Study Patient Characteristics.
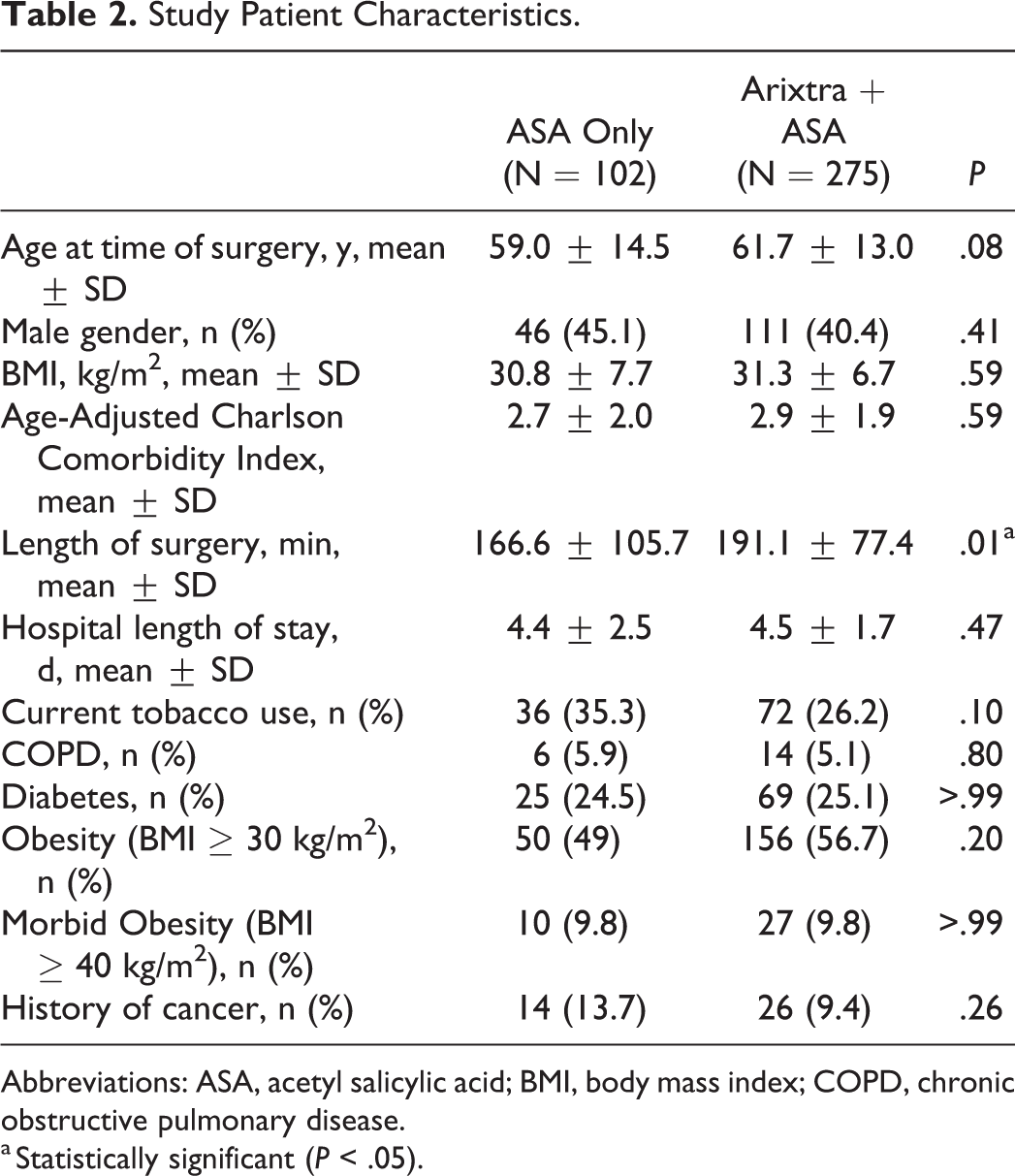
Abbreviations: ASA, acetyl salicylic acid; BMI, body mass index; COPD, chronic obstructive pulmonary disease.
a Statistically significant (P < .05).
Three patients in the ASA-only group and no patients in the fondaparinux + ASA group were diagnosed with a DVT (3/102, 2.9%) within 30 days of hospital admission (P = .02, Table 3). Two ASA-only patients (2/102, 2.0%) and 1 fondaparinux + ASA patient developed PEs (1/275, 0.4%, P = .49). The incidence of deep infections (6/275, 2.2% with fondaparinux + ASA vs 5/102, 4.9% with ASA-only, P = .18) and gross wound dehiscence were also equivalent (4/275, 1.5% with fondaparinux + ASA vs 2/102, 2% with ASA-only, P = .66). No epidural hematomas were diagnosed in either group and an equivalent number of packed red blood cell transfusions after postoperative day 2 were required (8/102, 8.2% in ASA-only vs 38/275, 15.0% in fondaparinux + ASA, P = .16). Eight patients in the ASA-only group required a return to operating room for infectious or drainage complication (7.8%), while 11 in the fondaparinux + ASA group required the same (11/275, P = .18).
Clinical Complications.
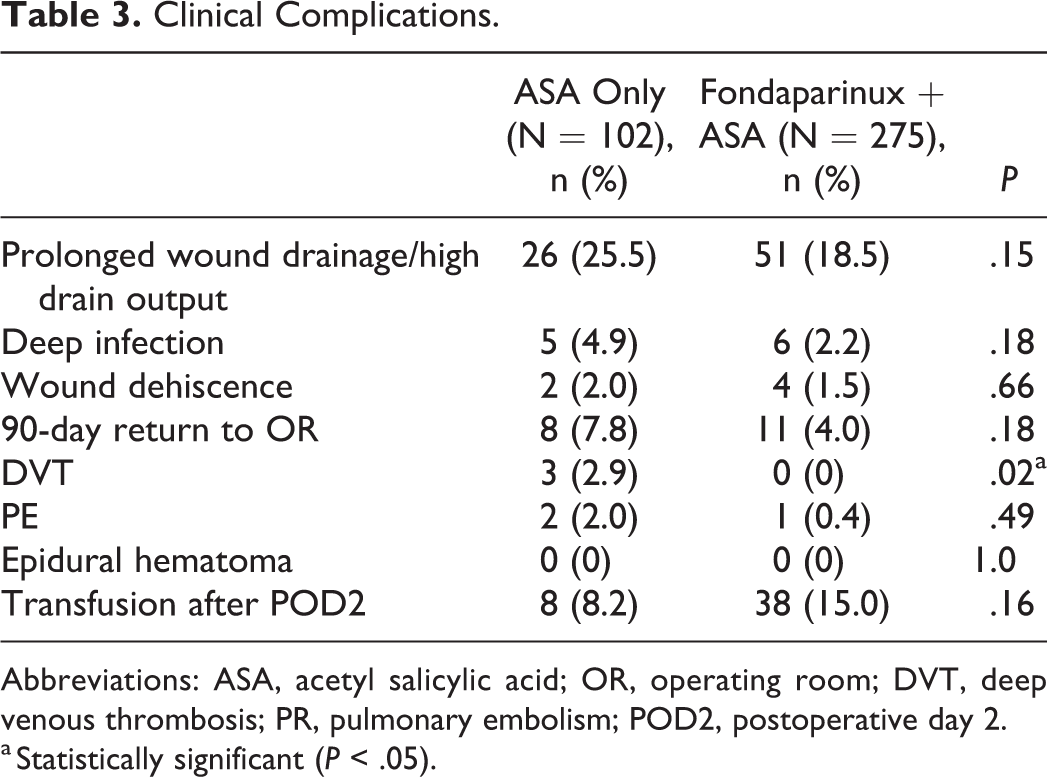
Abbreviations: ASA, acetyl salicylic acid; OR, operating room; DVT, deep venous thrombosis; PR, pulmonary embolism; POD2, postoperative day 2.
a Statistically significant (P < .05).
Discussion
In a retrospective analysis of a 6-year experience using inpatient fondaparinux in addition to home ASA as VTE chemoprophylaxis in select high-risk patients, patients administered fondaparinux had a significantly lower incidence of symptomatic DVTs, without an increased risk of postoperative complication. While prospective validation is required, the present study suggests that fondaparinux should be considered in patients with medical comorbidities that place them at a higher risk of perioperative VTE.
Current literature on VTE prophylaxis after elective spine surgery is underpowered, 17 heterogeneous, 18 or utilizes nonvalidated surgeon-response metrics. 19 Survey studies by Ploumis et al 20 and Glotzbecker et al 21 criticize the inconsistent application of VTE prophylaxis after high-risk spine procedures, noting that even spinal cord injuries did not clearly delineate common practice. This echoes prior reservations expressed in existing literature over the past 3 decades, 22 and may be related to vagaries in current recommendations. However, multifactorial medical comorbidity imparts a clear risk of VTE following elective spine surgery.
Retrospective works and national database studies on VTE after elective spine surgery suffer from underdiagnosis and systematic reporting bias. These studies report an incidence of DVT and PE following elective spine procedures of 0.78% to 2.5% and 0.06% to 0.8%, respectively. 17,23 -26 Prospective, universal screening protocols report an exponentially higher incidence of VTE. Takahashi et al 7 performed contrast-enhanced CT on 100 patients 1 week after elective spine surgery, identifying asymptomatic PEs in 18% of patients. This is similar to the CT screening protocol performed by Inoue et al, 8 who identified asymptomatic VTEs in 13% (PE in 8%) of patients. Tominaga et al 27 performed lower extremity duplex ultrasound on 80 patients following elective spine surgery, identifying DVTs in 25%. This incidence is as common as VTE after total knee arthroplasty. 28 While the understanding of the relative prognostic clinical significance of symptomatic versus asymptomatic VTE makes interpreting this difference difficult, these studies nonetheless demonstrate that the overall incidence of VTE after spine surgery is substantial.
Common risk factors for VTE after elective spine surgery include increasing age, 18,29,30 coagulopathy, 31 malignancy, 30 hypertension, 32 reduced mobility or functional disability, 33 -35 and surgical factors, including length of surgery and blood loss. 18,36 -38 Hohl et al 9 report a significant increase in symptomatic PEs (3%) in patients who underwent fusions of 5 or more segments. Jacobs et al 39 noted risk factors for VTE in spine trauma patients to be the result of prolonged operative time, reduced mobilization, and increased systemic inflammation. Piper et al, 36 in a NSQIP query of 22 434 patients who underwent any spine surgery, identified 13 predisposing factors for VTE, which included hypertension, an operative time of 4 hours or greater, American Society of Anesthesiologists classification of ≥3, quadriplegia/paraplegia, and inpatient status. However, their work studied all-comers and included both inpatient/outpatient procedures and acute/elective indications.
VTE prophylaxis efficacy and safety studies are largely inconsistent, retrospective, and underpowered. A systematic review by Glotzbecker et al 40 found a 50% reduction in symptomatic VTE when both compression stockings and pneumatic compression mechanoprophylaxis were employed following spine surgery in all-comers. In this broad population, pneumatic compression was equivalent to chemoprophylaxis in VTE risk reduction. Associations between VTE chemoprophylaxis modalities sporadically demonstrate an increased risk of bleeding, epidural hematoma, or wound drainage, are commonly underpowered to prove therapeutic efficacy, and rely on retrospective data. Cox et al, 12 determined that starting unfractionated heparin on the day of surgery in all-comers decreased the risk of VTE, although complications were not addressed. The risk of bleeding with unfractionated heparin was reported to be substantial. McLynn et al 34 in their NSQIP study reported that unfractionated heparin increased the relative risk of developing an operative hematoma by 7.37 times. Warfarin was similarly associated with increased perioperative blood loss, as preoperative dosing was required to achieve postoperative therapeutic effect. 41 In contrast, this bleeding risk was not present in patients treated with low-molecular-weight heparin starting 36 hours after cervical or lumbar elective spine procedures. 11 Few prior works have evaluated “nontraditional” VTE prophylaxis methods, such as factor Xa inhibitors, in the elective spine population. However, a single prospective randomized trial by Du et al 42 compared oral rivaroxaban and parnaparin started 6 to 8 hours after lumbar spine surgery for 14 days total. No difference was observed in risk reduction or complication between groups.
Limited literature has led to inconclusive consensus recommendations. The North American Spine Society cited a lack of high-quality studies regarding VTE prophylaxis after elective surgery, rendering an official recommendation that decisions regarding VTE prophylaxis be made on a patient-by-patient basis, balanced with a risk of postoperative bleeding that existing literature failed to demonstrate was outweighed by therapeutic efficacy. 43,44
The American College of Chest Physicians nearly universally recommended use of pneumatic compression devices following spine surgery. This included high-risk patients, despite the authors citing a lack of high-quality literature to support such recommendations. 45 Recommendations for postoperative spine VTE prophylaxis from the National Institute for Health and Clinical Excellence (NICE) in the United Kingdom included the use of mechanical thromboprophylaxis, with the addition of low-molecular-weight heparin for high-risk patients. 46 Individual works have proposed their own novel criteria for chemoprophylaxis. Eskildsen et al 47 proposed a point-based, 3-part criterion for VTE prophylaxis after spine surgery that considers patient, surgical, and bleeding risks. This algorithm reflects many of the same risk factors used as absolute criteria in our work, such as the use of estrogen-containing contraceptives, revision procedures, or multilevel interventions. Unique to their protocol was a score subtraction for high bleeding risk patients, which was not considered in our present study. The wide diversity of rendered opinions illustrates the importance of identifying an ideal therapy following major spine surgery, particularly with respect to comorbid patients. However, it also exposes the shortcomings of existing works.
The selection of fondaparinux, an indirect, selective factor Xa inhibitor, was because of its convenience, once-a-day dosing and previously effective use in the arthroplasty population. 48 While the mechanism of action of fondaparinux does significantly affect the coagulation cascade, it has no effect on platelets and has displayed the potential to prevent complications in patients with heparin-induced thrombocytopenia. 49 Concerns about major bleeding with fondaparinux therapy observed perioperatively after major abdominal surgeries 50 have largely not been borne out in the orthopedic literature when a dosing of 1.5 to 3.0 mg daily was employed. 51 While a slight, nonsignificant increase in the risk of bleeding was noted, Venker et al 52 in their meta-analysis comparing the efficacy and bleeding risks of newer anticoagulation modalities with enoxaparin in the total joint population found that fondaparinux was more effective than 30 mg twice-daily enoxaparin in reducing the risk of VTE. This agreed with a previous meta-analysis of 4 high-quality trials comparing fondaparinux and enoxaparin. 13 Unlike traditional anticoagulation modalities, there was no dose- or time-dependent renal accumulation of a reduced fondaparinux dosing (1.5 mg daily) in patients with chronic kidney disease, 53 with outcomes equivalent to healthy patients receiving enoxaparin. 54 Starting fondaparinux on postoperative day 2 was largely based on surgeon preference, although it should be noted that premature dosing of fondaparinux <6 hours after surgery has been associated with an increased risk of major bleeding after abdominal surgery. 50
Limitations
While this study is a retrospective analysis of prospectively collected data, the choice of fondaparinux therapy for higher risk patients invites a clear potential for selection bias. While powered to detect differences between groups, the present study includes a small sample size of convenience that was not designed to establish causality between the use of fondaparinux and a reduction in the incidence of VTE.
The study was conducted at a tertiary referral center where complex spine surgery is routinely performed, thus conclusions may not be generalizable to the population at large, and external validation studies are required. Therapeutic length was not standardized, as fondaparinux was administered only during the inpatient stay. Inpatient mechanoprophylaxis and postdischarge aspirin was employed in all patients. The utility of fondaparinux reported in the present study must therefore be considered as a part of a larger multimodal VTE prophylaxis strategy. Length of fondaparinux therapy and time until transition to aspirin was dependent on the length of hospital stay.
Findings of this work must be validated through a high-quality randomized controlled trial before clinical recommendations can be rendered. This study in no way replaces a randomized controlled trial and makes no claims about the safety or efficacy of fondaparinux.
Conclusion
The addition of fondaparinux as inpatient VTE prophylaxis following elective spine surgeries in comorbid patients significantly decreased the incidence of VTE compared with postdischarge ASA alone. The use of fondaparinux was also not associated with an increased incidence of post-operative complications. While the potential of fondaparinux in this patient group is encouraging, high-quality multicenter trials are required to validate these findings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.