
Abstract
Study Design:
Cross-sectional, international survey.
Objectives:
To identify factors influencing pharmacologic anticoagulation initiation after spine surgery based on the AOSpine Anticoagulation Global Survey.
Methods:
This survey was distributed to the international membership of AOSpine (n = 3805). A Likert-type scale described grade practice-specific factors on a scale from low (1) to high (5) importance, and patient-specific factors a scale from low (0) to high (3) importance. Analysis was performed to determine which factors were significant in the decision making surrounding the initiation of pharmacologic anticoagulation.
Results:
A total of 316 spine surgeons from 64 countries completed the survey. In terms of practice-specific factors considered to initiate treatment, expert opinion was graded the highest (mean grade ± SD = 3.2 ± 1.3), followed by fellowship training (3.2 ± 1.3). Conversely, previous studies (2.7 ± 1.2) and unspecified guidelines were considered least important (2.6 ± 1.6). Patient body mass index (2.0 ± 1.0) and postoperative mobilization (2.3 ± 1.0) were deemed most important and graded highly overall. Those who rated estimated blood loss with greater importance in anticoagulation initiation decision making were more likely to administer thromboprophylaxis at later times (hazard ratio [HR] = 0.68-0.71), while those who rated drain output with greater importance were likely to administer thromboprophylaxis at earlier times (HR = 1.32-1.43).
Conclusion:
Among our global cohort of spine surgeons, certain patient factors (ie, patient mobilization and body mass index) and practice-specific factors (ie, expert opinion and fellowship training) were considered to be most important when considering anticoagulation start times.
Keywords
Introduction
Venous thromboembolism (VTE) is a preventable cause of perioperative morbidity and mortality after spine surgery, with a variable reported incidence of 0.3% to 31%.1-7 This wide range of VTE after spine surgery can be explained by the variation in indication for spine surgery, diverse patient populations, as well as lack of consistency in the method and timing of diagnosis. Given the heterogeneity of medical comorbidities, spinal pathology, and surgical techniques, a need for patient-specific anti-coagulation guidelines is mounting.
Both pharmacologic and non-pharmacologic methods of VTE prophylaxis are available after spine surgery. Early patient mobilization, sequential compression devices (SCDs), and compression stockings are common non-pharmacologic approaches to VTE prophylaxis.4,8,9 Pharmacologic VTE prophylaxis consists of agents that target platelet function or other various points in the coagulation cascades.10-13 Examples of such medications include aspirin, heparin, low-molecular-weight heparin (LMWH), and warfarin. These agents can provide powerful prophylaxis against one potentially devastating complication (VTE), but their use must be balanced against equally significant adverse events, including epidural hematoma, excessive blood loss, and persistent wound drainage with subsequent infection.14-16
There are currently no widely accepted global guidelines regarding timing of initiation of perioperative VTE prophylaxis for patients undergoing spine surgery. Although some studies have made recommendations regarding timing of the start of anti-coagulation and anti-platelet medications, as well as created recommendations in patients undergoing spine surgery for spinal cord injury, these have been limited by small sample sizes that prevent extensive assessment of risk factors and heterogeneity among anti-coagulation methods.17-21 In 2009, the North American Spine Society (NASS) released clinical guidelines based on the current body of evidence related to anti-thrombotic therapies in spine surgery; however, thus far, these have failed to capture input from a global perspective and have yet to be adopted worldwide. 12
Given the growing need for consensus surrounding recommendations regarding perioperative anticoagulation management in spine surgery, we conducted a global survey of spine surgeons within the AOSpine network to gauge their knowledge, attitudes and practices on this topic. Our preliminary findings have been reported by Louie et al. 22 With that serving as a foundation, the specific focus of this study was to identify factors that contribute to the decision making of the initiation of anticoagulation after spine surgery among a global group of spine surgeons. We hypothesized that the survey responses will show heterogeneity in anticoagulation start times, with few instances of consensus of important patient or surgical factors influencing initiation decisionmaking.
Methods
Survey Design
AOSpine Anticoagulation Global Survey methodology and overall findings are detailed in Louie et al. 22 In brief, a survey questionnaire was developed and included surgeon demographics, rationale for anticoagulation following spine surgery, risk stratification, the use of published/unpublished guidelines to guide treatment, and the use of multidisciplinary teams. This survey was distributed to the AOSpine membership that opted to receive such requests via email (n = 3805 members out of approximately 6000 members).
The specific focus section assessed respondent demographics and perioperative factors that affect the timing of anticoagulation prophylaxis based on medical comorbidities and previous episodes of thrombosis and/or embolus. Survey respondents were queried to grade the influence of various practice-specific (fellowship training, expert opinion, previous studies, unspecified guidelines) and perioperative specific considerations (length of procedure, number of operative levels, estimated blood loss [EBL], drain output, patient mobilization, body mass index [BMI]) when making decisions regarding anticoagulation initiation. Practitioners were asked to utilize a Likert-type scale to grade practice-specific factors on a scale from low (1) to high (5) importance, and patient-specific factors a scale from low (0) to high (3) importance. 23
Respondents were then asked to report their postoperative day of anticoagulation initiation in a series of hypothetical patient scenarios. Twenty-five possible scenarios were assessed and included patients who were either anticoagulation naive or currently being medicated with aspirin, warfarin, or another pharmacologic agent with or without a history of deep venous thrombosis (DVT), pulmonary embolism (PE), atrial fibrillation, coronary artery disease (CAD), placement of a cardiac valve, or placement of a cardiac stent. For scenarios where patients were taking pharmacologic anticoagulation, possible responses ranged from postoperative day 0 to beyond postoperative day 5. For patients not previously taking anticoagulant medication, possible responses ranged from postoperative day 0 to beyond postoperative day 7.
Statistical Analyses
All statistical analyses were performed with Stata version 13.1 (StataCorp LLC). Interpretation and categorization of all free-response survey answers were made by one independent reviewer to group similar categories for analyses. Calculation of percentages and means was made for count data and rank-order questions, respectively. Hypothetical patient scenarios were further stratified to evaluate timing of thromboprophylaxis for history of specific conditions and individual medications, with survey responses right censored to the final postoperative day response. Kaplan-Meier and log-rank test analysis was used to assess individual variables for importance in influencing timing to postoperative anticoagulation. All variables were then fitted to a series of Cox proportional hazards models to further evaluate the hazard ratio (HR) and associated P values and 95% confidence intervals (CIs) for each factor considered. Higher HRs corresponded to earlier initiation of anticoagulation. Model covariates included age, specialty, fellowship, years since completion of fellowship training, geographic region, practice type (academic, private, combined), annual practice case volume, and all queried practice-specific (fellowship training, expert opinion, previous studies, unspecified guidelines, other specialty involvement) and perioperative-specific considerations (procedure length, number of operative levels, EBL, drain output, patient mobilization, and patient BMI). Proportional hazards assumptions were met and validated using Schoenfeld residuals. The threshold for statistical significance for all tests was established at P < .05.
Results
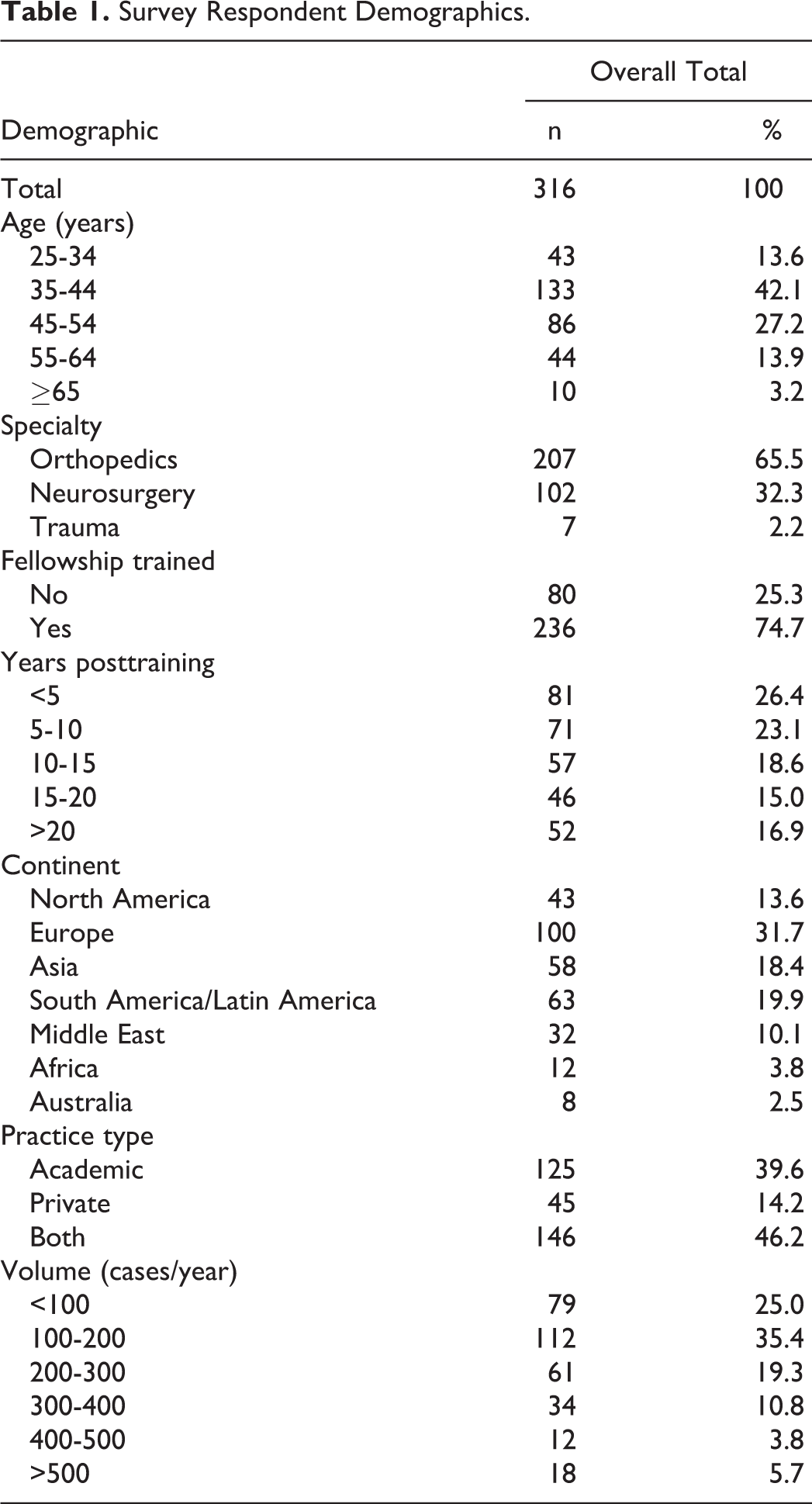
We have previously reported the initial findings from The AOSpine Anticoagulation Global Survey regarding the demographics of the respondents. 22 Briefly, 316 spine surgeons from 64 countries completed the survey (Table 1). When stratified by continent, Europe had the largest survey representation (31.7%), South America/Latin America (19.9%), and Asia (18.4%). Respondents were between the ages of 35 and 44 (42.1%) or 45 to 54 (27.2%) years, and were typically fellowship-trained (74.7%), and orthopedic surgeons (65.5%). Most were within 5 years (26.4%) or 5 to 10 years (23.1%) of completing their training, and practiced at academic (39.6%) or combined private/academic institutions (46.2%). The vast majority of respondents performed an estimated 101 to 200 cases per year (35.4%).
Survey Respondent Demographics.
Regarding general practice-specific factors considered during initiation of anticoagulation therapy, expert opinion was considered most important (mean grade ± SD = 3.2 ± 1.3), followed by fellowship training (mean grade: 3.2; SD ±1.3). Conversely, previous studies (mean grade: 2.7; SD ±1.2) and unspecified guidelines were considered least important (mean grade: 2.6; SD ±1.6). For patient-specific factors, most variables considered were graded with similar importance. Drain output (mean grade: 1.2; SD ±1.0) and number of operative levels (mean grade: 1.2; SD ±1.0) were considered least important, followed by EBL (mean grade: 1.2; SD ±1.0) and procedure length (mean grade: 1.3; SD ±1.1). Patient BMI (mean grade: 2.0; SD ±1.0) and postoperative mobilization (mean grade: 2.3; SD ±1.0) were deemed most important and graded highly overall. These results are further illustrated in Table 2.
Factors Ranked by Importance for Anticoagulation Initiation.
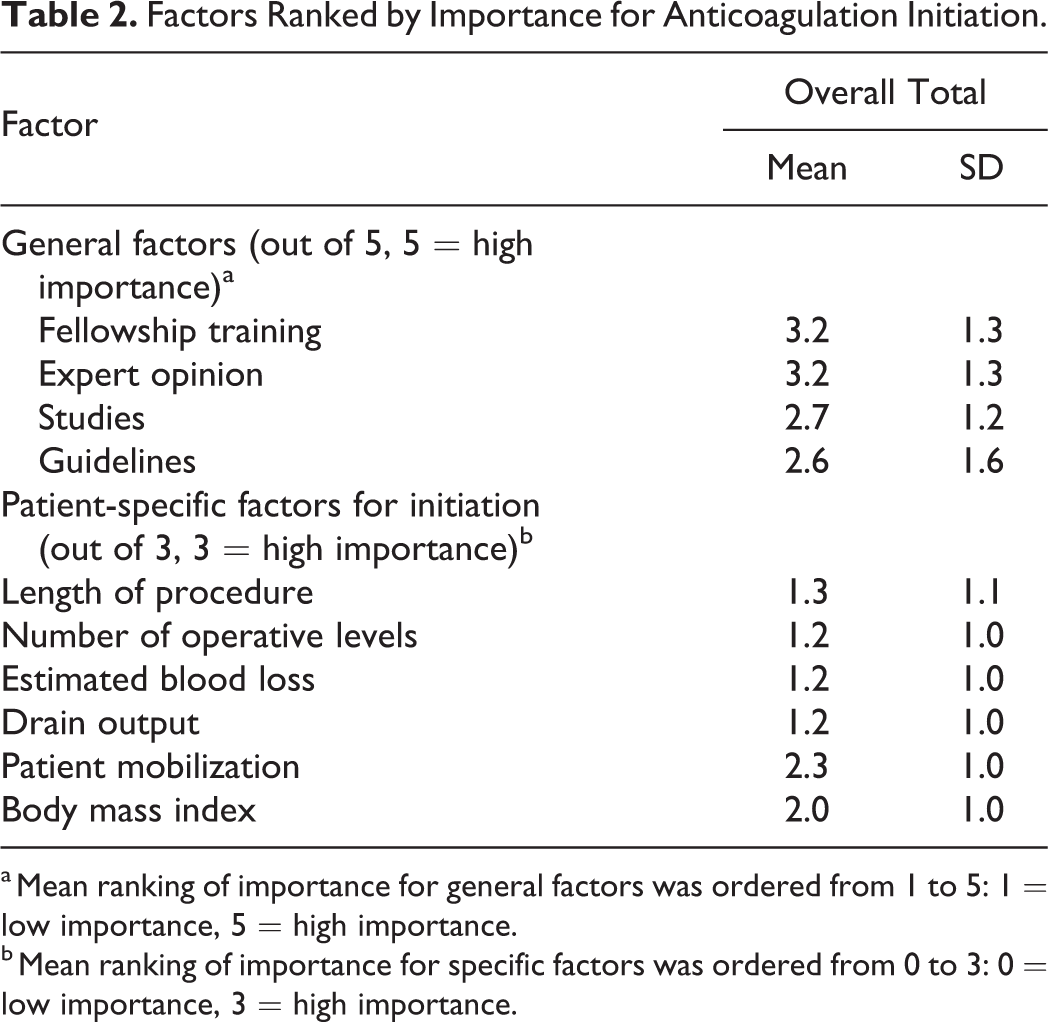
a Mean ranking of importance for general factors was ordered from 1 to 5: 1 = low importance, 5 = high importance.
b Mean ranking of importance for specific factors was ordered from 0 to 3: 0 = low importance, 3 = high importance.
When accounting for multiple factors using a Cox proportional hazards model approach, EBL and drain output were the only factors significantly associated with the provided scenarios that included both patient history (e.g. DVT, PE, CAD, etc) as well as previous anticoagulant use (e.g. warfarin, acetylsalicylic acid [ASA], or other agent) (Table 3). These variables demonstrated an inverse relationship with respect to anti-coagulation timing. Those who rated EBL with greater importance were likely to administer thromboprophylaxis at later times, and those who rated drain output with greater importance were likely to administer thromboprophylaxis at earlier times. This was particularly true in scenarios with patients with a history of DVT on warfarin (EBL: HR = 0.68, 95% CI = 0.49-0.93, P = .015; drain output: HR = 1.40, 95% CI = 1.05-1.87, P = .021), PE on ASA (EBL: HR = 0.69, 95% CI = 0.48-0.97, P = .035; drain output: HR = 1.43, 95% CI = 1.03-1.98, P = .033), or CAD on ASA (EBL: HR = 0.70, 95% CI = 0.50-0.96, P = .029; drain output: HR = 1.36, 95% CI = 1.02-1.81, P = .034), or another unspecified agent (EBL: HR = 0.71, 95% CI = 0.52-0.98, P = .035; drain output: HR = 1.32, 95% CI = 1.00-1.73, P = .049).
Cox Proportional Hazards Model for Perioperative Bridge Timing by Hypothetical Presentation Irrespective of Operative Location.a
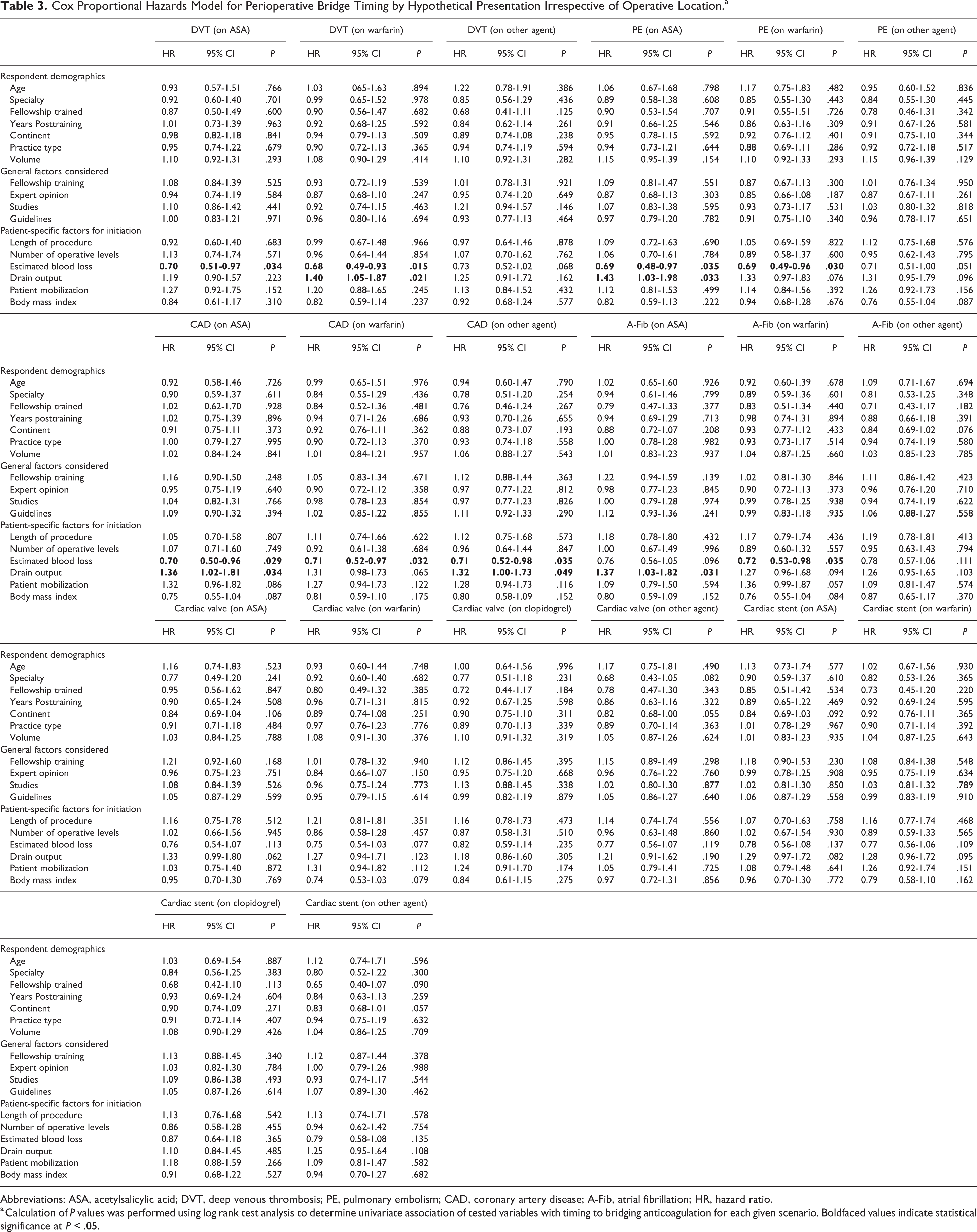
Abbreviations: ASA, acetylsalicylic acid; DVT, deep venous thrombosis; PE, pulmonary embolism; CAD, coronary artery disease; A-Fib, atrial fibrillation; HR, hazard ratio.
a Calculation of P values was performed using log rank test analysis to determine univariate association of tested variables with timing to bridging anticoagulation for each given scenario. Boldfaced values indicate statistical significance at P < .05.
These factors were also analyzed separately based on patient history (Table 4) or previous anticoagulant used (Table 5). In the setting of a history of DVT, EBL importance (HR = 0.71, 95% CI = 0.50-1.00, P < .050) was associated with shorter time to anticoagulation, while patient mobilization importance (HR = 1.40, 95% CI = 1.04-1.88, P = .029) was associated with longer time to anticoagulation. EBL was the only factor associated with an individual pharmacologic agent (previous warfarin use, HR = 0.71, 95% CI = 0.50-0.99, P = .046). Factors were also analyzed for scenarios where the patient was not previously on anticoagulation. In this analysis, no factors were significantly associated with the timing of anticoagulation (Table 6).
Cox Proportional Hazards Model for Perioperative Bridge Timing by Hypothetical Presentation Irrespective of Operative Location (Patient Previously on Pharmacologic Agent).a
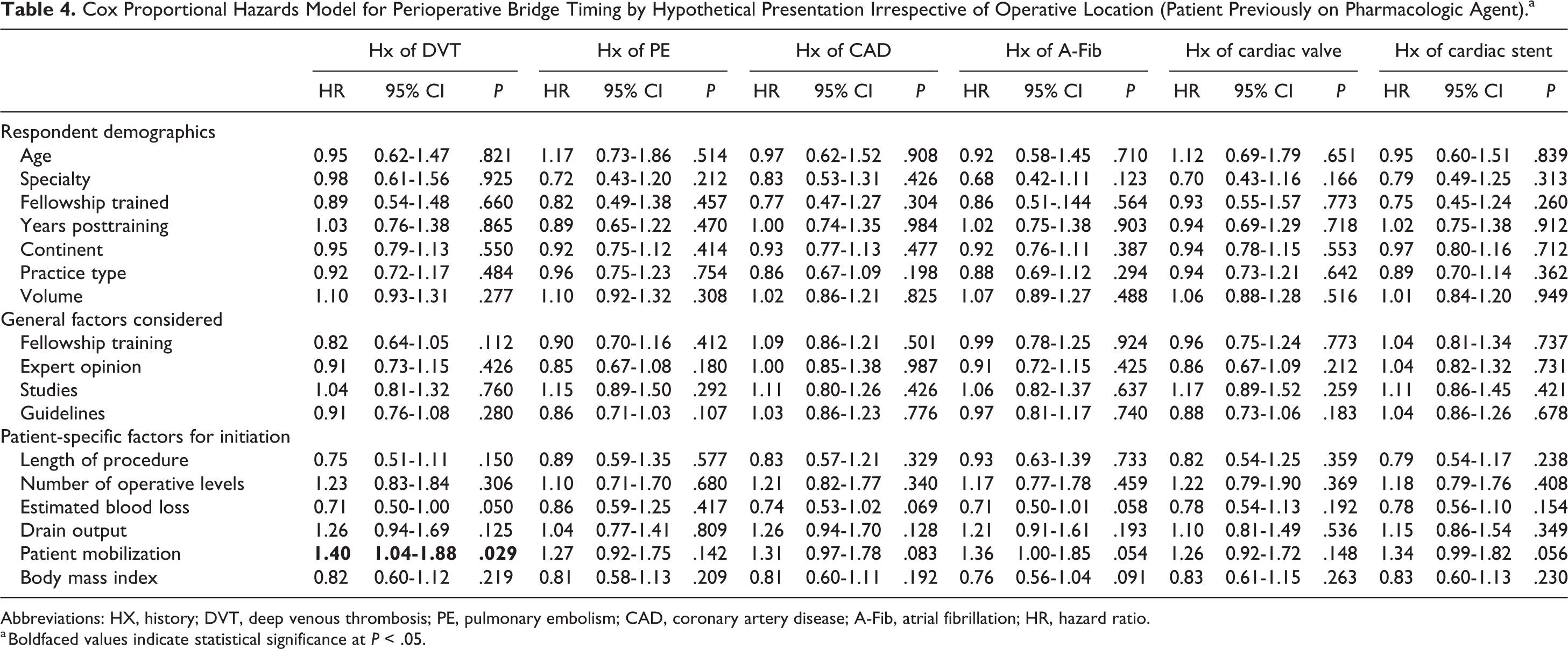
Abbreviations: HX, history; DVT, deep venous thrombosis; PE, pulmonary embolism; CAD, coronary artery disease; A-Fib, atrial fibrillation; HR, hazard ratio.
a Boldfaced values indicate statistical significance at P < .05.
Cox Proportional Hazards Model for Perioperative Bridge Timing by Pharmacologic Agent Irrespective of Operative Location (Patient Previously on Pharmacologic Agent).
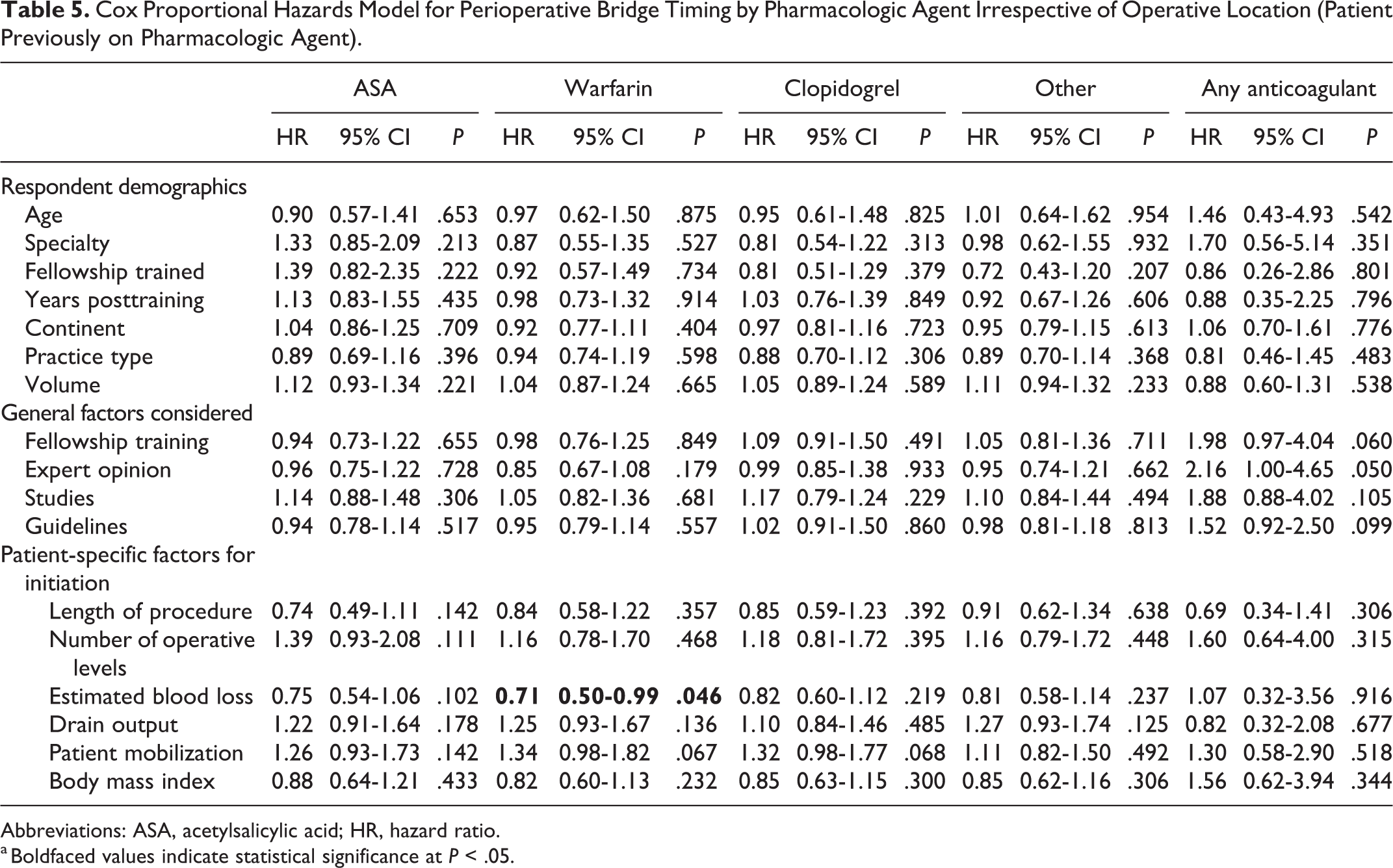
Abbreviations: ASA, acetylsalicylic acid; HR, hazard ratio.
a Boldfaced values indicate statistical significance at P < .05.
Cox Proportional Hazards Model for Perioperative Anticoagulation Irrespective of Operative Location (Patient Not Previously on Pharmacologic Agent).a
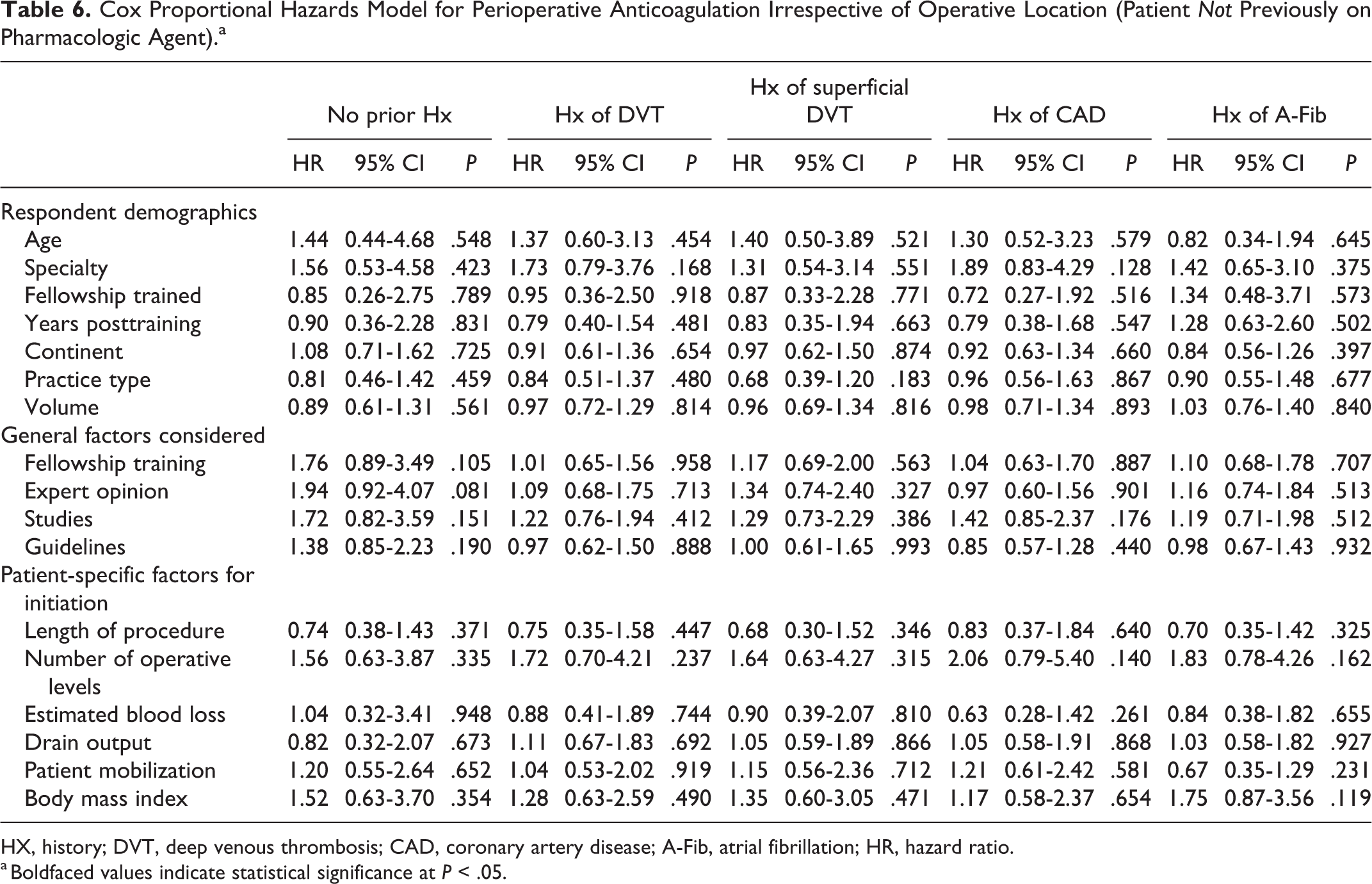
HX, history; DVT, deep venous thrombosis; CAD, coronary artery disease; A-Fib, atrial fibrillation; HR, hazard ratio.
a Boldfaced values indicate statistical significance at P < .05.
Discussion
Perioperative thromboprophylaxis usage and timing in spine surgery remains a controversial topic given the lack of consensus on optimal strategies. This area of perioperative management remains challenging for surgeons given the heterogeneity in patient populations as well as various indications for spine surgery. All strategies, unfortunately, weigh the risk of clinically significant VTE versus early postoperative. With no widespread acceptance, the timing of anticoagulation initiation in the perioperative period of spine surgery can remain challenging. To this end, we conducted the largest survey of spine experts worldwide, and have identified several factors in the decision making on the timing of initiation of perioperative anticoagulation. The following were noted to be relative among these spine experts: (1) patient mobilization and BMI are important “patient-specific” factors when deciding initiation of anticoagulation (without consideration of specific patient presentations); (2) expert opinion and fellowship training were the most substantial “practice-specific” factors, with formal guidelines and studies considered less important; (3) when accounting for multiple factors, opinions regarding the importance of EBL and drain output were associated with anticoagulation initiation timing in numerous patient scenarios involving both significant patient history (eg, DVT, PE, CAD, etc) as well as previous anticoagulant use (eg, warfarin, ASA, or other agent); and (4) opinions regarding the importance of EBL and patient mobilization were associated with anticoagulation timing in patients with a history of DVT.
The spine survey participants consensus was that their decisions concerning anticoagulation therapy were more heavily on expert opinion and fellowship training, rather than formal guidelines or literature, in directing them regarding timing of perioperative anti-coagulation. This highlights the lack of consensus on timing of anticoagulant initiation in spine surgery. Several survey studies have attempted to elucidate patterns regarding anticoagulant use in spine surgery, although these have been limited by geographic area, poor attention to timing regarding anticoagulation, and lack of discernable patterns driving decision making.18,19 In 2009, NASS released clinical guidelines regarding antithrombotic therapies in spine surgery. 12 Although these guidelines address the question of timing of anticoagulation in the perioperative period by cautioning surgeons to balance the risk of thromboembolic events with the risk of epidural bleeding and wound complications, they do not address the factors that should be considered, nor do they provide firm direction for decision making. Additionally, the lack of a global perspective in the NASS guidelines weaken their generalizability. In the preliminary findings from our survey data, Louie and colleagues 22 reported that only 14% of respondents described following hospital, national, or other unspecified guidelines when deciding on the use of anticoagulation. Despite this notion by our survey respondents, the AOSpine group has released thromboprophylaxis guidelines for patients suffering from spinal cord injury, which is the highest risk group for VTE in patients undergoing spine surgery.20,21 All in all, the existing literature, as well as our survey data recognizes the lack of reliable data, as well as a failure to widely disseminate existing guidelines.
When not involving patient scenarios specifically, our survey of surgeons found that patient mobilization and BMI are the most important patient-specific factors when considering anticoagulation initiation. These opinions may be reflective of the notion that patients who have high BMI or who may be slow to mobilize in the perioperative period may be at higher risk for VTE and may require earlier initiation of anticoagulation. Identification of these risk factors for VTE in the perioperative period has been shown in previously reported literature. Goz and associates 3 created a VTE risk index based on a review of 710 154 spinal fusions and included the presence of obesity as a significant factor in predicting VTE. Pannucci et al 24 reviewed a Michigan statewide surgical quality collaborative to identify predictors of 90-day VTE in postsurgical patients and found that among several other patient factors, BMI greater than 40 kg/m2 was associated with higher risk of VTE. McLynn and colleagues 25 confirmed these findings in their review of 109 609 patients from the National Surgical Quality Improvement Program (NSQIP) who underwent elective spine surgery, finding that increased BMI was a risk factor for VTE. Additionally, in a cohort of 1975 patients, Takahashi et al 26 reported a significantly lower symptomatic PE rate in patients who had early mobilization after spine surgery, compared to those patients who did not. To this end, the opinions expressed by the surgeons in our survey study are consistent with the current literature. Alternatively, some authors have linked VTE to length of procedure, number of levels, and intraoperative blood loss, although the respondents of our survey seemed to give less importance to these specific factors.25,27
In several patient scenarios, opinions regarding the importance of EBL and drain output were associated with the timing of anti-coagulation initiation in the perioperative periods. Increased intraoperative blood loss may alert the surgeon to an underlying or iatrogenic coagulopathy that may be exacerbated by the use of anticoagulants and/or antiplatelet medications. Awad et al 28 reviewed the records of 14 932 patients undergoing spine surgery and found that one of the risk factors for the development of postoperative spinal epidural hematoma included a high EBL (blood loss >1 L). Given this association with the development of postoperative spinal hematoma, our results show a prudent decision by spine experts to consider EBL of importance when determining when to begin anticoagulation. Similar to perioperative anti-coagulation management in spine surgery, closed suction drains represent another area of management where obvious consensus remains unestablished. Several authors have found no difference in symptomatic postoperative hematoma or wound complications after lumbar decompression and/or fusions with or without the use of closed suction drains.28-32 In fact, Chimenti and Molinari 33 reported that all four patients suffering from catastrophic epidural hematoma (ie, neurologic deficit to American Spinal Injury Association grade B or worse) in their series of 1750 patients had subfascial drains which failed to prevent this complication. Other authors have disputed that drains do not play an important role in preventing postoperative hematoma. Aono et al 34 reported the factors associated with the development of postoperative spinal epidural hematoma after surgery in their series of 6356 patients, finding that over half of the hematomas became symptomatic after closed suction drains were removed. They suggested that removal of such drains was the key trigger in a number of cases to allow the accumulation of hematoma to the point of neurologic deficit. Additionally, Kao and associates 35 found that drain output was significantly associated with the development of symptomatic epidural hematoma postoperatively (ie, patients with neurologic deficit were more likely to have lower drain output). Although our survey did not allow a detailed explanation as to the reasoning behind the association between anticoagulation timing and drain output among spine experts, this finding likely reflects the desire to use drain output to guide anticoagulation initiation at a point when epidural hematoma formation is unlikely. Literature is unclear at this point whether the opinion held by our respondents is a valid consideration in determining anticoagulation timing.
This study is strengthened by the inclusion of numerous patient scenarios that encompass the most common clinical dilemmas regarding anticoagulation facing spine surgeons. Although survey length limitations prevent an exhaustive list of clinical scenarios, pharmacologic options, and patient factors, the data is comprehensive enough to provide some insight into the decision making regarding anticoagulation initiation timing. Additionally, this study is the largest of its kind, with a global perspective that has not yet been described in the literature. This global perspective improves our findings’ generalizability, and provides promise that studies utilizing our data for follow-up explorations may be applicable to a wider population.
There are a number of limitations to our study. First, this is a survey study and limitations inherent to a study that does not include empiric data exists. Additionally, questions were not formatted in a way to allow the creation of specific guidelines. Rather, this data will be utilized to create focal points that may be useful in future follow-up survey studies, prospective, randomized studies or Delphi-esque consensus statements. In addition, survey distribution was limited to current spine surgeon members of the AOSpine network that opted-in to receive email notifications, and as such, there is still questionable generalizability despite our large sample size. Finally, the survey was sent out to 3805 spine surgeons worldwide with only 316 responses (8.3%). Although the response rate may appear low, perhaps we have captured respondents who take special interest in this topic and have placed greater thought to their anticoagulation practices. Other authors have found that a low response rate does not necessarily mean the study results have low validity, although there is a greater risk of this; therefore, low response rates should not be taken as an indicator of low validity. 36 Nonetheless, such a response rate is in line with other previous surveys circulated to a mass membership, such as AOSpine. Although these limitations exist, our work remains the largest, international survey to date focused on perioperative anticoagulation practices during spine surgery.
Conclusions
This AOSpine Anticoagulation Global Survey is the largest to date focusing on perioperative anticoagulation attitudes, practices, and beliefs among spine surgeons worldwide for VTE prophylaxis. The survey noted certain patient factors (ie, patient mobilization and BMI), certain practice-specific factors (ie, expert opinion and fellowship training), and certain surgical factors (ie, EBL and drain output) when faced with specific patient scenarios to be associated with decision making regarding anticoagulation timing in the perioperative period. Although certain areas of interest were identified in this survey study, we encountered significant heterogeneity in practices regarding decision making in timing of anticoagulation. Future studies will utilize these findings to develop more robust prospective studies to examine optimal anticoagulation timing in the perioperative period and create consensus guidelines that may more uniformly lead practice.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.