
Abstract
Study Design:
Technical report.
Objectives:
Dural tear is one of the most common complications of endoscopic spine surgery. Although endoscopic dural repair of the durotomy area may be difficult, we successfully repaired the dural tear area using nonpenetrating clips during biportal endoscopic surgery. We introduce the surgical technique of dural repair using nonpenetrating titanium clips in biportal endoscopic spine surgery and report its clinical outcome.
Methods:
We retrospectively reviewed and analyzed 5 patients who were treated via primary dural repair using nonpenetrating titanium clips during biportal endoscopic lumbar surgery. The 2 methods of dural clipping and repair include 2 or 3 portals. We analyzed radiological parameters such as cerebrospinal fluid collection as well as clinical parameters, including postoperative clinical outcomes.
Results:
Five patients underwent biportal endoscopic dural repair using nonpenetrating clips. Incidental durotomy was successfully repaired using nonpenetrating titanium clips in all 5 patients. No cerebrospinal fluid collection was detected in the postoperative magnetic resonance images. Clinically, preoperative symptoms improved significantly after surgery (P < .05).
Conclusions:
We repaired the dural tear area completely using nonpenetrating titanium vascular anastomosis clips in biportal endoscopic lumbar surgery. Dural repair via clipping method may be an effective alternative for incidental durotomy.
Introduction
Incidental durotomy is one of the common complications occurring during spine surgery.1-4 Cerebrospinal fluid (CSF) leakage induces headache, nausea, intracranial hypotension, intracranial hemorrhage and pseudo-meningocele. 3 Moreover, CSF leak from durotomy leads to wound infection, meningitis, and neurologic deficit.3,4 Endoscopic spine surgeries conducted using continuous irrigation affect spinal epidural pressure as well as intracranial pressure. Direct inflow of irrigation saline fluid into the intradural area may increase intracranial pressure. 5 Increased intracranial pressure triggers headache, neck pain, and seizure. Therefore, complete dural repair is important for prevention of complications caused by CSF leakage and intradural inflow of irrigation saline. Although incidental durotomy in conventional open surgery can be completely repaired by primary suture, sealing materials and glue materials, dural repair during spinal endoscopy may be difficult due to the limitations and difficulty associated with the handling of instruments and sealant materials.4,6
Direct primary dural suture may be impossible in approaches via uniportal endoscopy of spine. Surgical glue cannot be applied due to continuous saline irrigation in endoscopic surgery. Therefore, endoscopic spine surgery may need to be converted to open microsurgery for the repair of dura tear site.
Recently, biportal endoscopic spine surgery has increased in popularity in spine surgery.7-9 Since the working portal of biportal endoscopic spine surgery was derived separately from the endoscopic portal (Figure 1), instrumental handling may be relatively easier than in uniportal endoscopic surgery. Incidental dural injury is also one of the complications associated with biportal endoscopic approaches. 5 We successfully performed direct dural repair of incidental durotomy area using non-penetrating clips during biportal endoscopic surgery (Figure 1). The purpose of this study is to present a surgical technique of dural repair for incidental durotomy using non-penetrating titanium anastomosis vascular clips during biportal endoscopic spine surgery and report its clinical results.
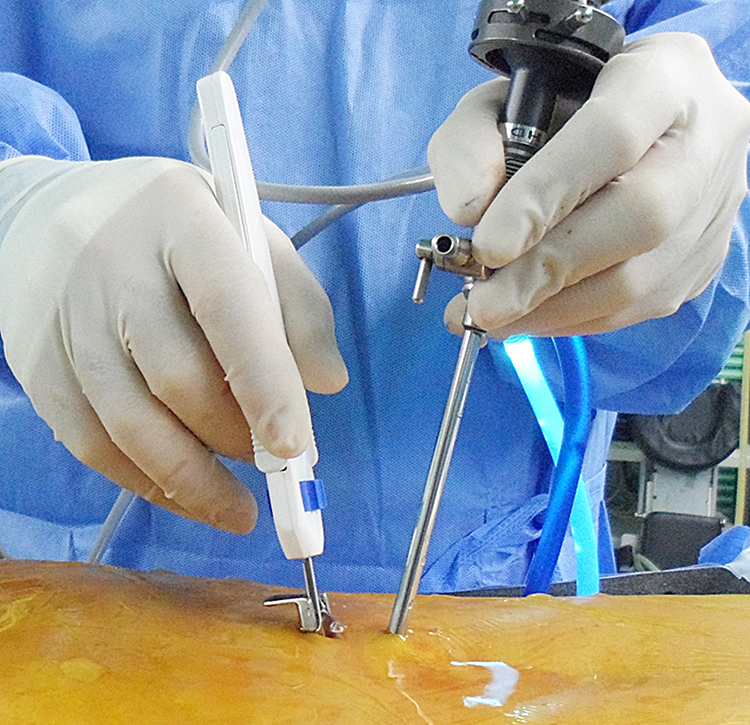
Overview of biportal endoscopic lumbar surgery. Nonpenetrating titanium clip instrument is inserted through working portal.
Materials and Methods
We retrospectively reviewed and analyzed 5 patients who were treated via primary dura repair using nonpenetrating titanium clips during biportal endoscopic lumbar surgery (Figure 1 and Table 1). All 5 patients received endoscopic lumbar surgeries for lumbar disc herniation or lumbar central stenosis via biportal endoscopic approaches with continuous saline irrigation. Incidental durotomy occurred during biportal endoscopy in the 5 patients. We used nonpenetrating titanium clips (Anasto-Clip Vessel Closure System, LeMaitre Vascular, Inc) for dural repair (Figure 2). This investigation was performed in accordance with our institutional guidelines, which comply with international laws and policies (institutional review board of Seoul Bumin Hospital).
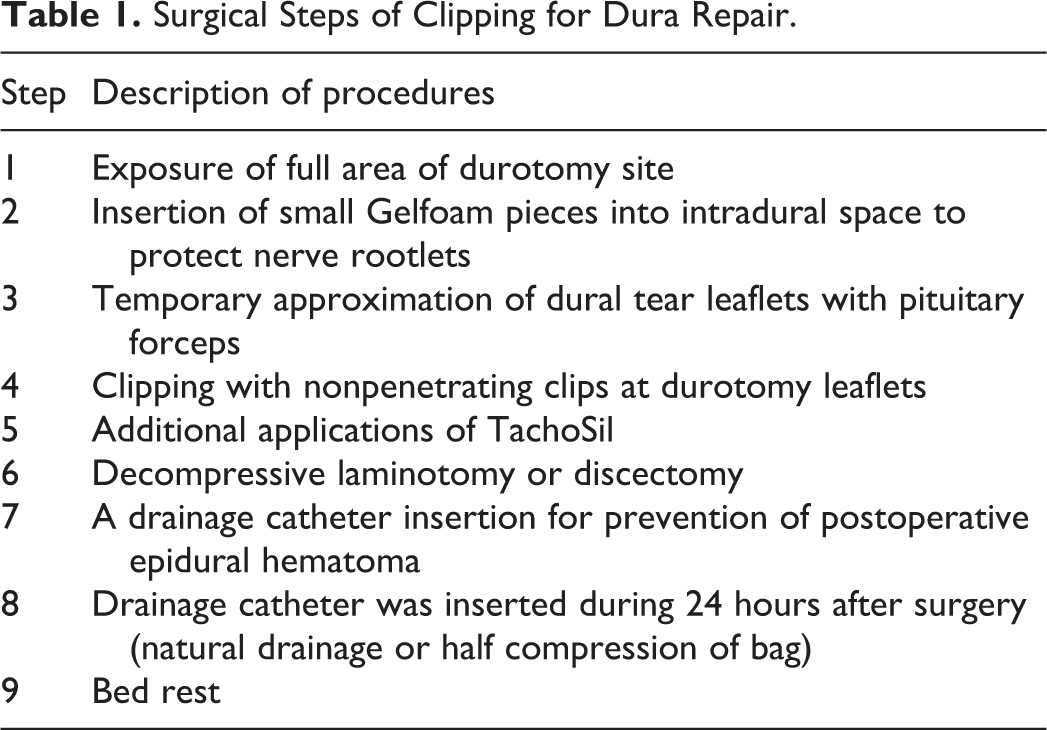
Surgical Steps of Clipping for Dura Repair.
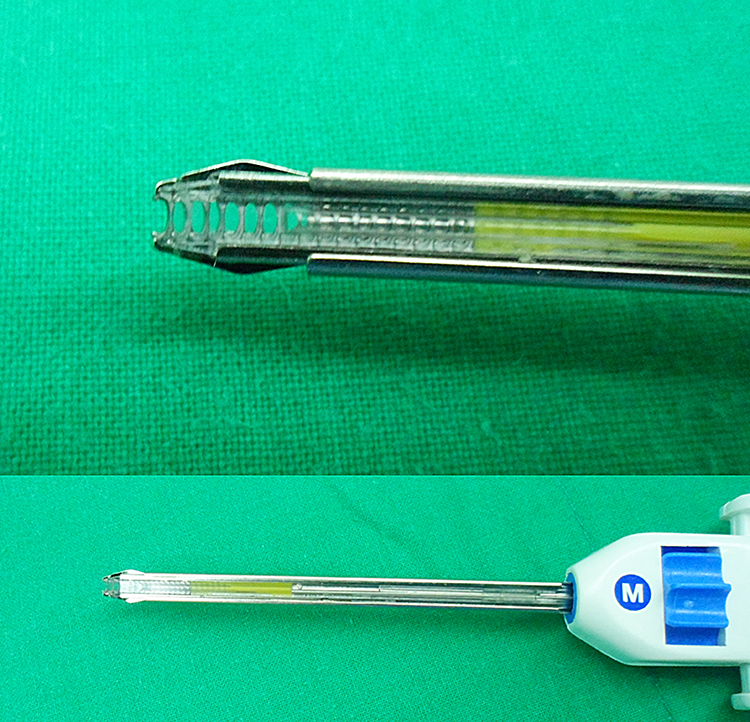
Images of nonpenetrating titanium vascular anastomotic clip system.
Surgical Technique of Dural Repair Using Clips (Table 1, Videos 1 and 2)
Two methods of dural clipping were used for dural repair: (1) 2-portal method (Figure 3 and Video 1) and (2) 3-portal method (Figure 4 and Video 2). The 2-portal methods used previously entailed creation of 2 channels for surgery. The 3-portal methods made use of an additional third portal for approximation of dura tear leaflets (Video 2).
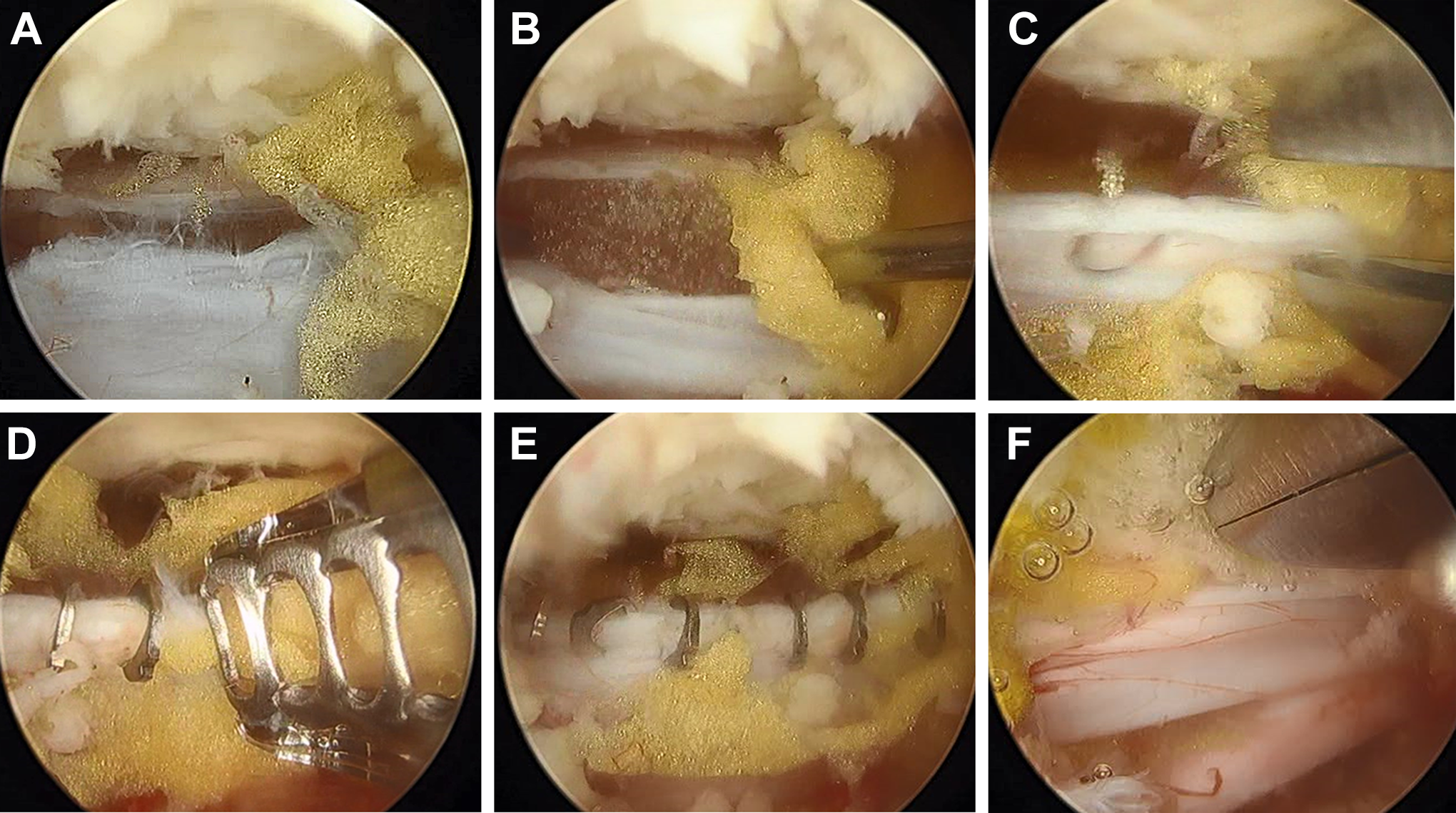
Steps in the serial clipping operation for dural repair via 2-portal method. (1) Full exposure of dura tear area (A). (2) Insertion of Gelfoam pieces to protect nerve rootlets (B). (3) Temporary approximation of dural tear leaflets using pituitary forceps (C). (4) Clipping in the durotomy area (D). (5) Final view of complete dural clipping (E). (6) Application of TachoSil pieces over the clipping area (F).
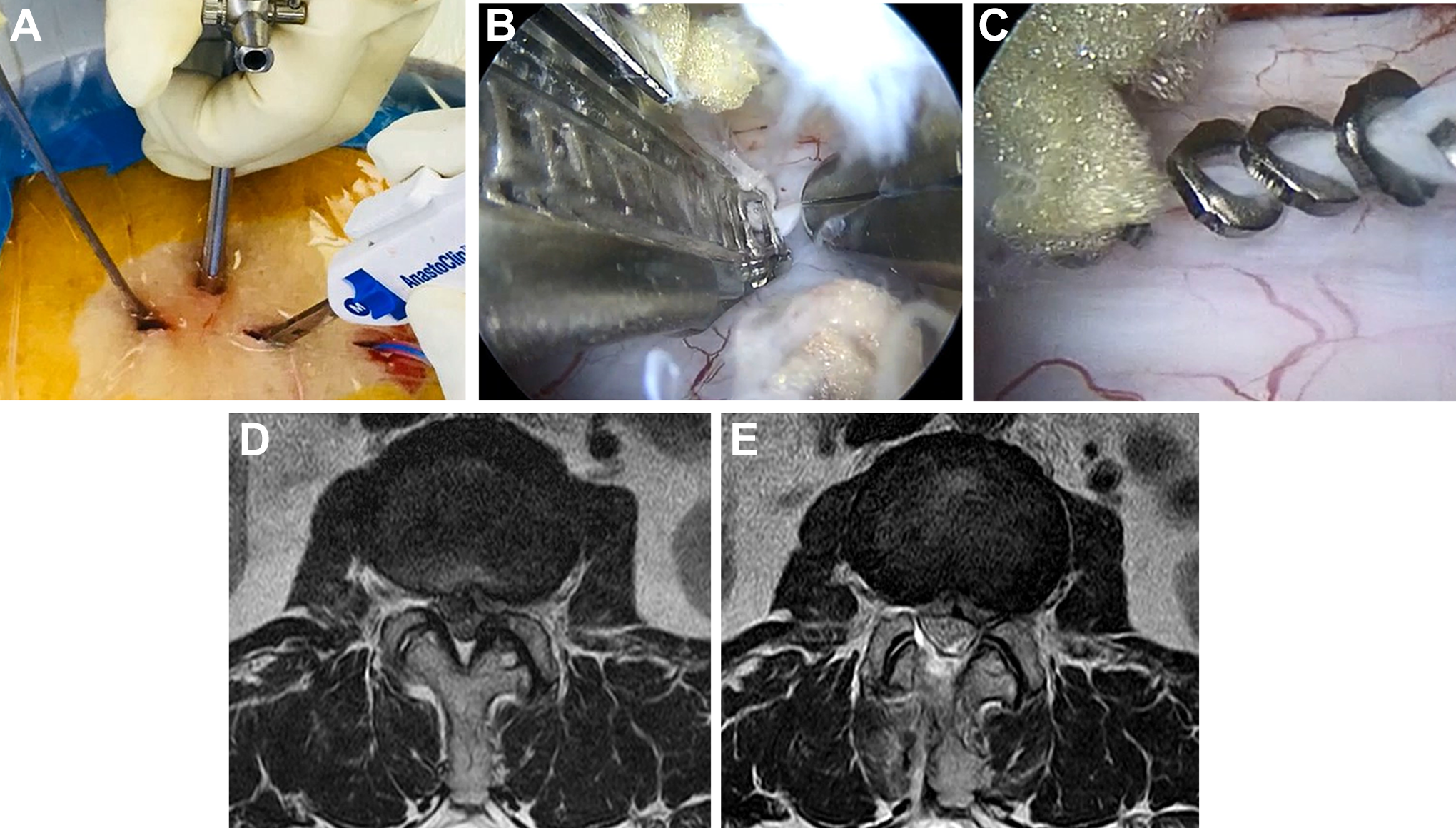
A 70-year-old female patient undergoing biportal endoscopic discectomy for lumbar stenosis and ruptured disc herniation of L2-3. Incidental durotomy was treated via 3-portal method (A). Durotomy area was completely repaired by clipping with pituitary assistance (B and C). Preoperative magnetic resonance imaging showed ruptured disc herniation with central stenosis of L2-3 (D). Postoperatively, the dura was well decompressed and the cerebrospinal fluid was not collected (E).
First, the durotomy area should be fully exposed from the proximal to the distal dura tear margin (Figure 3A). Epidural fat tissue is removed for clear exposure of dural tear margin. In the presence of extradural herniation of nerve rootlets in the dural tear area, we applied herniated nerve rootlets intradurally using dissectors. One or 2 pieces of Gelfoam (Pfizer) were inserted to protect the nerve rootlets via dural tear area (Figure 3B). A temporary approximation of dural tear leaflets was performed using a pituitary forceps (Figure 3C). Nonpenetrating clips were used with a gap of 1 to 2 mm (Figure 3D and E). We usually used medium-sized clips. After dural clipping, TachoSil was applied over the clipping area (Figure 3F).
In the event of failure of temporary approximation of durotomy leaflets, we considered an additional third portal as a second working portal (Figure 4A). With the help of an assistant who held the endoscope, an operator performed dural repair using 2 hands. The first hand was used to manipulate pituitary forceps for approximation of the dural tear area, and the other hand was used to apply clips (Figure 4B and C). We inserted a drainage catheter to prevent postoperative hematoma. Pressure of the drainage bag was less than half the compression of a bag. A drainage catheter was usually removed on day 1 after surgery. Finally, we recommended bed rest ranging from 3 to 5 days after surgery.
Analysis of Parameters
Postoperative magnetic resonance imaging (MRI) was performed at least 3 days after surgery in all five patients (Figures 4 and 5). We investigated the presence of postoperative CSF collection or pseudo-meningocele via postoperative MRI. Implants of metal artifacts by clips were evaluated via postoperative MRI.
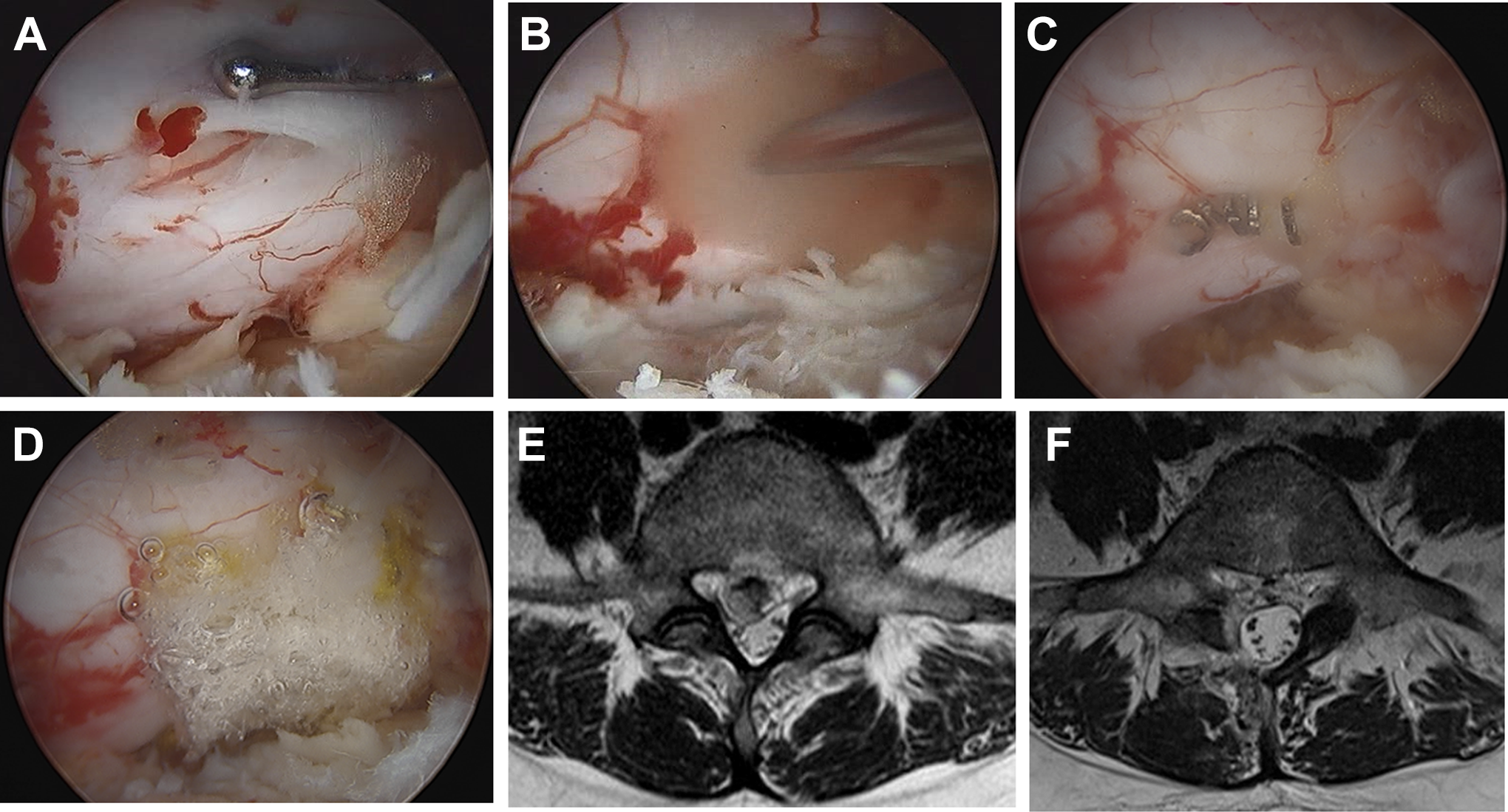
A 31-year-old female patient with disc herniation of L4-5 was treated via biportal endoscopic discectomy. Dural tear occurred during surgery (A). A Gelfoam piece was inserted for nerve protection (B). The durotomy site was repaired by clipping (C). A TachoSil piece was additionally applied over the clipping area (D). Preoperative magnetic resonance imaging showed ruptured disc herniation at L4-5 (E). After surgery, ruptured disc particles were completely removed and no fluid collection was detected (F).
Postoperative clinical results were assessed using a visual analogue scale (VAS) of back and leg and the modified Macnab scale. Also, clinical parameters including age, gender, diagnosis, follow-up periods, and the amount of postoperative drainage were analyzed.
We used Wilcoxon signed-rank test, and, a P value <.05 was considered to be statistically significant. We used R 3.1.2 for Windows for statistical analysis.
Illustrative Cases
Case 1
A 66-year-old female patient presented with right leg pain. Incidental dural tear occurred during the biportal endoscopic discectomy of L5-S1. Dura was repaired with nonpenetrating titanium clips using 2 portals (Figure 3 and Video 1).
Case 2
A 70-year-old female patient received decompressive laminotomy via discectomy due to lateral recess stenosis with ruptured disc herniation of L2-3 (Figure 4). Dura was torn in the dorsal area during removal of the ligamentum flavum. A third portal was made for assistance of dural approximation during clipping. Dura was repaired by clipping (Video 2). Postoperative MRI depicted full decompression of the L2-3 area, and no CSF collection in the laminotomy area.
Case 3
A 31-year-old female patient suffered from herniated disc of L4-5 on the right side. She underwent biportal endoscopic laminotomy with discectomy on the right L4-5. Incidental durotomy occurred in the shoulder dura area (Figure 5). Dura was completely repaired with nonpenetrating clips (Figure 5).
Results
The 5 female patients (mean age 60.2 ± 14.5 years, Table 2) underwent biportal endoscopic lumbar laminotomy or discectomy for lumbar degenerative disease. Incidental durotomy was successfully repaired using nonpenetrating titanium clips.
Diagnosis and Surgical Procedures of the 5 Enrolled Patients.

The mean VAS in the back decreased significantly from 8.6 ± 1.1 to 2.8 ± 0.8 and the mean VAS of leg also significantly decreased postoperatively from 9. ± 0 0.7 to 1.8 ± 0.8. The CSF was not drained after surgery, and the mean amount of drainage fluid including blood through drainage catheter was 26.2 ± 9.9 mL. The mean follow-up period was 12.2 ± 3.9 months. Wound problems related to CSF leak were not detected until the last visit.
The postoperative MRI images did not show CSF collection. No metal artifact of nonpenetrating titanium clips was detected in postoperative MRI. The patient scored excellent grade under 2 and good under 3 of the modified Macnab criteria.
Discussion
Although dural tear is one of the common complications associated with spine surgeries, incidental durotomy induced mortality and morbidity after spine surgery.3,10 Serious complications such as intracranial hypotension, neurological deficit and infection occurred after dural tear.3,10,11 Incidental durotomy occurred during uniportal as well as biportal endoscopic spine surgeries, which generally used continuous irrigation of saline fluid to ensure clear view and bleeding control during the surgery. 1 Intradural inflow of irrigation fluid through the durotomy site may increase intracranial pressure, and result in headache, neck pain and seizures. Therefore, dural tear should be repaired before proceeding with endoscopic procedures during spine surgery. Occasionally, endoscopic spine surgery may need to be converted to open microscopic surgery for primary dural repair.5,12
Sutureless nonpenetrating titanium vascular anastomosis clips already use dural repair in open surgery, including minimally invasive spine surgery. 2 This clip application device is available in biportal endoscopic surgery. Compared with uniportal endoscopic surgery, techniques for biportal endoscopic spine use instruments for general spine operation as well as specialized endoscopic instruments. The clip application device can be inserted and used via working portal.
We suggest that temporary approximation of dura tear leaflets using pituitary forceps is important for successful dural clipping. However, if temporary approximation failed, we considered an additional third portal for another working channel. An assistant held the endoscope, and an operator used 2 hands via the 2 working portals. A single hand was used to hold the pituitary forceps for approximation of dural tear leaflets, and another hand was used to manipulate the clip application device.
Small durotomy may be repaired by TachoSil. Previous studies reported good results of dura repair using TachoSil during uniportal endoscopic spine surgery.1,4 TachoSil application may be another treatment option for sealing of small dural injury.
Since the nonpenetrating clip system is too short for use in single-portal endoscopic surgery, the clip system cannot be used in uniportal endoscopic surgery. If uniportal endoscopic surgeries are adapted to biportal endoscopic spine by creating another working portal, the clipping systems are available for dural repair.
If endoscopic dural repair using clips or sealant materials failed, or large dural defects prevailed, we strongly recommend conversion to open microscopic surgery for dural suture. Since prolonged endoscopic surgery may increase the intracranial pressure due to influx of irrigation fluid, the possibility of serious complications, including seizures and incomplete dural repair, is increased. Since handling of clipping instrument may be relatively difficult compared with open microscopic approach, we strongly recommend a switch to open surgery during the learning curve of biportal endoscopic surgery
If CSF drainage through the drainage catheter is suspected after endoscopic dural repair, we recommend removal of the drainage catheter and bed rest for 5 days. 4 Insertion of lumbar CSF drainage catheter should be considered.
Laparoscopic or arthroscopic surgeries employ various types of suture or approximation instruments rather than spinal endoscopic surgery. They include instruments for bowel suture, bowel anastomosis, and vascular clips in laparoscopic surgeries. Joint arthroscopic approaches adopt instruments for endoscopic ligament suture. However, spinal endoscopic systems do not utilize any suture instruments for dural and annulus suture. We suggest that instruments for endoscopic suture should be developed in uniportal and biportal endoscopic spine approaches.
Nonpenetrating titanium clips may not injure nerve rootlets. Nonpenetrating clips should be small, round, and different from ordinary vascular penetrating clips. Both proximal ends of the clips are approximated, when the clips are applied. Therefore, these clips rarely affect the nerve during dural repair. Although nonpenetrating clips may be associated with a minor risk of neural injury, we applied minor pieces of Gelfoam (Pfizer) into the durotomy area to protect the nerve rootlets (Figures 3 and 5).
Non-penetrating titanium clips did not show metal artifacts during MRI (Figures. 4 and 5). Postoperative MR images were obtained after clipping. The metal artifacts of clips were also locked.
Conclusions
Incidental durotomy is a complication of endoscopic spine surgery. In the biportal endoscopic surgery, we repaired the dural tear area completely using non-penetrating, titanium vascular anastomotic clips, without conversion from a biportal endoscopic approach to open microsurgery. Clipping method may be an effective alternative method of dura repair for incidental durotomy.
Footnotes
Acknowledgment
*Dong Hwa Heo and Ji Soo Ha are co–first authors and the contributed equally to the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.