
Abstract
Study Design:
Retrospective cohort study.
Objectives:
Nonunion after posterior lumbar interbody fusion (PLIF) is associated with poor improvements in health-related quality of life (HRQOL). We aimed to investigate the influence of early osseous union after PLIF on HRQOL.
Methods:
We reviewed 138 patients with 1-level PLIF (mean age 67 years, follow-up period ≥1 year). Postoperative lumbar computed tomography was performed to assess screw loosening and intervertebral union. HRQOL was assessed using the Japanese Orthopaedic Association Back Pain Evaluation Questionnaire.
Results:
Thirty-nine patients (28%) showed complete union at 6 months postoperatively (early union group). Twenty-eight patients (20%) showed complete union at 6 to 12 months postoperatively (delayed union group), while 71 patients demonstrated noncomplete union. Effective improvement of lumbar spine dysfunction and psychological disorders was achieved in 19 (63.3%) and 17 (50.0%) patients in the early union group, in 9 (42.9%) and 14 (53.8%) patients in the delayed union group, and in 22 (34.9%) and 19 (29.2%) patients in the nonunion group, respectively (P = .036 and P = .036, respectively). The nonunion group had a significantly higher proportion of cases with screw loosening at 6 and 12 months postoperatively than the complete union group (P = .033 and P = .022).
Conclusions:
Lumbar spine dysfunction and psychological disorders improved in cases with early complete union compared to those with nonunion. Screw loosening occurred in cases with nonunion predominantly from 6 months postoperatively. Therefore, the achievement of early complete union might be helpful for better HRQOL and lower incidence of postoperative complications.
Keywords
Introduction
The number of surgeries for lumbar degenerative diseases have increased. 1 Posterior lumbar interbody fusion (PLIF) is a common surgery to treat lumbar degenerative diseases and provides better physiological alignment in the spine. 2 Nevertheless, complete fusion can depend on the quality and quantity of bone. 3 Thus, postoperative complications related to poor bone quality, such as pseudoarthrosis and instrumentation failure, including cage subsidence or screw loosening, are known to occur. 4
Recent trends in patient evaluation have resulted in the growing use of patient-based outcome measures to assess health-related quality of life (HRQOL). Most studies showed that lumbar arthrodesis surgery improves HRQOL outcomes.1,5 However, delayed union or pseudoarthrosis after PLIF is associated with poor outcomes in HRQOL.6,7 Therefore, an early complete union must be achieved for a successful clinical outcome after PLIF.
In our first report using a multicenter, randomized, open-label, and parallel-group trial, the titanium-coated polyetheretherketone (PEEK) cage maintained better bone fusion with the endplate than the PEEK cage 6 months after PLIF; however, there was no difference in clinical outcomes related to HRQOL. 8 Therefore, we analyzed this discrepancy in our second report. We hypothesized that early intervertebral osseous union could improve HRQOL, and the present study aimed to retrospectively investigate the influence of early intervertebral osseous union after PLIF on HRQOL.
Materials and Methods
Institutional Review Board Approval
This multicenter randomized controlled trial was approved by the institutional review boards (research approval no. 15-276) and registered with the University Hospital Medical Information Network (UMIN) clinical trials registry (UMIN000022618).
Participants
The data obtained in the aforementioned randomized trial was analyzed retrospectively. We analyzed 138 patients who underwent single-level PLIF or transforaminal lumbar interbody fusion (TLIF) for degenerative spondylolisthesis, degenerative scoliosis, lumbar spinal canal stenosis, lumbar radiculopathy, lumbar herniation, or isthmic spondylolisthesis at 3 university hospitals and their affiliated hospitals between 2016 and 2018 (Figure 1). The inclusion criteria were age ≥20 years with lumbar degenerative disease and provision of informed consent for study participation. Patients with histories of radiation treatment to the lumbar spine, bone tumors, metabolic bone disease, or previous back surgeries were excluded. Patients were randomly allocated treatment with either a titanium-coated PEEK cage or PEEK cage by open-label trial (64 and 74 patients, respectively). Postoperatively, all patients wore a lumbar soft corset for at least 3 months and underwent standardized physical therapy, including exercises for strengthening the back muscles and walking. All the patients were followed up for at least 1 year. Most patients had complete datasets, which were sufficient for analysis.
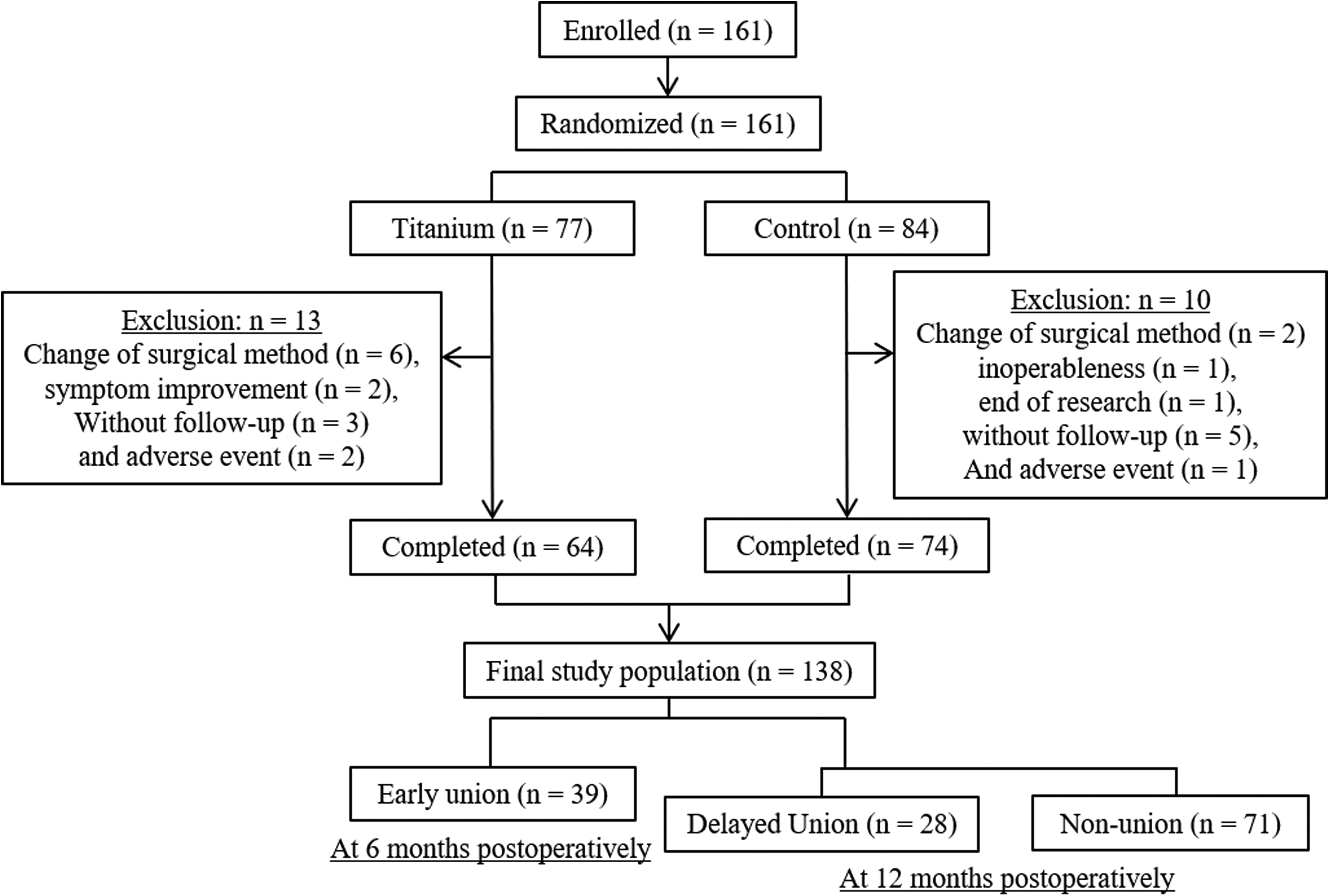
Study design.
Radiographic, Clinical, Osteoporotic Evaluation, and Grouping
Patient characteristics and surgical data, which included the type of surgery and surgical level, were obtained by reviewing medical records. Lumbar instability was assessed by angular motion on flexion-extension radiographs. Intervertebral osseous union was independently assessed by four blinded physicians using dynamic radiography and 3-dimensional (3D) computed tomography (CT) scans at 6 and 12 months postoperatively, with the grading of fusion based on the system of Bridwell et al. 9 Bone formation was graded into 3 categories: grade I, bridging bone bonding with both adjacent vertebral bodies; grade II, bridging bone bonding with either superior or inferior vertebral body; or grade III, incomplete bony bridging. Two CT slices, the center slices of the cage in both coronal and sagittal views, were used to evaluate osseous fusion. We defined complete intervertebral osseous union as an angular motion of <5° at the fusion level and the presence of upper and lower complete fusions, whereby both coronal and sagittal CT slices in the center cage region were evaluated as grade I, and each was given a score of 1 (for a total score of 2; Figure 2) based on previous studies.10,11 Incomplete intervertebral osseous union was given total scores of 3 to 6. Screw loosening was defined as the presence of the “halo sign” around the pedicle screws. Cage subsidence was defined as sinking of the cage when compared with its position immediately after surgery. Screw loosening and cage subsidence were also evaluated using CT scans at 1, 2, 4, 6, and 12 months postoperatively. Femoral neck bone mineral density (BMD) was measured using dual X-ray absorptiometry, preoperatively. Whole spine standing radiographic measurements were obtained at preoperatively, 2, and 12 months postoperatively. The following spinal parameters were assessed: thoracic kyphosis (T4 and T12); lumbar lordosis; sagittal vertical axis; pelvic tilt; sacral slope; pelvic incidence; and Cobb angle. Patients were classified into two groups: union group, including patients who achieved complete intervertebral osseous union (bone fusion score = 2; Figure 2) after PLIF or TLIF, and nonosseous union group, including patients who did not achieve complete intervertebral osseous union. Furthermore, patients with complete union at 6 months were placed in the early union group, and among the other patients, those with complete union at 12 months were placed in the delayed union group, and others in the non-union group (Figure 1).
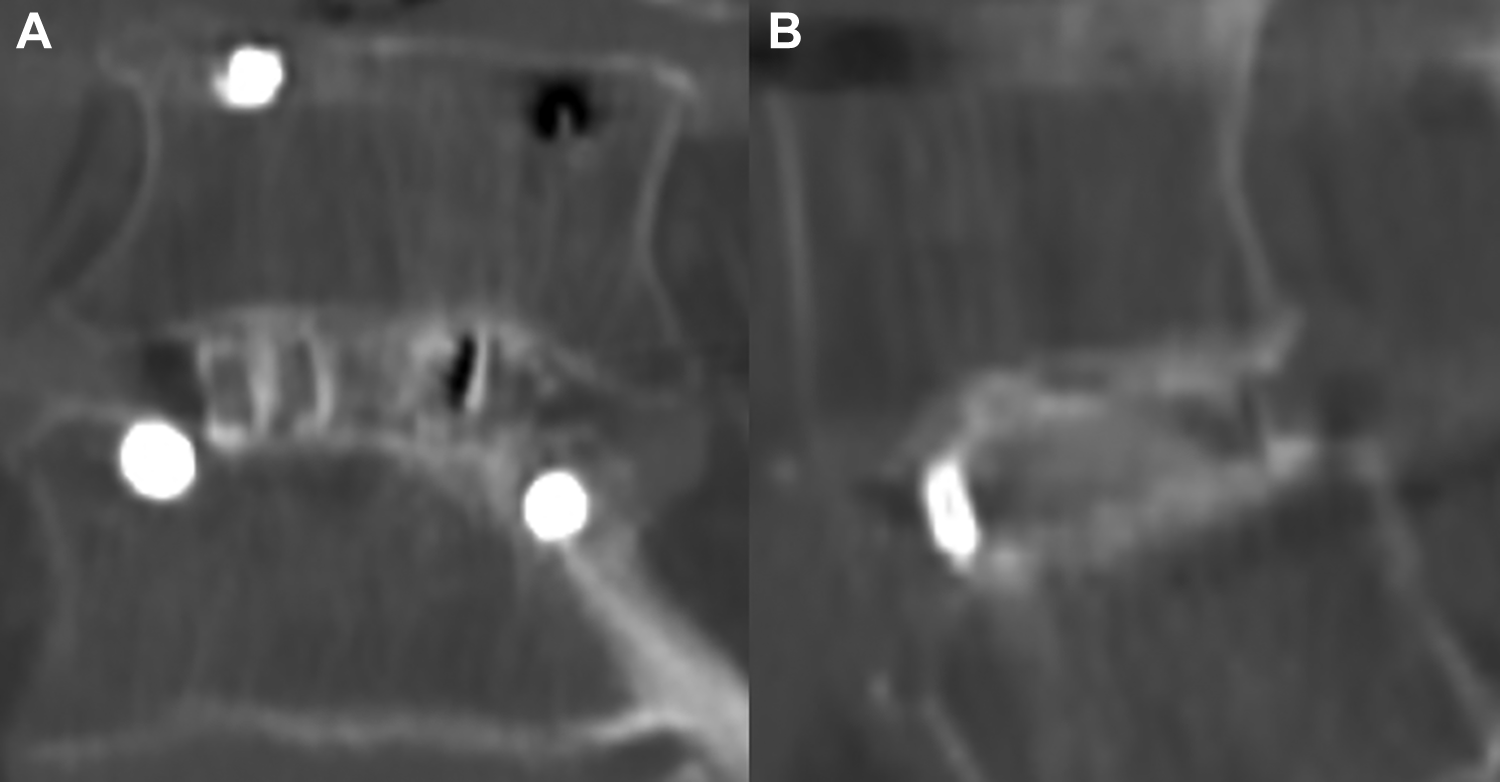
A case with complete osseous union. Both coronal (A) and sagittal (B) computed tomography slices in the center cage region were evaluated as grade I, and each was given a score of 1 (for a total score of 2).
Assessment of HRQOL
Clinical and neurological symptoms were assessed preoperatively, 6, and 12 months postoperatively using the Japanese Orthopaedic Association Back Pain Evaluation Questionnaire (JOABPEQ), 12 composed of parameters (pain-related disorders, lumbar spine dysfunction, gait disturbance, social life dysfunction, and psychological disorders) scored from 0 to 100 points (a higher score indicated a better condition), and the Oswestry Disability Index (ODI). 13 QOL scores for the 5 categories in the JOABPEQ, preoperatively, 6 and 12 months postoperatively, were calculated for each patient. According to the user’s guide for the JOABPEQ, 12 an increase of 20 points or more in the improvement score (the difference between the preoperative and postoperative scores) was determined to indicate “effective” treatment.
Statistical Analysis
Categorical variables are expressed as absolute numbers and percentages and were analyzed by chi-square test or Fisher’s exact test, as appropriate. Shapiro-Wilk tests were used to determine whether continuous variables were normally or nonnormally distributed. Continuous variables with normal distributions expressed as means ± standard deviations were analyzed with unpaired t tests, whereas nonnormally distributed data are expressed as median and interquartile range (IQR) and was analyzed with the Mann-Whitney U test. One-way analysis of variance followed by the Tukey post hoc test and chi-square test were used to detect differences between the groups. Statistical analyses were conducted with SPSS version 23.0 (IBM Corp). P values <.05 were considered significant.
Results
Union Versus Nonunion Groups
Sixty-seven patients (48.6%; union group) showed complete union (bone fusion score = 2) after PLIF, while 71 patients (nonunion group) did not achieve complete union (Figure 1). The non-union group had 17 patients with a bone fusion score = 3, 23 patients with score = 4, 15 patients with score = 5, and 16 patients with score = 6. Both groups did not differ in age, presence of hypertension or diabetes mellitus, type of surgical treatment, surgical level, usage of titanium-coated PEEK cage, and femoral BMD (Table 1).
Comparison of Baseline, Surgical, and Osteoporotic Data Between the Union and Nonunion Groups.a
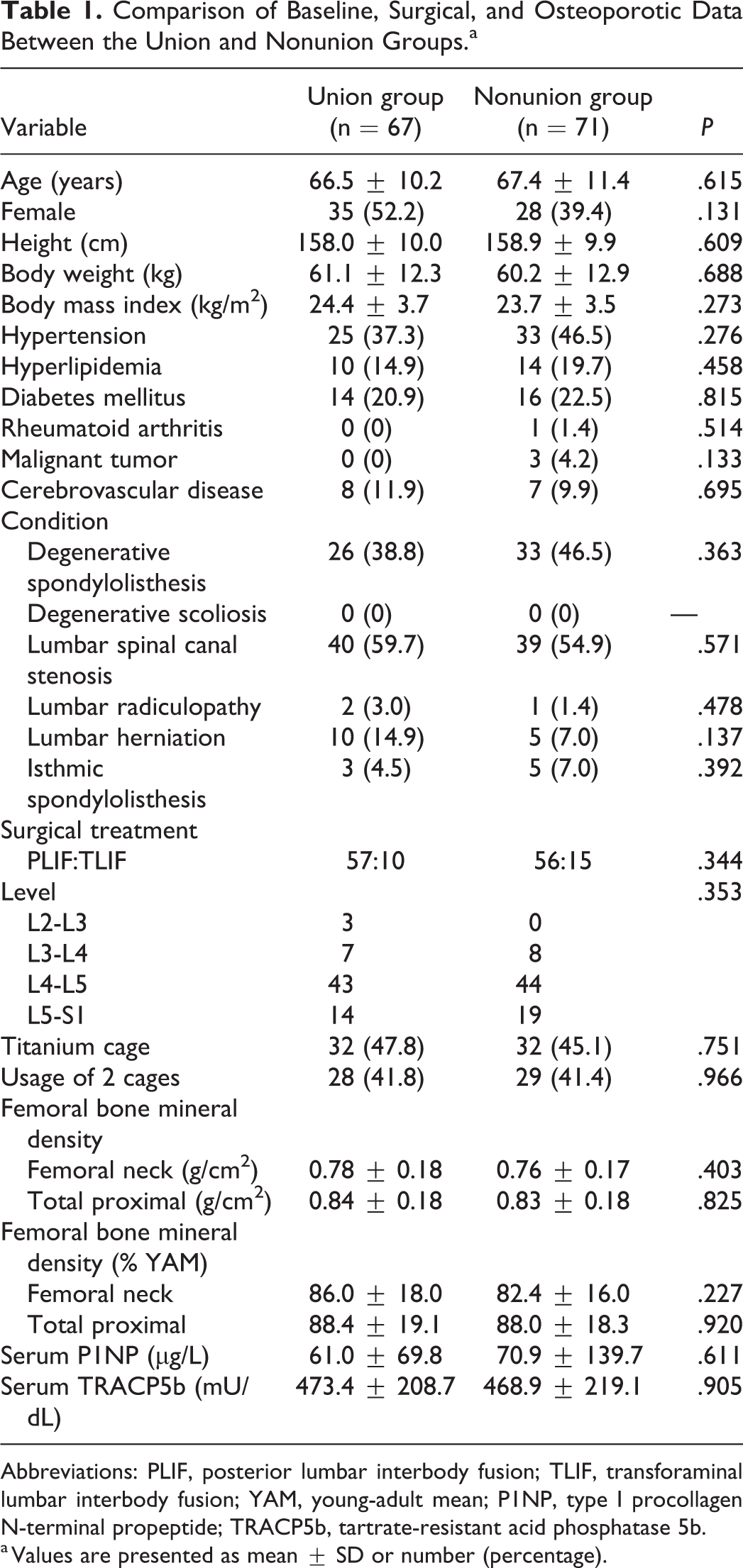
Abbreviations: PLIF, posterior lumbar interbody fusion; TLIF, transforaminal lumbar interbody fusion; YAM, young-adult mean; P1NP, type I procollagen N-terminal propeptide; TRACP5b, tartrate-resistant acid phosphatase 5b.
a Values are presented as mean ± SD or number (percentage).
The preoperative JOABPEQ scores for all subdomains and ODI scores did not differ between the groups, and all scores improved postoperatively compared with the preoperative scores in both groups (Table 2). The change in JOABPEQ subdomain scores for psychological disorders at 6 and 12 months postoperatively was significantly higher in the union group than in the nonunion group (P = .024 and P = .011, respectively; Table 2). Effective improvement of lumbar spine dysfunction was achieved in 28 patients in the union group (54.9%) and in 22 patients in the nonunion group (34.9%, P = .033). Effective improvement of psychological disorders was achieved in 31 patients in the union group (51.7%) and in 19 patients in the nonunion group (29.2%, P = .011). The change in ODI scores was not significantly different at 6 and 12 months postoperatively between the union and nonunion groups (P = .414 and P = .289, respectively).
Pre- and Postoperative Japanese Orthopaedic Association Back Pain Evaluation Questionnaire (JOABPEQ) and Oswestry Disability Index Scores, and the Changes (Postoperative Score − Preoperative Score) Between the Union and Nonunion Groups.a
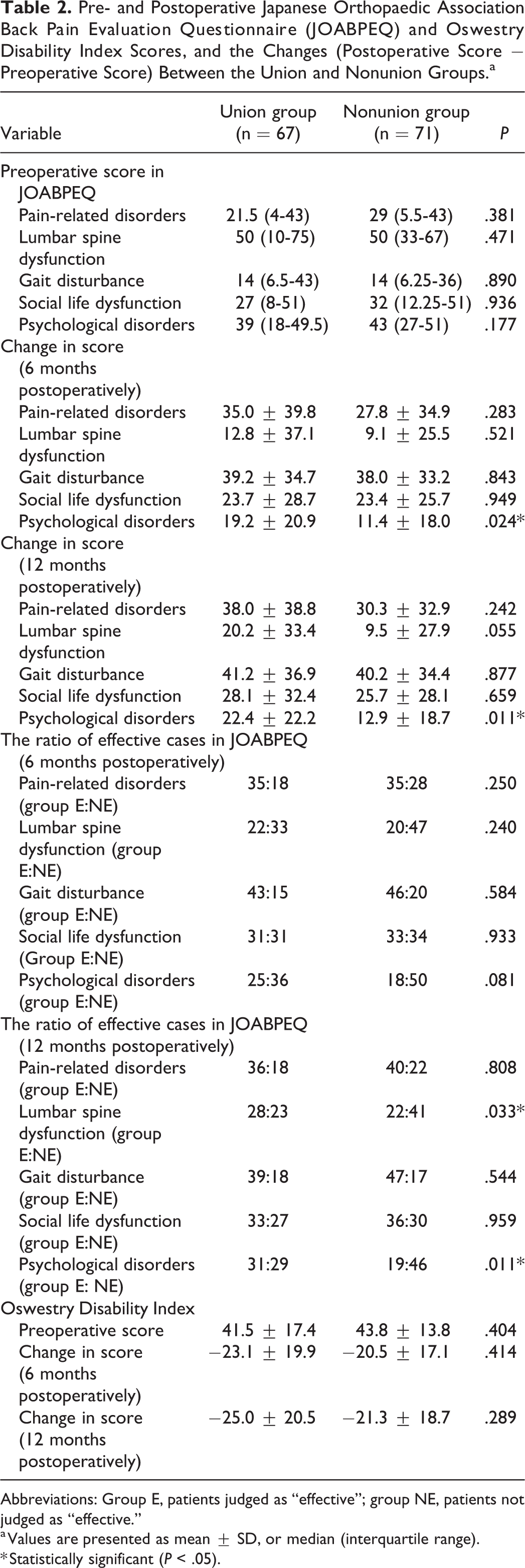
Abbreviations: Group E, patients judged as “effective”; group NE, patients not judged as “effective.”
a Values are presented as mean ± SD, or median (interquartile range).
* Statistically significant (P < .05).
Early Union Versus Delayed Union Versus Nonunion Groups
The number of patients in the early union, delayed union, and nonunion groups was 39, 28, and 71, respectively (Figure 1). There was a significant difference in sex between the groups (P = .023; Table 3). There was no significant difference in age, presence of hypertension or diabetes mellitus, type of surgical treatment, surgical level, usage of titanium-coated PEEK cage, and femoral BMD between the groups (Table 3).
Comparison of Baseline, Surgical, and Osteoporotic Data in the Early Union, Delayed Union, and Nonunion Groups.a
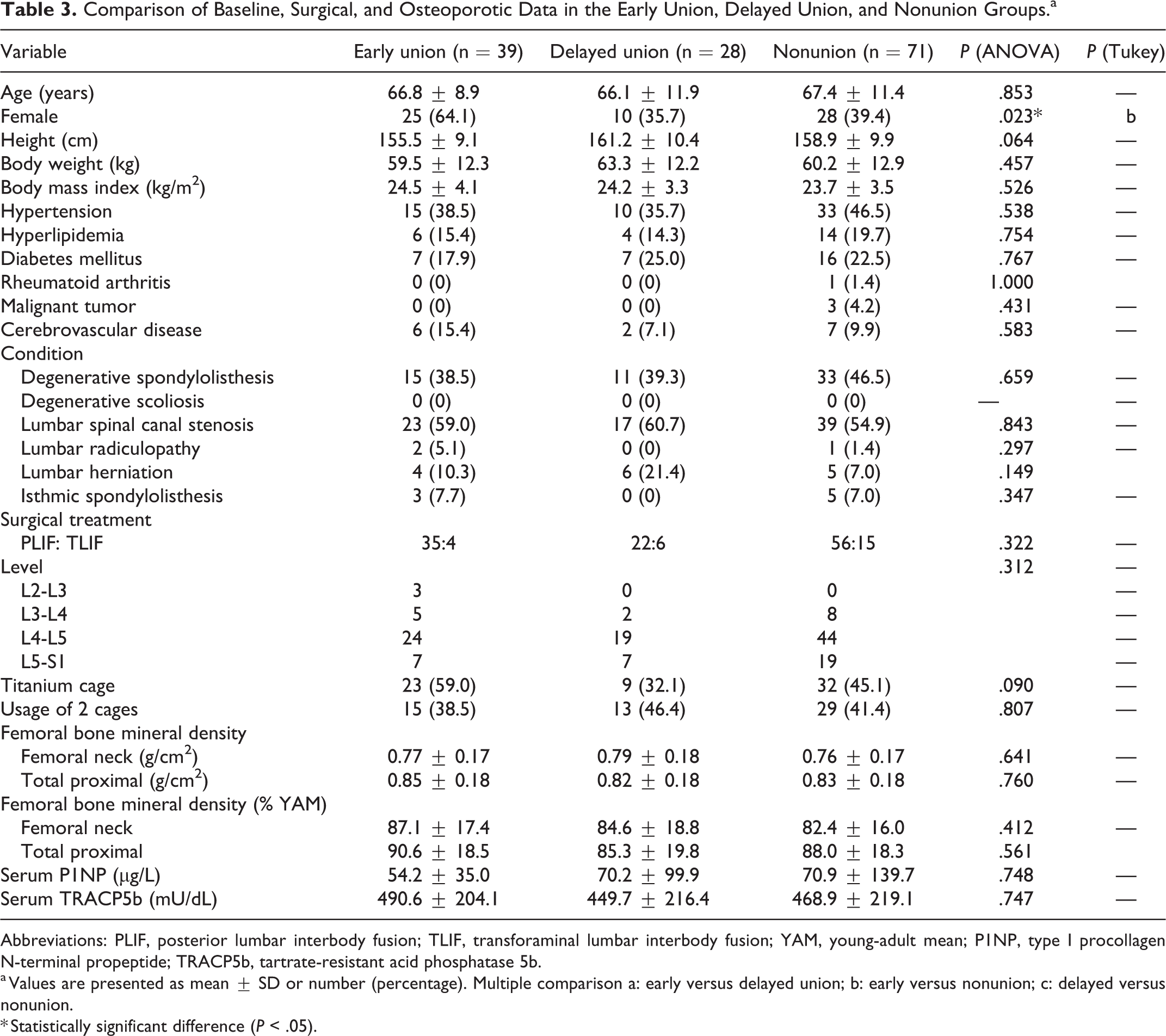
Abbreviations: PLIF, posterior lumbar interbody fusion; TLIF, transforaminal lumbar interbody fusion; YAM, young-adult mean; P1NP, type I procollagen N-terminal propeptide; TRACP5b, tartrate-resistant acid phosphatase 5b.
a Values are presented as mean ± SD or number (percentage). Multiple comparison a: early versus delayed union; b: early versus nonunion; c: delayed versus nonunion.
* Statistically significant difference (P < .05).
The preoperative JOABPEQ scores for all subdomains and ODI scores did not differ between the groups, and all scores improved postoperatively compared with the preoperative scores in 3 groups (Table 4). The change in JOABPEQ subdomain scores for psychological disorders at 12 months postoperatively was significantly higher in the early union and delayed union groups than in the nonunion group (P = .039; Table 4). Effective improvement of lumbar spine dysfunction was achieved in 19 patients in the early union group (63.3%), in 9 patients in the delayed union group (42.9%), and in 22 patients in the nonunion group (34.9%, P = .036). Effective improvement of psychological disorders was achieved in 17 patients in the early union group (50.0%), in 14 patients in the delayed union group (53.8%), and in 19 patients in the nonunion group (29.2%, P = .036). The change in ODI scores were not significantly different at 6 and 12 months postoperatively between the groups (P = .464 and P = .500, respectively).
Pre- and Postoperative Japanese Orthopaedic Association Back Pain Evaluation Questionnaire (JOABPEQ) and Oswestry Disability Index Scores, and the Changes (Postoperative Score − Preoperative Score) in the Early Union, Delayed Union, and Nonunion Groups.a
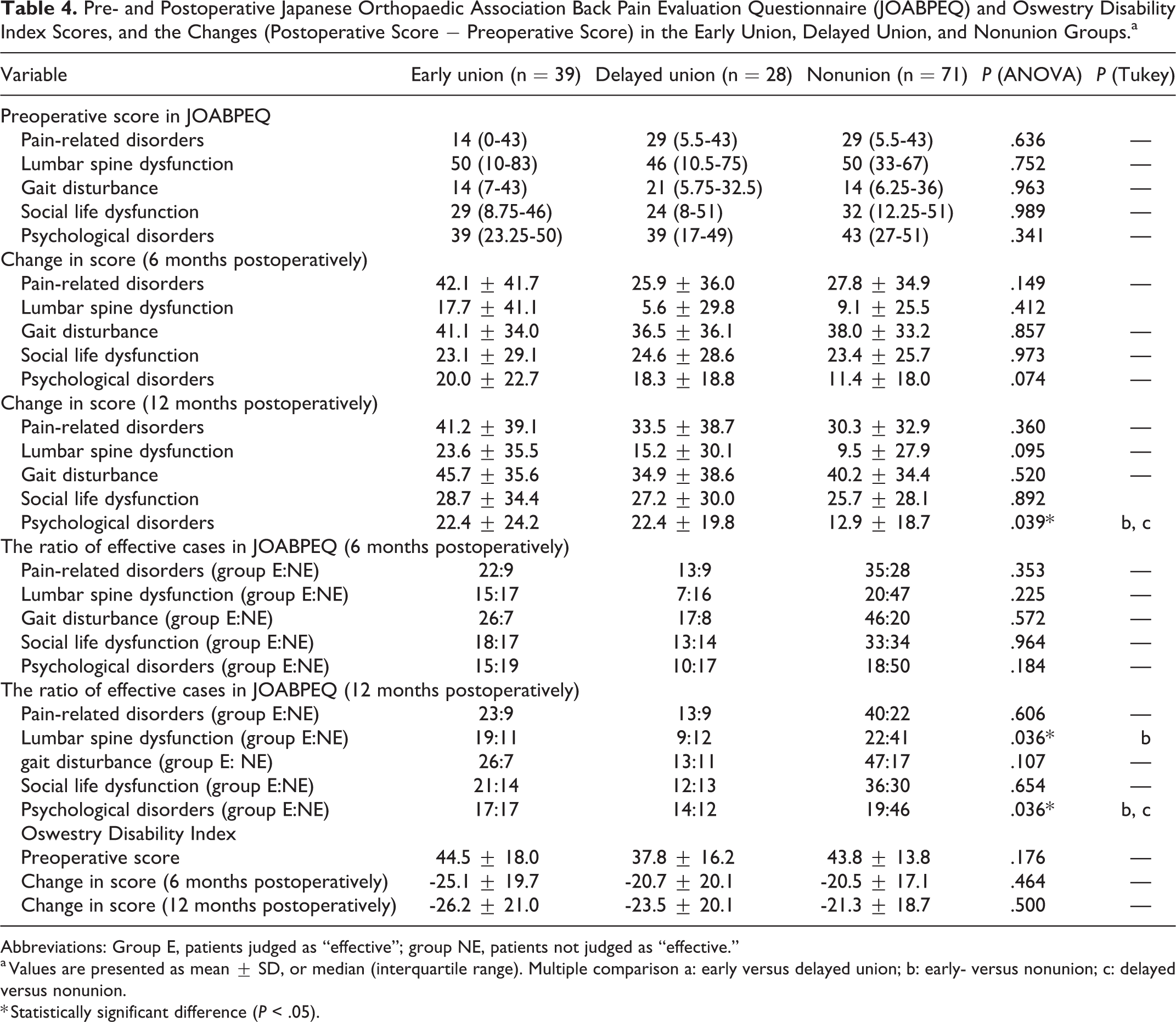
Abbreviations: Group E, patients judged as “effective”; group NE, patients not judged as “effective.”
a Values are presented as mean ± SD, or median (interquartile range). Multiple comparison a: early versus delayed union; b: early- versus nonunion; c: delayed versus nonunion.
* Statistically significant difference (P < .05).
Radiographic Assessment
The radiographic data from the early union, delayed union, and nonunion groups are shown in Table 5. There were no significant differences in all preoperative and postoperative parameters between the groups. Postoperative changes in ratio of cases with cage subsidence and screw loosening between the union and nonunion groups are shown in Figure 3. The nonunion group had a significantly higher proportion of cases with cage subsidence at 12 months postoperatively than the union group (P = .003). The nonunion group had a significantly higher proportion of cases with screw loosening at 6 and 12 months postoperatively than the union group (P = .033 and P = .022, respectively).
Comparison of Radiographic Parameters in the Early Union, Delayed Union, and Nonunion Groups.a
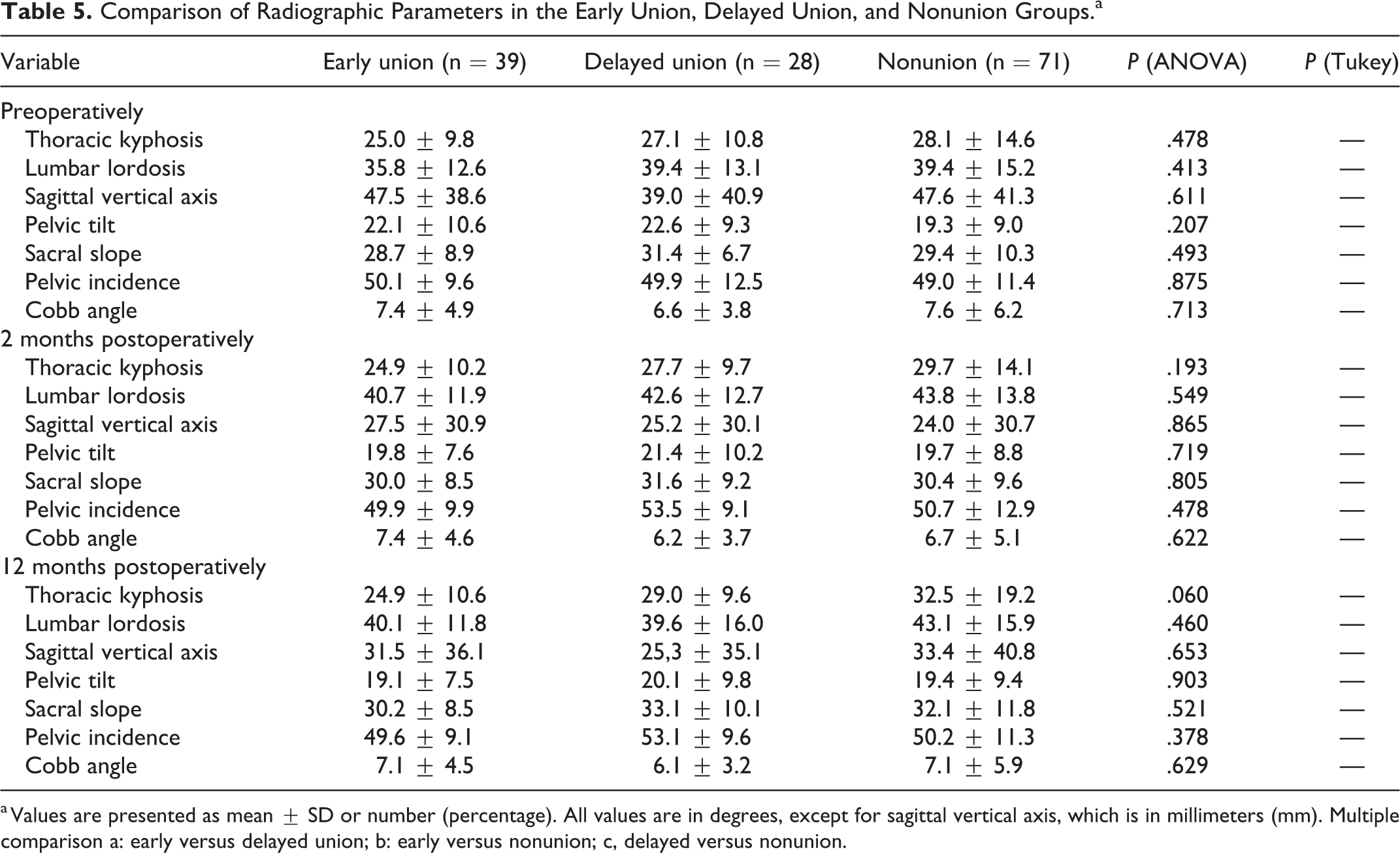
a Values are presented as mean ± SD or number (percentage). All values are in degrees, except for sagittal vertical axis, which is in millimeters (mm). Multiple comparison a: early versus delayed union; b: early versus nonunion; c, delayed versus nonunion.
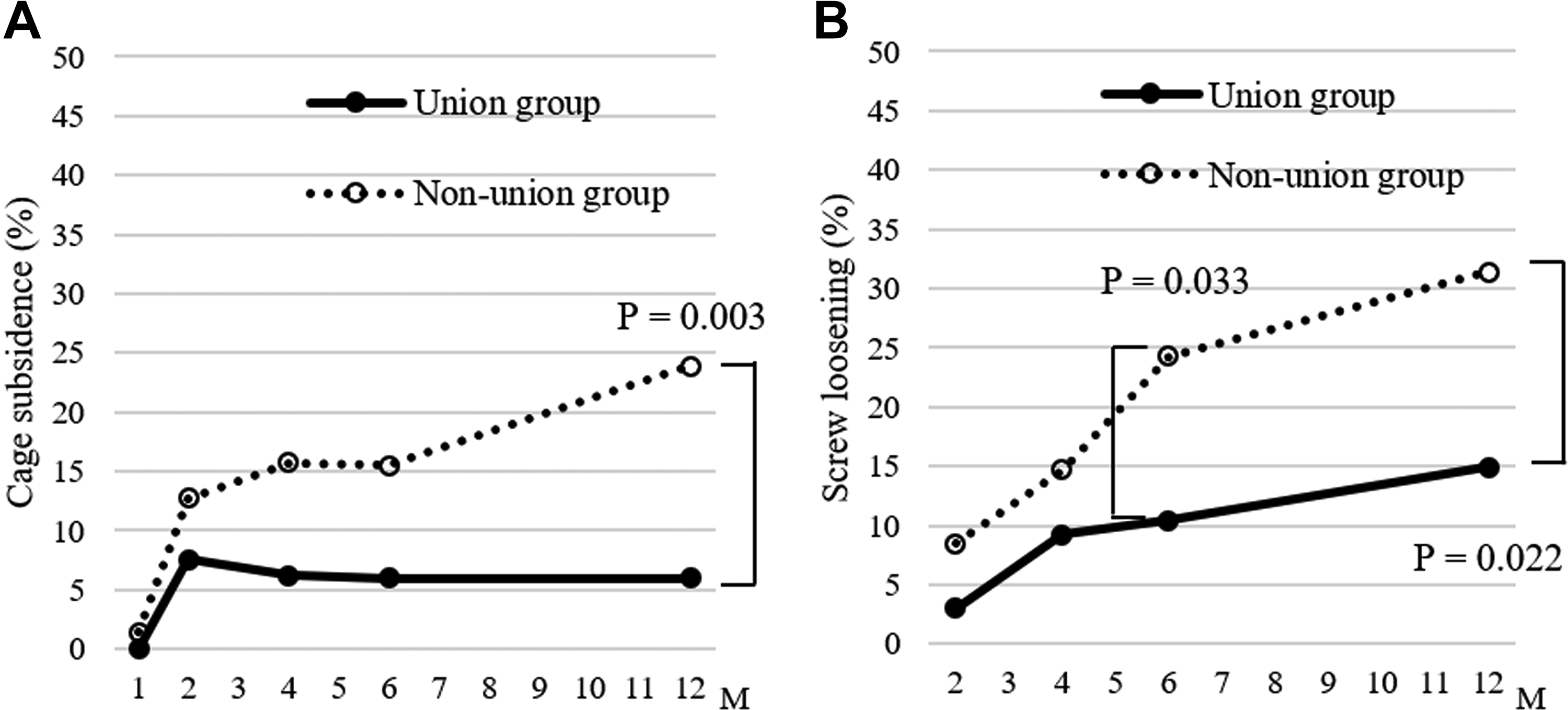
Postoperative Changes in Ratio of Cases With Cage Subsidence (A) and Screw Loosening (B) Between Union and Nonunion Groups.
Discussion
The intervertebral union rate (48.6%) within 12 months postoperatively in this study was lower than that of previous reports assessed by plain radiographs (more than 71% to 96%).7,14 This was presumably because the CT slices were blindly evaluated in detail, and complete union in both coronal and sagittal slices was defined according to the union outcome, which was a very strict definition (Figure 2). Considering that the lumbar spine dysfunction and psychological disorders significantly improved in cases with early complete union within 6 months, it would appear that early complete union must be obtained for improved HRQOL, especially in cases where lumbar spine function is concerned.
Although lumbar arthrodesis surgery with instrumentation has reduced the ration of pseudoarthrosis (2%-10%), pseudoarthrosis remains one of major radiographic complications after PLIF.15,16 The clinical impact of fusion status has been underestimated according to previous reports, which suggest pseudoarthrosis did not affect the deterioration of short-term outcomes after PLIF.16,17 In contrast, few studies showed that pseudoarthrosis affects the deterioration of long-term outcomes.17,18 The impact of fusion status after PLIF on HRQOL has been controversial. To evaluate the true effect of complete osseous union and influence of union period on HRQOL, we assessed the clinical outcomes at both 6 and 12 months postoperatively. In this study, ODI scores in the union and nonunion groups improved postoperatively and did not significantly differ between both groups. Our results using ODI scores supported previous findings. 16
The JOABPEQ is a low back pain-specific and patient-based evaluation questionnaire, 12 and its advantage is that it allows independent evaluation of 5 subdomains, whereas ODI score comprises a single overall score. In this study, the lumbar spine dysfunction significantly improved in cases with early complete union within 6 months postoperatively. Makino et al 6 reported that nonunion was a risk factor for poor improvement of lumbar spine function after PLIF with 2 years of follow-up. 6 They speculated that repetitive micromotion between cages and adjacent endplates can induce lumbar spine dysfunction. 19 In this study, screw loosening and cage subsidence at 12 months postoperatively occurred predominantly in the nonunion group compared to the union group. Our results support their speculation that nonunion causes micromotion, resulting in screw loosening and/or cage subsidence, and can induce lumbar spine dysfunction. However, cases with non-union at 12 months postoperatively exhibited poor improvement of psychological dysfunction in this study. Patients with lower mental health scores tend to rate HRQOL scores poorly and often have psychological disorders due to emotional problems. Mental health dysfunction can be associated with surgical outcomes. 20 Magni et al 21 reported that patients with psychological disorders may be predisposed to chronic low back pain, and the emotional problems are reactions to chronic low back pain. 21 We speculated about a few reasons regarding incomplete union caused poor improvement in psychological dysfunction. One possible reason is the presence of chronic low back pain induced by screw loosening and/or cage subsidence due to the presence of micromotion. Lumbar endplate injuries associated with disc degeneration or cage subsidence can induce low back pain.7,19 The other reason is the effect on mental health caused by recognition of incomplete union. If patients are informed of incomplete union in an outpatient setting, they might develop anxiety and pay closer attention in their daily life to prevent undesirable complications, such as instrumentation failure. The functional evaluation of each domain provided by the JOABPEQ may have contributed to the clarification of the effect of complete osseous union on HRQOL in our study. Our results showed that complete osseous union after PLIF was essential for short-term HRQOL outcomes, especially in cases where lumbar spine function and psychological dysfunction were concerned.
Currently, titanium-coated PEEK cages are available for PLIF. In addition to biological advantages due to cellular attachment and osteoblastic phenotype expression reported by in vitro studies, titanium-coated PEEK has osteoconductive activity and increased shear strength. 22 However, a systematic review showed similar fusion rates between titanium-coated PEEK cages and PEEK cages. 23 In our first report using a randomized controlled trial, titanium-coated PEEK cages significantly increased early complete union ratios compared with PEEK cages. 8 Our findings commensurate with previous in vitro studies. 22 The current study defined union outcome as completed osseous union, which was a very strict definition compared to previous clinical studies. Thus, usage of the titanium-coated PEEK cage may successfully achieve early intervertebral union and improve HRQOL.
Spinal and pelvic parameters are generally assessed using whole spine standing radiographs to evaluate the sagittal alignment of the spine. 24 Han et al 14 reported that preoperative pelvic parameters were not related to an osseous union after one-level PLIF. To our knowledge, there are no reports on the relationship between global sagittal alignment and intervertebral osseous union. In this study, we assessed preoperative and postoperative whole spine standing radiographs, and we observed no spinopelvic parameters related to early complete union. Our findings commensurate with a previous clinical study of Han et al. 14 We hope to assess dynamic whole spine standing radiographs to clarify the relationship between spinal compensation mechanisms and intervertebral osseous unions in a future study.
This study has several limitations. First, this was a small-sized retrospective study with an observation period of 12 months postoperatively. Second, we used dynamic radiographs and CT images to assess intervertebral osseous union. CT is the most definitive imaging tool for evaluating osseous union, although it involves exposing patients to radiation which can pose a risk. 25 However, we used a CT technique that required only 50% of the usual radiation exposure and we employed an iterative reconstruction method for image generation. Third, future studies may provide a convincing radiological parameter to predict the functional outcome postoperatively using dynamic whole spine standing radiographs. We hope to find and develop new radiographic parameters or confounding factors to predict the functional outcome in a future study with a well-designed multicenter randomized controlled trial and a large sample size. Finally, the maximum follow-up period of 12 months did not allow for the assessment of long-term outcomes over 2 years; a longer follow-up period would be needed to evaluate the long-term outcomes.
Conclusions
Lumbar spine dysfunction and psychological disorders significantly improved in cases with complete union at 12 months postoperatively, dominantly in cases with early complete union within 6 months postoperatively. However, cases with non-union exhibited poor improvement of lumbar spine dysfunction and psychological dysfunction, and screw loosening occurred predominantly from 6 months postoperatively. Therefore, the achievement of early complete union might be helpful for better HRQOL and lower incidence of postoperative complications.
Footnotes
Acknowledgments
We appreciate the help of Daisuke Togawa, Tatsuya Yasuda, Tomohiro Banno, Hideyuki Arima, Tomohiro Yamada, Yu Watanabe, Toshimasa Futatsugi, Masashi Uehara, Takashi Takizawa, Shugo Kuraishi, Shota Ikegami, Kunitada Fujita, Nagakazu Watanabe, Ryo Munakata, Yasuo Fujita, Kaneo Sato, Takashi Igarashi, Yuka Ozawa, Takashi Miyagawa, Shiro Inoue, Yoko Suzuki, Naomi Uchiyama, Nao Kuwahara, and Chieko Suzuki for case collections or manuscript discussions. We would like to thank Editage (![]() ) for English language editing.
) for English language editing.
Author Contributions
Dr Matsuyama and Dr Hasegawa were responsible for the study’s conception and design. Dr Ushirozako acquired, analyzed, and interpreted data; drafted the article; and approved the final version on behalf of all authors. All authors critically revised the article and reviewed the submitted version. Dr Matsuyama supervised the study.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Yamato belongs to a donation-funded laboratory called the “Division of Geriatric Musculoskeletal Health.” Donations to this laboratory have been received from Medtronic Sofamor Danek, Inc; Japan Medical Dynamic Marketing, Inc; and the Meitoku Medical Institution Jyuzen Memorial Hospital.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the B. Braun Aesculap.