
Abstract
Study Design
Systematic Review.
Objectives
Compare the outcomes of stand-alone lateral lumbar interbody fusion (LLIF) and LLIF with supplemental posterior instrumentation in the treatment of lumbar degenerative disease by a Meta-analysis.
Methods
In this meta-analysis, we searched Pubmed, Embase, and Cochrane databases from inception to Aug 2023. In this study, only study reporting stand-alone LLIF(stand-alone group) and LLIF with supplemental posterior instrumentation (posterior instrumentation group) in the treatment of lumbar degenerative disease and we excluded duplicate publications, research without full text, incomplete information or inability to conduct data extraction, animal experiments, reviews, and systematic reviews. STATA 15.1 software was used to analyze the data.
Results
Among the 15 included articles, the total number of patients was 1177, with 469 patients (638 fused segments) in the standalone group and 708 patients (1046 fused segments) in the posterior instrumentation group. The posterior instrumentation group was better than stand-alone group with significant differences in fusion rate, cage subsidence rate,the restoration of disc height and segmental lordosis, the improvement of ODI, and reoperation rate. While, comparing with posterior instrumentation group,the stand-alone group had less intraoperative blood loss.
Conclusions
Both stand-alone and instrumented LLIF were effective in improving the clinical outcomes of patients with lumbar degenerative disease. However, the stand-alone LLIF was associated with lower fusion rate, inferior maintenance of indirect decompression, and higher reoperation rate due to high-grade cage subsidence. For patients with risk factors of high-grade cage subsidence, the LLIF with posterior instrumentation may be a better choice.
Keywords
Introduction
Degenerative diseases of the lumbar spine are among the most common spinal conditions, causing symptoms like lower back and leg pain as well as restricted mobility, significantly affecting patients’ quality of life. 1 Lumbar interbody fusion techniques are widely used surgical methods to treat degenerative lumbar spine conditions, with traditional approaches including posterior lumbar interbody fusion (PLIF), transforaminal lumbar interbody fusion (TLIF), and anterior lumbar interbody fusion (ALIF). 2 Lateral lumbar interbody fusion (LLIF) is an emerging surgical technique that accesses the lumbar spine from the side, either passing through or bypassing the large muscles of the lower back, to treat degenerative lumbar spine conditions. The LLIF technique encompasses various types, such as extreme lateral interbody fusion (XLIF), oblique lateral interbody fusion (OLIF), crenel lateral interbody fusion (CLIF), direct lateral interbody fusion (DLIF), and lateral-anterior lumbar interbody fusion (LaLIF), among others.3-5 In comparison to traditional surgical approaches, LLIF allows for the placement of larger interbody fusion devices, which aids in safeguarding back muscles, ligaments, and other structures, while also reducing the risk of major vascular injury. As a result, LLIF is progressively finding widespread application in the treatment of degenerative lumbar diseases.3,6 LLIF typically requires additional posterior fixation to enhance segmental stability and fusion success rates . 7 In recent years, some scholars have suggested that, under appropriate patient selection, the use of stand-alone LLIF can yield clinical outcomes similar to LLIF with added posterior fixation. 8 However, stand-alone LLIF lacks the stress dispersion provided by internal fixation, leading to increased stress on the endplate and a higher likelihood of subsidence of the interbody spacer postoperatively. 9 Therefore, there remains a debate regarding whether LLIF necessitates additional posterior fixation. This study aims to conduct a comparative Meta-analysis of domestic and international research on stand-alone LLIF and LLIF with added posterior fixation for the treatment of degenerative lumbar diseases, aiming to provide valuable insights for clinical decision-making.
Materials and Methods
Literature Search Strategy
A comprehensive literature search was conducted from the inception of the databases up to Aug 2023, using various databases including PubMed, EMBASE and Cochrane Library. The earch terms included: ((((fixation[Title/Abstract]) OR (instrumentation[Title/Abstract])) OR (screw[Title/Abstract])) OR (instrumented[Title/Abstract])) AND (((stand-alone[Title/Abstract]) OR (stand alone[Title/Abstract])) AND ((((((lateral lumbar interbody fusion[Title/Abstract]) OR (extreme lateral interbody fusion[Title/Abstract])) OR (direct lateral interbody fusion[Title/Abstract])) OR (oblique lateral interbody fusion[Title/Abstract])) OR (crenel lateral interbody fusion[Title/Abstract])) OR (lateral-anterior lumbar interbody fusion[Title/Abstract]))).
Inclusion and Exclusion Criteria
Inclusion Criteria: (1) Subjects: Patients with degenerative lumbar spine diseases; (2) Intervention measure: Patients who underwent stand-alone LLIF without additional lateral fixation (stand-alone group); (3) Control: Patients who underwent LLIF with bilateral percutaneous pedicle screw fixation (fixation group); (4) Outcome indicatiors: Fusion rate at the latest follow-up, incidence of subsidence of fusion device, improvement in radiographic parameters from preoperative to postoperative imaging at the latest follow-up, improvement in visual analogue scale (VAS) scores for leg pain, improvement in Oswestry disability index (ODI) scores, intraoperative blood loss, length of hospital stay, incidence of complications, revision rate, and adjacent segment disease occurrence. (5) Study design: Cohort study.
Exclusion Criteria: Duplicate publications; studies for which full text was not available or for which data extraction was not possible; studies using animal studies; reviews and systematic reviews.
Assessment of Literature Quality
Two reviewers independently conducted literature screening and quality assessment. Initially, titles and abstracts were reviewed for inclusion. Full texts of remaining articles were examined, and those meeting the inclusion and exclusion criteria were selected for quality evaluation. Quality assessment of randomized controlled trials followed the Cochrane Handbook guidelines, while non-randomized controlled trials were assessed using the Newcastle-Ottawa Scale (NOS) 10 recommended by the Cochrane Collaboration Network. High-quality studies were selected based on the results of quality assessment. Disagreements were resolved through discussion with a third reviewer to achieve consensus.
Data Extraction
Data extraction was conducted independently by 2 researchers and subsequently summarized and cross-checked by a third researcher. Extracted data were required to be reported in at least 2 articles. Demographic information included age, gender, body mass index (BMI), number of cases, fused segments. For primary outcome measures, continuous variables encompassed improvement in intervertebral height, segmental lordosis angle, lumbar lordosis angle, VAS scores for leg pain, ODI improvement, intraoperative blood loss, and postoperative hospital stay. Binary variables included fusion rate, incidence of subsidence of fusion device, incidence of adverse events and reoperation rate.
Data Analysis
Meta-analysis was conducted using STATA 15.1 software. 11 Weighted mean differences (WMD) were used for continuous variables, while odds ratio (OR) were used for binary variables. All effect sizes were presented with their 95% confidence intervals (CI). Heterogeneity among studies was assessed using I2 values and P-values. If I2 ≤ 50% and P > 0.1, it indicated low heterogeneity, and a fixed-effects model was used. If I2 > 50% and P ≤ 0.1, indicating substantial heterogeneity, sensitivity analysis was performed to assess the impact of individual studies on heterogeneity, and subgroup analysis was conducted if necessary. If heterogeneity could not be resolved, a random-effects model was employed for studies with clinical consistency. A significance level of P < 0.05 indicated statistically significant intergroup differences. Furthermore, we employed funnel plots and Egger’s test to assess the presence of publication bias in the included studies.
Results
Literature Search Results
A total of 584 articles were collected for this study. After excluding duplicate studies, 298 studies were included in this study. A total of 208 articles were identified after reading their titles and abstracts. Finally, 15 studies were included in the meta-analysis (Figure 1). Flow diagram for selection of study.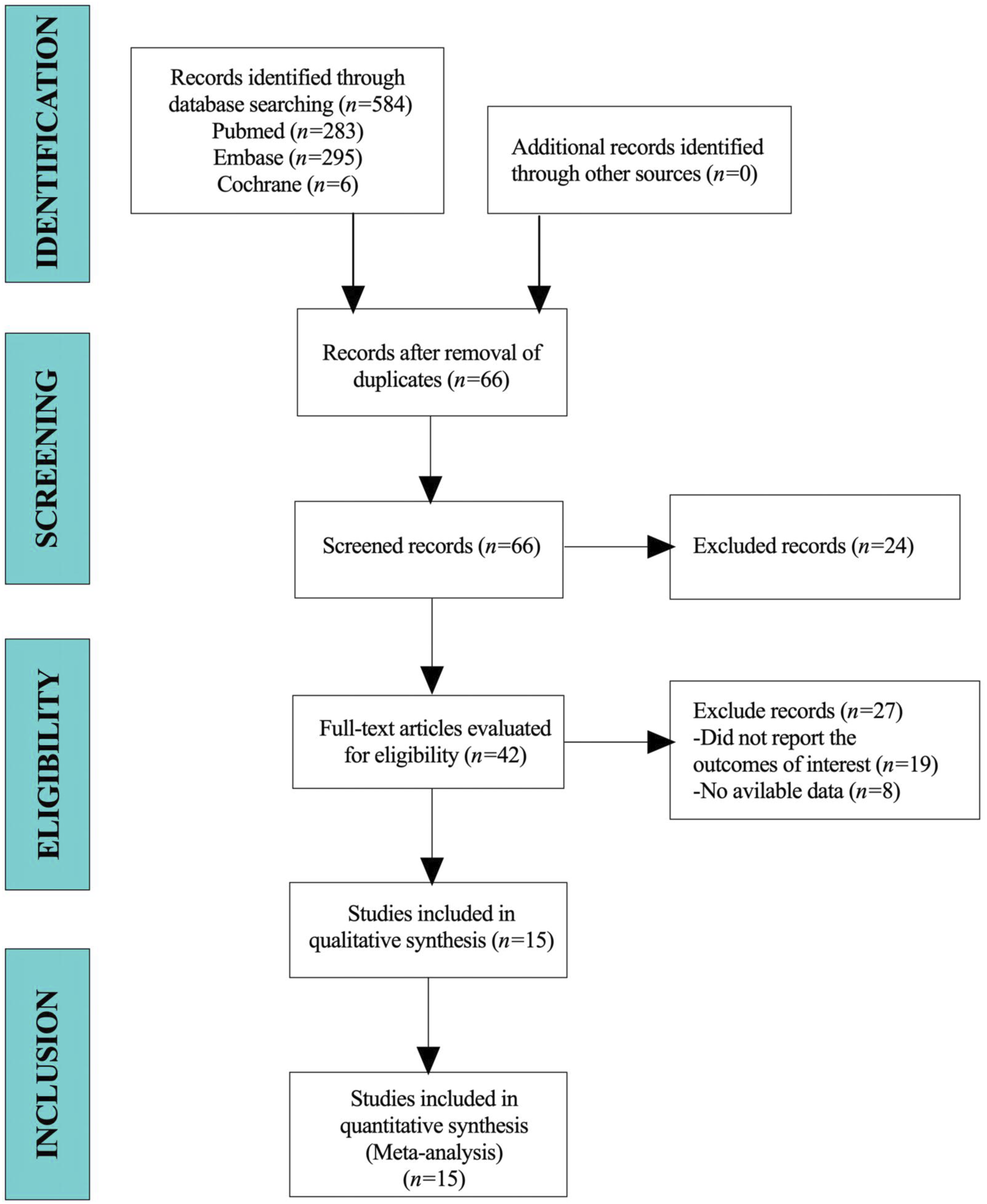
Baseline Characteristics and Quality Assessment of the Included Studies
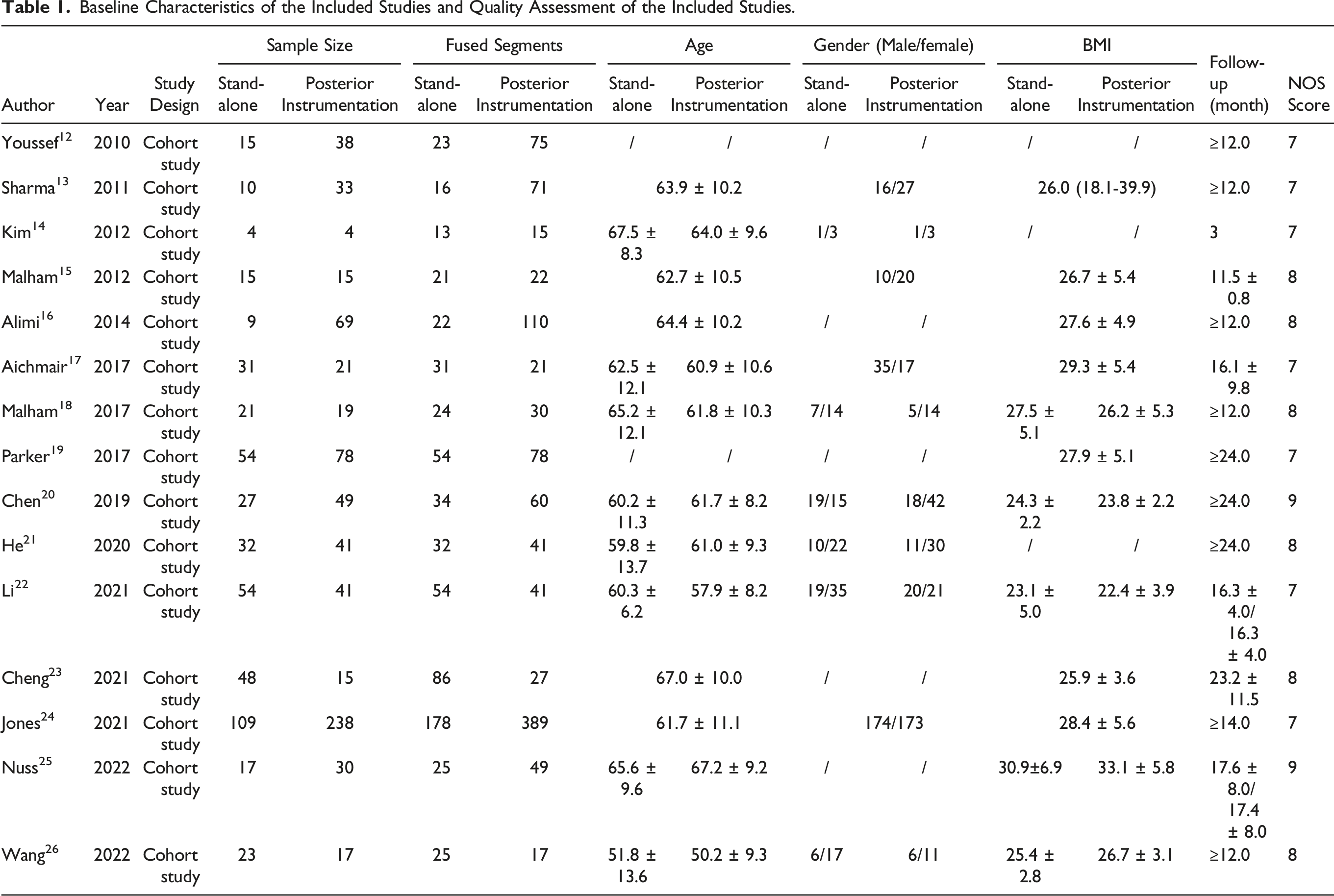
Baseline Characteristics of the Included Studies and Quality Assessment of the Included Studies.
Meta-Analysis Results
Fusion Rate
8 articles reported the fusion rate at the last follow-up after surgery. As no significant heterogeneity was observed (I2 = 40.9%, P = 0.106), a fixed-effect model was employed for the meta-analysis. The combined results indicated a statistically significant lower fusion rate in the stand-alone group compared to the posterior instrumentation group (OR = 0.41, 95%CI: 0.23 to 0.74, P = 0.003) (Figure 2). Forest plot of the fusion rate for the stand-alone and the posterior instrumentation groups.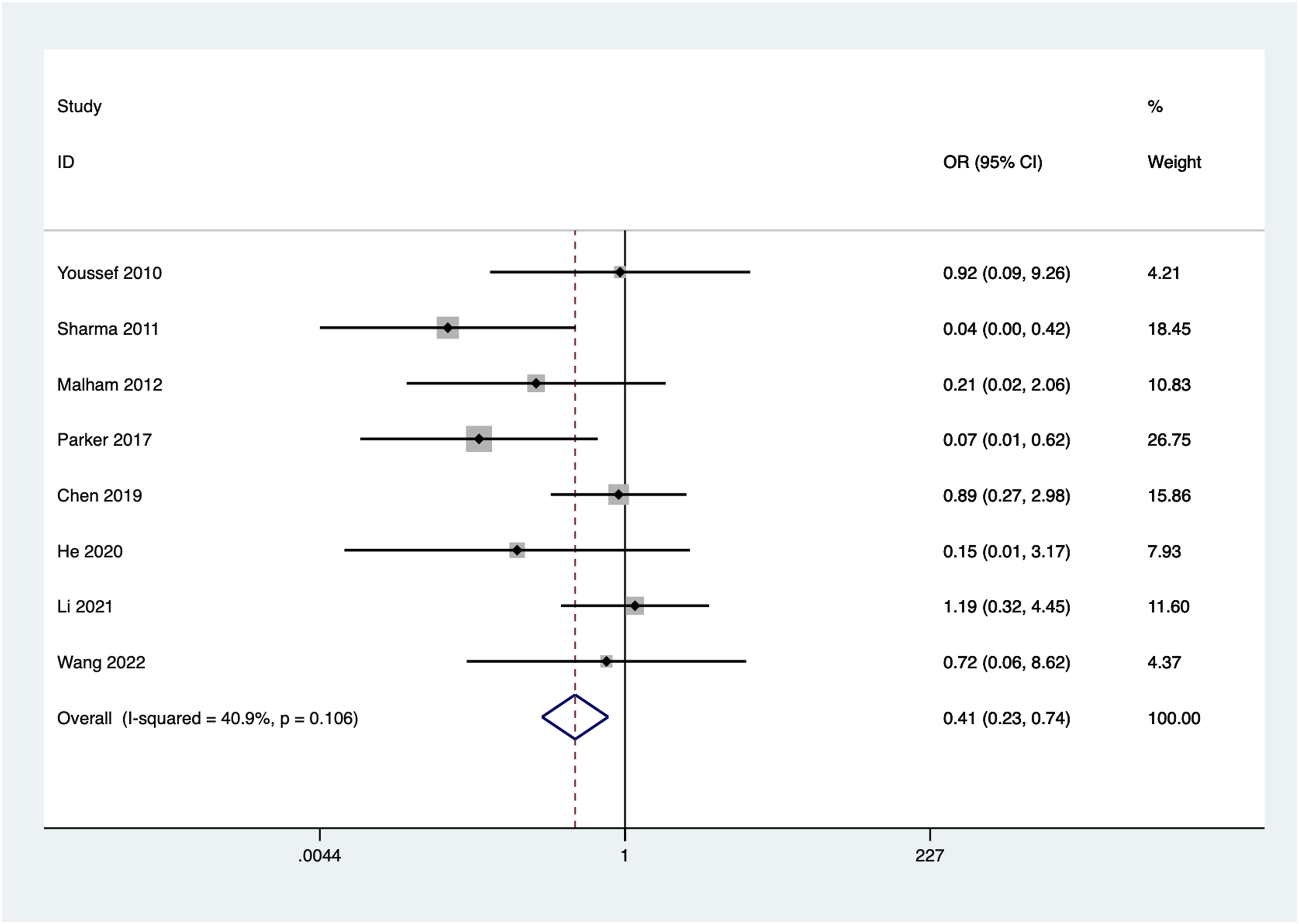
Cage Subsidence Rate
12 articles reported the cage subsidence rate at the last follow-up after surgery. No significant heterogeneity was observed among the included studies (I2 = 0.0%, P = 0.680). Using a fixed-effect model, the combined results showed a statistically significant higher implant subsidence rate in the stand-alone group compared to the posterior instrumentation group (OR = 2.09, 95%CI: 1.55 to 2.81, P = 0.000) (Figure 3). Forest plot of the cage subsidence rate for the stand-alone and the posterior instrumentation groups.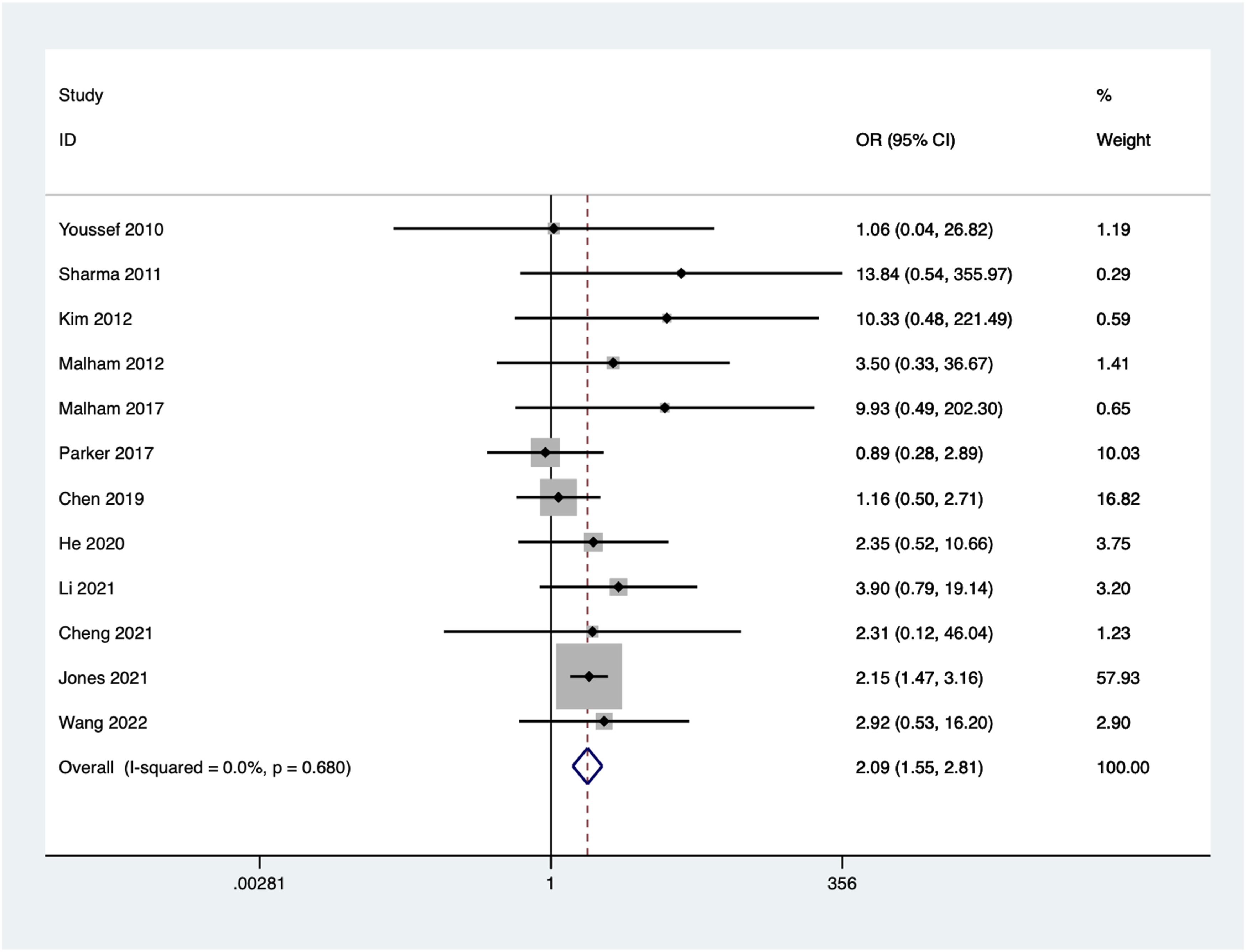
Interbody Height Improvement
6 articles reported the improvement in interbody height from preoperative to the last follow-up. As no significant heterogeneity was observed (I2 = 42.8%, P = 0.120), a fixed-effect model was employed for the meta-analysis. Pooled results indicated a statistically significant lower interbody height improvement in the stand-alone group compared to posterior instrumentation group (WMD -0.68, 95%CI: −1.04 to −0.32, P = 0.000) (Figure 4). Forest plot of the interbody height improvement for the stand-alone and the posterior instrumentation groups.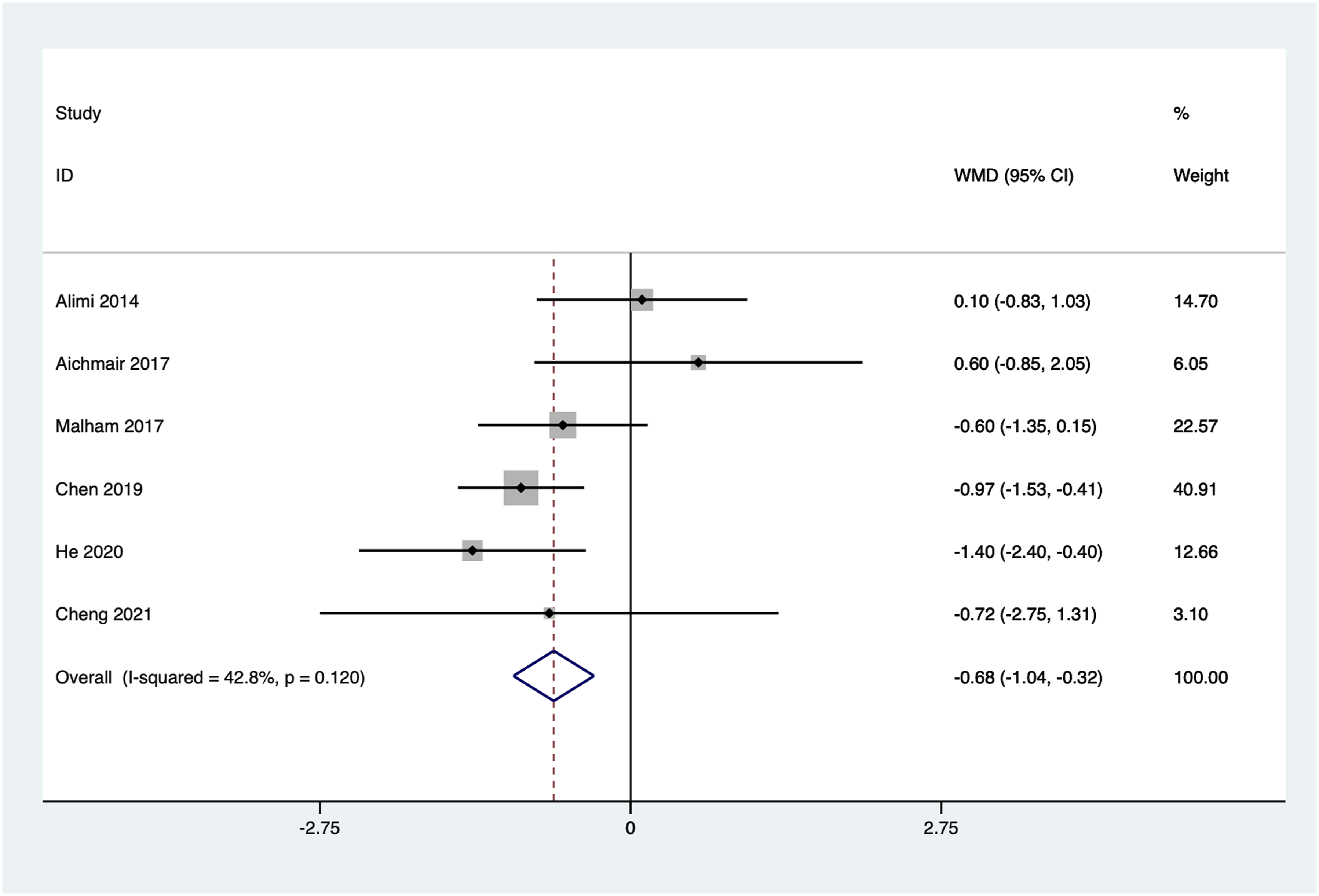
Segmental Lordosis Improvement
Four articles reported the improvement in segmental lordosis from preoperative to the last follow-up. As no significant heterogeneity was observed (I2 = 0.0%, P = 0.455), a fixed-effect model was employed for the meta-analysis. Pooled results indicated a statistically significant lower segmental lordosis improvement in the stand-alone group compared to the posterior instrumentation group (WMD = −1.34, 95% CI: −2.28 to −0.40, P = 0.005) (Figure 5). Forest plot of the segmental lordosis improvement for the stand-alone and the posterior instrumentation groups.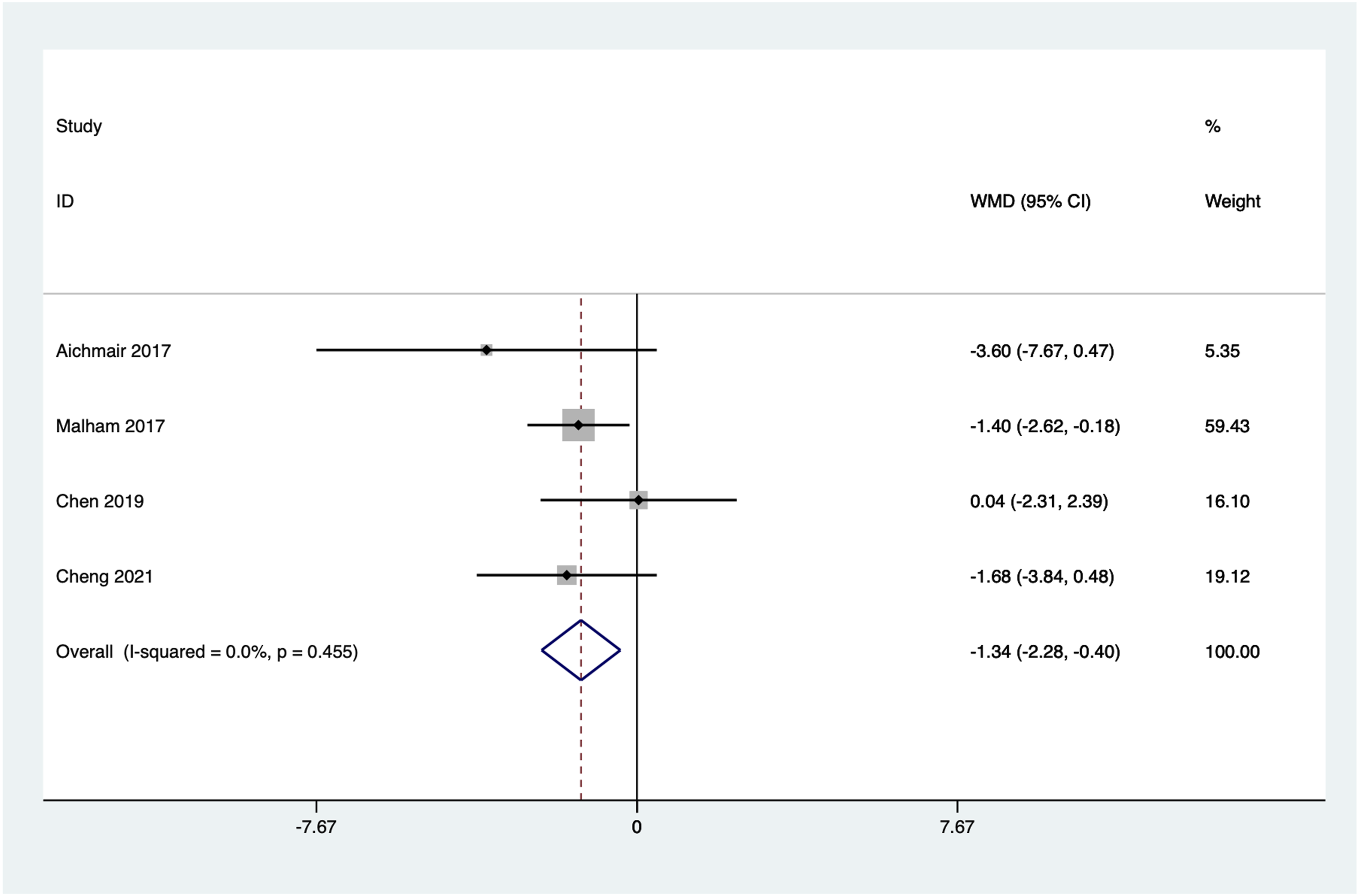
Lumbar Lordosis Improvement
Five articles reported the improvement in lumbar lordosis from preoperative to the last follow-up. Significant heterogeneity was observed among the included studies (I2 = 63.8%, P = 0.026). Using a random-effect model, the combined results showed no statistically significant difference between the 2 groups (WMD = −0.62 95% CI: −3.39 to 2.15, P = 0.662) (Figure 6). Forest plot of lumbar lordosis improvement for the stand-alone and the posterior instrumentation group.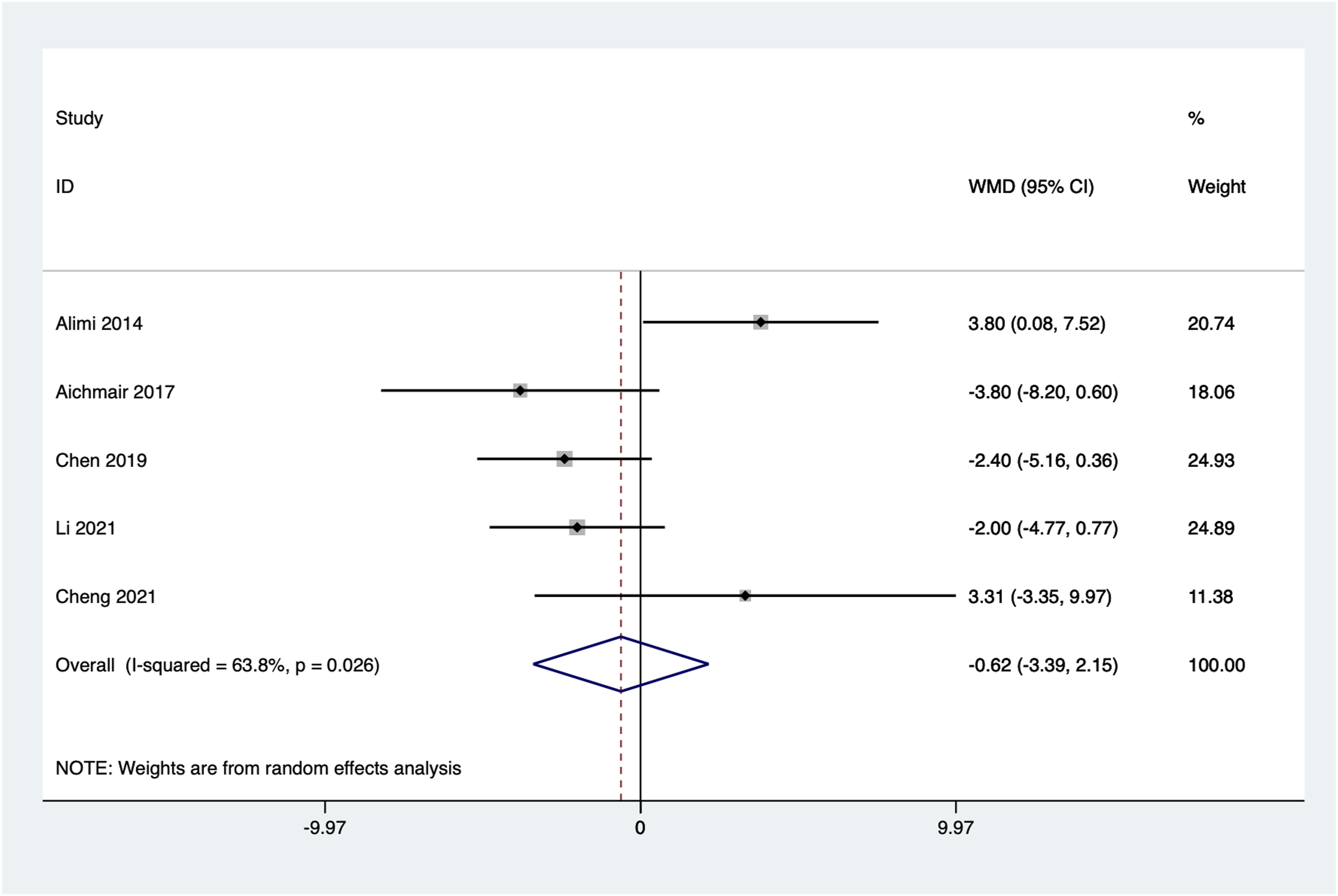
VAS Score Improvement
Eight articles reported the improvement in VAS scores from preoperative to the last follow-up. Significant heterogeneity was observed among the included studies (I2 = 86.5%, P = 0.000) and a random-effects model was used to combine effects. The pooled results showed no statistically significant difference between the 2 groups in VAS scores improvement (WMD = 0.60, 95%CI: −0.21 to 1.42, P = 0.147) (Figure 7). Forest plot of VAS scores improvement for the stand-alone and the posterior instrumentation groups.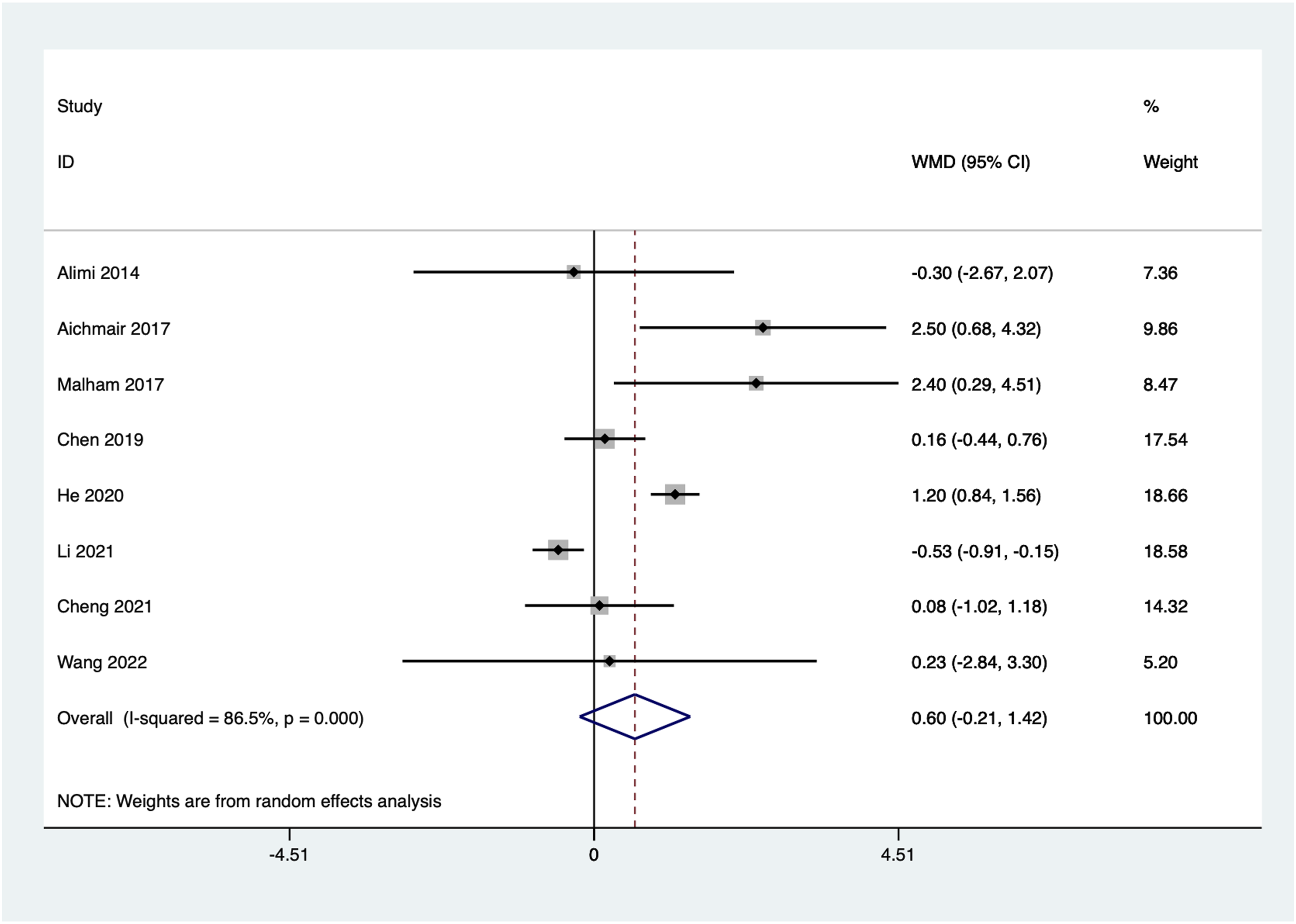
ODI Improvement
Five articles reported the improvement in Oswestry Disability Index (ODI) scores from preoperative to the last follow-up. No significant heterogeneity was observed among the included studies (I2 = 44.4%, P = 0.126), and a fixed-effect model was used. The combined results showed a statistically significant lower ODI improvement in the standalone group compared to the posterior instrumentation group (WMD = −1.39, 95%CI: −2.45 to −0.32, P = 0.011) (Figure 8). Forest plot of ODI improvement for the stand-alone and the posterior instrumentation groups.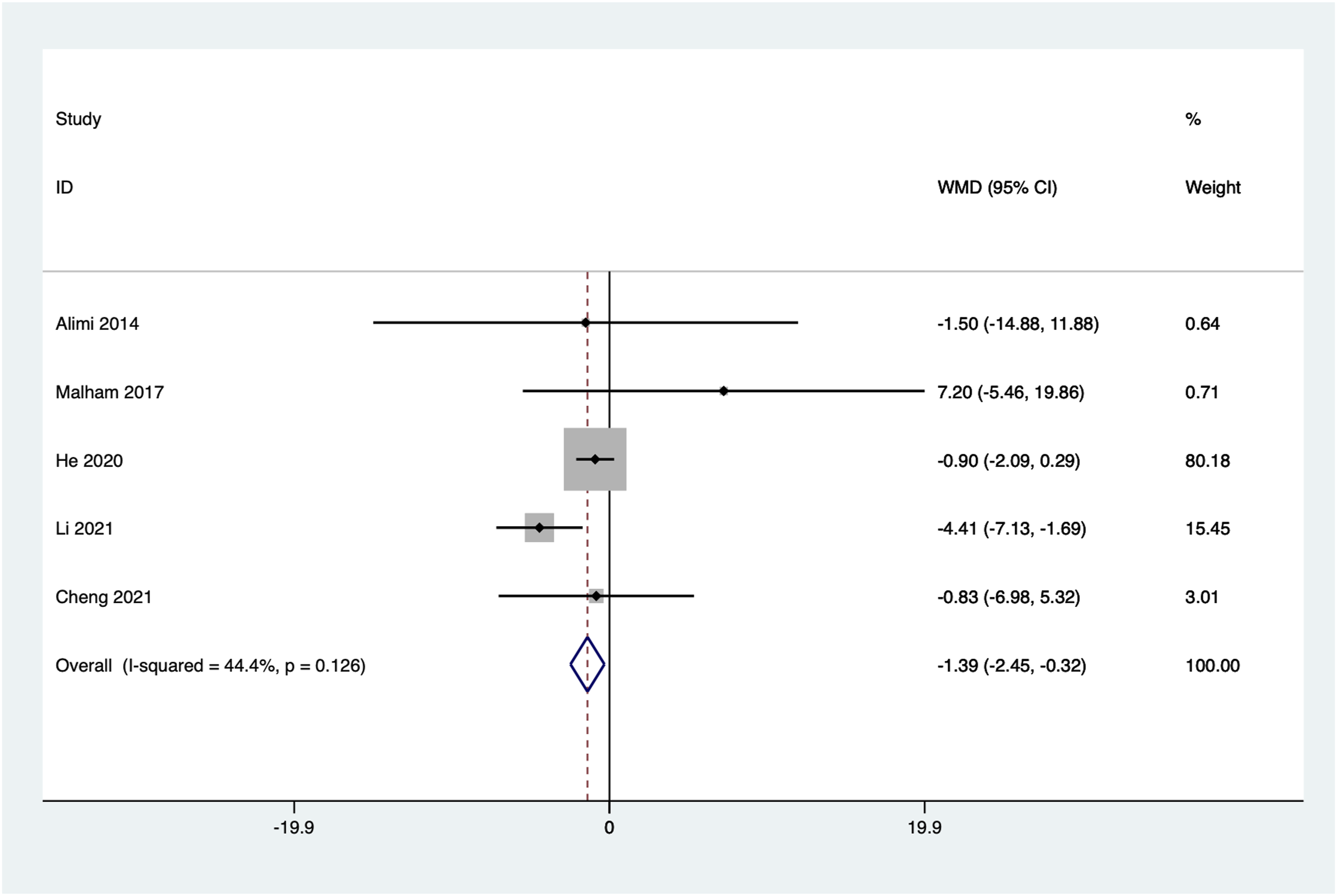
Intraoperative Blood Loss
Five articles reported intraoperative blood loss. Significant heterogeneity was observed among the included studies (I2 = 97.4%, P = 0.000). Sensitivity and subgroup analyses were conducted, and a random-effects model was used. The combined results showed a statistically significant lower intraoperative blood loss in the stand-alone group compared to the posterior instrumentation group (WMD = −73.82, 95% CI: −117.28 to −30.36, P = 0.001) (Figure 9). Forest plot of the intraoperative blood loss for the stand-alone and the posterior instrumentation group.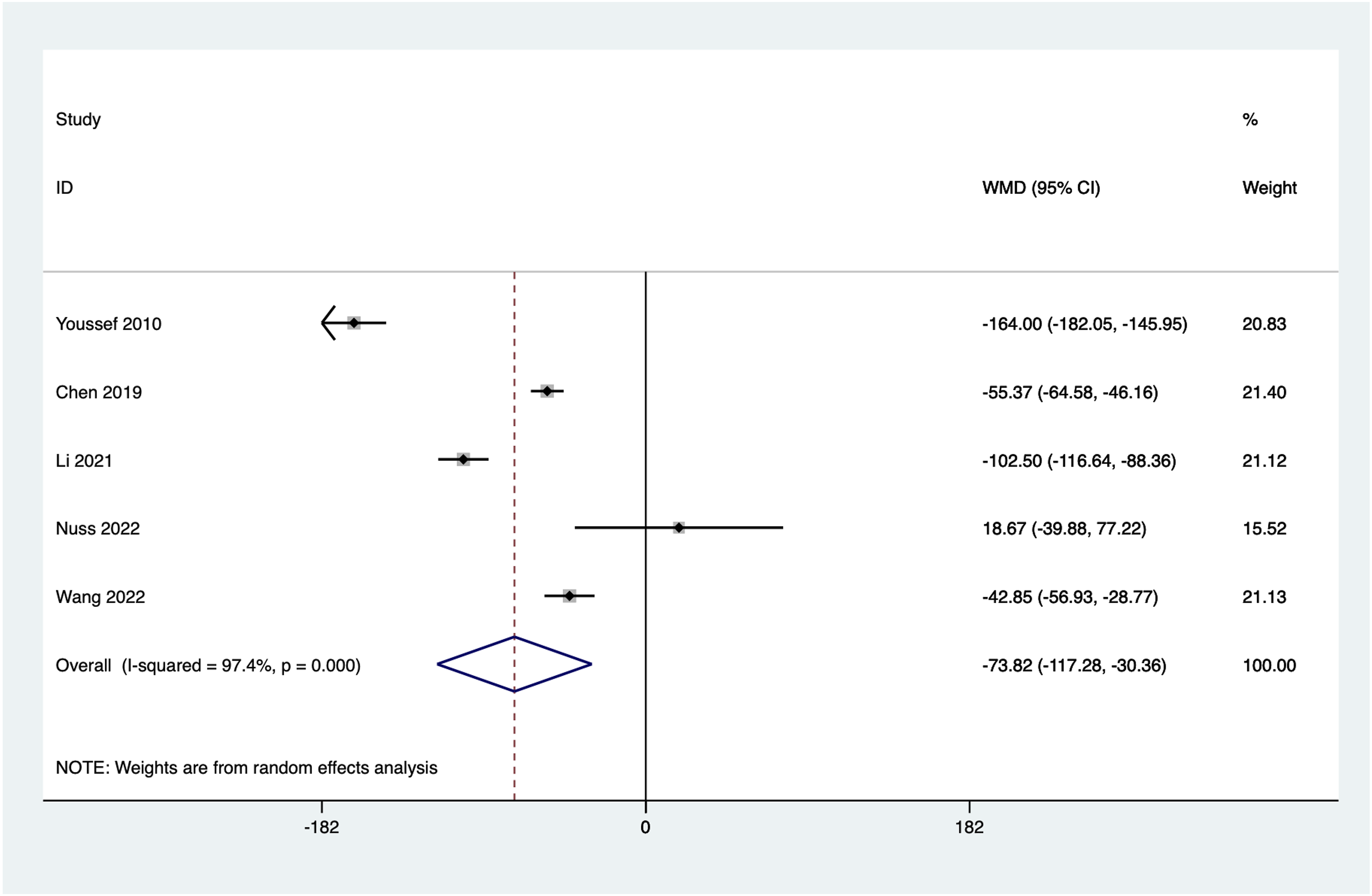
Postoperative Hospital Stay
Four articles reported postoperative hospital stay. Significant heterogeneity was observed among the included studies (I2 = 81.6%, P = 0.001). Sensitivity and subgroup analyses were conducted, and a random-effects model was used. The combined results showed no statistically significant difference in postoperative hospital stay between the 2 groups (WMD = −1.29, 95%CI: −2.54 to −0.04, P = 0.044) (Figure 10). Forest plot of the postoperative hospital stay for the stand-alone and the posterior instrumentation group.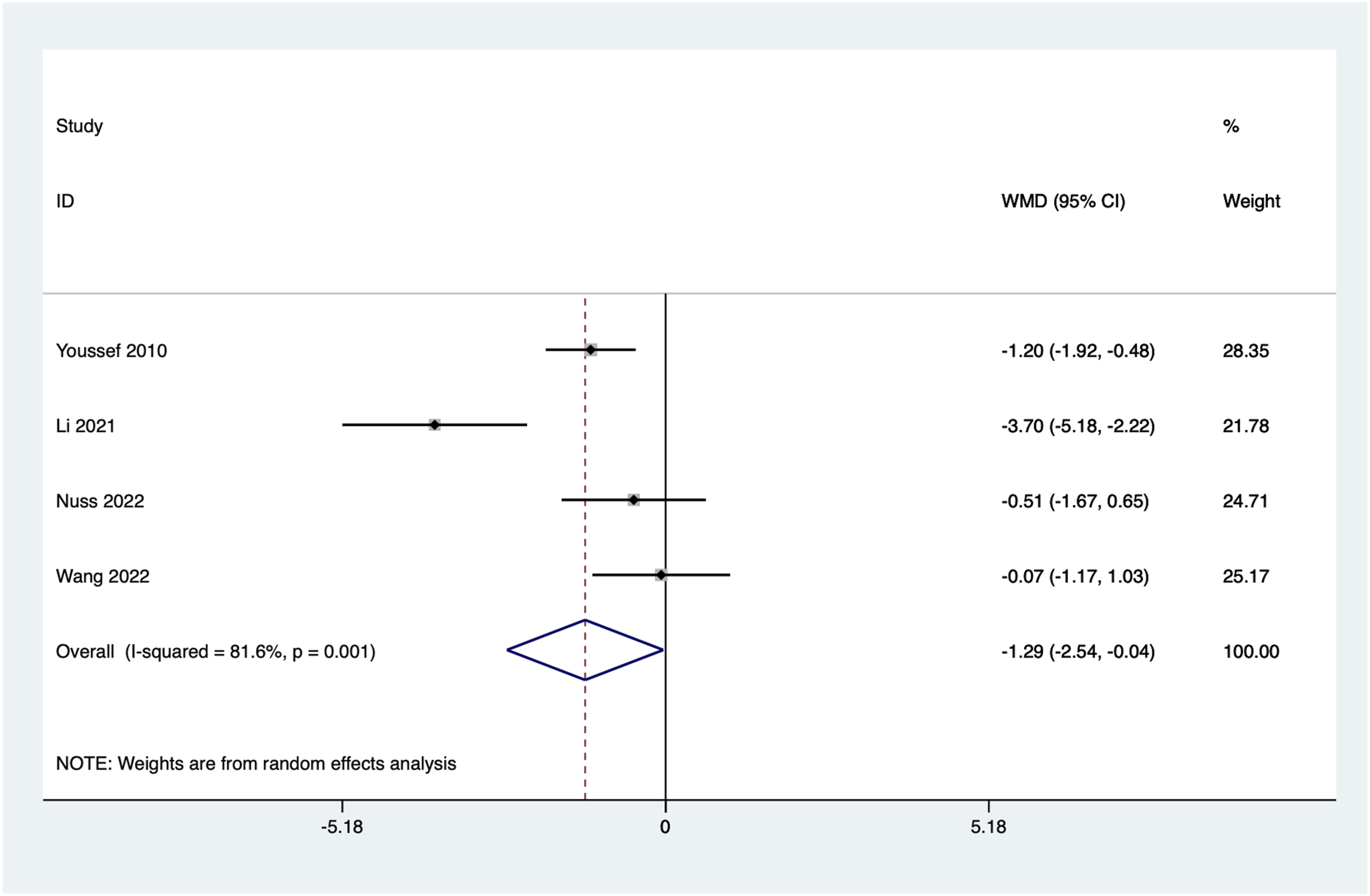
Reoperation Rate
Seven articles reported reoperation after the initial procedure. No significant heterogeneity was observed among the included studies (I2 = 8.0%, P = 0.367), and a fixed-effect model was used. The combined results showed a statistically significant higher reoperation rate in the standalone group compared to the internal fixation group (OR = 23.06, 95%CI: 1.38 to 6.79, P = 0.006) (Figure 11). Forest plot of the reoperation rate for the stand-alone and the posterior instrumentation group.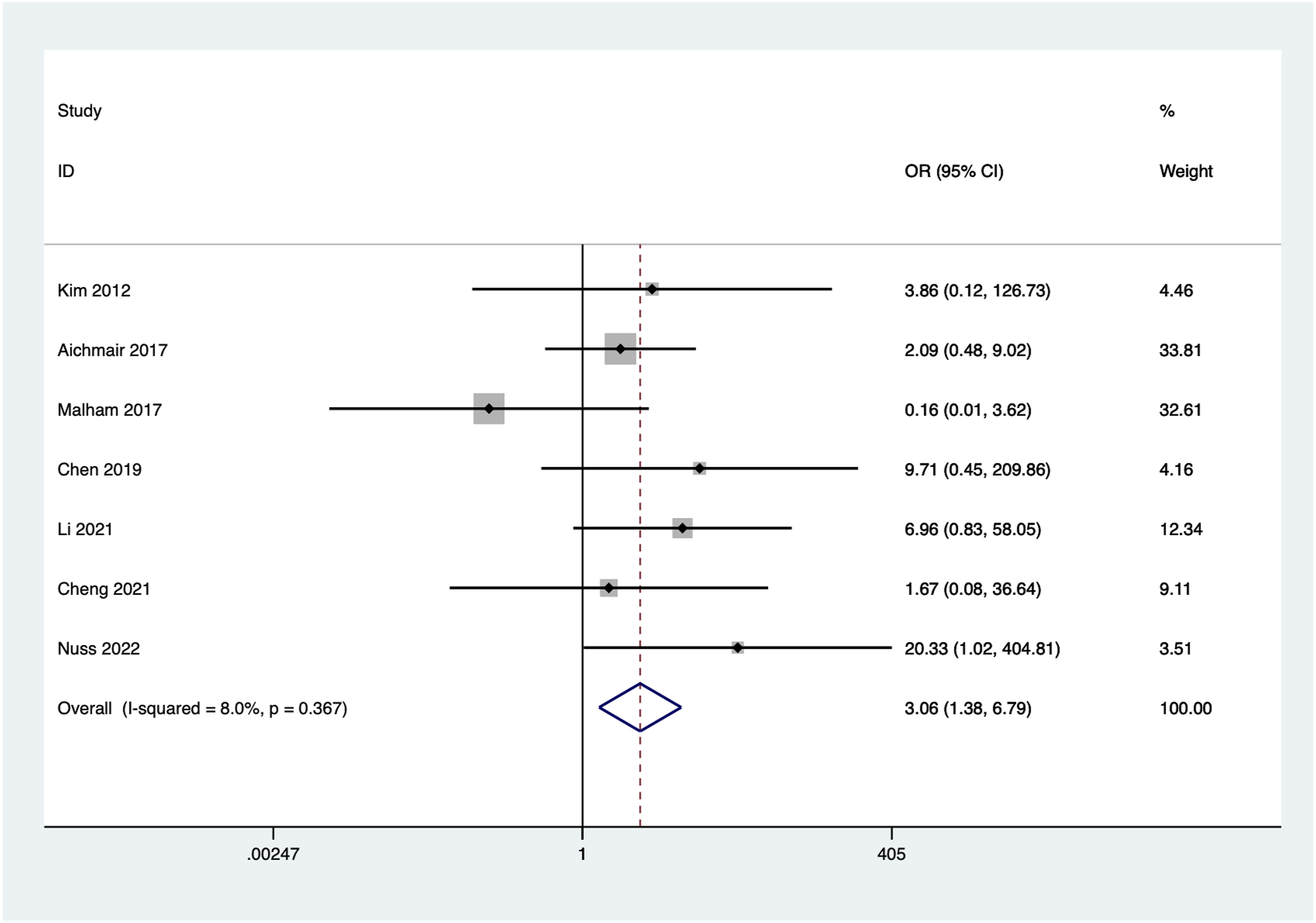
Incidence of Adverse Events
Nine articles reported the incidence of adverse events. No significant heterogeneity was observed among the included studies (I2 = 0.0%, P = 0.714), and a fixed-effect model was used. The combined results showed no statistically significant difference in incidence of adverse events between the 2 groups (OR = 1.44, 95% CI 0.91 to 2.28, P = 0.12) (Figure 12). Forest plot of incidence of adverse events for the stand-alone and the posterior instrumentation group.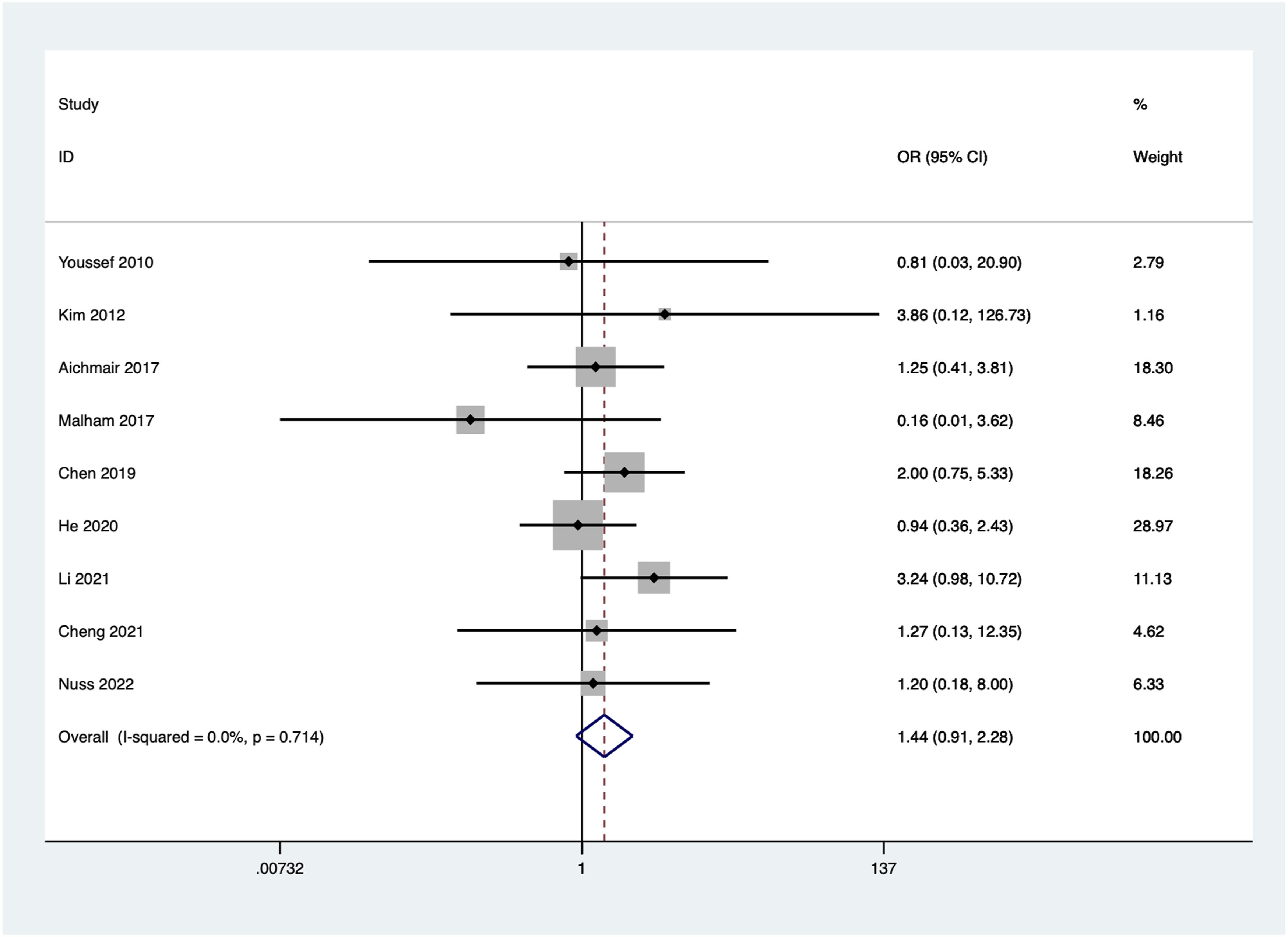
Sensitivity Analysis
A sensitivity analysis was conducted in which each trial was excluded individually, followed by a combined analysis of the remaining trials for various outcomes. The results of these sensitivity analyses did not reveal any articles that significantly influenced the overall results. This suggests that the findings of this study are stable and reliable, with no individual trial having a substantial impact on the results.
Publication Bias
Figure 13 present the funnel plots. The funnel plots were symmetrical, and the P-values of Egger’s tests were 0.260, which indicated there was no obvious publication bias in this study. Funnel plot for evaluating the publication bias of this meta-analysis.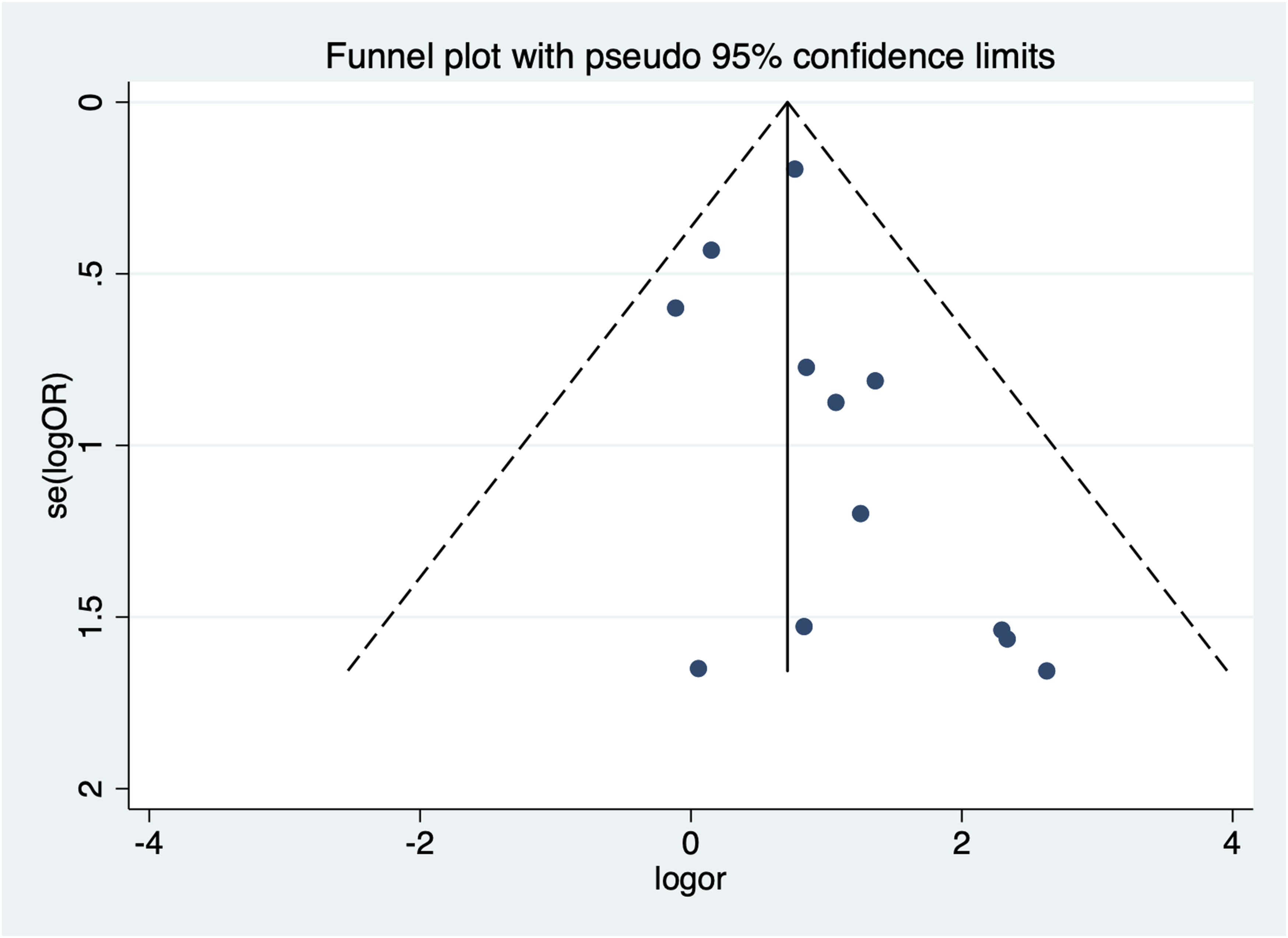
Discussion
Due to its minimal impact on the paraspinal muscles, lateral lumbar interbody fusion (LLIF) has been increasingly utilized in the treatment of various degenerative lumbar conditions.27-29 LLIF allows for the placement of larger fusion devices through a lateral approach while preserving the posterior spinal structures.18,19 Therefore, some spine surgeons believe that standalone LLIF is sufficient to achieve stabilization of the operative segment and fusion, potentially avoiding the need for additional posterior fixation. However, other studies have indicated that standalone LLIF is associated with a higher incidence of fusion cage subsidence, which could impact the indirect decompression effect and fusion quality. 30 To address this controversy, we conducted this study.
Fusion rate is a crucial measure of the effectiveness of LLIF treatment, as fusion failure (non-union or pseudarthrosis) can impact surgical outcomes and patient quality of life. The presented meta-analysis demonstrates that the fusion rate in the stand-alone group is significantly lower than in the additional fixation group, consistent with the results of a systematic review by Manzur et al. 6 This discrepancy in fusion rates can be attributed to several factors. In the standalone LLIF group, the absence of supplementary posterior fixation may lead to insufficient stabilization of the vertebral segments, resulting in micro-movements that hinder the fusion process. In contrast, the additional posterior fixation in the instrumentation group provides enhanced mechanical stability, which promotes a more conducive environment for bone healing and fusion. 31 Additionally, biomechanical studies have shown that posterior fixation can effectively distribute the mechanical loads across the fusion site, reducing the risk of graft micromotion and subsequent non-union. 32 Patient-specific factors also play a critical role in influencing fusion rates. Factors such as patient age, bone density, and the presence of comorbidities like osteoporosis can significantly affect the fusion outcome. In patients with poor bone quality, the standalone LLIF approach might not provide sufficient stability to support successful fusion, whereas the additional posterior instrumentation can compensate for these deficiencies. Furthermore, surgical technique and the choice of graft material are crucial determinants of fusion success. Autografts, allografts, and synthetic graft materials each have different properties that can impact the rate and quality of fusion. The use of osteoinductive materials in conjunction with posterior instrumentation may further enhance fusion rates by promoting new bone formation. 33 While both standalone and additional fixation groups achieved satisfactory fusion rates in this study, the addition of posterior fixation significantly enhances the likelihood of successful fusion. It’s important to note that while the study provides valuable insights, the discussion seems to be truncated and not fully expanded.
Spine surgeons can utilize LLIF to place fusion devices with larger sizes and anterior lordotic angles, thereby restoring intervertebral disc height, segmental lordosis, and lumbar lordosis. This approach indirectly decompresses nerves and helps in reconstructing the spinal alignment. Studies suggest that regardless of whether additional posterior fixation is performed, patients undergoing LLIF can achieve satisfactory radiographic outcomes. However, it’s been observed that the standalone LLIF group tends to have poorer maintenance of corrective radiographic parameters during follow-up periods.17,21,22 The findings of this study support previous research, indicating that the improvement in intervertebral disc height and segmental lordosis from preoperative to the last follow-up is significantly smaller in the standalone group compared to the additional fixation group. This phenomenon might be related to the higher rate of fusion cage subsidence observed in the standalone group.
Fusion cage subsidence is an imaging complication that’s associated with the loss of the effects of indirect decompression and spinal alignment reconstruction. 34 This phenomenon is often the result of multiple factors working together. Previous research has shown that inadequate fusion cage size, lateral fixation, intraoperative damage to bony endplates, as well as patient-related factors such as advanced age, obesity, and osteoporosis, can all contribute to an increased risk of fusion cage subsidence.19,20,22 Several mechanisms can explain why these factors contribute to subsidence. Firstly, an inadequate fusion cage size might fail to provide sufficient support to the vertebral endplates, leading to localized stress concentrations that promote endplate collapse. Secondly, improper positioning or orientation of the cage can exacerbate these stress concentrations, particularly in the absence of lateral fixation which would otherwise help to stabilize the construct. Thirdly, intraoperative damage to the bony endplates can weaken the structural integrity of the vertebral bodies, making them more susceptible to subsidence under the physiological loads experienced postoperatively. 35 Therefore, in cases where these risk factors are present, the addition of posterior fixation can help distribute the stress on the endplates and enhance the stability of the operated segments. Posterior fixation works by providing additional support and stabilization to the vertebral column, thereby reducing the mechanical load transmitted through the fusion cage alone. This distributed load can help to mitigate the risk of subsidence by ensuring that the stress on the endplates remains within tolerable limits. 36
Moreover, the meta-analysis sheds light on the differential effects of standalone vs instrumented LLIF on clinical outcomes such as pain relief and functional recovery, measured by VAS and ODI scores. While both techniques provide significant improvement postoperatively, the addition of instrumentation appears to offer a marginal yet clinically significant advantage in terms of maintaining these improvements long-term. The need for reoperation due to complications such as pseudarthrosis, hardware failure, or adjacent segment disease is notably higher in the standalone LLIF group. This underscores the importance of considering patient-specific factors and the potential long-term benefits of additional fixation, especially in populations at higher risk for mechanical failure or those with challenging anatomical conditions.
This study has several limitations: (1) Due to the limited research available on the effects of additional posterior fixation on the efficacy of LLIF for degenerative lumbar diseases, we were unable to gather a sufficient number of articles specifically focusing on individual LLIF techniques. (2) Most studies lacked information on pre-existing patient comorbidities, which could influence the accuracy of our study results. (3) The limited number of studies prevented us from conducting subgroup analyses based on patient disease types.
In summary, both standalone LLIF and LLIF with additional posterior fixation are effective in improving clinical outcomes for patients with degenerative lumbar diseases. Compared to LLIF with additional posterior fixation, standalone LLIF is more prone to fusion cage subsidence, resulting in lower fusion rates, poorer maintenance of indirect decompression effects, and higher revision rates. Appropriate patient selection is crucial for the success of both procedures. For patients with high risks of fusion cage subsidence, LLIF with additional posterior fixation might be a better choice. When patients are suitable candidates for standalone LLIF, the use of larger fusion cages should be considered.
Footnotes
Authors’Contributions
XiaoCheng Zhou conceived the manuscript, Qiujun Zhou and XiaoCheng Zhou wrote the manuscript, Xiaoliang Jin and Jinjie Zhang participated in literature review and drawing, Qiujun Zhou and Zhoufeng Song participated in the revision of the article. Zhoufeng Song read and approved the final article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent for Publication
All of the authors are aware of and agree to the content of the paper and their being listed as a co-author of the paper.
Data Availability Statement
The datasets are available from the corresponding author on reasonable request.