
Abstract
Study Design
Retrospective study.
Objective
To compare clinical outcomes, radiographic evaluations including bony union rate and incidence of osteoporotic vertebral fractures (OVFxs), and perioperative complications following posterior lumbar interbody fusion (PLIF) between patients ≥80 years of age and those <80 years.
Methods
Ninety-six patients ≥70 years old who underwent PLIF were reviewed. We divided the patients into the two age groups, ≥80 group (n = 19) and <80 group (n = 77), and compared the clinical outcomes using Japanese Orthopaedics Association (JOA) scores and the Short-Form Health Survey (SF-36). We also evaluated bony union and the incidence of OVFxs in the both groups.
Results
The JOA score improved 47.6% in the ≥80 group and 49.1% in the <80 group. There were no significant differences between the two groups. Only the bodily pain component of the SF-36 improved significantly in the ≥80 group, and seven of eight components (exception was general health) improved significantly in the <80 group. Bony union rate was significantly superior in the <80 group (94.8%) compared with that of the ≥80 group (73.7%, p = 0.013). OVFx prevalence and incidence were not significantly different between the two groups, although postoperative OVFx worsened the JOA score improvement in the ≥80 group (38.8%, p = 0.02).
Conclusions
The present study indicated that surgical outcomes of PLIF in patients ≥80 years were comparable to those < 80 years. However, bony union rate was significantly lower and postoperative OVFx worsened the clinical outcomes in patients ≥80 years.
Keywords
Introduction
Posterior lumbar interbody fusion (PLIF), which was first described by Cloward, 1 has been indicated for the patients who have neurologic claudication and segmental spinal instability. Several authors have already reported that PLIF and other lumbar interbody arthrodesis can provide good surgical outcomes. 2 , 3 , 4 However, to our knowledge, there is little written on these procedures for patients in the eighth and ninth decades of life, despite the fact that the application of lumbar arthrodesis for lumbar degenerative disease in elderly patients has become substantially more widespread over the past decade due to the lengthening life expectancy. 5 , 6
One of the concerns about surgical interventions in elderly patients is the potential risk associated with their comorbidities and osteoporosis. Severe comorbidities may lead to several perioperative complications, and osteoporosis would impact the bony union and incidence of osteoporotic vertebral fractures (OVFxs) during follow-up. Also, alleviation of their neurologic symptoms with PLIF does not always lead to maintenance or improvement in the patient's quality of life. Spinal surgeons are therefore in a quandary about whether decompression with or without fusion is better for elderly patients. It is important to study the surgical outcomes and complications following PLIF in patients ≥80 years of age.
The purpose of this study was to compare clinical outcomes, radiographic evaluations including bony union rate and incidence of OVFxs, and perioperative complications following PLIF between patients ≥80 years of age and those <80 years. We hypothesized that clinical outcomes and complications of PLIF would be comparable in patients ≥80 years of age and those <80 years; on the other hand, the bony union rate might be lower and the incidence of OVFxs higher in the ≥80 years of age group, and the OVFx incidence could influence the clinical outcomes in both age groups.
Materials and Methods
Patient Population
A total of 105 patients who were >70 years of age and who underwent PLIF for lumbar degenerative disease at our institution from 2008 to 2011 were reviewed. Informed consent was obtained from all participants, and the institutional review board at the Osaka City Graduate School of Medicine approved this study (approval number: 3170). Therefore, this study was performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
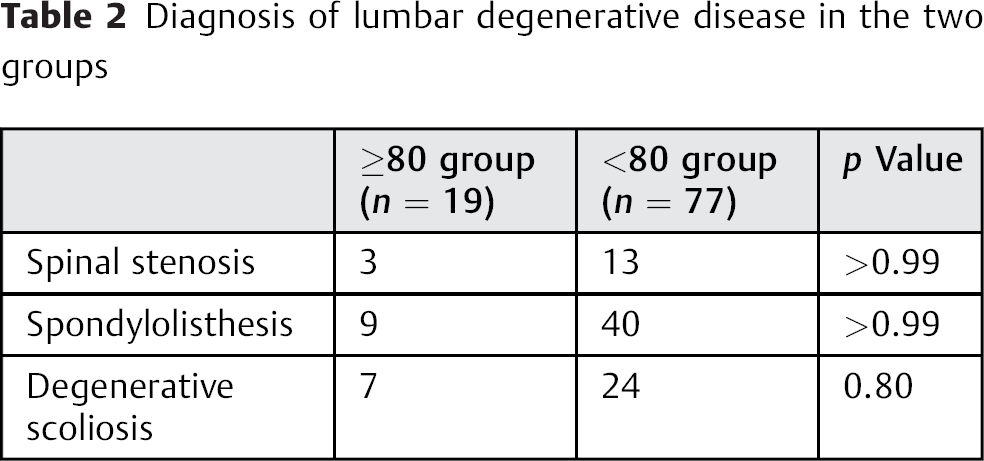
Ninety-six of the 105 patients were followed for a minimum of 2 years and were evaluated radiographically and clinically. These 96 patients were enrolled in this study, and the follow-up rate was 91.4%. We divided the patients into two groups according to age: those ≥80 years of age (≥80 group: n = 19; mean age 82.2 years, range 80 to 91 years) and those < 80 years of age (<80 group: n = 77; mean age 74.6 years, range 70 to 79 years). Of the 96 patients, there were 65 women and 31 men, with no significant difference between the two age groups. The mean follow-up of the two groups was 39.0 months (24 to 62 months) in the ≥80 group and 41.9 months (24 to 74 months) in the <80 group. The mean numbers of fused levels were 1.42 and 1.29, respectively. In the ≥80 group, the number of fused cases in L2–L3, L3–L4, L4–L5, L5–L6, L5–S1 was 2, 22, 57, 2, 16 cases, and in the <80 group, 2, 8, 13, 1, 3 cases, respectively. Seven patients in the ≥80 group (37%) had a history of previous decompression at the fusion levels. This rate was higher than that of the <80 group (12 cases, 16%). There was no significant difference between the two groups in patient demographics, which are summarized in Table 1. The number of lumbar disease diagnoses in the two groups was quite similar (Table 2).
Patients demographics of the two groups
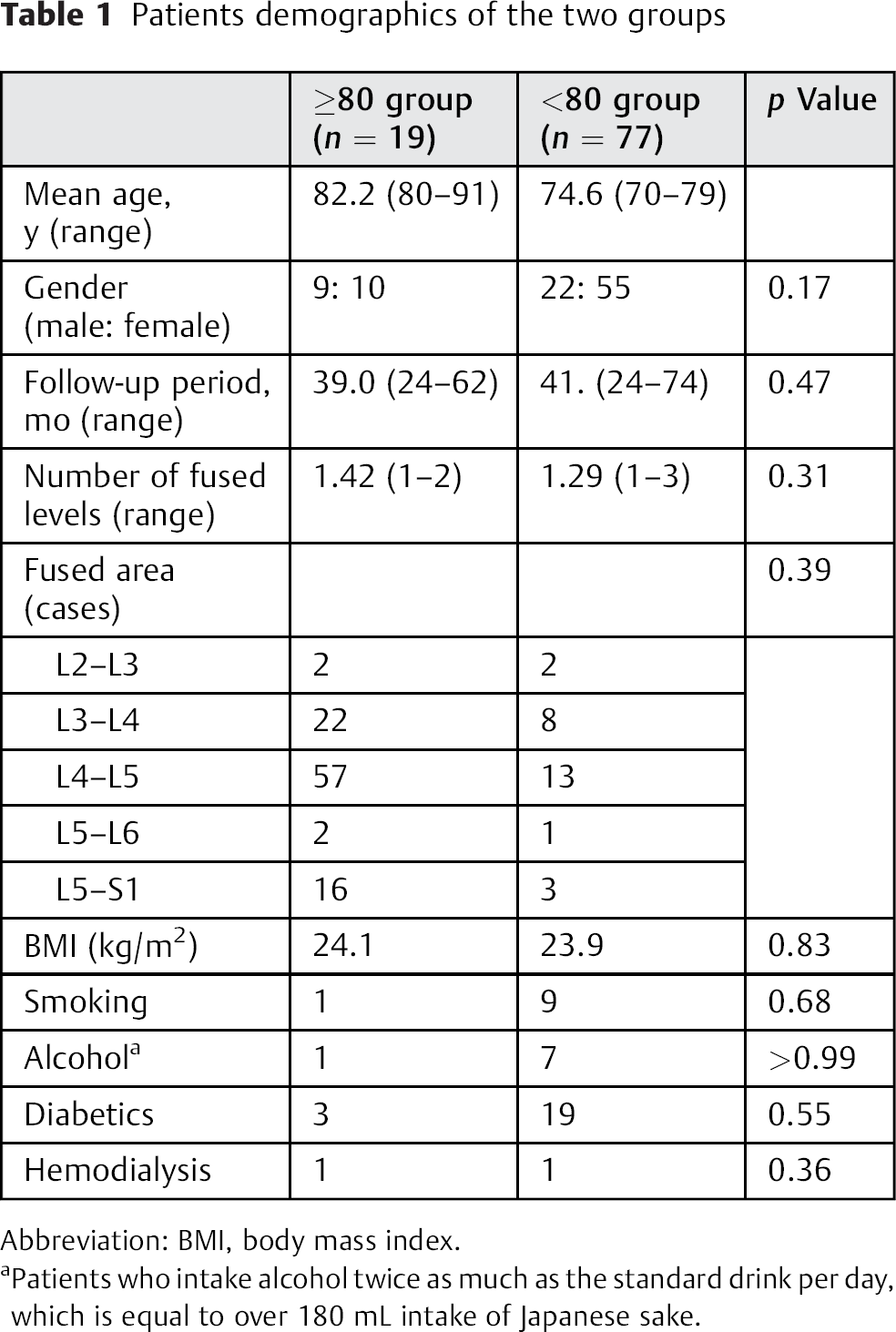
Abbreviation: BMI, body mass index.
Patients who intake alcohol twice as much as the standard drink per day, which is equal to over 180 mL intake of Japanese sake.
Diagnosis of lumbar degenerative disease in the two groups
Surgical Indications of PLIF
We performed PLIF in patients who complained of leg pain, neurogenic claudication, and low back pain due to the spinal canal stenosis with segmental spinal instability or spondylolisthesis or degenerative lumbar scoliosis. All patients underwent PLIF using pedicle screw and rod system (Fig. 1). Two open box cages were placed with morselized local bone graft into the disk space. The indications for PLIF were the following:
Segmental spinal instability shown in the bending films; segmental kyphosis of more than 5 degrees or anterior translation was more than 3 mm
Grade 2 spondylolisthesis in the Meyerding grading system 7
Segmental scoliotic disk wedging angle more than 5 degrees or lateral slip more than 3 mm in standing anteroposterior X-ray.
Cobb angle more than 20 degrees in standing anteroposterior X-ray
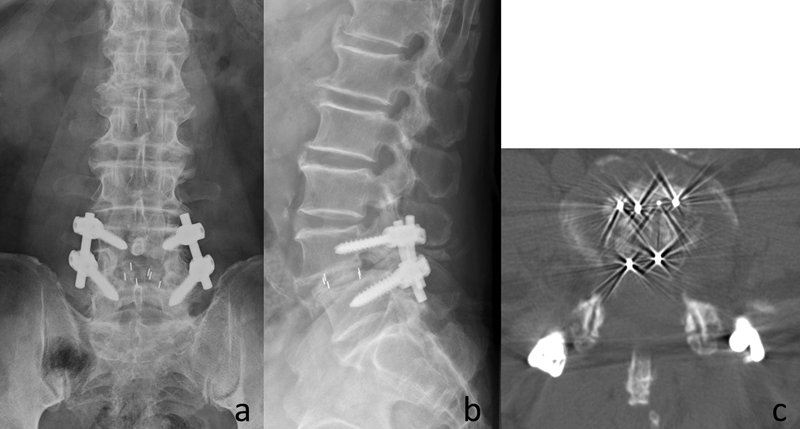
A 76-year-old man treated with a L4–L5 posterior lumbar interbody fusion for spondylolisthesis. (a) X-ray, anteroposterior view, taken postoperatively. (b) X-ray, lateral view, taken postoperatively. (c) Computed tomography, axial view, at fused level; two box cages were placed with local bone graft.
Exclusion Criteria
We excluded the patients who met the following conditions:
Prevalent OVFxs at the fusion levels
Previous fusion surgery at the fusion level
Any previous OVFx in the thoracic or lumbar spine that met the grade 2 or in semiquantitative (SQ) technique 8
Clinical Outcomes
We evaluated clinical outcomes with the Japanese Orthopaedics Association (JOA) score for low back pain and the health-related quality of life (HRQOL) with the Short Form-36 Health Survey (SF-36) Japanese edition, before surgery and at the latest follow-up. 9 The maximum JOA score is 29 points, based on three subjective symptoms, three clinical signs, activities of daily living, and bladder dysfunction (Table 3). Improvement of the JOA score was calculated using the formula demonstrated by Hirabayashi et al. 10 The SF-36 has eight health components that were analyzed: physical functioning; role physical; bodily pain (BP); general health (GH); viability; social functioning; role emotional (RE); mental health (MH). 9 Surgical data, including operation time and estimated blood loss, was also evaluated.
JOA score for low back pain
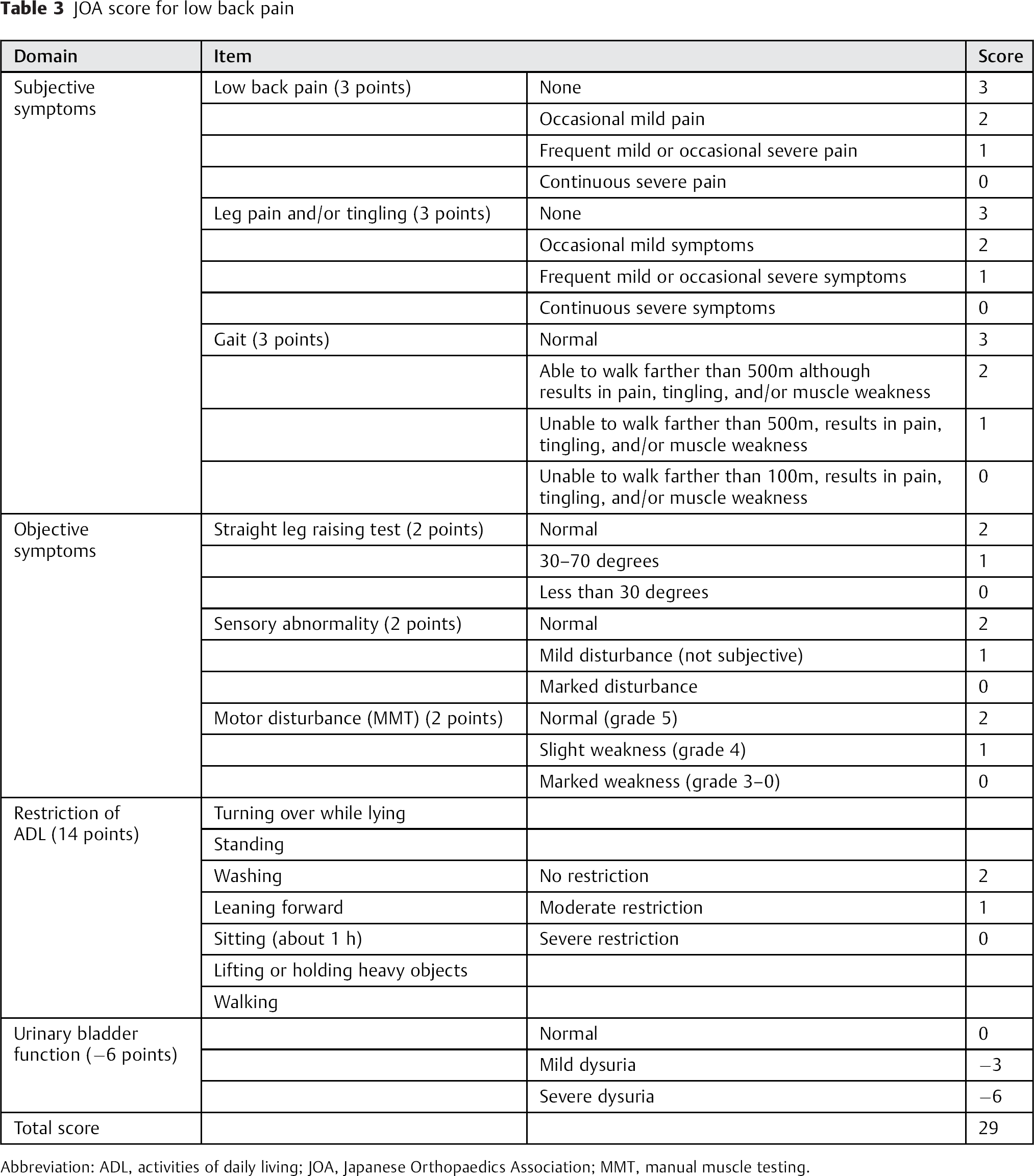
Abbreviation: ADL, activities of daily living; JOA, Japanese Orthopaedics Association; MMT, manual muscle testing.
Radiographic Evaluations
Bony union was assessed using the criteria described by Rothman and Glenn on multiplanar reconstruction computed tomography images, and the prevalence of OVFxs were investigated with standing plain X-rays. 11 OVFx was also evaluated with the SQ grading technique proposed by Genant and colleagues, and we defined OVFx as matching SQ grade 2 or 3 in this study. 8 Bony union was evaluated 2 years after surgery, and OVFx was investigated before surgery and 2 years after surgery.
Complications
The perioperative complications were investigated using the medical charts in each group. The medical complications, including anemia and cardiopulmonary, gastrointestinal, or urinary tract adverse effects during the perioperative period, and reduction of their own comorbidity were evaluated. Additionally, surgery-specific complications were evaluated including dural tear, hematoma, neurologic deficits, infection, implant failure, nonunion, and adjacent segmental degeneration. We classified these events into minor or major complications according to the modified World Health Organization Recommendations for Grading of Acute and Subacute Toxic Effects. 6 12 Blood infusion, additional antibiotics, treatment by another department, revision surgery, and additional surgery associated with any complications were classified as major complications.
Statistical Analysis
Statistics were analyzed using the paired t test and Fisher exact test. Probability values < 0.05 were considered statistically significant.
Results
Operation Data and Clinical Outcomes
The mean operative time was 274 minutes in both groups. The mean blood loss was estimated to be 411 g in the ≥80 group and 409 g in the <80 group. There was no significant difference between the two groups (Table 4).
Operation data and evaluation of the JOA score of the two group
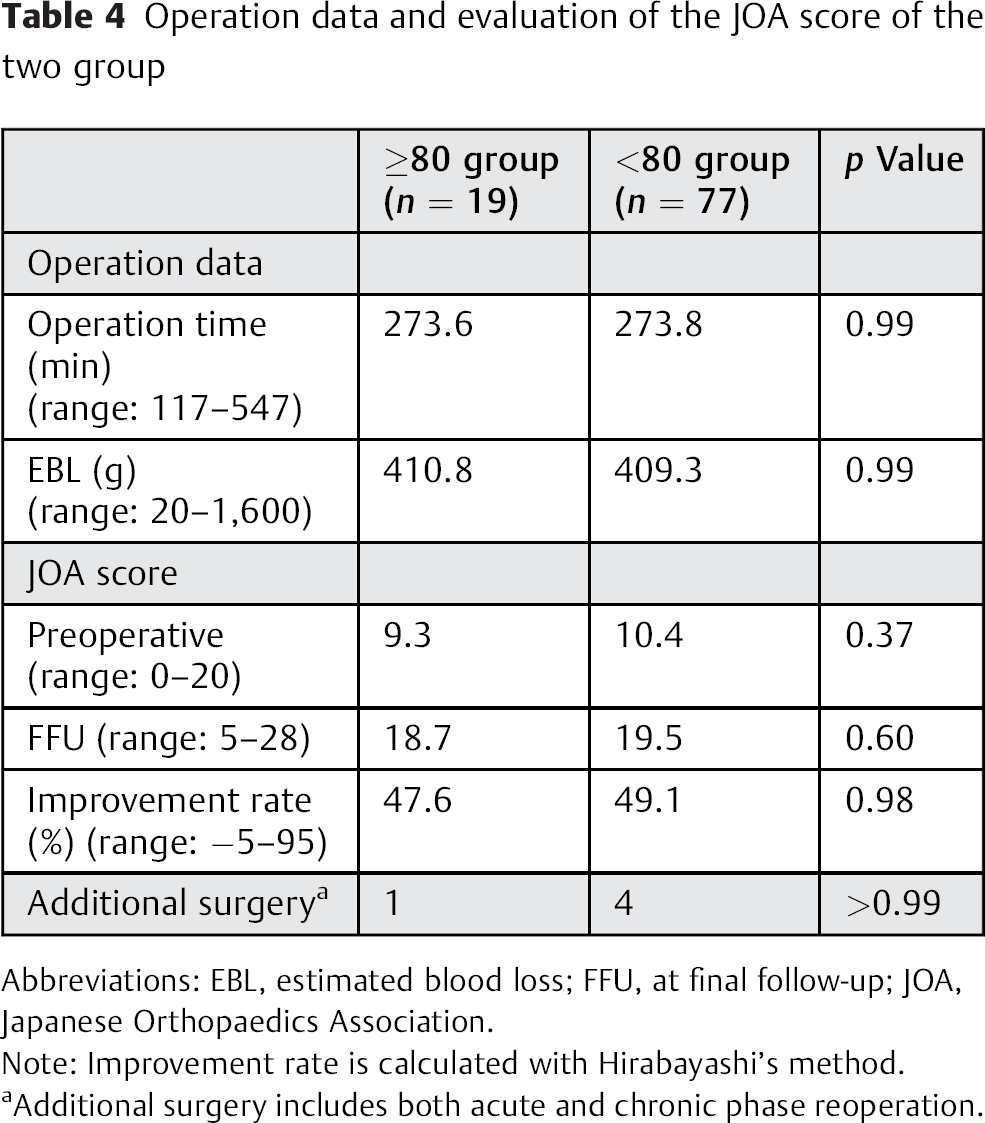
Abbreviations: EBL, estimated blood loss; FFU, at final follow-up; JOA, Japanese Orthopaedics Association.
Note: Improvement rate is calculated with Hirabayashi's method.
Additional surgery includes both acute and chronic phase reoperation.
The mean JOA score for the ≥80 group was 9.3 before surgery and improved to 18.7 at the latest follow-up. The mean JOA score in the <80 group was 10.4 before surgery and improved to 19.5 at the latest follow-up. The JOA score improvement rates were 47.6 and 49.1%, respectively (Table 4). There was no significant difference between the two groups (p = 0.98). The SF-36 evaluation revealed no significant differences between the two groups for all components before surgery. Only the BP component improved significantly in the ≥80 group. In contrast, 7 of the 8 components (the exception was GH) improved significantly at the final follow-up in the <80 group. The RE and MH components of the <80 group were significantly superior to those of the ≥80 group at the final follow-up (Fig. 2).
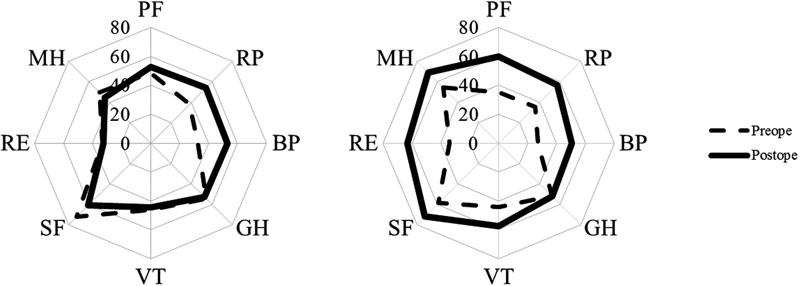
The comparison of the two groups with eight components in Short Form-36 Health Survey (left: ≥80 group, right: <80 group). Abbreviations: BP, bodily pain; GH, general health; MH, mental health; PF, physical functioning; RE, role emotional; RP, role physical; SF, social functioning; VT, viability.
Radiographic Evaluation
Multiplanar reconstruction computed tomography images 2 years after surgery showed bony union in 14 of the 19 patients in the ≥80 group and in 73 of the 77 patients in the <80 group. The bony union rate was 73.7% in the ≥80 group and 94.8% in the <80 group. There was a significant difference between the two groups (p = 0.013). Two cases of spinal stenosis, 2 of spondylolisthesis, and 1 of degenerative scoliosis in the ≥80 group and 1 case of spinal stenosis, 2 of spondylolisthesis, and 1 of degenerative scoliosis in the <80 group were diagnosed as nonunion.
Five patients (26%) in the ≥80 group and 13 (17%) in the <80 group had newly identified OVFxs postoperatively (PO OVFx), and there were no significant differences (p = 0.52). However, in the ≥80 group, PO OVFxs significantly impacted the JOA score improvement, and those patients who had PO OVFx did not show substantial JOA score improvement (with PO OVFx versus without OVFx = 38.8 versus 55.0%, respectively; p = 0.02). By contrast, there were no significant differences in the JOA score improvement with or without PO OVFx in the <80 group (44.4 and 50.5%, p = 0.47).
The SQ analysis of OVFxs was also evaluated and is summarized in Table 5. No significant differences were noted between the two groups regarding the numbers of OVFx.
Thoracic and lumbar OVFxs of the two groups
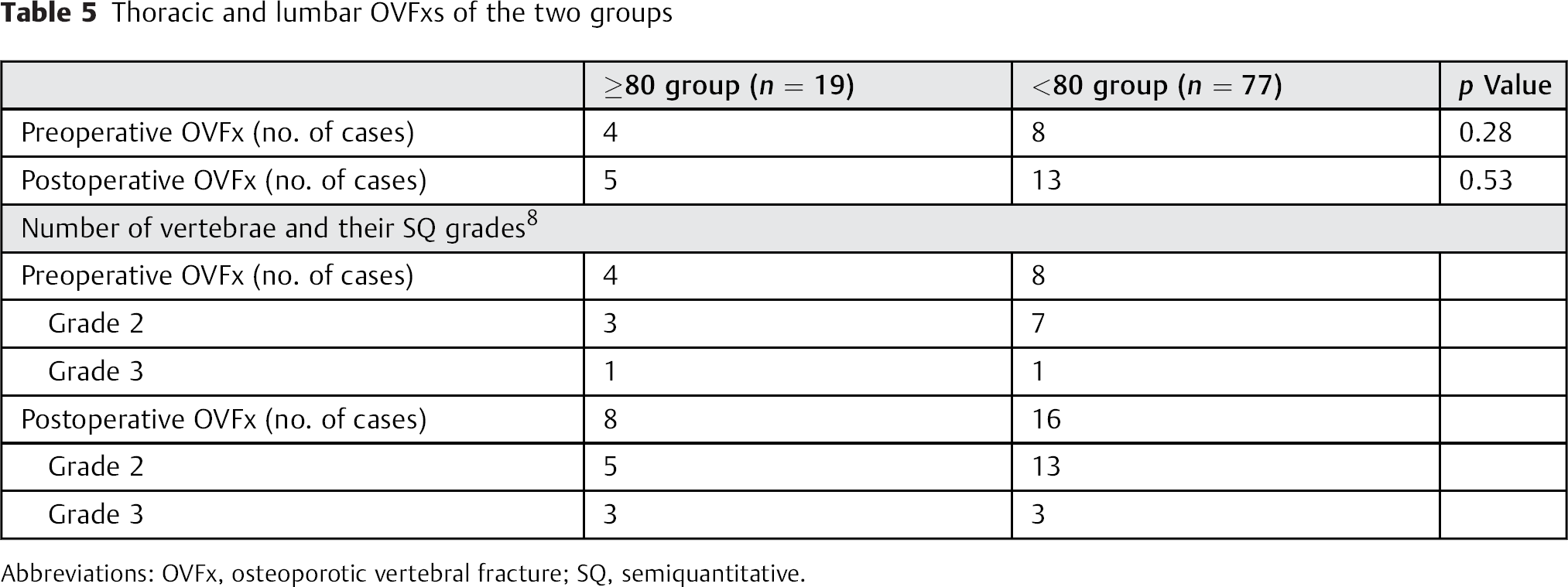
Abbreviations: OVFx, osteoporotic vertebral fracture; SQ, semiquantitative.
Complications
Perioperative medical complications were identified in 4 patients (21%) in the ≥80 group and 12 patients (16%) in the <80 group. Likewise, surgery-specific complications occurred in 7 patients (37%) in the ≥80 group and 15 patients (19%) in the <80 group. Except for nonunion, surgery-related complications occurred in 3 patients (16%) in the ≥80 group and 11 patients (14%) in the <80 group. In contrast, major complications were noted in 4 patients (16%) in the ≥80 group and 7 patients (9%) in the <80 group. There were no significant differences between the two groups. Additional spinal surgeries were required in 1 patient in the ≥80 group and in 4 patients in the <80 group. Two reoperations in the <80 group were needed because of nonunion. This data is summarized in Table 6. There were no life-threatening complications in either group.
Complications of the two groups
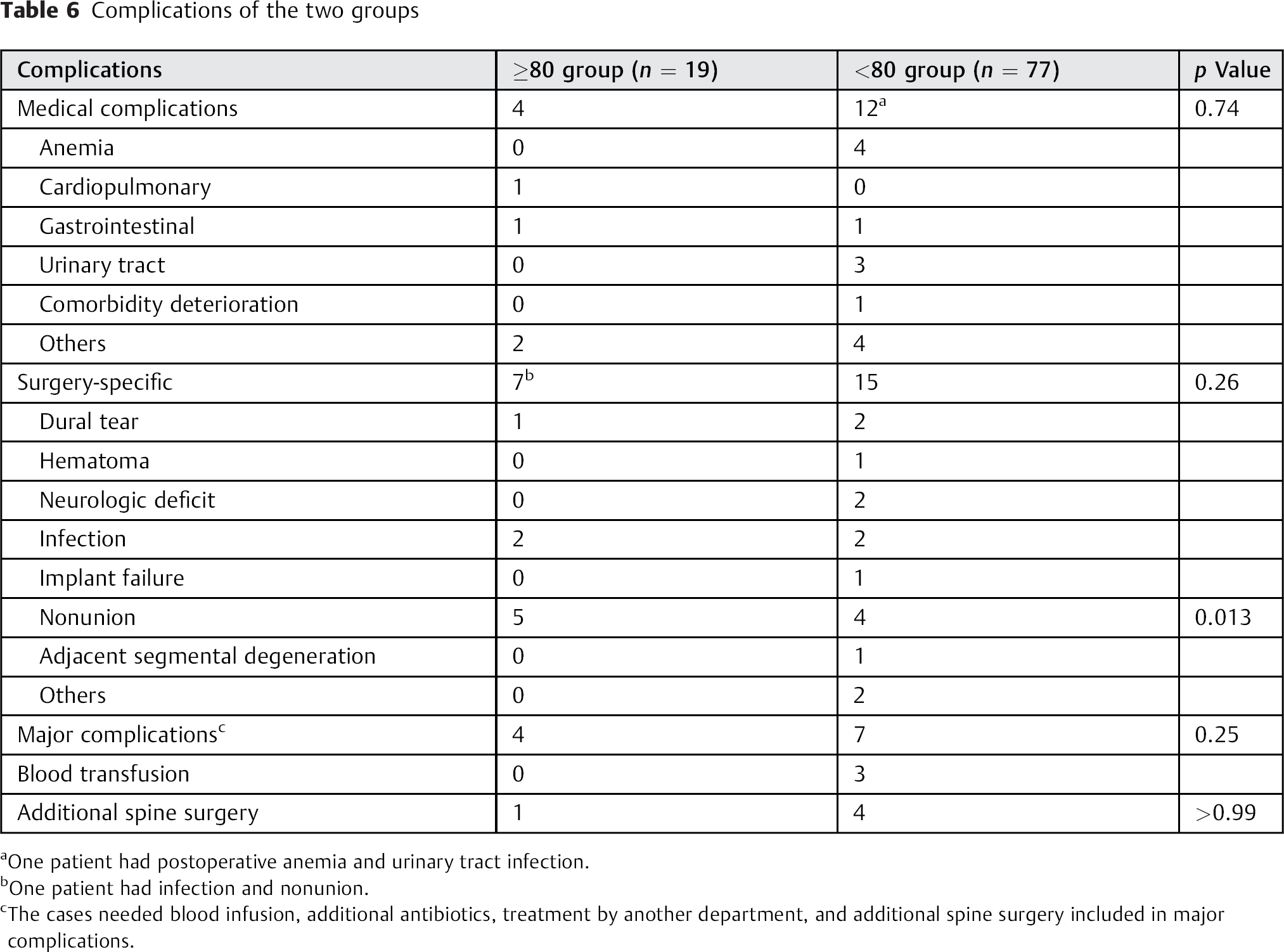
One patient had postoperative anemia and urinary tract infection.
One patient had infection and nonunion.
The cases needed blood infusion, additional antibiotics, treatment by another department, and additional spine surgery included in major complications.
Discussion
Several authors reported that lumbar arthrodesis with PLIF could provide good clinical outcomes for elderly patients with lumbar spinal canal stenosis. 6 , 13 , 14 , 15 , 16 Okuda et al reported that the surgical outcomes of PLIF were comparable in patients ≥70 years of age and those <70 years of age. 13 Glassman et al evaluated the HRQOL data (SF-36) following lumbar posterolateral fusion in patients ≥65 years of age, and they showed improvement in physical component, which was similar to that of the younger patients. 6 Despite the good clinical outcomes, the authors also indicated that lumbar arthrodesis for elderly patients was associated with a relatively high rate of complications. Most previous studies of lumbar arthrodesis were thought to be inadequate regarding the patients’ ages, which meant that 65 or 70 years of age was not “definitively” elderly. In Japan, it is reported that the remaining life expectancy of men at 80 years of age is 8.6 years, and for women it is 11.5 years. 17 Likewise, in the United States, the remaining life expectancy of 75-year-old men is 11.0 years, and for women it is 12.9 years. 14 , 18 Recently, Rihn and colleague reported operative outcomes in an octogenarian population. 19 They included a large number of the as-treated patients with lumbar degenerative disease, and they concluded that operative treatment offered a significant benefit over conservative treatment in their population. As noted, they compared the SF-36 BP and physical functioning subdomains in subjects at least 80 years of age and in subjects younger than 80 years. However, they mixed lumbar decompression only and lumbar decompression with fusion as operatively treated patients. Moreover, they did not assess all subdomains in the SF-36.
In this study, we evaluated the clinical outcomes and HRQOL data of PLIF for patients older than 80 years old. We found that the JOA score improvement rates were 47.6% in the ≥80 group and 49.1% in the <80 group. There was no significant difference between the two groups. For the SF-36, only the BP component improved significantly in the ≥80 group, whereas 7 of the 8 components (GH being the only exception) improved significantly in the <80 group. Comparative analysis indicated that the RE and MH components were significantly superior in the ≥80 group compared with those in the <80 group. The reason of the gap between JOA score and SF-36 subdomain improvement in the ≥80 group might be the lack of the assessment for social and mental status in the JOA score. The incidence of complications was not significantly different between the two groups, although patients in the ≥80 group had a higher tendency of complications. Therefore, our study indicated that PLIF could provide comparable clinical outcomes and adequate pain relief for the patients ≥80 years of age with acceptable perioperative complications; however, spinal surgeon have to recognize that postoperative HRQOL of the patients ≥80 years of age cannot improve in comparison with the patients <80 years of age.
Bony union is one of the most important outcomes following lumbar arthrodesis. In some previous studies, the bony union rates following PLIF were reported to be 85 to 100%. 13 , 15 , 20 In this study, the rate of bony union in the ≥80 group was 73.7%, which was significantly lower than that of the <80 group (94.8%). Considering both previous reports and our data, aging would be one of the possible risk factors of nonunion. In the future, we should clarify the relationship between age, bone mineral density, and bone union rate in these populations. There was some discrepancy between the clinical outcomes evaluated by JOA score and the bony union rate. However, a previous report noted that the bony union rate was not associated with clinical outcome during the first 2 to 3 postoperative years. 21 Longer follow-ups are necessary to evaluate the impact of nonunion on the clinical outcome.
The postoperative incidence of OVFx in the ≥80 group (26%) was relatively high, but was not significantly different compared with that in the <80 group (17%). Toyone et al reported that 15% patients over 55 years of age had either adjacent or nonadjacent vertebral fracture after posterior lumbar fusion. 22 Our data is thought to be consistent with their data. On the other hand, postoperatively acquired OVFx significantly worsened the JOA score improvement in the ≥80 group. OVFx causes severe low back pain and neurologic compromise, and it also worsens the quality of life and increases mortality risk. 23 , 24 Our results indicate that adequate treatment for osteoporosis could reduce the incidence of postoperative OVFx and prevent the deterioration of the clinical outcomes of PLIF in elderly patients. Recently, Ohtori et al reported that teriparatide improved the bony union rate after spinal arthrodesis. 25 Using teriparatide may be beneficial to improve the clinical outcome of elderly patients following PLIF.
There were some limitations to this study. First, the study cohort consisted of small number of patients ≥80 years of age and a relatively short follow-up. We should continue to investigate the clinical and radiographic outcomes following PLIF in patients ≥80 years of age. Second, we did not evaluate the sagittal spinal balance in this cohort, and we could not investigate the relationship between clinical outcome or bony union rate and sagittal balance. Third, we did not evaluate bone mineral density for all the patients, and so we could not evaluate the relationship between nonunion and bone mineral density.
In conclusion, we demonstrated that clinical outcomes of PLIF evaluated by JOA score in patients ≥80 years of age were comparable to those of patients < 80 years of age in midterm follow-up. However, a higher rate of nonunion was found in patients ≥80 years of age, and OVFxs incidence worsened their latest clinical outcomes. Treatment of osteoporosis might be beneficial to prevent the deterioration of the clinical outcomes and to deal with activities of daily living following PLIF.
Disclosures
Kazunori Hayashi: none
Akira Matsumura: none
Sadahiko Konishi: none
Minori Kato: none
Takashi Namikawa: none
Hiroaki Nakamura: none