
Abstract
Study Design:
Prospective cohort.
Objective:
To investigate whether intraoperative neuromonitoring (IONM) positive changes affect functional outcome after surgical intervention for myeloradiculopathy secondary to cervical compressive pathology (cervical compressive myelopathy).
Methods:
Twenty-eight patients who underwent cervical spine surgery with IONM for compressive myeloradiculopathy were enrolled. During surgery motor-evoked potential (MEP) and somatosensory evoked potential (SSEP) at baseline and before and after decompression were documented. A decrease in latency >10% or an increase in amplitude >50% was regarded as a “positive changes.” Patients were divided into subgroups based on IONM changes: group A (those with positive changes) and group B (those with no change or deterioration). Nurick grade and modified Japanese Orthopaedic Association (mJOA) score were evaluated before and after surgery.
Results:
Nine patients (32.1%) showed improvement in MEP. The mean preoperative Nurick grade and mJOA score of group A and B were (2.55 ± 0.83 and 11.11 ± 1.65) and (2.47 ± 0.7 and 11.32 ± 1.24), respectively. The mean postoperative Nurick grade of groups A and B at 6 months was 1.55 ± 0.74 and 1.63 ± 0.46, respectively, and this difference was not significant. The mean postoperative mJOA score of groups A and B at 6 months was 14.3 ± 1.03 and 12.9 ± 0.98, respectively, and this difference was statistically significant (P = .011). Spearman correlation coefficient showed significant positive correlation between the IONM change and the mJOA score at 6 months postoperatively (r = 0.47; P = .01).
Conclusion:
Our study shows that impact of positive changes in MEP during IONM reflect in functional improvement at 6 months postoperatively in cervical compressive myelopathy patients.
Introduction
Cervical compressive myelopathy (CCM) is the most common cause of spinal cord dysfunction in adults and is produced by mechanical compression of the spinal cord secondary to disc herniation, spondylosis, and ossification of the posterior longitudinal ligament.1-7 Patients with CCM with mild symptoms are often managed conservatively. Surgical decompression is increasingly recommended as the treatment strategy for the full spectrum of myelopathy severity.
There are studies that show that preoperative magnetic resonance imaging (MRI) spinal cord signal change is a predictor of postoperative functional outcome following CCM decompression.8-10 However, certain studies are against this hypothesis.11,12
In the recent decades, many surgeons have been using intraoperative neurophysiological monitoring (IONM) in spinal surgery to reduce the incidence of postoperative neurological complications. Several established technologies are available, and combined motor-evoked potentials (MEPs) and somatosensory evoked potentials (SSEPs) are considered mandatory for practical and successful IONM.13-16 For many years, only SSEPs were monitored during spinal cord surgeries before MEP techniques were developed. Since the multipulse technique was introduced in the mid-1990s, combined muscle MEP and SSEP monitoring have been routinely used intraoperatively in high-risk spine surgeries. Many authors have reported that combined SSEP/MEP monitoring provided higher sensitivity and higher positive/negative predictive values than single-modality monitoring techniques and that optimal monitoring requires both SSEPs and MEPs.13-16
Current safe spine surgery guidelines recommend multimodal IONM during spinal surgery as a reliable and valid diagnostic adjunct to assess spinal cord integrity. 17 IONM accurately identifies the topography of neural structures and gives real-time alarm to the surgical team about intraoperative surgical insults. Though the role of IONM was initially adopted for deformity correction and intramedullary tumor surgeries, it is now being increasingly used in various high-risk spinal surgeries where the risk of iatrogenic injury to neural structures is considered high.
There is insufficient evidence on the therapeutic relationship between IONM changes during cervical spinal decompressive surgery for cervical spondylotic myelopathy and neurological outcomes. In recent years, we have been utilizing IONM for CCM spine surgeries, and we observed in our practice that the intraoperative transcranial MEP improvement is associated with postoperative neurological recovery. Thus, in this current study, we prospectively assess the effect of IONM changes in predicting postoperative neurological recovery in patients with CCM.
The primary objective of the present study was to investigate whether IONM positive changes can predict functional outcome after surgical intervention for cervical myeloradiculopathy.
Materials and Methods
We prospectively collected data on patients who underwent spinal surgery with IONM for cervical compressive myeloradiculopathy at our center between January 2018 and October 2019 with a minimum of 6-month follow-up. The diagnosis of myeloradiculopathy was made clinically and radiologically on MRI. Patients with CCM in whom baseline effective MEPs were recorded were included in the study. We excluded 5 patients with unreliable or absent MEPs at the start of surgery as these patients are very different from those with effective baseline MEPs from the viewpoint of corticospinal pathway. We routinely use neuromonitoring in all our cases, and this study was categorized as institutional review board exempt, as it has no greater than minimal risk to participants.
During the surgery, patients underwent IONM using MEP and SSEP. MEP and SSEP were checked before and after decompression. A decrease in latency >10% or an increase in amplitude >50% was regarded as “positive change” as documented previously.18,19 Subjects were divided according to the presence of positive changes. Early postoperative outcomes at the end of 1 week postsurgery were assessed for the following functions: motor, sensory, pain, or 15-second grip and release test. 8 Modified Japanese Orthopaedic Association (mJOA) score20,21 and Nurick grading 22 were evaluated before and at 3 months and at 6 months after operation. The neurological improved rate was calculated by the use of the following equation: [(postoperative JOA score − preoperative JOA score)/(18 (full score) − preoperative JOA score) * 100%].23-25
Anesthesia Management
Total intravenous anesthesia with propofol and opioids is our standard protocol whenever SSEP and MEPs are to be monitored intraoperatively. After intravenous induction using injection propofol 2 to 2.5 mg/kg, injection fentanyl 5 to 6 μg/kg, and injection morphine 0.15 mg/kg, the airway was secured and the patient positioned. Maintenance of anesthesia was with an infusion on injection propofol 4 to 6 mg/kg/h titrated to maintain a BIS value (bispectral index) of 45 to 55. A mixture of air and oxygen to provide FiO2 of 0.4 was used. Further doses of analgesics were given as per the patient’s requirement. No muscle relaxant or inhalation agent was used during MEP recording. All patients were kept under normothermic and normotensive conditions intraoperatively.
Statistical Analysis
Data analysis was done using SPSS version 13. All quantitative variables were checked for normal distribution within each category of explanatory variable by using visual inspection of histograms and normality Q-Q plots. Shapiro-Wilk test was also conducted to assess normal distribution. All the quantitative variables were normally distributed except Nurick grading. We used unpaired t test for normally distributed data and Wilcoxon-Mann-Whitney test for nonparametric data to compare the means between the group that showed improvement in MEP and the group that showed no improvement or deterioration in the MEP. The Spearman correlation coefficient was used to ascertain the strength of association. Data was presented as mean ± SD or SEM. P value <.05 was considered statistically difference.
Results
Twenty-eight patients were included in this study. Average follow-up was 14.5 months. No enrolled patients were lost to follow-up. Pathology included cervical spondylotic myelopathy in 20 cases (20/28, 71.5%) and ossification of posterior longitudinal ligament in 8 cases (8/28, 28.5%). Nineteen patients (19/28, 67.8%) had anterior cervical surgery and 9 patients (9/28, 32.2%) had posterior cervical surgery in the form of multilevel laminectomy. All patients were operated for pathology between C3 and C7 levels (Table 1). Anterior cervical surgery was either in the form of discectomy/decompression and fusion (anterior cervical discectomy and fusion [ACDF]) or corpectomy, decompression, and fusion (anterior cervical corpectomy and fusion [ACCF]). Nine cases (32.1%) showed improvement in MEPs, but no change in SSEPs. Eighteen cases (64.3%) demonstrated no change in MEPs or SSEPs compared to baseline findings. Deterioration in MEP was observed in one patient (3.6%). The cohort was divided into group A (9 participants showing improvement in MEPs) and group B (19 participants who showed no change in MEPs compared to baseline or showed deterioration in MEPs).
Patient Characteristics in the 2 Groups.
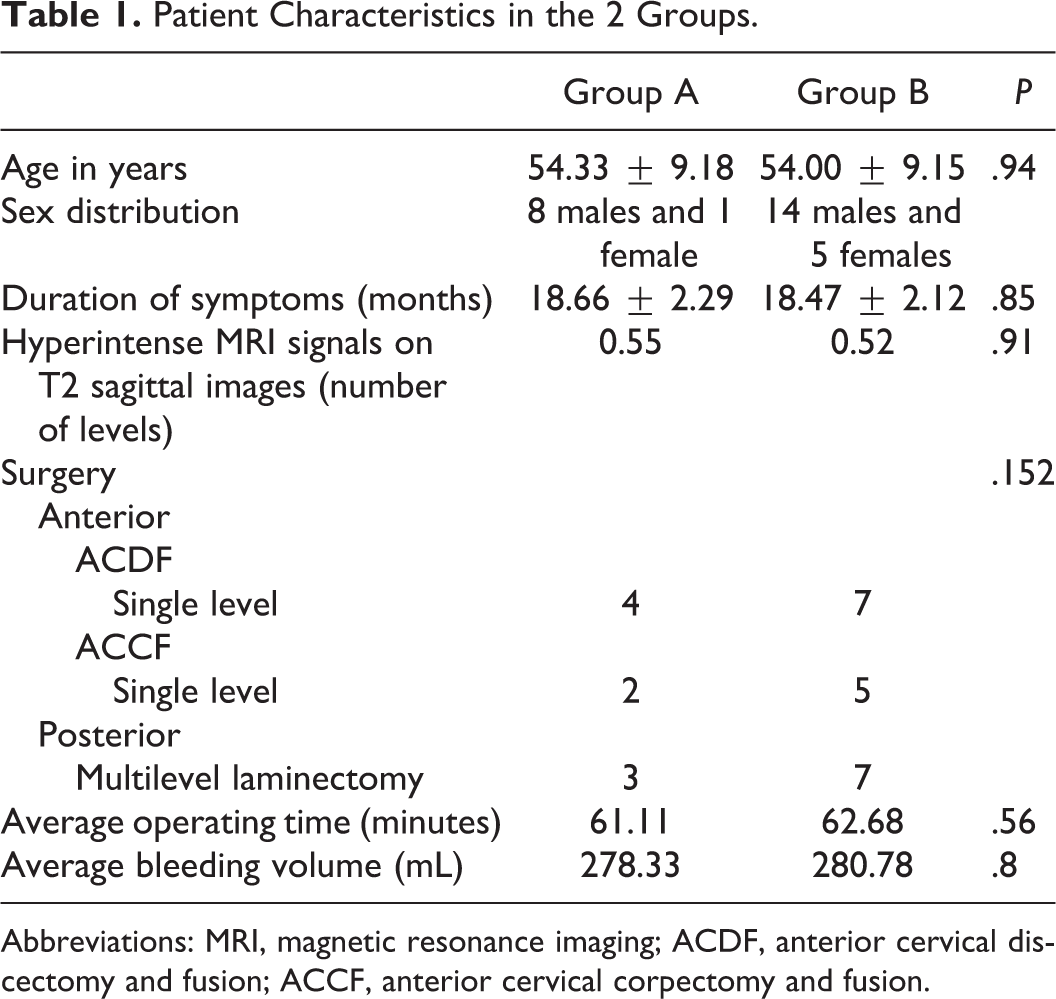
Abbreviations: MRI, magnetic resonance imaging; ACDF, anterior cervical discectomy and fusion; ACCF, anterior cervical corpectomy and fusion.
The mean preoperative Nurick grade and mJOA score of groups A and B were (2.55 ± 0.83 and 11.11 ± 1.65) and (2.47 ± 0.7 and 11.32 ± 1.24), respectively. The mean postoperative Nurick grade of groups A and B at 3 months was 1.8 ± 0.97 and 2.0 ± 0.67, respectively, and this difference was not significant. The mean postoperative Nurick grade of groups A and B at 6 months was 1.55 ± 0.74 and 1.63 ± 0.46, respectively, and this difference was not significant.
The mean postoperative mJOA score of groups A and B at 3 months was 13.1 ± 1.76 and 12.1 ± 1.39, respectively, and this difference was not significant. The mean postoperative mJOA score of groups A and B at 6 months was 14.33 ± 1.03 and 12.89 ± 0.98, respectively, and this difference was statistically significant (P = .011). Spearman correlation coefficient showed significant positive correlation between the intraoperative findings of neurological monitoring and the mJOA score at 6 months postoperatively (r = 0.47; P = .01; Table 2).
Summary Data of mJOA and Nurick Grade of Patients Groups.
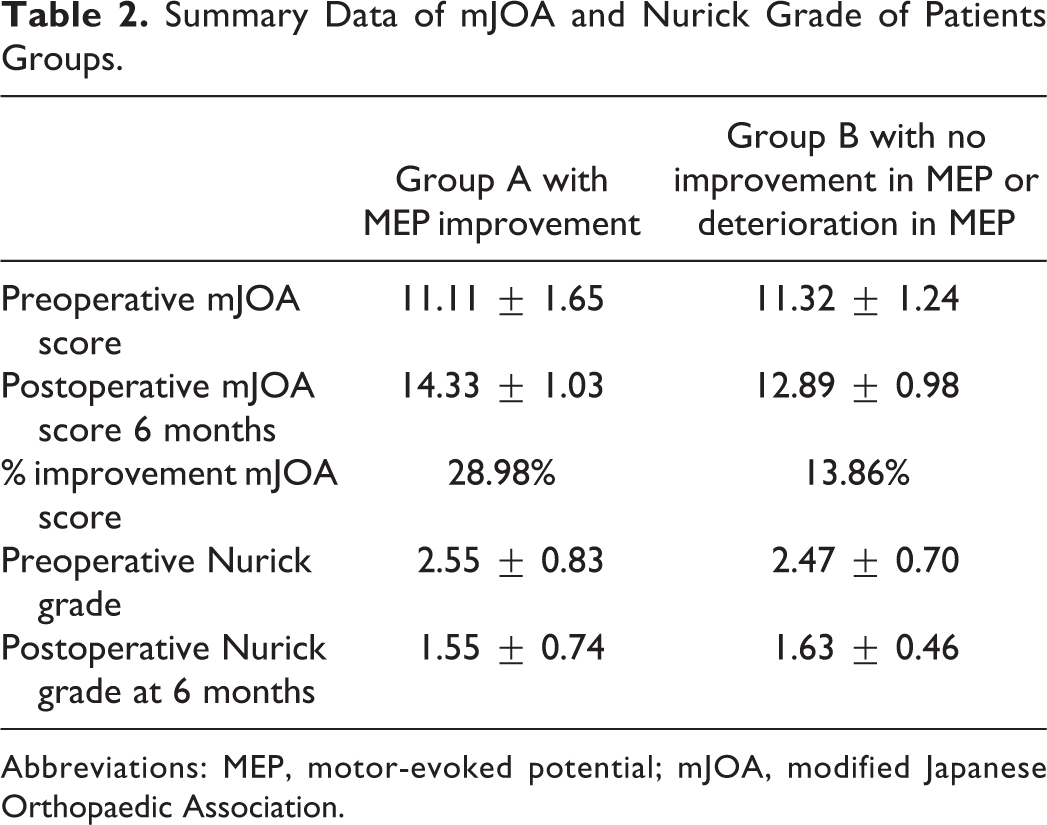
Abbreviations: MEP, motor-evoked potential; mJOA, modified Japanese Orthopaedic Association.
The percentage change in mJOA score in group A at 6 months postoperatively was 28.98% and in group B at 6 months postoperatively was 13.86% (Figure 1).
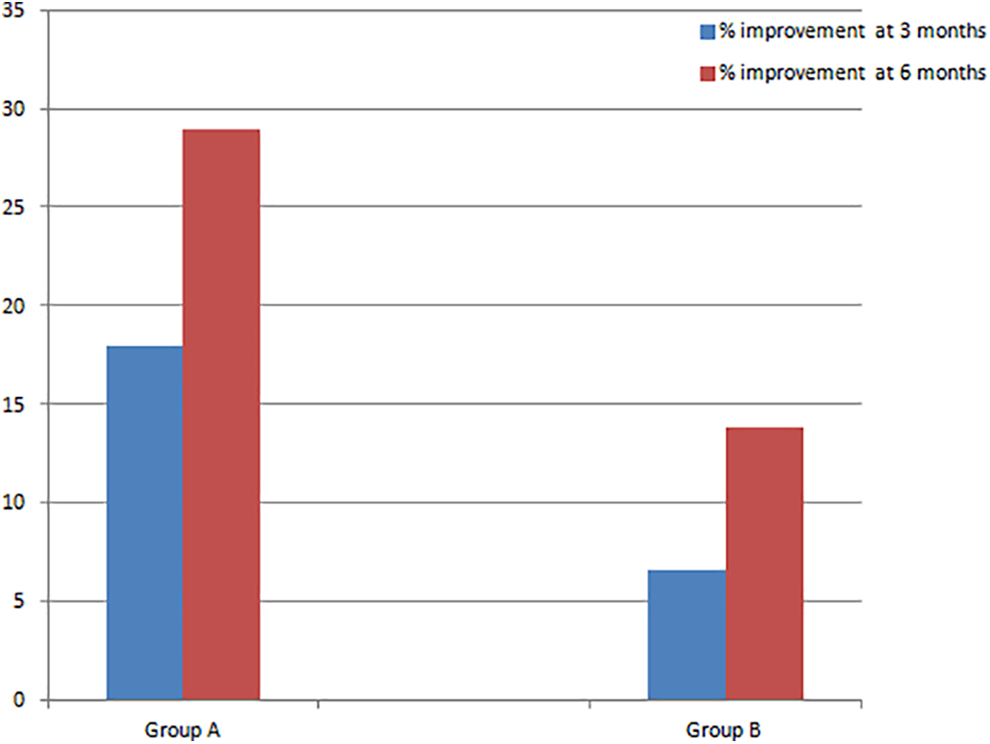
Graph showing percentage changes in mJOA scores in groups A and B at 3 months and 6 months.
Discussion
The current study reports a correlation of intraoperative neurophysiologic changes to postoperative neurological recovery in patients undergoing decompressive surgery for CCM. The results suggest that patients with improved intraoperative MEPs after cervical cord decompression had a better prognosis in neurological recovery compared with the other group in which there was no MEP improvement or deterioration in MEP. This study highlights that IONM changes are a valuable tool in predicting the neurological recovery after decompressive surgery for CCM.
Although we evaluated both MEP and SSEP during IONM; SSEP did not show significant changes. This is consistent with the fact that SSEP is slow to respond to spinal decompression, which may be related to the low sensitivity of SSEP. 26 Clinical guidelines also recommend that MEP recordings are superior to SSEP recordings during spinal cord/spinal column surgery as diagnostic adjuncts for the assessment of spinal cord integrity. 17
In addition, to provide a check on intraoperative cord injury, intraoperative neuromonitoring particularly MEPs can be used as a predictor for neurological recovery. Previous studies have shown that numerous factors affect postoperative outcomes of patients with CCM, including age, duration of myelopathy symptoms, preoperative mJOA score, and signal changes on preoperative MRI.8-10,27 Although MRI signal intensity changes in preoperative MRI as predictive factor of outcome was studied extensively, some authors debated that the presence or absence of a high-intensity area does not correlate with the severity of myelopathy or with surgical results in the group of patients with ossification of the posterior longitudinal ligament and the cervical spondylotic myelopathy groups.10,11,28 However, the list of predictive factors differ according to researchers, and the prognostic significance of these factors remains controversial. In addition to above-mentioned predictors, we demonstrate that intraoperative MEP changes predict the functional outcomes in cervical compressive myelopathic patients.
The early cord recovery outcome was monitored with sensory, motor, pain, and finger grip release assessments as documented previously.18,29 Our results demonstrate that in group A (9 patients) there were positive changes in MEP following decompression (Figure 2) showed varying degrees of sensory and motor improvement and increase in grip and release cycles in 15-second intervals in early postoperative period as compared to their preoperative status. This shows that intraoperative MEP improvement can predict early cord recovery following cervical compressive myelopathy surgery.
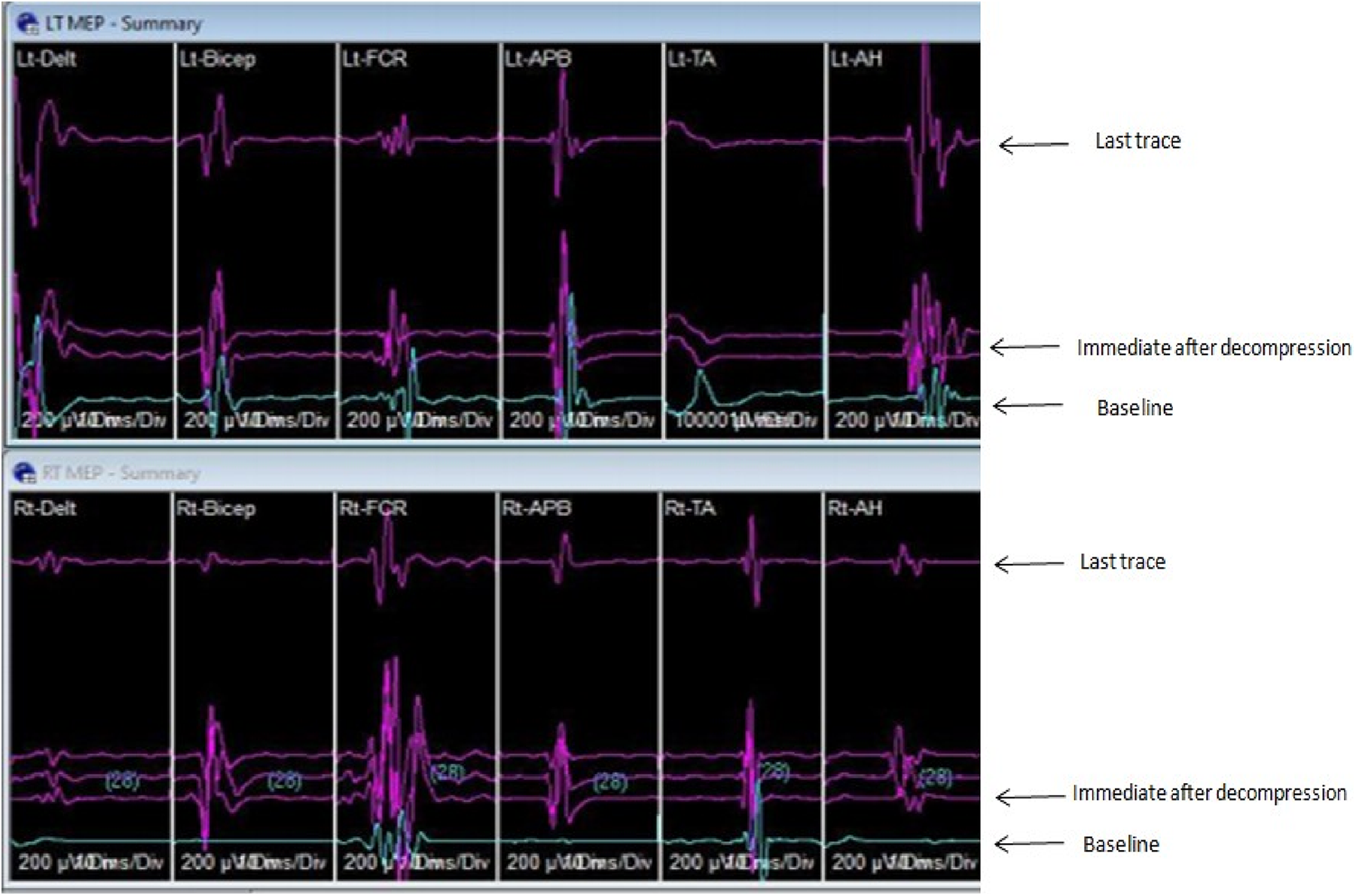
IONM graph in a case of cervical compressive myelopathy showing improvement in almost all group of muscles as compared to baseline following decompression by means of C3-C5 laminectomy.
For long-term outcome, mJOA and Nurick grading were evaluated at 3-month and 6-month interval. 30 Our results suggested that the mJOA improvement rate was significantly better in patients with intraoperative MEP improvement (group A) than those with no improvement or deterioration in MEPs (group B). There was a significant positive correlation between the MEPs improvement and change in the mJOA score at 6 months postoperatively. We also document improvement in Nurick grading in the group with improvement in MEPs. There was a significant negative correlation (r = −0.77; P < .0001) observed between Nurick grade and the mJOA. This is consistent with our expected finding given that improvement in Nurick grade is suggested by a decrease in the value, whereas improvement in mJOA score is suggested by an increase in the value. Thus, on the basis of the above-mentioned observation, we report that neurological recovery is significant in patient with intraoperative improved MEP after cervical cord decompression for CCM.
Two recent studies have evaluated positive changes during IONM and functional status in patients with CCM. Wang et al 18 reported that improvement in MEP amplitude after cervical spinal cord decompression indicate a favorable prognosis in CCM patients. They evaluated the mJOA score before and at 6 months after surgery and found that patients with intraoperative MEP improvement after cervical spinal cord decompression experience good neurological recovery both short and long time after surgery. Park et al 19 studied the effect of positive IONM changes on the functional outcome in patients undergoing CCM surgery. They evaluated the functional outcome with the Korean version of Modified Barthel Index (K-MBI). 31 They reported that differences in the functional improvement rate between the “positive change” and “no positive change” groups was significant at 1 month after surgery but no difference at 6 months, which is contrary to Wang et al findings. The differences between the Wang et al and Park et al studies may have been due to differences in evaluation tools, namely, the use of the mJOA and K-MBI score, respectively. Several outcome measures assess the functional impairment and quality of life in patients with cervical myelopathy. However, mJOA is the widely used disease-specific patient-reported outcome measure to assess the functional impairment and quality of life in a cervical compressive myelopathy population. The mJOA is responsive to change and sensitive to detect any change in the patients clinical condition and reflect the change in the functional score. Thus, mJOA has been adopted as the gold standard tool for evaluating functional status in cervical myelopathy population. In our study, we evaluated the functional outcome with mJOA and our findings concur with Wang et al that intraoperative positive MEP changes are associated with significant improvement in neurological recovery both at early and long term postoperatively reflecting on functional improvement at immediate, 3 months and 6 months after decompressive surgery. The current study and the other 2 studies18,19 do note the neurological improvement in patients with no positive IONM change group over time after decompression, but not as significant as in patients with intraoperative MEP improvement.
Few other studies also showed a correlation of IONM positive change with functional outcome in different spine surgery population. Voulgaris et al 32 studied series of patients who underwent decompressive surgery for lumbar canal stenosis and reported that an increase of intraoperative MEP amplitude after decompression was seen in 17/25 patients and then these patients had a greater postoperative improvement than those without MEP increase. In a similar study population, Piasecki et al 33 reported that neurophysiological response in IONM after decompressive surgery for lumbar spinal stenosis is correlated with a positive effect on the clinical outcome after an average of 8 months of follow-up. Visser et al 34 and showed that in patients with compression of the spinal cord or cauda equina due to intramural tumor, canal stenosis, or disc herniation an improvement of IONM potentials after surgical decompression can indicate motor function recovery postoperatively. Both Pratheesh et al 35 and Barley et al 36 showed an association of intraoperative MEP improvement in motor and clinical recovery in patients undergoing spinal cord detethering surgery.
One of the theories postulated for the correlation of surgical decompression and intraoperative neurophysiological change is that the nervous tissue of the spinal cord does not undergo necrosis, but limit the capability of neurological function in CCM, so it is reversible through surgical decompression. 18 Following surgical decompression, the immediate MEP improvement is probably due to the improving excitability of neuron or corticospinal tract. Also the increasing arterial supply will improve spinal cord ischemia, which will then benefit the MEP augment.
Intraoperative MEPs can detect the functional integrity of corticospinal tracts with high sensitivity and specificity. 37 Compared to previously published outcome variables such as MRI changes, intraoperative neurophysiological change is a quantitative measure in predicting neural and functional recovery following CCM surgery and our findings confirm the notion of Wang et al. 18
Small sample size is the limitation of this prospective observational study evaluating the impact of positive IONM signal change on the outcome of targeted surgical patients. Prior sample size calculation and power analysis not feasible as the effect size of the IONM change on the outcome is not known and not quantifiable from existing limited literature due to heterogeneity in the reported functional outcome measurement tool. Other limitation is that our sample size does not allow subgroup analysis for meaningful conclusion on the differences in outcome between the groups for various pathologies or procedures and this is inherent limitation of any small sample series. Nevertheless, our study results has greater clinical significance and will guide future large scale prospective studies on the topic.
Conclusion
Intraoperative neuromonitoring is a valuable tool in predicting neurological recovery in patients undergoing decompressive surgery for CCM. Patients with improved MEP after cervical cord decompression have a better prognosis in immediate and long-term neurological function recovery. Improvement in functional mJOA score is more significant at 6 months postsurgery in patients with improved MEP changes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.