
Abstract
Study design
Randomized Control Trial.
Objective
DCM refers to compression of spinal cord either due to static/dynamic causes or commonly, a result of combination of both. Number of variables exist, which determine prognosis post-surgery. Role of intra-operative blood pressure has not been analyzed in depth in current literature. Elevating MAP post SCI is widely practiced and forms a recommendation of AANS/CNS Joint Committee Guidelines. This led us to investigate role played by elevated MAP during surgery for DCM, in order to optimize outcomes.
Methods
This prospective randomized comparative pilot study was conducted at a tertiary care spine centre. 84 patients were randomly divided in two groups. Group 1 had intra-operative MAP in normal range. Group 2, had intra-operative BP 20 mmHg higher than preoperative average MAP with a variation of + 5 mmHg. Outcomes were recorded at 3 months, 6 months and 1 year by mJOA, VAS and ASIA scale.
Results
Neurological improvement was documented in 19/30 (63.3%) patients of hypertensive group compared to 16/30 (53.3%) patients of normotensive group. Improvements in mJOA scores were better for hypertensive group during the 1-year follow-up. Improvement in VAS scores were comparable between two groups, but at 1-year follow-up the VAS score of hypertensive groups was significantly lower.
Conclusion
MAP should be individualized according to preoperative average blood pressure assessment of patient. Keeping intraoperative MAP at higher level (preoperative MAP + 20 mmHg) during surgery for DCM can result in better outcomes.
Introduction
Degenerative cervical myelopathy (DCM) refers to presence signs and symptoms of compression of the spinal cord in the cervical spine either due to static or dynamic causes or more commonly as a result of a combination of both secondary to the degenerative changes. The management of the same depends on the degree and site of compression, duration of symptoms etc. Mild cases with stable clinical features can be managed conservatively but in moderate/severe cases as per the modified Japanese Orthopedic Association (mJOA) score and those worsening clinically, surgical intervention remains the preferred modality of management. 1 Though a number of variables exist, which determine the prognosis post-surgery, the role of intra-operative blood pressure has not been studied in-depth in current literature.
Studies employing intraoperative neuro-monitoring have shown that, raising the blood pressure immediately after an observed reduced signal amplitude/increased latency improves the neuro-monitoring signals and hence, indirectly, have demonstrated the importance of systemic blood pressure in maintaining the cord perfusion intra-operatively. However, we could not find a consensus among them, with regards to the minimum blood pressure recommendation. Also, the rationale and physiology behind such episodes remains to be understood.2-4
Studies on the spinal cord blood flow pattern after a spinal cord injury (SCI) observed that maintaining a higher mean arterial pressure (MAP) favored a better cord perfusion as compared to a hypotensive state. 5 The practice of elevating MAP post SCI is widely practiced and also forms a recommendation of AANS/CNS Joint Committee Guidelines.6,7
The above observations lead us to investigate the role an elevated MAP has to play during surgery in order to optimize outcomes and minimize complications. It is known that hypotension can lead to hypo-perfusion resulting in organ injury. The vital organs such as the kidney, myocardium, brain and spinal cord are the most susceptible to hypotension. Organ and tissue perfusion can be maintained with the help of adequate MAP. A systemic hypotension occurs post SCI for example during cord manipulation due not just to interruption of sympathetic fibers but also to direct myocardial dysfunction. Moreover, these local and systemic alterations are not mutually exclusive and systemic hypotension can potentiate the damage due to local post traumatic ischemia. This may make a relatively well-maintained MAP capable of managing cord blood flow during normal stages inadequate for tissue perfusion during such hypotension-causing events.8-10 Therefore, it was hypothesized that elevated MAP during the course of the surgery may be beneficial to tide over such injurious events. The purpose of the current study is thus to compare the effect of intra-operative blood pressure on functional outcome of surgeries in DCM.
Materials and Methods
This prospective randomized comparative pilot study was conducted at a tertiary care spine centre at Mumbai over 18 months from November 2018 to June 2020 (Figure 1). IRB approval was taken prior to commencement (IRB number- EC/BYC/22.11.2018/Dr. A. J.). A total of 84 patients were enrolled in the study as per the inclusion and exclusion criteria (Table 1). Myelopathy as diagnosed based on clinical and radiological criteria; mJOA score below 15 associated with MRI features suggestive of myelopathy. Patients were enrolled by the primary investigator (PI) who took responsibility for completing the consent process and responding to patient queries (A. S.). The current study was designed as a pilot study and therefore an a-priori sample size estimation was not done. The sample was included based on the availability of sufficient number of patients in each group. CONSORT 2010 flow diagram for RCT. Inclusion and Exclusion Criteria for the Enrolment of the Patients for the Study.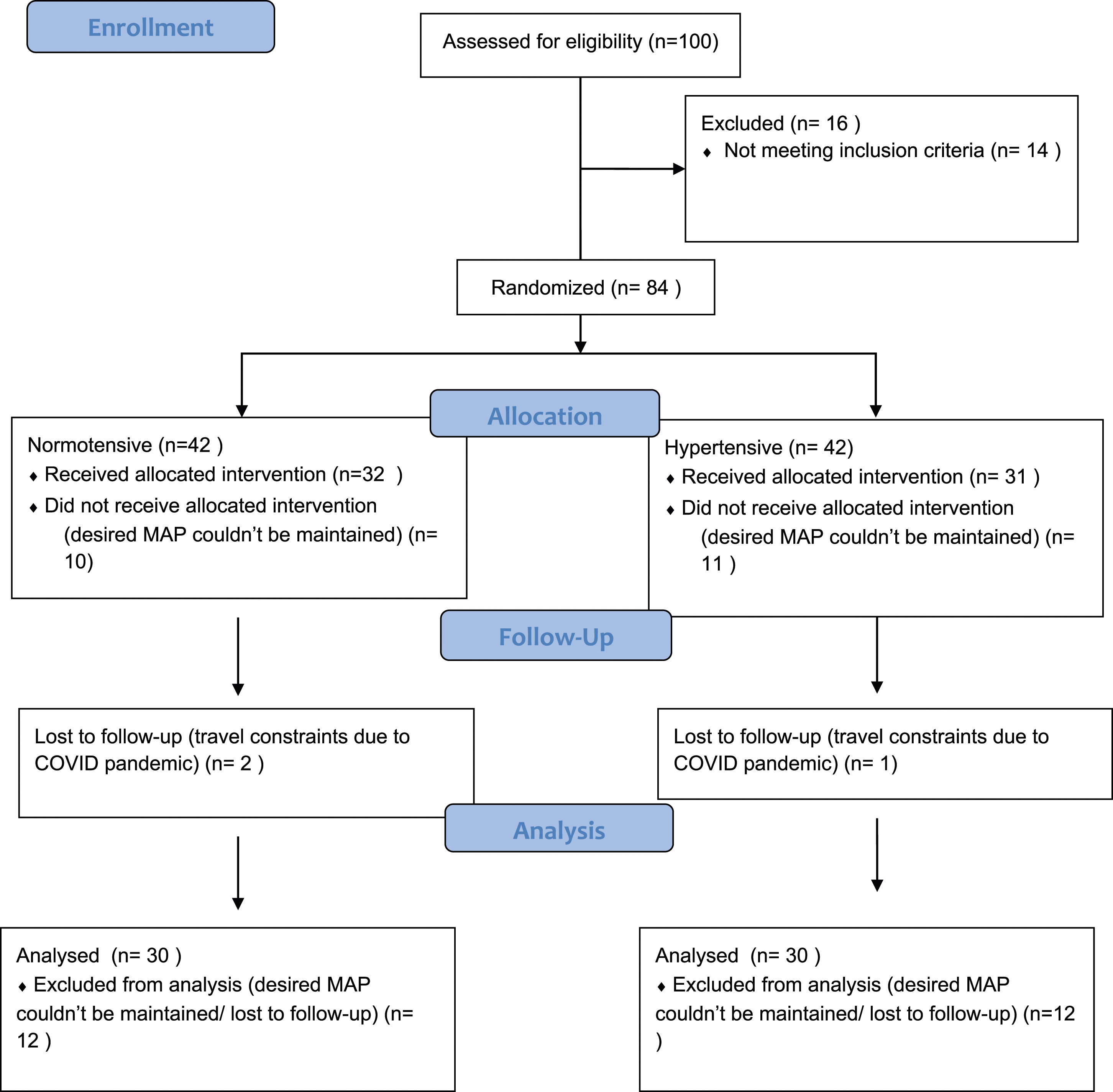
The clinical diagnosis was confirmed with X-rays and MRI scans. For the MRI, 1.5 Tesla machine was used and fast spin echo (FSE) T2 and spin echo (SE) T1 sequences in both sagittal and axial planes were analyzed. CT scan was done in cases where a MRI suggested the presence of ossification of posterior longitudinal ligament (OPLL). X-rays were utilized to assess the sagittal alignment and post-operatively to look at the status of the instrumentation. Similarly, an EMG/NCV study was done when there was doubt regarding concomitant presence of anterior horn cell disease. Patients with medical causes of myelopathy were excluded from the study. The clinical severity of DCM and the neurological status was graded using the mJOA score.
11
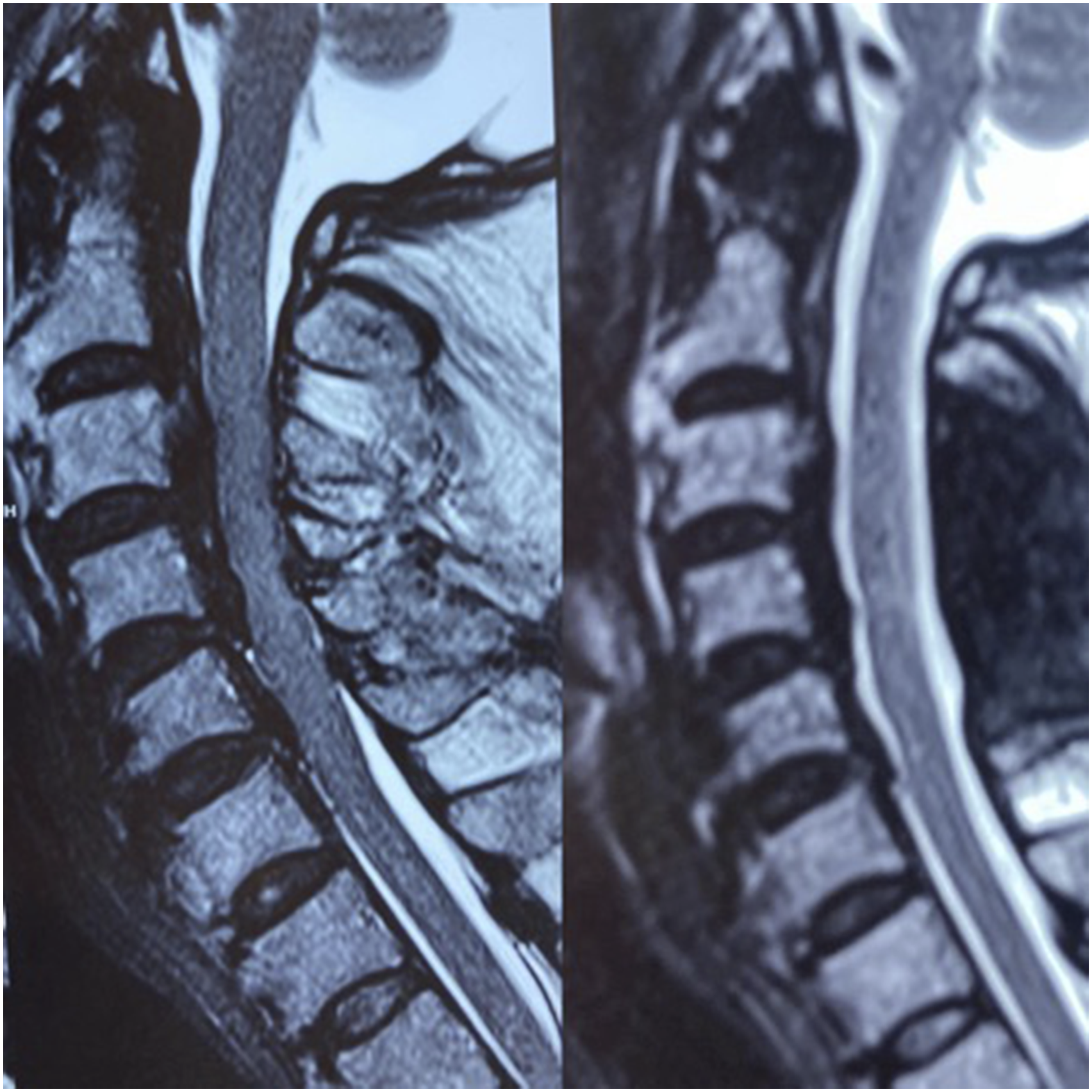
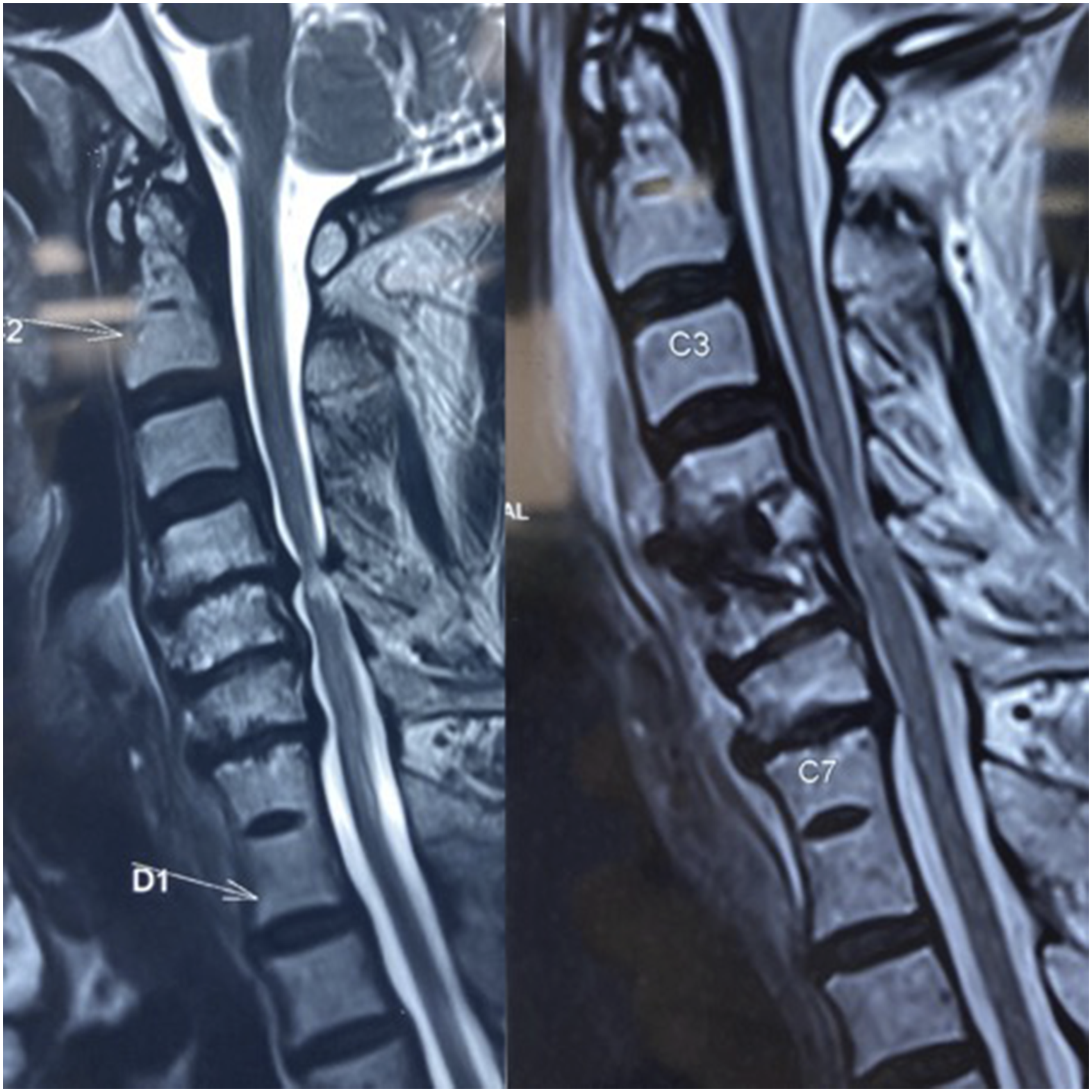
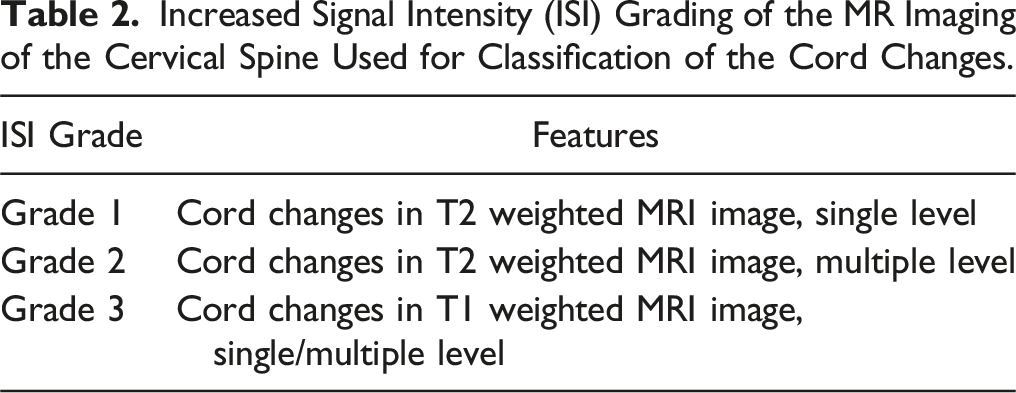
Increased signal intensity grade (ISI) was used to evaluate the preoperative and postoperative 1-year follow up MRI (Figures 2–5) to document the radiological improvement in cord signal changes in T1 and T2 images
12
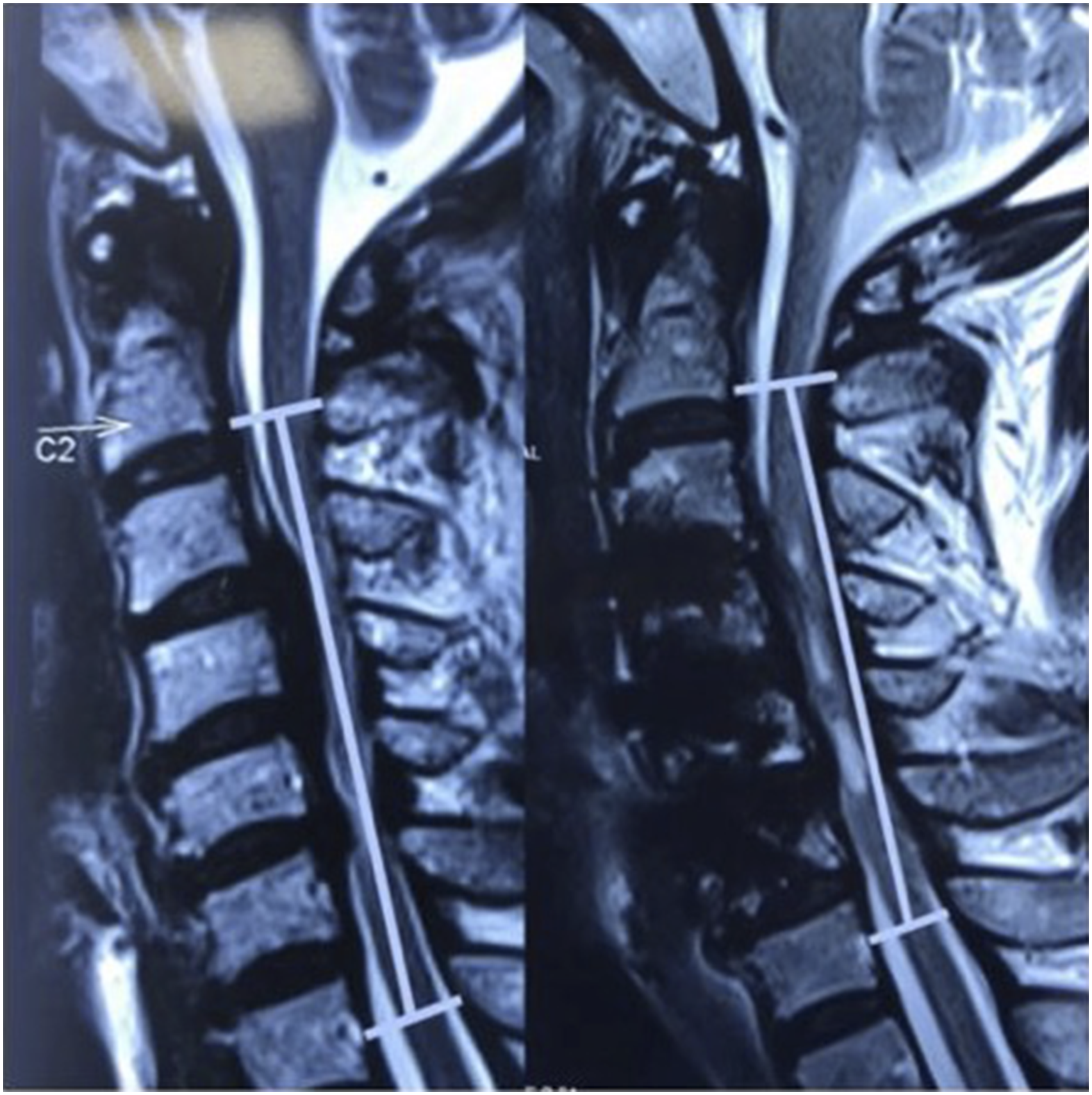
(Table 2). Patient in normotensive group showing progression of cord changes. Pre and post surgery MRI depicting alteration in the K line in a patient operated by anterior approach. MRI in a know case of DISH showing good decompression and cord fall back after posterior decompression. MRI showing reversal of signal change at one year follow up in a patient operated by the anterior approach. Increased Signal Intensity (ISI) Grading of the MR Imaging of the Cervical Spine Used for Classification of the Cord Changes.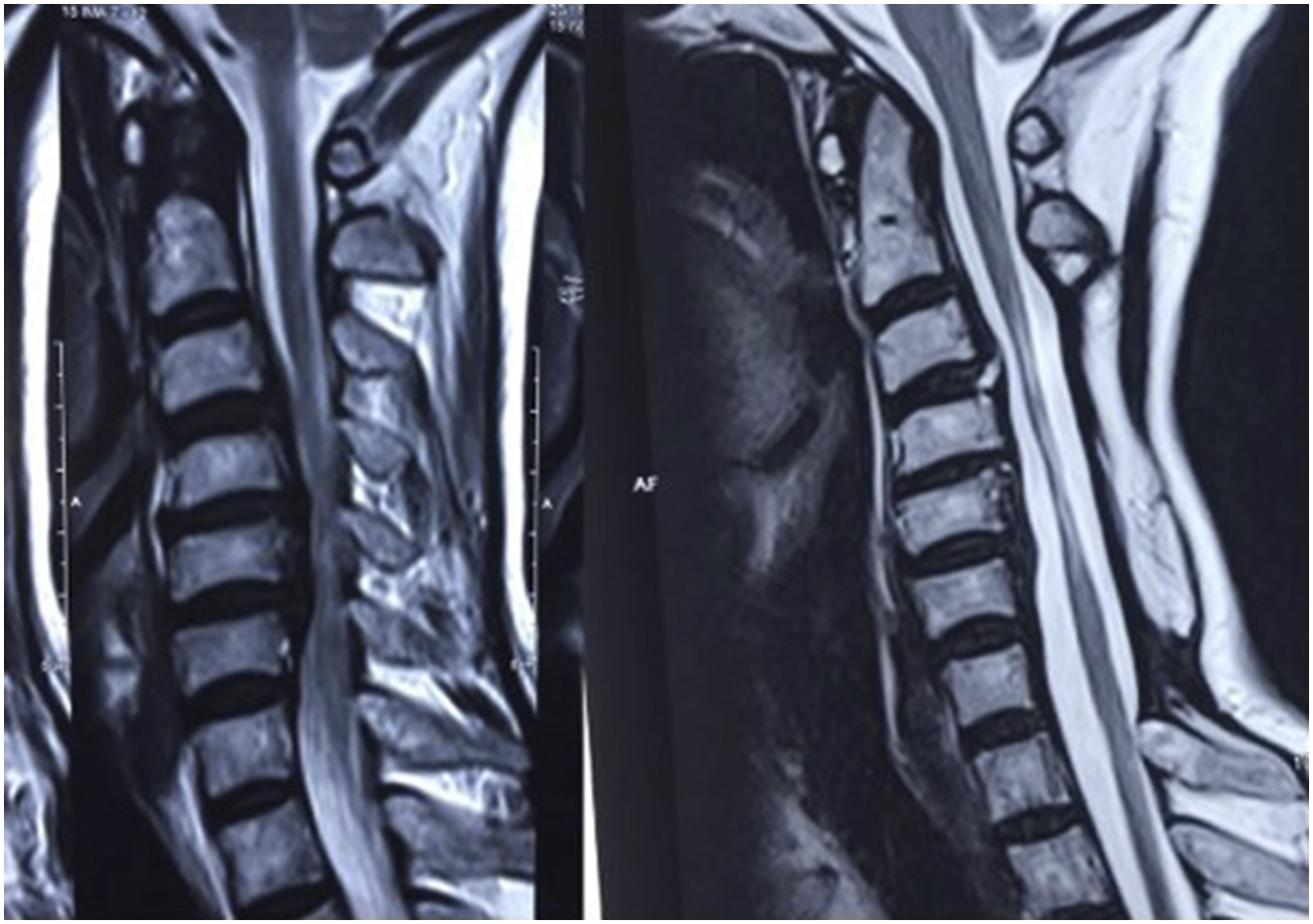
84 patients, fulfilling the selection criteria were randomly divided into two groups. Surgeons and patients were both blinded to the treatment intervention. Sequentially numbered, opaque, sealed envelopes with pressure sensitive paper inside the envelope were used in our study for randomization. To minimize the effect of bias, the random allocation sequence was concealed from A.S. who was the PI enrolling patients into the study. Independent investigator audit was performed at the end of the study period. Group 1, named “NORMOTENSIVE”, had intraoperative mean arterial pressure in the normal range. The normal range of MAP was drawn by the mean of 5 blood pressure readings, of which the first two was taken 2 weeks and 1 week preoperatively and the remaining three were taken over 3 consecutive days immediately preoperatively at least 24 hours before the surgery. Group 2, named “HYPERTENSIVE”, had intra-operative BP 20 mm of Hg higher than the preoperative average MAP with the variation of + 5 mmHg. The preoperative and intra-operative blood pressure recording was done by digital sphygmomanometer. All patients were operated by the same surgical team. The lead surgeon (A.S.) was the same in all these cases and he is also the P.I. for this study. The surgical approach was decided depending on the sagittal alignment/number of levels of pathology/modified K-line (Figures 3, and 6). Typically, patients with >3 level involvement and K-line (+) were approached posteriorly and those with <3 level and K-line (−) were approached anteriorly. The outcomes were recorded, evaluated and followed up by an independent observer at immediate postoperative period, 3 months, 6 months and 1 year by the mJOA, visual analogue score (VAS) and American spine injuries association impairment scale (ASIA) score.
13
Pre and post surgery MRI depicting reversal of signal changes at 1 year follow up in a patient of the hypertensive group.
The data was entered in Microsoft excel and analyzed using SPSS version 20.0. The qualitative data was analyzed using tables and bar diagrams. The quantitative data was expressed in mean and standard deviation. The association between two variables was done with chi-square test. Comparison of mean between two groups was done with unpaired t test and comparison of mean values at different time intervals was done with repeated measures ANOVA and multiple comparison within groups was done with Sidak test. A P-value less than .05 was considered significant. This study was conducted at a public hospital and did not receive any funding or grants.
Results
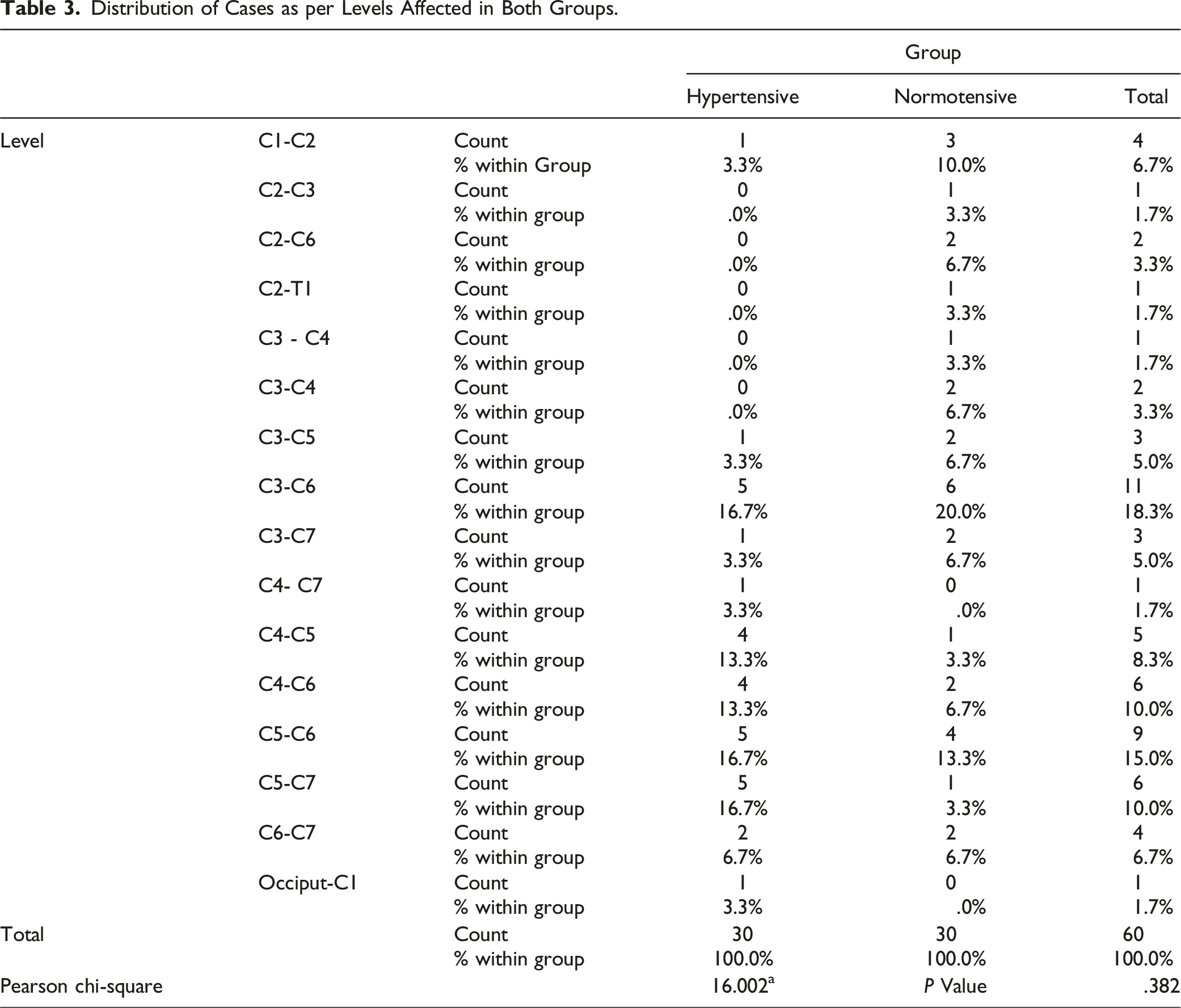
Distribution of Cases as per Levels Affected in Both Groups.
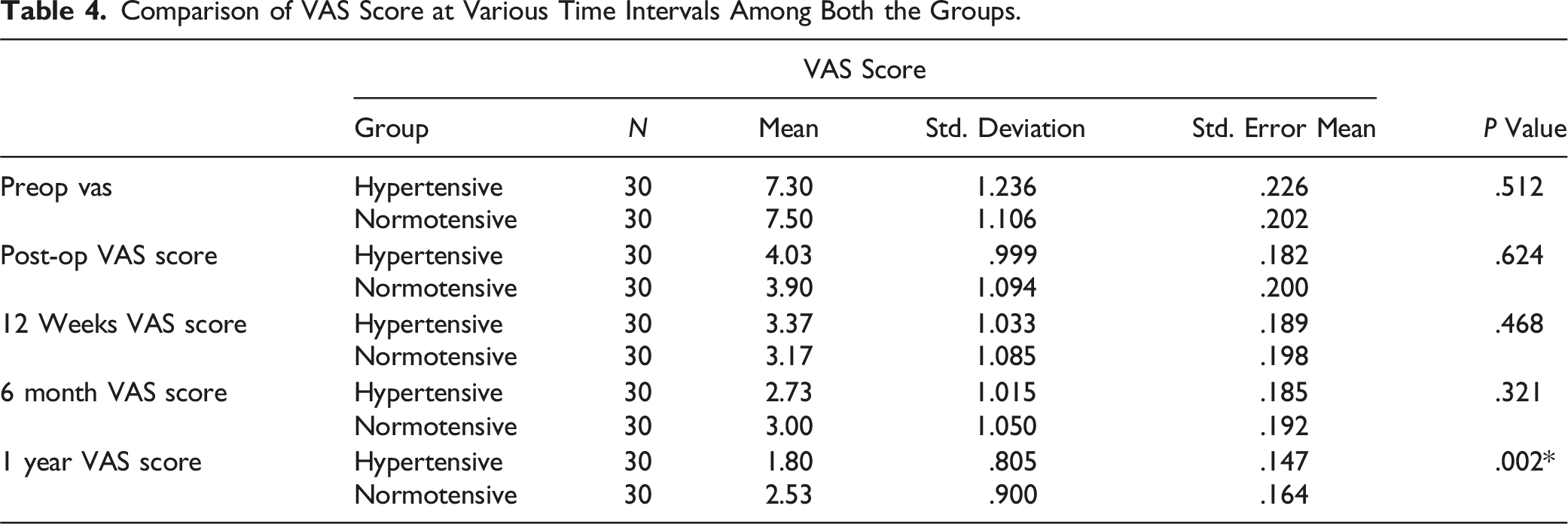
Comparison of VAS Score at Various Time Intervals Among Both the Groups.
VAS SCORE Pairwise Comparison.
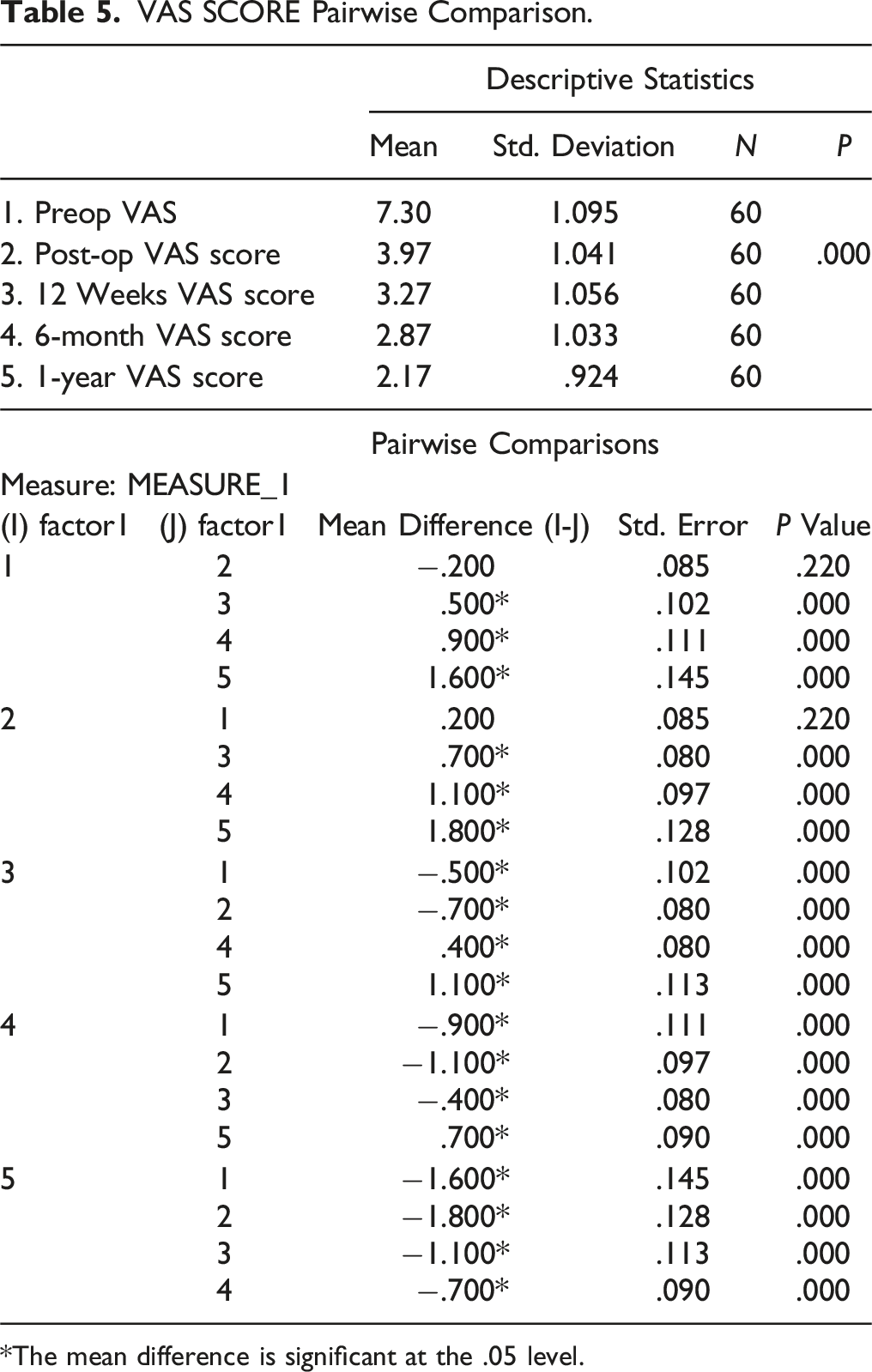
*The mean difference is significant at the .05 level.
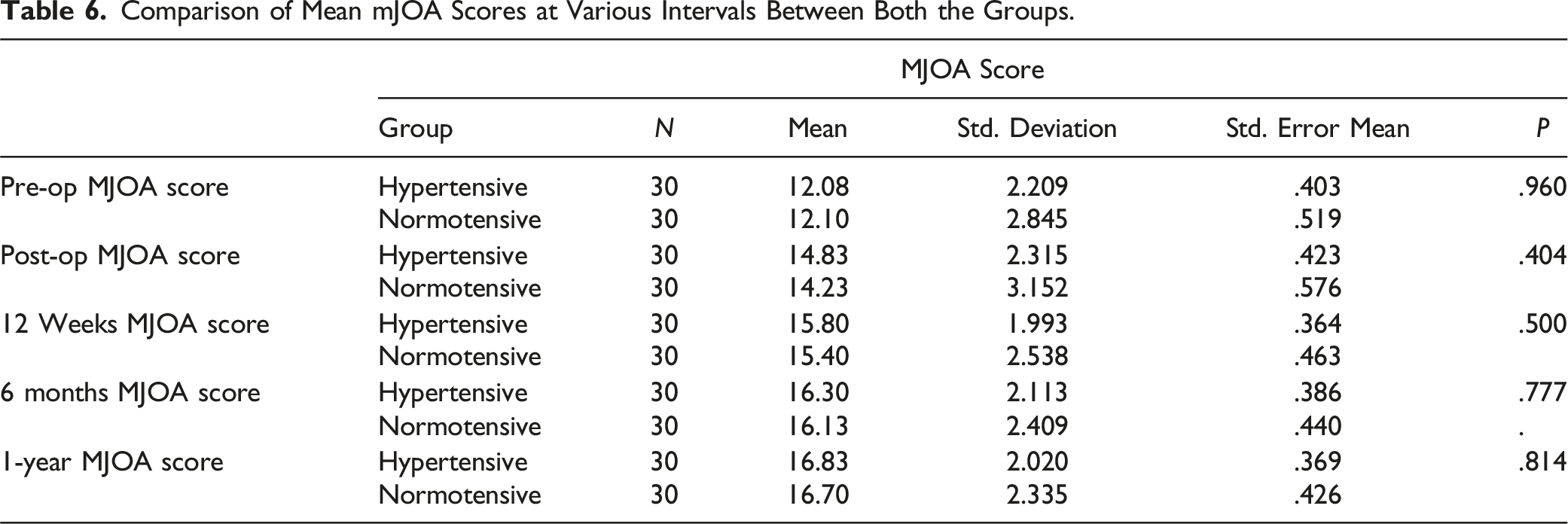
Comparison of Mean mJOA Scores at Various Intervals Between Both the Groups.
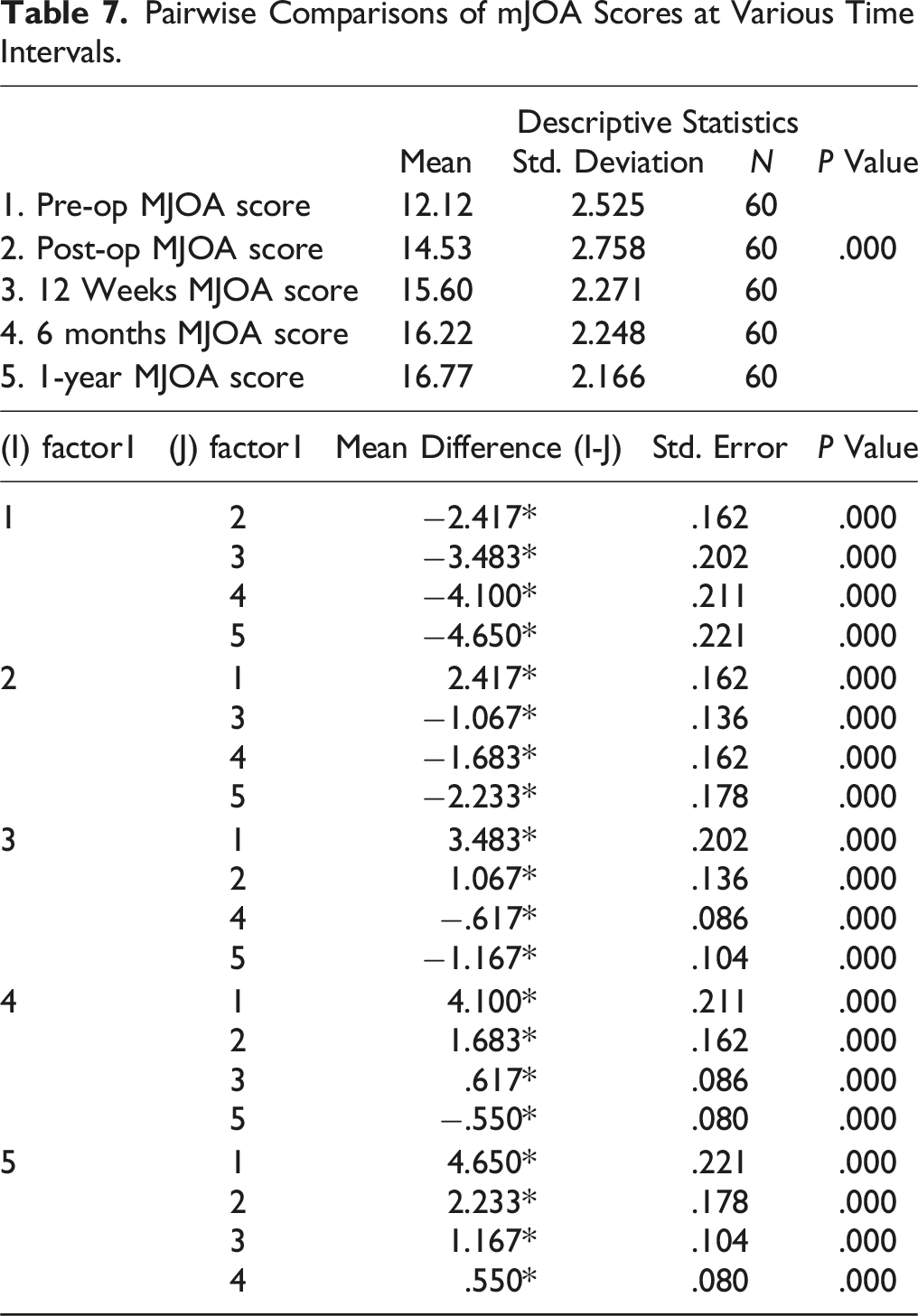
Pairwise Comparisons of mJOA Scores at Various Time Intervals.
On comparing the mJOA scores between the two groups, improvement in mJOA scores was better for the hypertensive group during the 1-year follow-up although this difference was statistically not significant. Similarly, improvement in VAS scores was comparable between the two groups, but, at 1-year follow-up, the VAS score of hypertensive groups was significantly lower compared to the normotensive group (P = .02). In our study, the ISI grade improved to Grade 1 in 66.7 % of the patients in both the groups from a preoperative ISI grade of 2 or 3 in 60% of the patients in the hypertensive group and 56.7% patients with ISI Grade 1 in the normotensive group (Figure 4).
Discussion
The term DCM describes myelopathy resulting from degenerative pathology in cervical spine. The optimum management of DCM continues to be debated due to the inadequacy of information available regarding the natural history of this disorder.14,15 However, there is some agreement in literature, that a shorter duration of symptoms and milder neurological deficit prior to surgery, yields a better post-surgical outcome . 7 There is good amount of literature supporting that MAP should be of 85-90 mmHg for better functional outcomes, but there is no in-depth literature comparing the patients for functional outcome of intraoperative raised MAP with intraoperative normal MAP.
Guha et al demonstrated in their study on rats that an induced moderate hypertension (121-140 mmHg) after a mild SCI improved spinal cord blood flow significantly, whereas hypotension decreased it in a linear fashion. They also showed that induced extreme hypertension (160-180 mmHg) was detrimental to the cord function. 5 This is also seen in our study, as the hypertensive group fared better in terms of functional outcome and improvement in the radiological findings as compared to the normotensive group. This can be explained by the increased spinal blood flow secondary to the raised MAP. In our study, the most common affected level in both hypertensive and normotensive group was C5-C6 followed by C6-C7, 16 which was similar to our previous study conducted in 2018. 17 Pandita et al, in their study of 30 CSM patients also found that the most commonly affected level was C5–C6. 15
The mean duration of symptoms in months till surgery in hypertensive group was 9.23 ± 2.56 months while in the normotensive group it was 5.96 ± 2.98 months. This difference was statistically significant, suggesting that the hypertensive group had worse symptoms to start with. Pandita et al 15 concluded that there was a definite correlation between the symptom duration until surgery and the postoperative mJOA score at 6 months. Yamazaki et al have shown that a shorter symptom duration is an important factor that contributes to excellent recovery in elderly patients. 18 In our study as well, neurological improvement was better when the patient was operated within 3 months from the onset of symptoms.
In our study, a majority of the patients in hypertensive group had preoperative ISI grade of 2 or 3 (60%) whereas most of the patients in the normotensive group presented with ISI grade 1 findings (56.7%) suggesting comparatively worse and chronic compression in the hypertensive group as compared to the other and also supported by the significantly longer duration of symptoms in the hypertensive group. In contrast, the 1-year postoperative MRI demonstrated an ISI Grade 1 in 66% in both the groups of the patients suggesting better improvement in the hypertensive group. The better outcome could at-least partially be attributed to a better cord perfusion management intra-operatively in addition to other factors. Although a significant improvement in the VAS score at 1 year supported the finding, a similar improvement could not be reflected in the mJOA.
Moreover, there was better neurological recovery in the hypertensive group as compared to the normotensive group. Although the difference was statistically insignificant, out of the 29 patients who had neurological deficit preoperatively in hypertensive group, 19 showed neurological improvement at one year compared to 15 patients in the normotensive group.
Studies have shown that a decrease in MAP leads to a decrease in the somatosensory evoked potential (SSEP) signal. This was explained to be due to a decreased spinal flow leading to cord dysfunction secondary to ischemia. These studies also showed that, patients with uncontrolled hypertension on the day of surgery had greater fall in MAP and hence greater loss in SSEP signal intensity. This also demonstrates the need for an individualized MAP target for the prevention of such injuries. 2 Yang et al also demonstrated the improvement in the neuromonitoring signals in 20% of the patients with a loss of signals intraoperatively by raising the MAP alone. 3 Similar results were obtained by Schwartz et al and Samdani et al. This shows the danger of maintaining a lower MAP and at the same time the importance of MAP in maintaining the cord function.4,19 Whereas these studies recommended different minimum cut-offs for the MAPs, we maintained the MAPs of the patients with respect to their preoperative measurements, without sticking to a fixed cut-off, thus making the target MAP specific to each patient. We thus recommend, based on our findings, to maintain the intraoperative MAP slightly higher than the mean preoperative MAP of the patient.
The limitations of our study include its single centre analysis and a relatively small sample size. Also, objective correlation between the ISNCSCI on MRI and the corresponding ASIA motor score has not been added as a part of this study. A multi centric study with a larger sample size will further validate our findings. Also, we can expand this study and analyze the role played by intra-operative MAP in other spine pathologies. The blood pressure is one factor that can be easily controlled and monitored, with no additional costs and good communication with the anesthesia team. Hence, we believe, the changes suggested in our study, can be widely adopted, in various practice settings.
Conclusion
Based on the study of the effect of intraoperative MAP on functional outcome of patients operated for CSM, we conclude that MAP intraoperatively should be individualized according to preoperative average blood pressure assessment of the patient. Keeping intraoperative MAP at higher level (preoperative MAP + 20 mmHg) during surgery for CSM, can result in better neurological improvement.
Footnotes
Acknowledgments
Independent investigator audit was performed at the end of the study period by Dr. Anuradha Mohapatra, director of “Quick-Stats solutions”, [email-
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Code Availability
software application/custom code available.
Trial Registration Number
EC/BYC/22.11.2018/Dr. A. J.
Data Availability Statement
We have been transparent in sharing all the necessary data.