
Abstract
Study Design:
Retrospective case-control study
Objectives:
To determine whether diffuse idiopathic skeletal hyperostosis (DISH) can be diagnosed based on anterior longitudinal ligamental ossification in the lumbar spine using plain lumbar spine X-ray images.
Methods:
This study included 100 patients (59 men and 41 women; mean age, 64.8 ± 13.8 years; range, 27-89 years) who underwent computed tomography (CT) of the chest to the pelvis in our hospital and plain lumbar spine radiography within 6 months before and after CT scanning. DISH was diagnosed based on the thoracolumbar spine CT findings using Resnick’s diagnostic criteria. The patients were grouped according to DISH diagnosis into the DISH (+) and DISH (−) groups. On the frontal and lateral lumbar spine X-ray images, each spinal level from Th11/12 to L5/S was scored based on the Mata scoring system. The distribution of the Mata scores was compared between the 2 groups.
Results:
Forty (40%) patients were diagnosed with DISH based on the CT findings. A cutoff value ≥8 provided a sensitivity of 75% and specificity of 100% for diagnosing DISH, thus, indicating the validity of the cutoff value. In the DISH (−) group, no patient had ≥3 consecutive spinal levels with a Mata score ≥2, suggesting that DISH can be diagnosed on the basis of at least 3 consecutive spinal levels with a Mata score ≥2.
Conclusion:
On lumbar spine X-ray images of the T11/12 to L5/S levels, a Mata score ≥2 for at least 3 consecutive levels or a total score ≥8 strongly indicates the presence of DISH.
Keywords
Introduction
Diffuse idiopathic skeletal hyperostosis (DISH) is a condition characterized by progressive ossification of ligaments throughout the patient’s body. In the spine, ossification of the anterior longitudinal ligament leads to the formation of bony bridging between vertebrae, resulting in ankylosis. This condition was first reported by Forestier 1 in 1949 and then established as DISH by Resnick and colleagues.2,3 DISH is diagnosed by the presence of at least 4 bony bridges in the anterior or lateral aspect of vertebrae, a relatively preserved intervertebral disc height, and the absence of sacroiliac ankylosis. 3
Clinical symptoms associated with DISH include back pain, limited range of motion, 4 decreased vital capacity, aspiration, and airway obstruction. 5 Other features characterized by recent reports include increased vulnerability to vertebral fracture, 6 difficulty in achieving bone fusion during conservative treatment after vertebral fracture, 7 high possibility of requiring surgery, 8 a risk factor for thoracic myelopathy, 9 increased risk of pseudarthrosis after lumbar spinal fusion, 10 and a poor prognostic factor due to a high reoperation rate after lumbar decompression surgery.11-13 Hence, DISH affects the diagnosis, treatment, and posttreatment outcome of spinal diseases. It is therefore important to determine the possible coexistence of DISH in spinal diseases.
Particular attention is required in lumbar spinal diseases. In patients with lumbar spinal canal stenosis, the coexistence of DISH increases the re-decompression rate and may necessitate expansion of the decompression range.11-13 DISH is also associated with an increased incidence of pseudarthrosis after lumbar spinal fusion for spondylolisthesis or other conditions 10 and may necessitate expansion of the fixation range or prolonged postoperative external fixation. DISH is a predisposing factor for thoracic myelopathy. 9 In patients with lower extremity symptoms who were diagnosed with lumbar spinal canal stenosis and underwent lumbar decompression alone, additional thoracic decompression may be required for overlooked thoracic myelopathy. 14
Evidence of ossification of at least 3 consecutive spinal levels is required for the diagnosis of DISH. 3 Because of a high incidence of DISH bridging in the thoracic spine 14 and a high rate of being overlooked on plain thoracic spine X-ray, 15 spinal computed tomography (CT) is recommended for diagnosing DISH. However, performing CT and additional X-ray of the thoracic spine to determine the presence or absence of DISH in patients with lumbar spinal complaints is not desirable because it increases stress, radiation exposure, and medical economic burden to patients.
Since plain lumbar spine X-ray is performed in almost all patients scheduled for lumbar spine surgery, the ability to infer the presence or absence of DISH on plain lumbar spine X-ray images will help determine the need for additional tests to diagnose DISH and the treatment strategy for the primary disease. It may also lead to early detection of thoracic myelopathy. Another advantage of using plain lumbar spine X-rays, as compared with thoracic spine X-rays, is the absence of overlapping ribs, making it easier to identify ligamental ossification.
The objective of this study was to examine whether DISH can be diagnosed based on characteristic findings of ligamental ossification on lumbar spine X-ray in patients who had been definitively diagnosed with or without DISH by CT.
Materials and Methods
This retrospective case-control study included 100 patients who underwent CT scans of the chest to the pelvis in our hospital for any disease between 2010 and 2018 and plain lumbar spine X-ray (frontal and lateral) within 6 months before and after CT scanning. Patients with thoracolumbar spinal CT findings that met the diagnostic criteria for DISH, as described by Resnick and Niwayama, 3 were included in the DISH (+) group, and those who did not meet the criteria were included in the DISH (−) group.
All lumbar spine X-ray photographs included the Th11 to S1 vertebrae. On the frontal and lateral lumbar spine X-ray images, each of the 7 spinal levels from Th11/12 to L5/S was scored based on the Mata scoring system 16 : 0, no ligamental ossification; 1, ossification without bridging; 2, ossification with incomplete bridging; 3, complete bridging of the disc space, with higher scores indicating more severe ligamental ossification. When different scores were derived from the frontal and lateral images, the higher score was taken. The presence or absence of DISH on CT and the Mata score on X-ray were determined by discussion among 3 spinal surgeons.
Age, sex, and the prevalence of DISH in all patients were reported. The DISH (+) and DISH (-) groups were compared for sex, age, and the total Mata score for the T11/12 to L5/S levels (7 levels; score range 0-21). The distribution of spinal levels with a Mata score ≥2 was compared in all patients. A cutoff value of the Mata score was defined to determine the sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) for diagnosing DISH. Receiver operating characteristic (ROC) curves were created from the total Mata score for the presence or absence of DISH to determine the area under the curve and optimal cutoff value.
For statistical analysis, the chi-square test was used to compare categorical variables. Analysis of variance was used to compare continuous variables between the 2 groups. Mann-Whitney U test was used to compare rank variables between the 2 groups. The cutoff value of the total Mata score for 7 spinal levels to determine the presence of DISH was determined based on the area under the curve (AUC) in the ROC curve. Differences were considered significant for P < .05. All analyses were performed using JMP version 14.3 for Macintosh (SAS Institute).
The study was approved by the institutional review board at our hospital.
Results
The patients comprised 59 men and 41 women, with mean age of 64.8 ± 13.8 years (range, 27-89 years). Forty (40%) patients were diagnosed with DISH based on thoracolumbar spinal CT findings. Although the DISH (+) group had a higher proportion of men than women, the difference was not statistically significant. Meanwhile, the mean age was significantly higher in the DISH (+) group. The mean Mata score for the 7 spinal levels from T11/12 to L5/S was significantly higher in the DISH (+) group than in the DISH (−) group (Table 1).
Demographic Data and Comparison Between the DISH (+) and DISH (−) Groups.
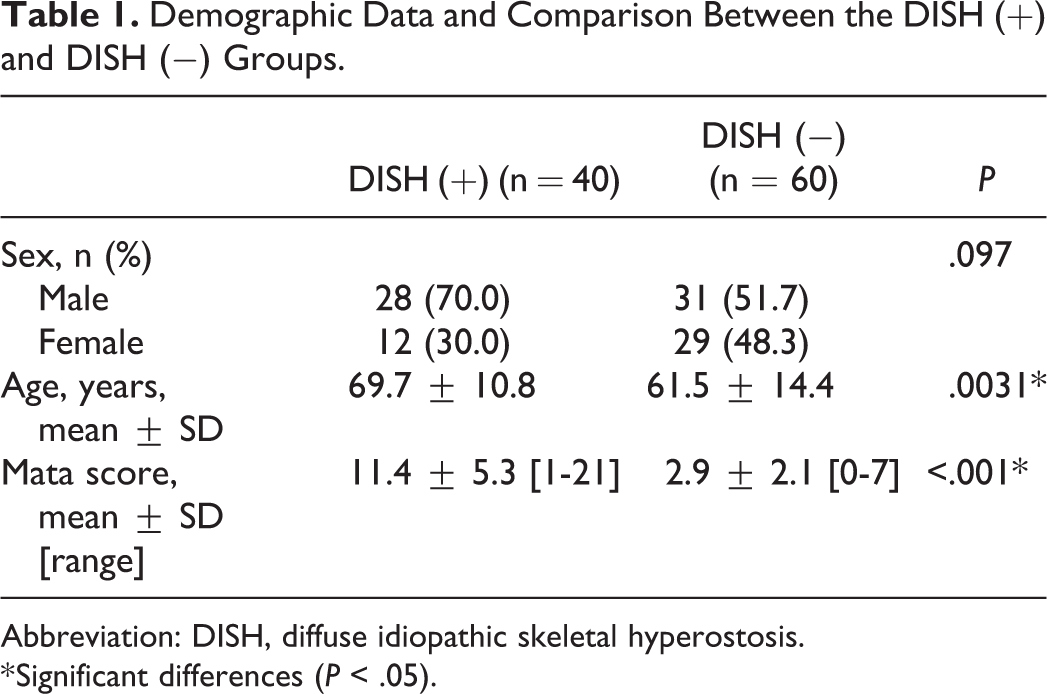
Abbreviation: DISH, diffuse idiopathic skeletal hyperostosis.
* Significant differences (P < .05).
When the cutoff value for diagnosing DISH was ≥8, the sensitivity, specificity, PPV, and NPV were 75%, 100%, 100%, and 86%, respectively, demonstrating the validity of the cutoff value (Table 2). In the DISH (−) group, no patient had ≥3 consecutive spinal levels with a Mata score ≥2, suggesting that DISH can be diagnosed by at least 3 consecutive spinal levels with a Mata score ≥2 (Figures 1 and 2).
Number of Patients in the DISH (+) and DISH (−) Groups When the Cutoff Value Was Set at 8.
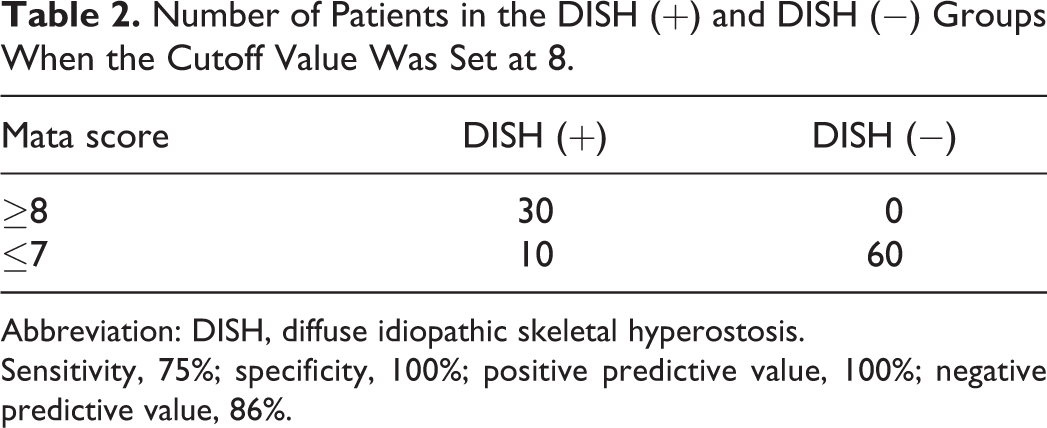
Abbreviation: DISH, diffuse idiopathic skeletal hyperostosis.
Sensitivity, 75%; specificity, 100%; positive predictive value, 100%; negative predictive value, 86%.
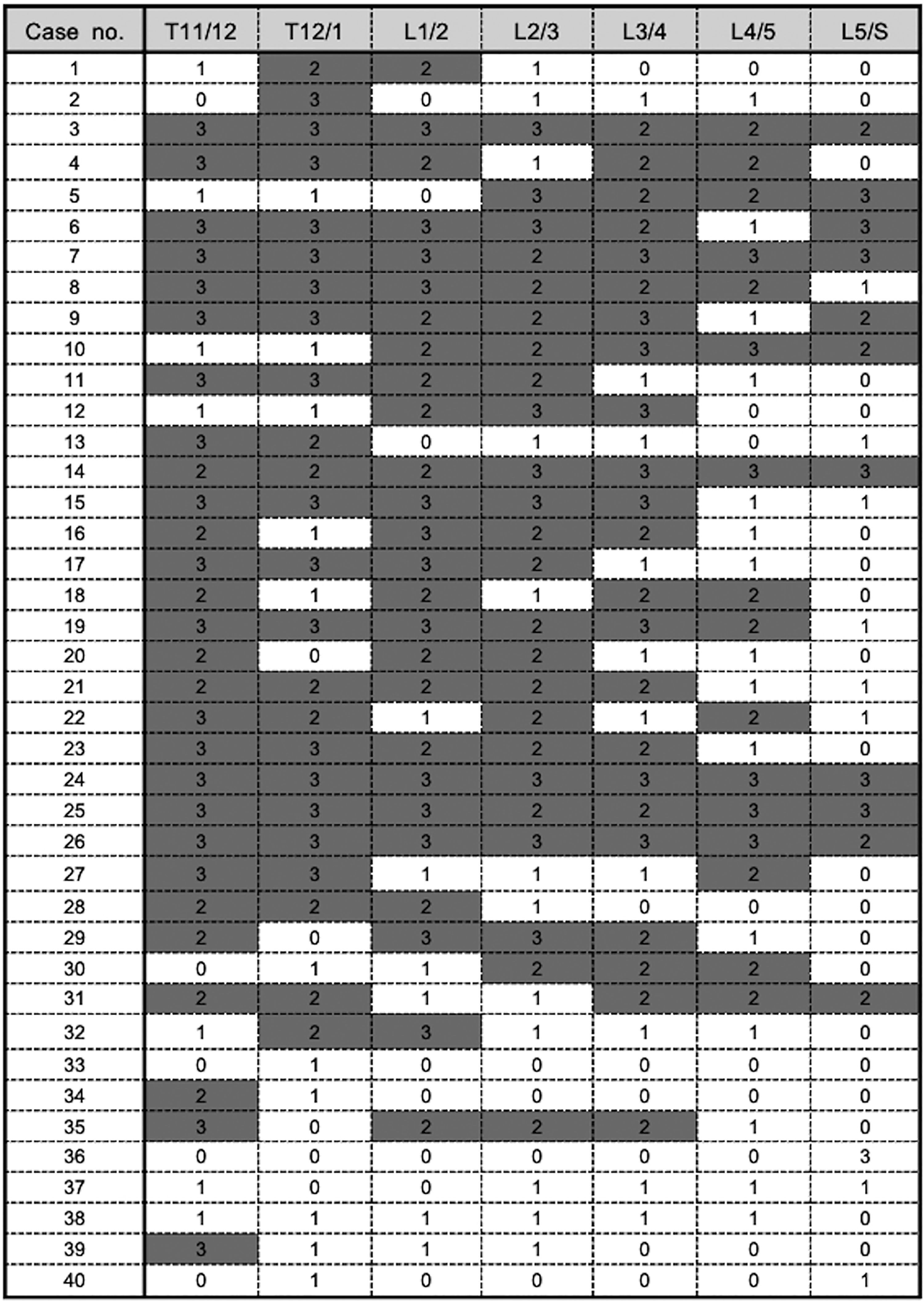
Mata scores for the 7 spinal levels from Th11/12 to L5/S in the DISH (+) group. Shaded cells, spinal levels with Mata score ≥2. A large proportion of patients had ≥3 consecutive spinal levels with Mata score ≥2. DISH, diffuse idiopathic skeletal hyperostosis.
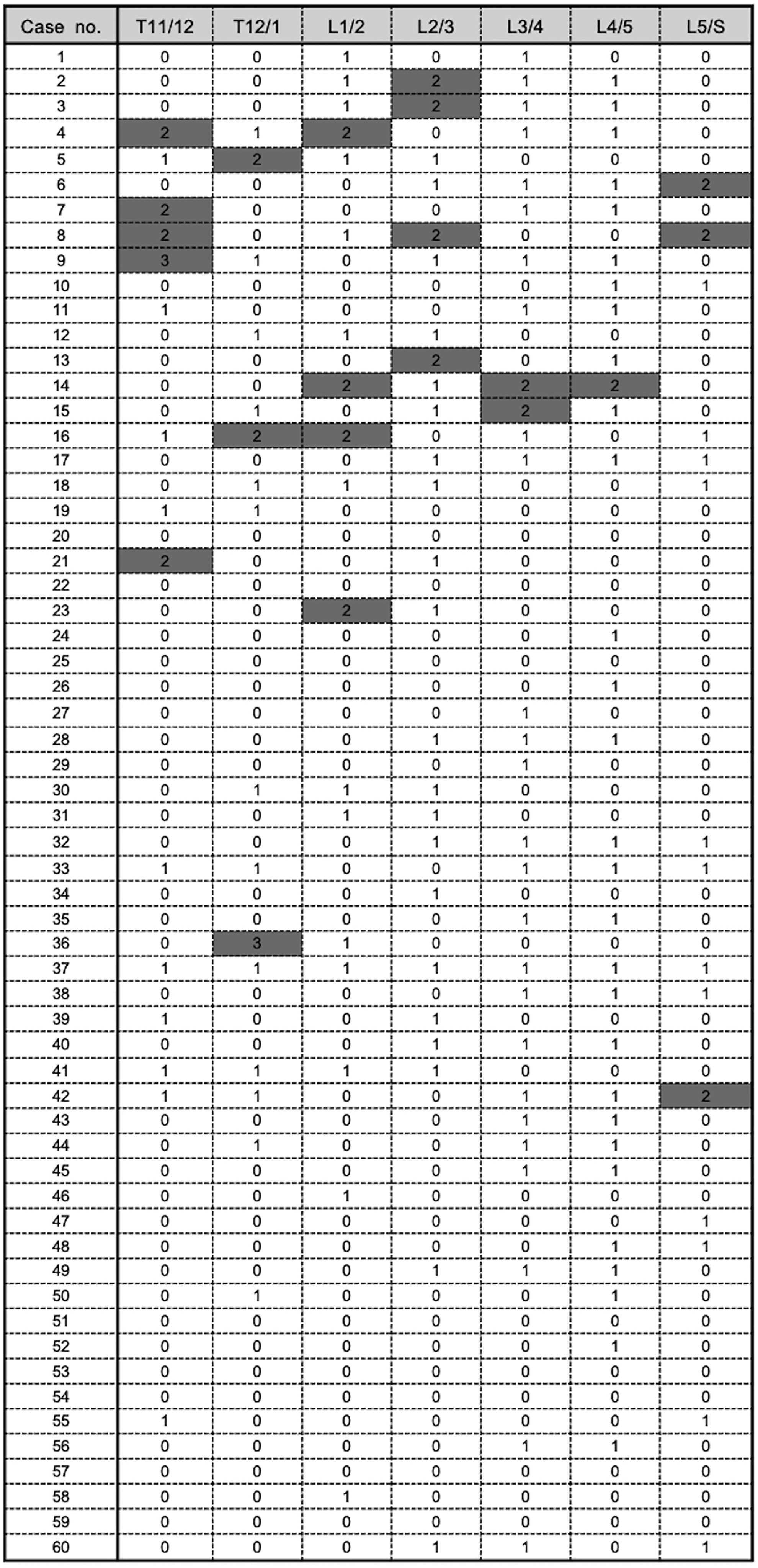
Mata scores for the 7 spinal levels from Th11/12 to L5/S in the DISH (−) group. Shaded cells, spinal levels with Mata score ≥2. No patient had ≥3 consecutive spinal levels with a Mata score ≥2. DISH, diffuse idiopathic skeletal hyperostosis.
An ROC curve was created from the total Mata score for Th11/12-L5/S levels to identify DISH (+) cases, and a cutoff value of 6 provided a sensitivity, specificity, and AUC of 88%, 88% and 0.93, respectively (Figure 3).
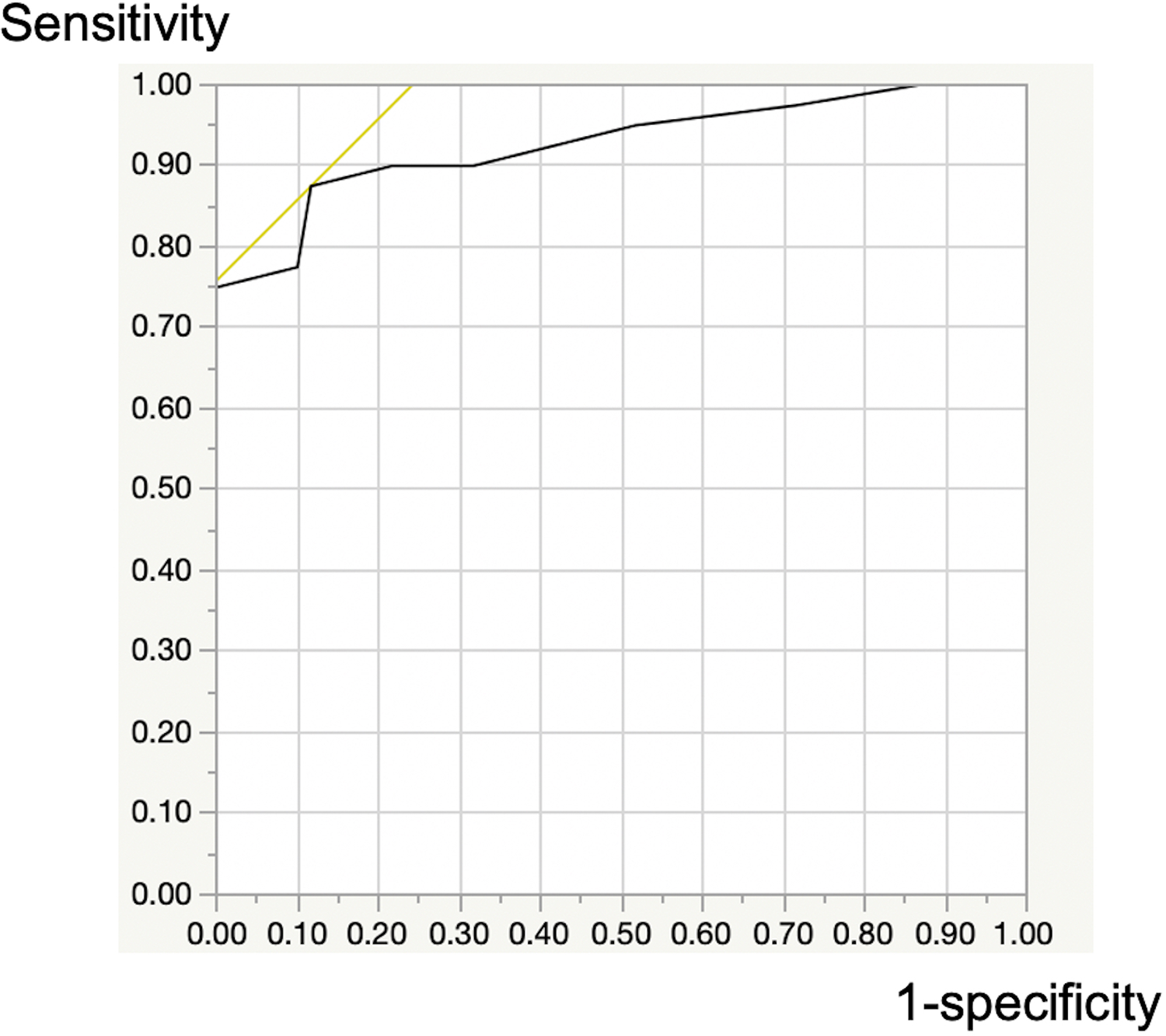
Receiver operating characteristic curve with the cutoff value of the total Mata score set at 6 to identify DISH (+) cases. A cutoff value of 6 provided high diagnostic accuracy, with a sensitivity of 0.88, specificity of 0.88, and area under the curve (AUC) of 0.93. DISH, diffuse idiopathic skeletal hyperostosis.
Discussion
This study evaluated 100 patients who were confirmed to have or not have DISH based on CT findings from the thoracic spine to the pelvis to determine whether DISH can be diagnosed based on the degree of ligamental ossification, which can be determined on frontal and lateral plain lumbar spine X-ray images, and determined that, in the 7 spinal levels from T11/12 to L5/S, a Mata score ≥2 in at least 3 consecutive levels strongly suggested DISH, a total score ≥8 for the 7 levels strongly suggested DISH, and a total score ≥6 for the 7 levels suggests DISH, with a sensitivity of 88% and specificity of 88%.
The prevalence of DISH has been reported to be 2.9% to 27.2%.15,17,18 The prevalence in the present study was as high as 40%, which was probably due to the high mean age of the participants (64.8 years); although there was a higher proportion of male patients than female patients, it was not significant. The mean age of the DISH (+) group was higher than that of the DISH (−) group, which is consistent with previous reports.
Resnick and Niwayama 3 proposed the diagnostic criteria for DISH using plain X-ray images of the whole spine in 1976. Since then, most studies on DISH have used their diagnostic criteria, 19 and so did the present study.
Mata proposed a scoring system for the degree of progression of DISH ossification in 1998. The Mata score 16 increases as the severity of ossification increases and thus could be used as a rank variable. In this study, the individual and total scores were used to indicate the degree of progression of ossification in each spinal level and the 7 levels as a whole, respectively.
The assumption that DISH can be diagnosed by a Mata score ≥2 in at least 3 consecutive spinal levels out of the 7 levels from T11/12 to L5/S (Figures 1 and 2) was based on the fact that none of the 60 patients in the DISH (-) group had ≥3 consecutive levels with a Mata score ≥2. This assumption for 100 patients in this study would be true with a very high probability, and the probability would been nearly 100% if the study had a higher number of participants. The other assumption that DISH can be diagnosed if the total score for the 7 spinal levels is ≥8 (Table 2) was based on the observation that none of the patients in the DISH (−) group had a total score ≥8. This would also be true with a high, but uncertain, probability. The criterion that a total score ≥6 for the 7 spinal levels indicates DISH with a sensitivity of 88% and specificity of 88% (Figure 3) also has high accuracy, with an AUC of 0.93.
DISH, a condition previously not well recognized, has recently attracted attention and has been suggested to affect the surgical procedures for and treatment outcomes of various spinal diseases, including fractures and lumbar spinal canal stenosis.6-13 Although lumbar spine X-ray is often performed in patients with low back pain or suspected lumbar spinal canal stenosis, thoracic spine X-ray and CT are performed less frequently due to lower incidence of thoracic spine diseases. The ability to infer the presence of DISH on plain X-ray images of the lumbar spine will allow for narrowing down of diseases to be screened and thereby reduce patients’ exposure to radiation and medical costs. Moreover, DISH has been associated with high prevalence of concomitant obesity, diabetes, and hyperlipidemia20-22 and subsequent increased risk of cerebral infarction 23 and coronary artery diseases. 24 Therefore, detection of coexisting DISH will warn asymptomatic patients and may be helpful in detecting and preventing these diseases.
Conclusion
DISH can be diagnosed based on anterior longitudinal ligamental ossification in the lumbar spine using plain lumbar spine X-ray images. On lumbar spine X-ray images of T11/12 to L5/S levels, a Mata score ≥2 for at least 3 consecutive levels or a total score ≥8 strongly indicates the presence of DISH, and a total score ≥6 indicates probable presence of DISH. There is a high probability that DISH can be diagnosed based on anterior longitudinal ligamental ossification in the lumbar spine using plain lumbar spine X-ray images.
Footnotes
Authors’ Note
The study was approved by the institutional review board at Ehime University hospital.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.