
Abstract
Study Design:
Retrospective study.
Objectives:
Unilateral biportal endoscopic surgery (UBES) is a popular surgical method used to treat degenerative spinal diseases because of its merits, such as reduced tissue damage and outstanding visual capacity. However, dural injury is the most common complication of UBES with an incidence rate of 1.9% to 5.8%. The purpose of this study was to analyze the pattern of dural injury during UBES and to report the clinical course.
Methods:
We retrospectively reviewed the medical and radiographic records of surgically treated patients who underwent UBES at a single institute between January 2018 and December 2019.
Results:
Fifty-three patients, representing 67 segments, underwent UBES. Seven dural injuries occurred, and the incidence rate was 13.2%. Among 16 far lateral approaches, 2 dural injuries of the exiting roots occurred and were treated with fibrin sealant reinforcement. Among 51 median approaches, dural injury occurred at the thecal sac (n = 3) and traversing root (n = 2). A dural injury of the shoulder of the traversing root was treated with a fibrin sealant; however, a defect in the thecal sac required a revision for reconstruction. The other 2 thecal sac injuries were directly repaired via microscopic surgery.
Conclusions:
Dural injury during UBES can occur because of the various anatomical features of the meningo-vertebral ligaments. Direct repair of the central dural defect should be considered under microscopic vision. A linear tear in the lateral dura or root can be controlled with a simple patchy reinforcement under endoscopic vision.
Keywords
Introduction
Endoscopic surgery has been suggested as an alternative to microscopic surgery because it results in reduced postoperative pain and recovery time. 1 Unilateral biportal endoscopic surgery (UBES) uses 2 different portals and provides a closer view via the insertion of an endoscope on one side. In the uniportal transforaminal approach, the endoscope needs to be docked in the bony structure; however, in UBES, surgeons can move the endoscope freely, which has the advantage of providing a wider range of vision. 2 Given an aging society, the scope of endoscopic surgery has been expanding based on these strengths. Favorable outcomes have been reported for spinal stenosis, extraforaminal disc herniation, and spondylolisthesis, as well as for discectomy for disc herniation in the lateral recess. 3 -7
The most common complication of UBES is dural injury. Recent studies report an incidence rate of 1.9% to 5.8%. 8,9 Once a dural injury occurs in UBES, managing the dural injury is not easy as it would be with other endoscopic surgeries because only one portal exists for the instrument. Treatment outcomes for UBES have recently been reported, 10 but few articles have focused on dural injury. The purpose of this study was to analyze the pattern of dural injury during UBES and to report the clinical course.
Methods and Materials
This retrospective study was approved by the institutional review board. This retrospective study did not involve an intervention. The need for the patients’ written consent was waived.
Between January 2018 and December 2019, a total of 53 consecutive patients who underwent UBES for degenerative spine disease were identified, based on the surgical records of a single institution. Patients who underwent UBES for trauma and infection were excluded. Surgical approaches were classified as ipsilateral discectomy, bilateral decompression, and extraforaminal approach. 11,12 All surgeries were performed by a single neurosurgeon with 7 years of experience.
Dural injury was recognized during surgery, and the injury position and size were measured by analyzing the surgical video. The position of the injury was simply classified as the thecal sac, traversing root, or exiting root.
Results
Table 1 summarizes the clinical features of the entire operation. The surgery was performed on 67 segments, which included 25 cases of ipsilateral discectomy, 26 cases of bilateral decompression, and 16 extraforaminal approaches. Dural injury occurred in seven patients and had an incidence of 13.2% (n = 7/53). Clinical data and management of the seven patients with dural injury are summarized in Table 2.
Clinical Characteristics of the Entire Surgery (Total n = 53, Segments = 67).
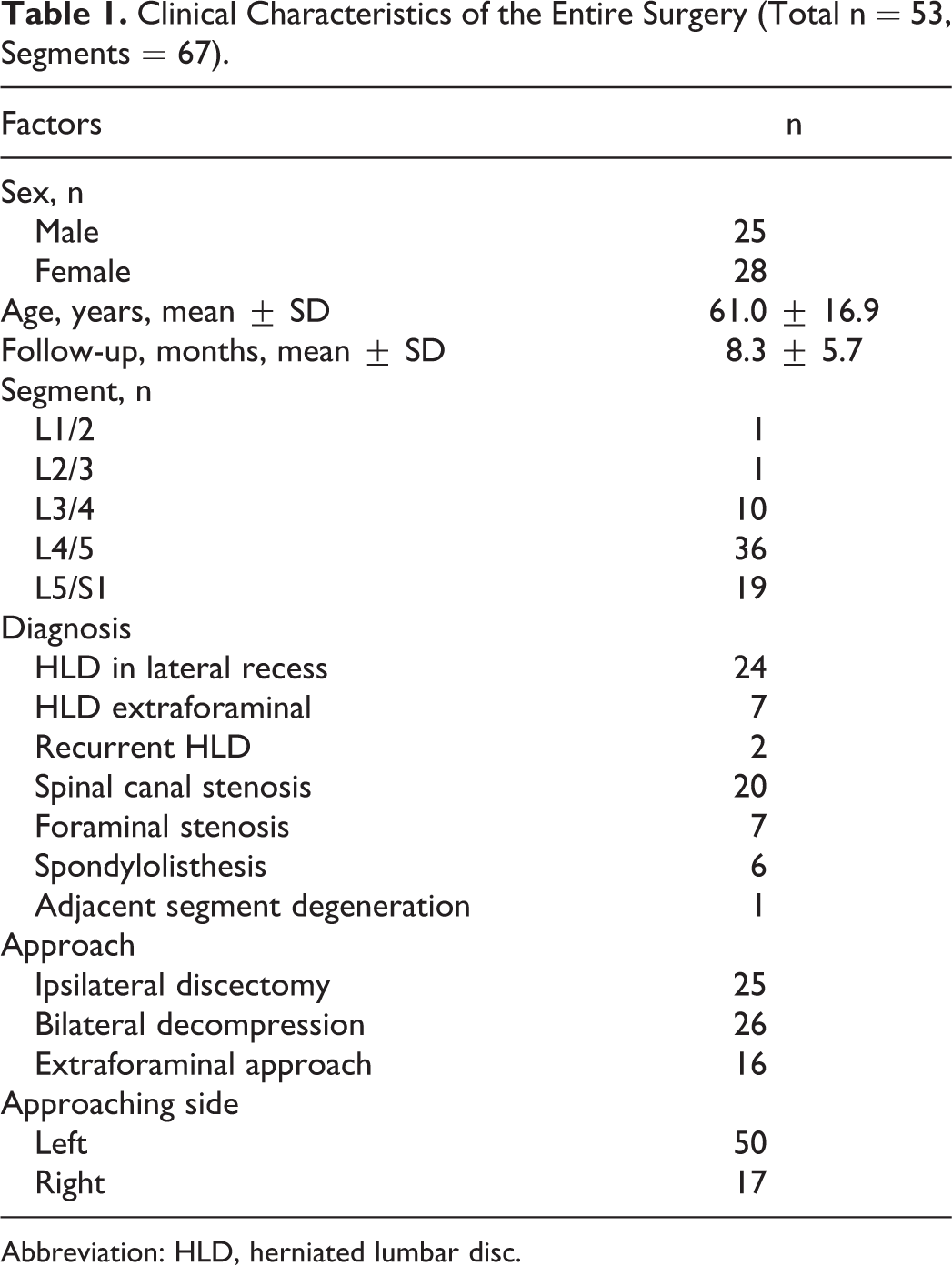
Abbreviation: HLD, herniated lumbar disc.
Dural Injury of the Thecal Sac
Three injuries occurred in the dorsal aspect of the thecal sac: one injury occurred with the extraforaminal approach, and the remaining two injuries occurred with bilateral decompression.
Clinical and Surgical Features of the Dural Injuries.
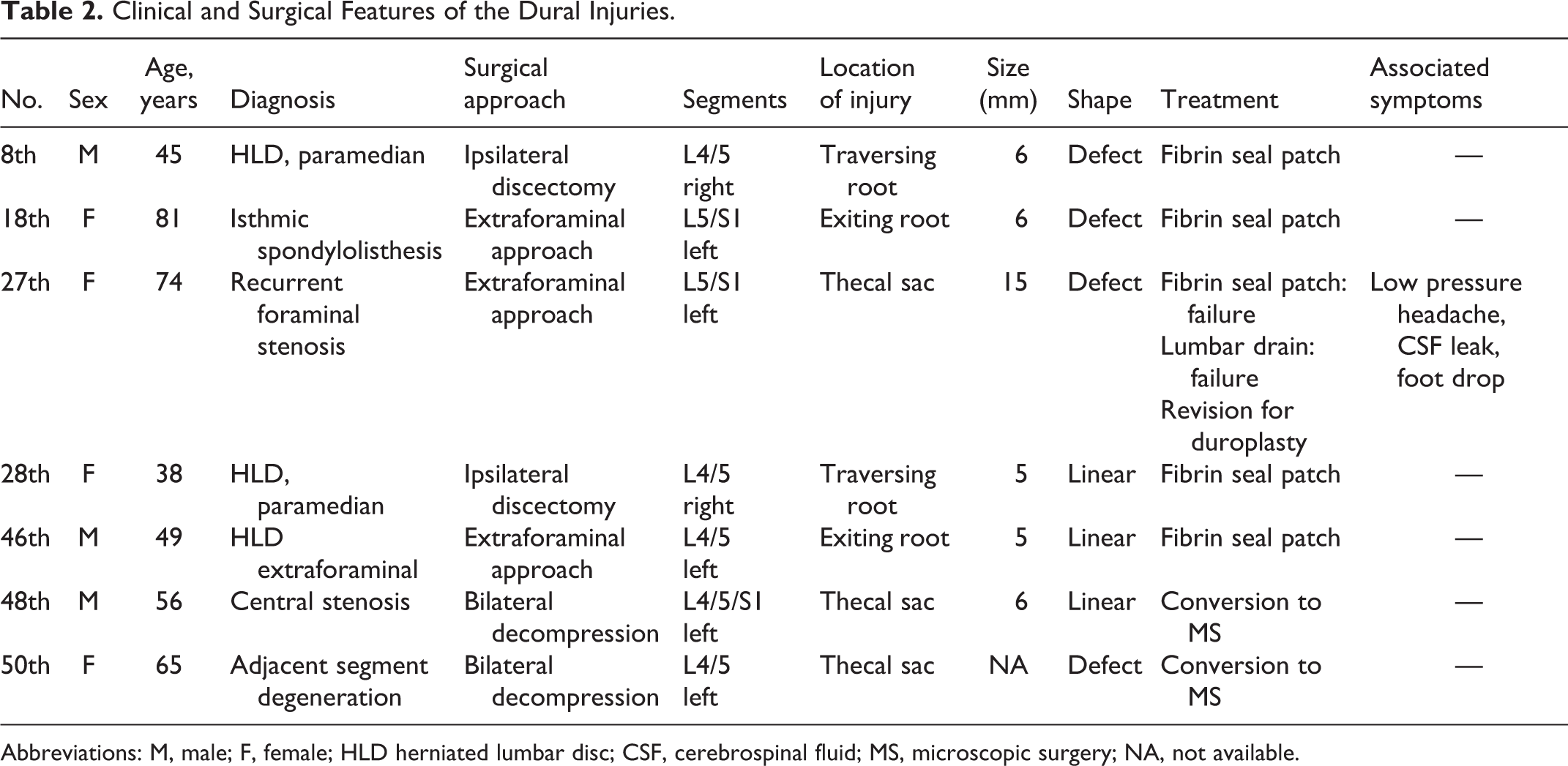
Abbreviations: M, male; F, female; HLD herniated lumbar disc; CSF, cerebrospinal fluid; MS, microscopic surgery; NA, not available.
In a 74-year-old woman (Case 27), thecal sac injury occurred because of an adhesion from a previous surgery and because the lateral recess was unexpectedly reached early during the extraforaminal approach. The injury occurred during the removal of the ligament flavum with the forceps and was accompanied by cauda equina damage. A defect, but not a linear injury, occurred. A surgical sponge was loosely placed on the lesion during the surgery. We did not lower the hydrostatic pressure during the operation; therefore, the intracranial pressure (ICP) may have been elevated. She had a drowsy mental status after general anesthesia and required 10 hours to regain full consciousness.
From postoperative day 1, cerebrospinal fluid (CSF) leakage occurred in the wound. On a postoperative magnetic resonance imaging (MRI) scan, only a small collection of fluid under the muscle layer was observed (Figure 1). We successively attempted a reinforcement suture with a large thread, compression dressing, and lumbar drainage catheter insertion; however, all these efforts failed. The CSF leakage was eventually stopped with duraplasty using artificial dura under microscopic vision.
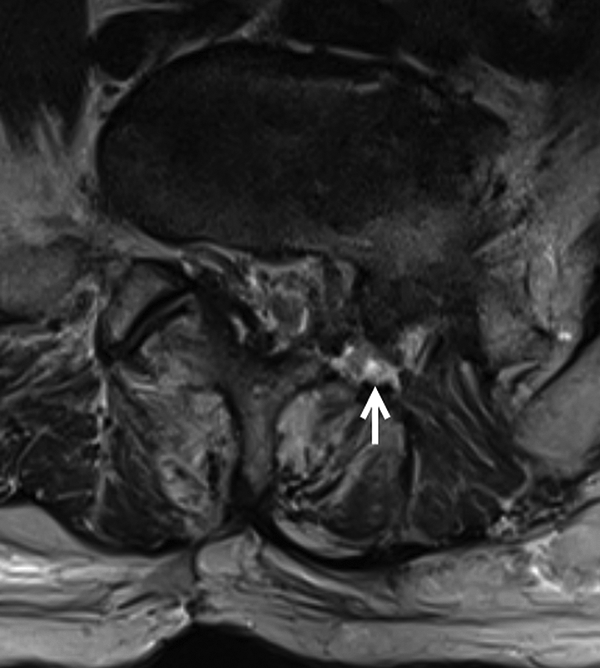
Postoperative magnetic resonance imaging in case 27. The white arrow indicates the accumulation of cerebrospinal fluid in the area where the facet was removed.
The other 2 cases of thecal sac injury occurred during removal of the ligament flavum in bilateral decompression. These injuries incurred primarily during the removal of the midline ligament flavum near the upper or lower lamina in a piecemeal fashion with a punch or a pair of forceps, which resulted in a defect rather than a linear injury. This error was attributed to the insufficient dissection of the posterior meningo-vertebral ligament connecting the dura and the periosteum of the lamina. In case 48, the cauda equina herniated through defects because of severe redundancy of the cauda equina in the thecal sac (Figure 2). In case 50, the patient had a diagnosis of adjacent segment degeneration, and the dissection of the perimeter of the dural injury was difficult because of the formation of an adhesion after the injury. Both these patients then underwent microscopic surgery, and the dura was directly repaired. No clinical complications such as postoperative CSF leakage occurred.
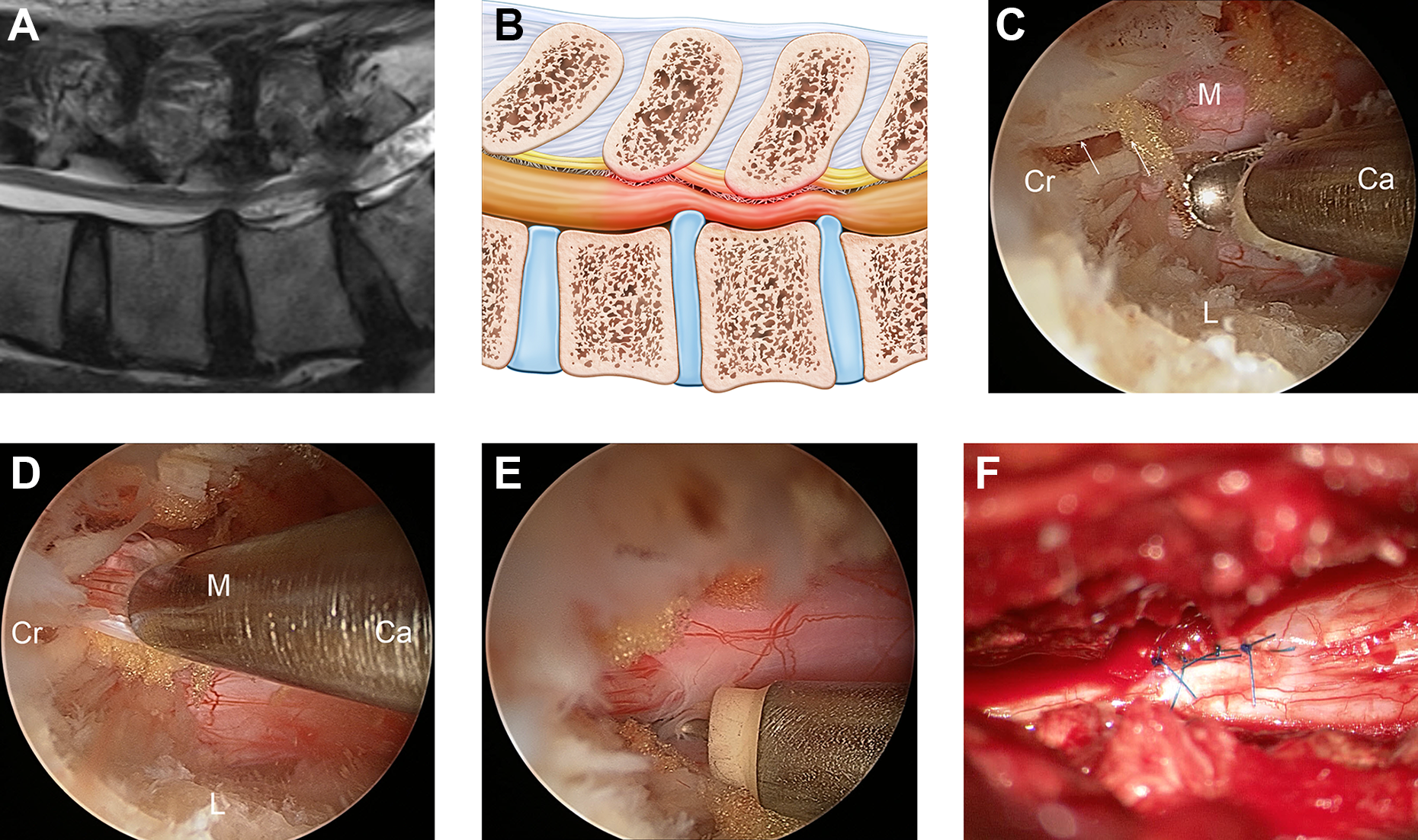
Case 48 with the dural injury of the thecal sac. (A) Preoperative magnetic resonance imaging showing central stenosis and redundancy of cauda equina in L4/5 and L5/S1 segments. (B) A simplified schematic design depicts meningo-vertebral ligaments under the ligament flavum. (C) The ligament flavum is removed in a piecemeal fashion at the L5/S1 segment. The white arrow points to the ligament flavum of the midline. (D) Injury of the cauda equina occurred by erroneous punching of the central folding of the midline dural sac. (E) A dural defect is observed in the central thecal sac, and the risk of nerve herniation and incarceration was present due to redundancy of cauda equina. (F) The dural defect was sutured under microscopic vision, and the patient recovered without cerebrospinal fluid leakage after surgery. M, midline; L, lateral side; Cr, cranial direction; Ca, caudal direction.
Dural Injury of the Traversing Root
In case 8, damage was caused when the shoulder of the traversing roots was pushed in a medial direction to expose the disc lesions. In Case 28, a dural injury occurred during discectomy because of the repetitive friction from the insertion and removal of the forceps without root retraction. In both patients, surgery was terminated after reinforcement with a fibrin seal patch was applied to the injury site. No postoperative clinical event such as increased ICP or CSF leakage occurred.
Dural Injury of the Exiting Root
In the extraforaminal approach, small blood vessels bleed frequently from a detaching adhesion (Figure 3). Two cases of belated recognition of dural injury occurred. Both operations were also terminated with a fibrin seal patch. Cerebrospinal fluid leakage was not observed on a postoperative MRI scan.
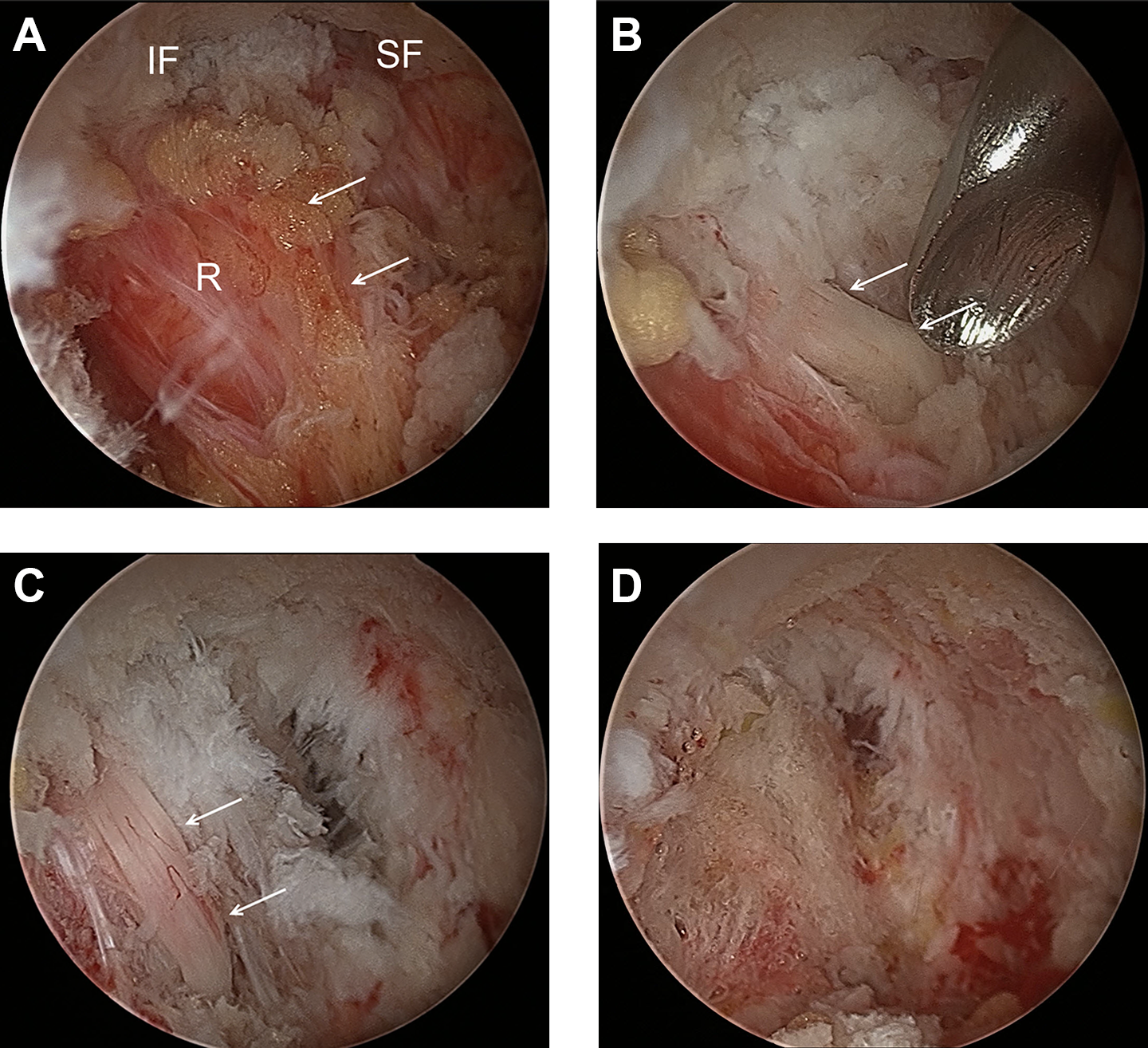
Case 46 with dural injury of the exiting root. (A) During the left far lateral approaches, an exiting root is observed after partial inferior and superior facetectomy and removal of the ligament flavum. The white arrow points to the inferior margin of the exiting root. The boundary is unclear due to the surrounding hyperemia. (B) During the dissection process, dura injury occurred and the root (white arrow) was exposed. Since there were no blood vessels on the root, it was difficult to distinguish them from the surrounding ligament. (C) After discectomy, the blood flow increased, showing a typical root shape. (D) Fibrin seal patch was applied and cerebrospinal fluid leakage was not observed. IF, inferior facet; SL, superior facet; R, exiting root.
Discussion
Incidental durotomy is the most common complication during spinal surgery and has an incidence rate of 1.8% to 14%. 13,14 UBES has been recently introduced; however, there have been few studies that have focused on its complications. One systemic review mentions an incidence rate of 1.5% to 5.8% for dural injury. 10 Other studies have reported that patients with a dural tear that is recognized and treated during endoscopic spinal surgery have a relatively better outcome; therefore, a thorough diagnosis and secure treatment decisions for a dural tear are important. 15 The purpose of this retrospective study was to analyze the pattern of dural injury during UBES and to report its clinical course.
Mechanism of Dural Injury
Dural breach and subsequent CSF leakage can occur through various mechanisms. In this study, we frequently observed a tear in the dorsal face of the dural sac, primarily during the removal of the ligament flavum (Figure 2B). The meningo-vertebral ligament is a web-like anatomical structure that links the dorsal side of the dura with the lamina and ligament flavum. 16 -18 This ligament can vary in thickness and shape ranging from thin strips to thick sheets, and is primarily distributed in the midline or near the midline surface. Insufficient dissection of this structure may be the main mechanism of injury.
In UBES, the dural sac can be detached from the ligament flavum because of hydrostatic pressure. However, near the midline, a central folding occurs because of the meningo-vertebral ligament, which is vulnerable to injury with the same dissection approach as that used for the periphery. Dural central folding is usually hidden under epidural central fat tissue. Therefore, access to the contralateral side over the epidural fat is recommended by Choi et al. 19
In addition to dural deformation resulting from hydrostatic pressure during surgery, one disadvantage of UBES is the use of a single instrument portal. In “2-handed” microscopic surgery, the dura can be easily exposed by retracting the structures at the surgical site with the nondominant hand. However, the dissection should be performed without retraction in UBES, and this process requires surgical experience.
We recommend the removal of thin strips between the ligament flavum and dura with an angled curette and confirming the detachment before using a punch or a pair of forceps to bite the ligament flavum. Laminectomy that is sufficiently wide to allow for visualization of the cranial and caudal edges of the ligament flavum and removal of the ligament in an en bloc fashion can also be helpful in reducing injury.
Many epidural vessels exist within the meningo-vertebral ligament and are easily damaged. Endoscopic vision is frequently obscured, even with a small amount of bleeding, which increases the risk of dural injury. Monopolar coagulation is primarily used for hemostasis, which surgeons are hesitant to perform because of the lack of safety guidelines for its use in the surgical circumstance of UBES. Accumulation of a small amount of bleeding can obscure the field of vision and increase the risk of a dural breach. Thorough hemostasis is usually needed whenever bleeding occurs before moving to the next steps.
In patients with chronic pain in the lumbar spine, changes in the epidural space such as root hyperemia, fibrosis, and increased vascularity of the periphery are common. 20,21 In the extraforaminal approach, the exiting root is often difficult to recognize because of this pathological condition. After anatomic orientation is determined by intraoperative radiography, surgeons can safely perform a dissection around the upper pedicle while being mindful of the exiting root.
In cases where an additional discectomy is performed after removal of an extruded or protruded disc herniation, repetitive friction occurs at the shoulder of the traversing root, which results in dural injury. To prevent this outcome, an annular window should be made for the insertion of the instrument outside of the traversing shoulder or continuing the use of the retractor when inserting the instrument.
Management of Dural Injury
If a dural injury is detected during surgery, a temporary barrier against water pressure should be formed by applying a gelfoam or fibrin seal patch. In general, patients with dural injury after UBES complain of headache or sweating owing to a low postoperative ICP. 22,23 Unlike other endoscopic surgeries, irrigation is used to create spaces in UBES, which can raise the ICP once a dural breach occurs. A previous report described cases of intraoperative back or neck pain caused by irrigation fluid pressure, although the dura was not torn during surgery. 24 In the current study, a delayed awakening after anesthesia occurred in one patient, which was presumed to be a result of the increased ICP. Therefore, lowering the height of the irrigation fluid hanger after injury should be considered.
To date, there is a lack of consensus in the literature regarding the management of incidental durotomy in UBES. Park et al 25 suggested a strategy for managing an incidental durotomy by sorting, based on size and location of injury, including the traversing root, exiting root, and thecal sac. They recommended absolute bed rest and simple observation for small tears of less than 4 mm. For large defects of more than 12 mm, especially in the thecal sac, they suggest conversion to microscopic direct repair.
Kim et al 26 experienced 27 incidental durotomies and categorized them based on the size, location of the injury, and incarceration of a nerve root; however, they did not create a direct classification for dural injury in UBES. They recommend using a simple fibrin seal patch for traversing root injury, and open repair for complex dural injury larger than 1 cm. Their strategy highlighted the risk of nerve incarceration in addition to the size and location of the injury. Even with a minor injury in the cranial-caudal direction of less than 1 cm, if nerve root incarceration is a concern, enlarged durotomy to prevent incarceration was considered. For a large defect, irregular margin, or accompanying incarceration of the nerve root, an open repair was considered a safe treatment method.
In the series presented in this article, we experienced secondary microscopic repair of pseudomeningocele owing to a large and irregular defect of the thecal sac. We thereafter intraoperatively switched to an open repair for two patients with dural injury in the thecal sac. One patient was at risk of incarceration of nerve root because of the redundancy of the cauda equina, and the other patient had an eminent adhesion because of previous surgery.
Eismont et al 27 suggest performing a delicate and complete closure of a durotomy that is recognized at the time of surgery. They insisted on running locked sutures or simple sutures using fat graft, or fascial graft with interrupted suture and revalidation via the Valsalva maneuver. One case study reported treatment of pseudomeningocele with revisional UBES 22 ; however, given the risk of meningitis or pseudomeningocele in a case of failed repair, it is difficult to conclude whether the repair with UBES is safe.
In general, transforaminal endoscopic spinal surgery is beneficial in preventing CSF leakage because it passes through a small 1-cm corridor and follows a 10- to 15-cm long muscle trajectory. 28 In UBES, the trajectory is relatively shorter than that of the transforaminal approach, but has the same strengths. However, on account of the narrow field of view, it is relatively disadvantageous for confirming an incidental durotomy. Another disadvantage is that indirect reinforcement such as patch reinforcement or loose stitches with a surgical clip is possible during management.
Several limitations of this study need to be acknowledged. In this study, a relatively small number of patients were examined. As a consequence, the statistical significance in the context is difficult to determine. The incidence rate of dural injury in this study was relatively higher than that of existing studies, presumably because the surgeon was a novice for UBES and experiencing a learning curve. However, this study is sufficiently meaningful because it provides a surrogate experience for novice surgeons to reduce serious clinical complications.
Conclusions
Incidental durotomy is a common complication in UBES. Owing to the nature of UBES, which is performed without retraction with one hand, delicate dissection of the meningo-vertebral ligament is important in the approach. Surgeons should carefully consider the treatment options from a simple patch to open repair, based on the location, size, irregularity of the margin, and risk of incarceration of the nerve root.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.