
Abstract
Study Design
Cross-sectional survey.
Objectives
To determine the prevalence and predictors of incidental durotomy (ID) among AO Spine surgeons globally, and assess current management strategies and associated complications.
Methods
An electronic questionnaire was distributed to 937 AO Spine surgeon members in October-November 2024, to collect data on surgeon demographics, work characteristics, experience with ID, and preferred management techniques. Logistic regression identified predictors of frequent IDs (>5% of surgeries). Significance was set at P ≤ 0.05.
Results
Surgeons reported ID frequencies ranging from 1% to >20%. Overall, 12% reported frequent IDs. Longer surgical experience (OR = 0.406, P = 0.031) was protective, while working in a public/ governmental hospital (OR = 1.775, P = 0.023) was a risk factor. Medium-sized IDs (1-10 mm) were most common in lumbar surgery (52.2%). Sutures and sealants were commonly used for medium and large tears. Prolene sutures (76.5%) and autologous grafts (53.8%) were preferred. Subfascial drains without suction were frequently used. Management of large and medium tears commonly included 48 and 24 hours of bed rest, respectively. Immediate ambulation was most frequent for small tears. Most surgeons (79.2%) reported occasional or rare complications from dural tears, with a significant association with dural graft repair (OR = 1.946,P < 0.001). Disclosure of IDs to patients was nearly universal (97.3%).
Conclusion
The study highlights the frequency with which incidental durotomy occurs globally during spinal surgery. Longer surgical experience was a protective factor of frequent ID, while working in a public/ governmental hospital was a risk factor. Standardized protocols for small tears or guidelines for deciding between repair and non-repair are recommended.
Introduction
One of the most frequent side effects of spine surgery is incidental durotomy (ID). Depending on the kind of surgery and its complexity, the incidence reported in the literature ranges from 1 to 17%.1,2 The frequency of dural damage associated with spinal surgery was 5.8%, according to a meta-analysis of 23 studies. 3 Two commonly known risk factors associated with increased dural rips are revision procedures and dural calcifications/adhesions. Devastating side effects, such as delayed wound healing, surgical site infection, pseudo-meningocele formation, arachnoiditis, and generally poor surgical results, can arise from prolonged cerebrospinal fluid (CSF) leakage caused by dural injuries.4-6 Dural rips can occasionally result in significant medico-legal issues as well as long-term clinical aftereffects.7,8 Only a few studies, if any, have found that patients with appropriately identified and repaired rips do not experience an increase in perioperative morbidity or complications.
A systematic review and meta-analysis of 49 papers on managing unintentional dural rips during spine surgery found that the overall failure rate for spinal dural repair, irrespective of treatment modality, was 6.1%. 9 Therefore, in practical practice, dural repair materials should be replaced regularly. 10 A questionnaire was administered to members of the Canadian Neurological Surgical Society to explore methods of closure of iatrogenic durotomy, showed areas of uncertainty about iatrogenic dural tear management, and disagreement regarding management of anterior and nerve root tears, pinhole-sized tears in any location of the spine, and whether patients should be admitted to hospital or should be on bed rest following a pinhole-sized dural tear. This study recommended a robust comparative research study of dural repair strategies. 11 Thus, several unanswered questions remain concerning proper intra- and postoperative care and consequences after dural damage. Therefore, the purpose of this study was to determine the prevalence of frequent dural tears as reported by AO spine surgeons around the world, as well as to identify the predictors of frequent dural tears, describe current surgical practices and management strategies for spinal dural tears, and list the complications that arise after an incidental dural injury.
Methods
AO Spine represents a premier global academic community dedicated to advancing education and research in spine care. A cross-sectional electronic questionnaire survey was conducted among spine surgeon members of AO Spine across various AO regions over two months in October and November 2024. All active on-duty surgeons at the time of the survey were eligible for inclusion. A total of 937 surgeons submitted valid, completed questionnaires. Questionnaires with incomplete responses or missing data were excluded.
Data Collection
An online survey generator created a web-based, cross-sectional survey informed by a comprehensive literature review and expert insights.12,13 A panel of experts performed a preliminary screening through consensus, followed by testing an initial version of the questionnaire on a pilot sample of 5 Orthopedic surgeons and 5 Neurosurgeons with diverse years of experience to address ambiguity, confirm comprehension, and assess completion time. In response to their feedback, certain questions were rephrased to enhance clarity. In developing the final questionnaire, we assessed the logical arrangement of items and the anticipated relationships between responses to ensure overall coherence. The tool demonstrated strong internal consistency, evidenced by an overall Cronbach’s alpha of 0.83. This survey was reviewed and approved by the AO Spine Degenerative Knowledge Forum. The e-questionnaire comprised three sections designed to gather data on demographics, experiences with spinal dural tears, and preferred management techniques,11,13-15 as outlined below:
Section (1) encompasses work-related characteristics that examine the nature of participants’ responsibilities. Enquiries concerning the work environment, spine practice community, workload volume (including estimated population served, specialty—orthopedics or neurosurgery, years of experience, surgical caseload, workdays per week and hours per operational day), and overall workload level were incorporated.
Section (2) provides information regarding incidental durotomy. Enquiries regarding the incidence of durotomy includes categories of infrequent (<1% of surgeries), moderate (1–5%), and frequent (>5% of surgeries). Additionally, considerations involve the complication rate, types of complications, and the extent of disclosure to patients, categorized as always, sometimes, or never. Dural tears were categorized as small (<1 mm), medium (1 to 10 mm), and large tears (>10 mm) based on surgeons’ subjective estimates.
Section (3) Management of dural tear. The enquiries focused on management types (sutures, sealant, artificial dural patch, tissue graft, drain), materials utilised (Silk, Prolen, Gortex, others), sealant classifications (fibrin glue, synthetic, others), patch categories (autologous graft, absorbable collagen, dura substitute, others), drain types (subfascial under negative pressure, subfascial without suction, subcutaneous drain), and postoperative protocols (immediate ambulation or the following day, bed rest for 24 hours, 48 hours, or longer).
This study was conducted electronically from October to November 2024, involving three contacts (including two reminders), which yielded an 82% response rate (Of 1143 surgeons contacted, 937 surgeons responded).
Data Analysis
Data analysis was conducted using SPSS software version 28 for data entry and analysis. Descriptive statistics were employed, including mean score, standard deviation, frequency, and percentages of all independent variables. Analytic statistics were utilized to examine the associations between the frequency of dural tears and work-related characteristics. The Pearson chi-square and Chi-square tests for linear trend were employed for qualitative data analysis. Univariate analyses investigated the associations between frequent dural tears (occurring in more than 5% of the surgeries performed by the surgeon) and potential risk factors. Logistic regression analysis was conducted to identify the key predictors of frequent dural tears, incorporating only those independent variables that demonstrated significance in the univariate analyses (Years of experience, training background, and practice setting). Another logistic regression analysis was conducted to identify the association between different ID repair techniques and post-ID complications, adjusting for all independent variables that showed significant associations with complications in univariate analyses (region, practice setting, specialty, and years of experience). Odds ratios and their corresponding 95% confidence intervals were calculated to evaluate the strength of association of potential risk factors with frequent dural tear and its complications. Significance was defined as P-values of ≤.05.
Results
Demographic and Work-Related Characteristics of the Study’s Spine Surgeons
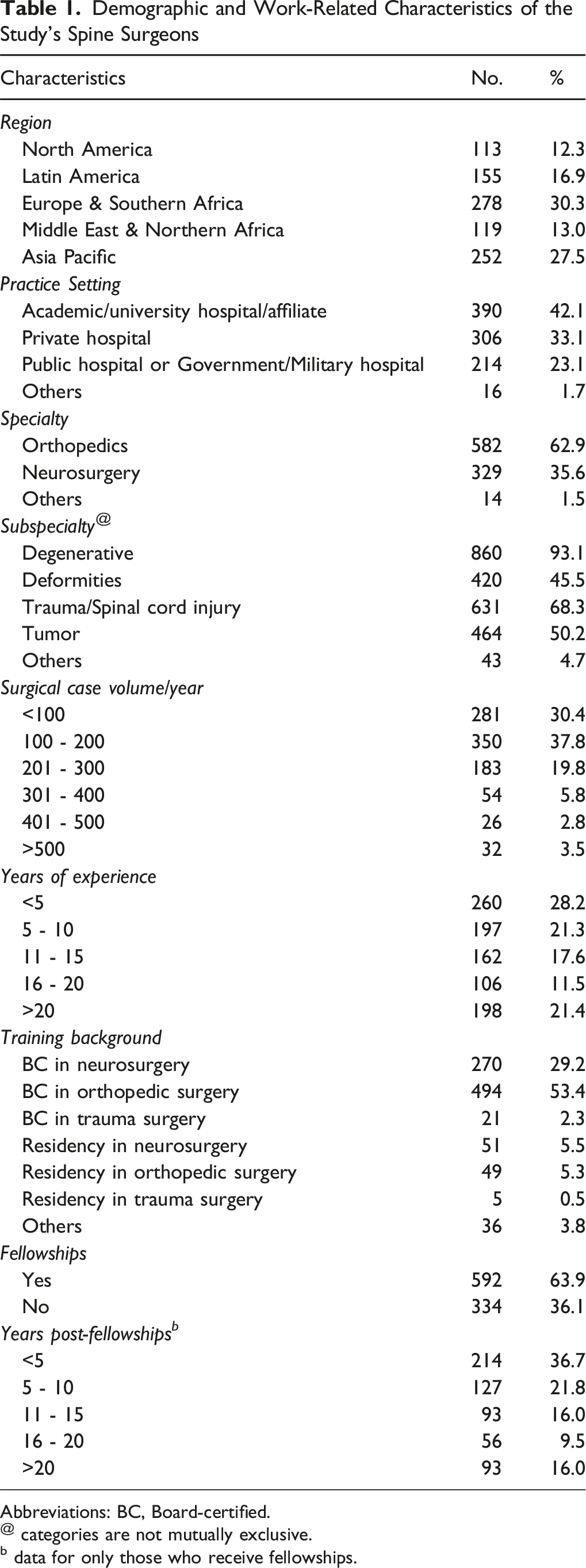
Abbreviations: BC, Board-certified.
@ categories are not mutually exclusive.
b data for only those who receive fellowships.
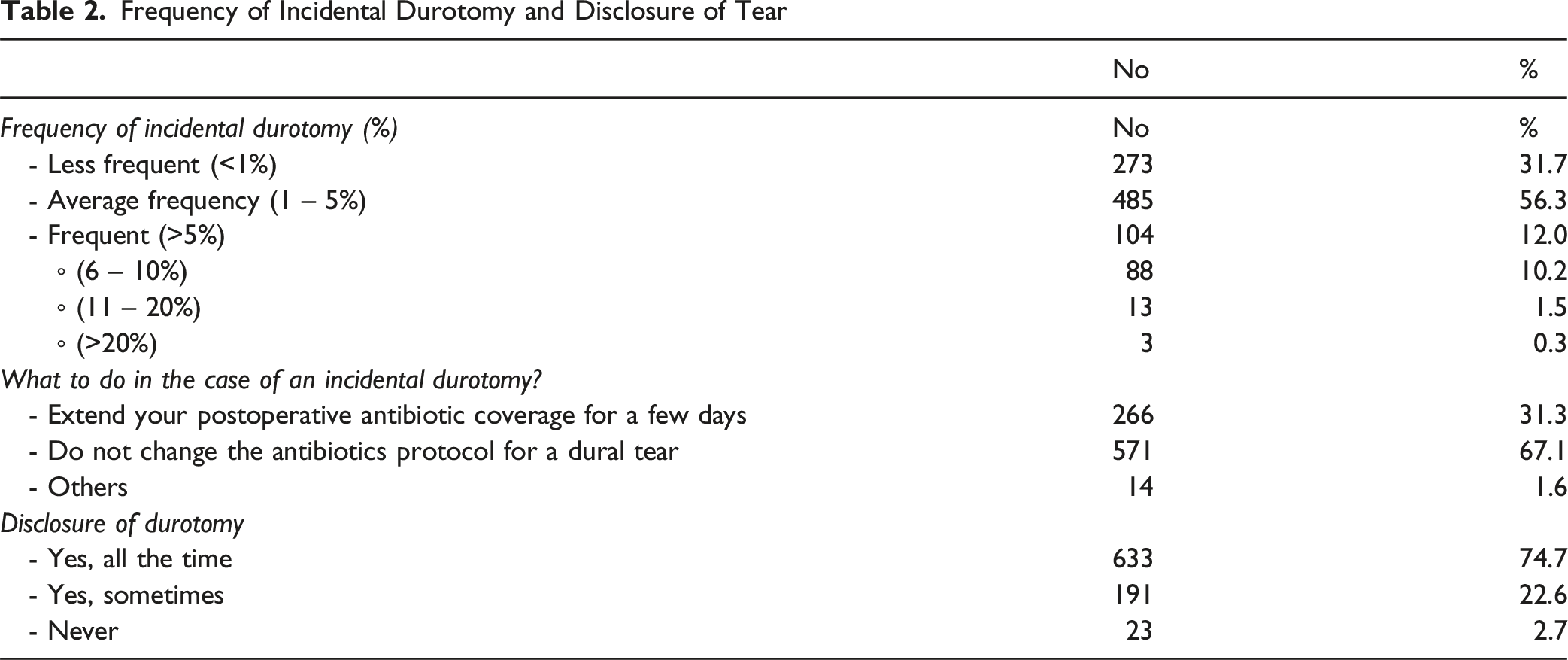
Frequency of Incidental Durotomy and Disclosure of Tear
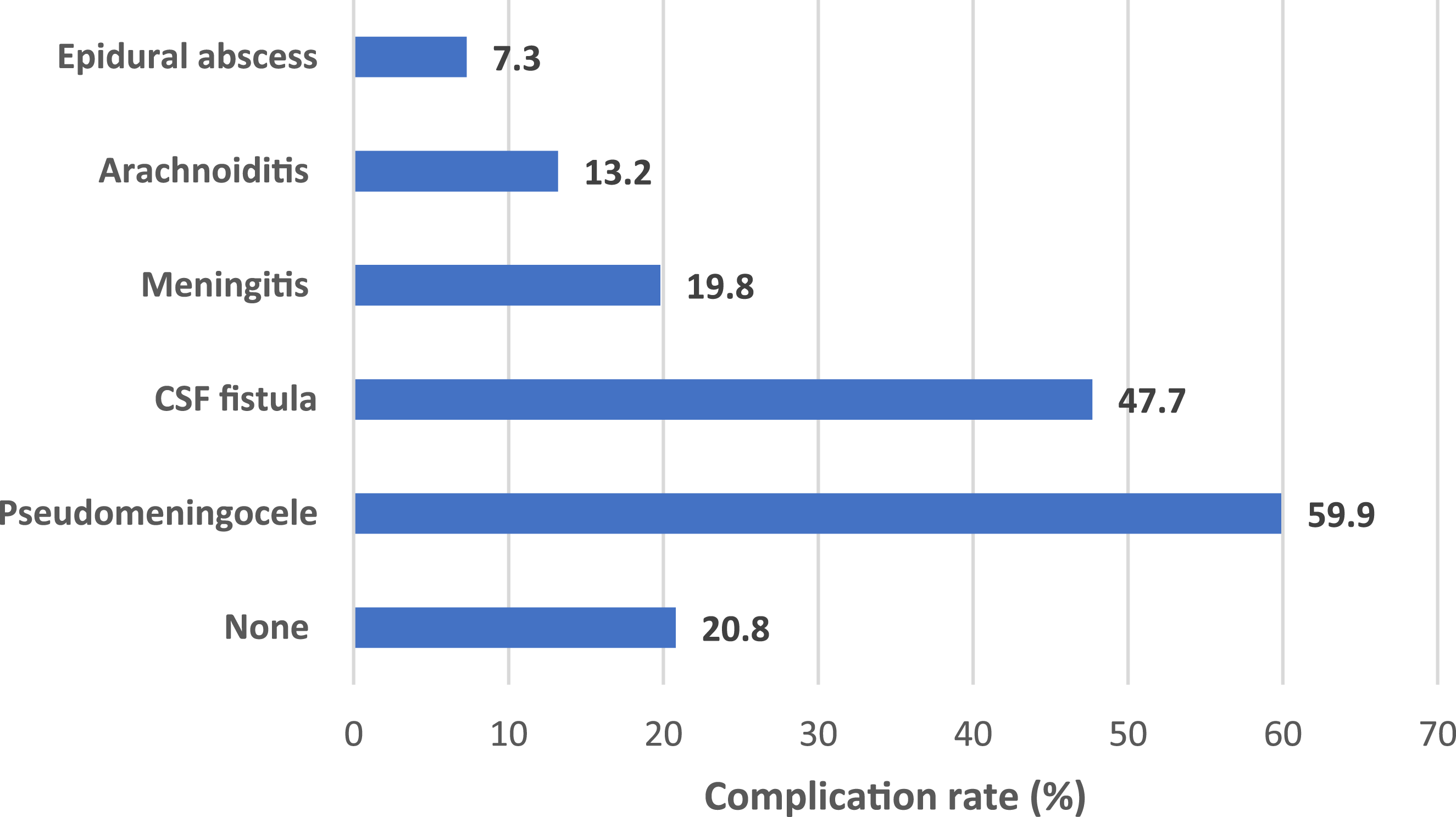
The Rate of Different Complications of Incidental Durotomy
Management of Dural Tear According to Tear Size
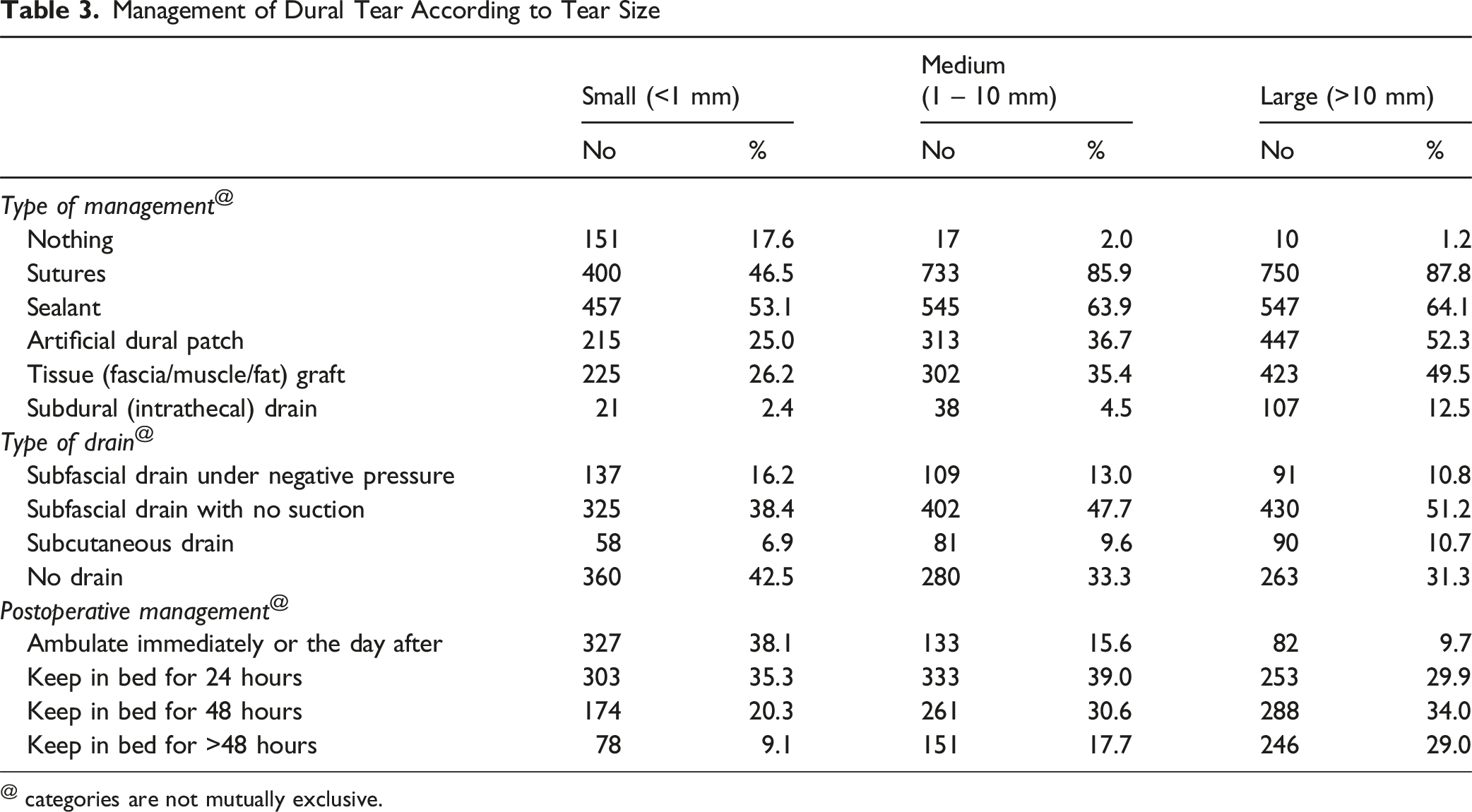
@ categories are not mutually exclusive.
The subfascial drain without suction was the predominant type of drain utilised across all sizes of dural tears, with usage rates of 38.4%, 47.7%, and 51.2% for small, medium, and large tears, respectively.
The predominant management approach for large tears involved 48 hours of bed rest (34%), whereas 24 hours was the most prevalent strategy for medium-sized tears (39%). Immediate ambulation or ambulation the following day was the most common management approach for small-sized tears (38.1%), while it was the least common for large-sized tears (9.7%).
Figure 2 shows the repair techniques according to different geographical distributions. Patch and sealant were more frequently used in ID repair in North America, while they were the least frequently used in the Middle East and North Africa (P < .001). There was no significant geographical difference in the use of sutures in repair (P = .32) Repair Techniques of Incidental Durotomy in Different Geographical Regions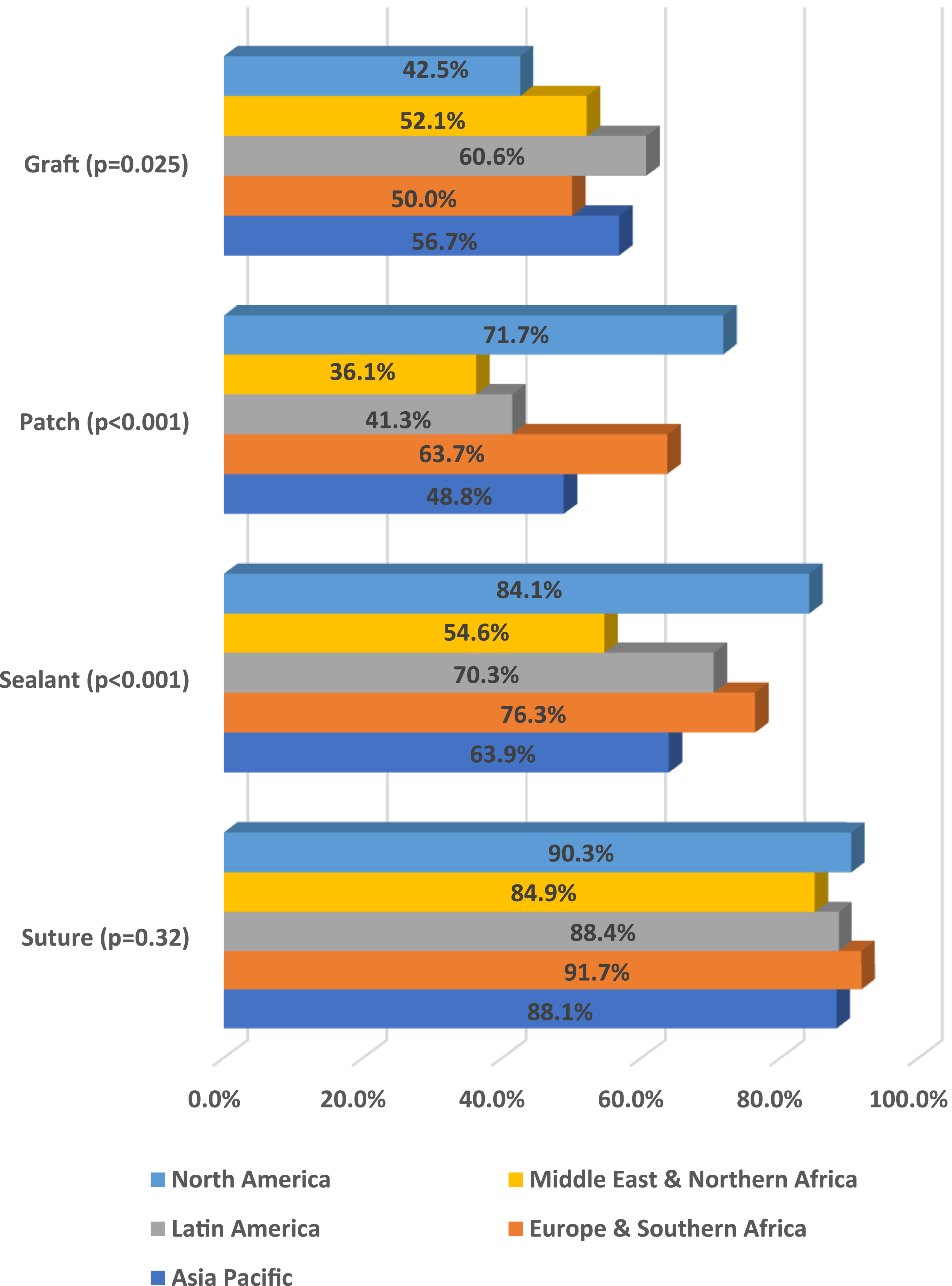
Types of Suture Materials, Sealants, and Patches Used in Dural Tear
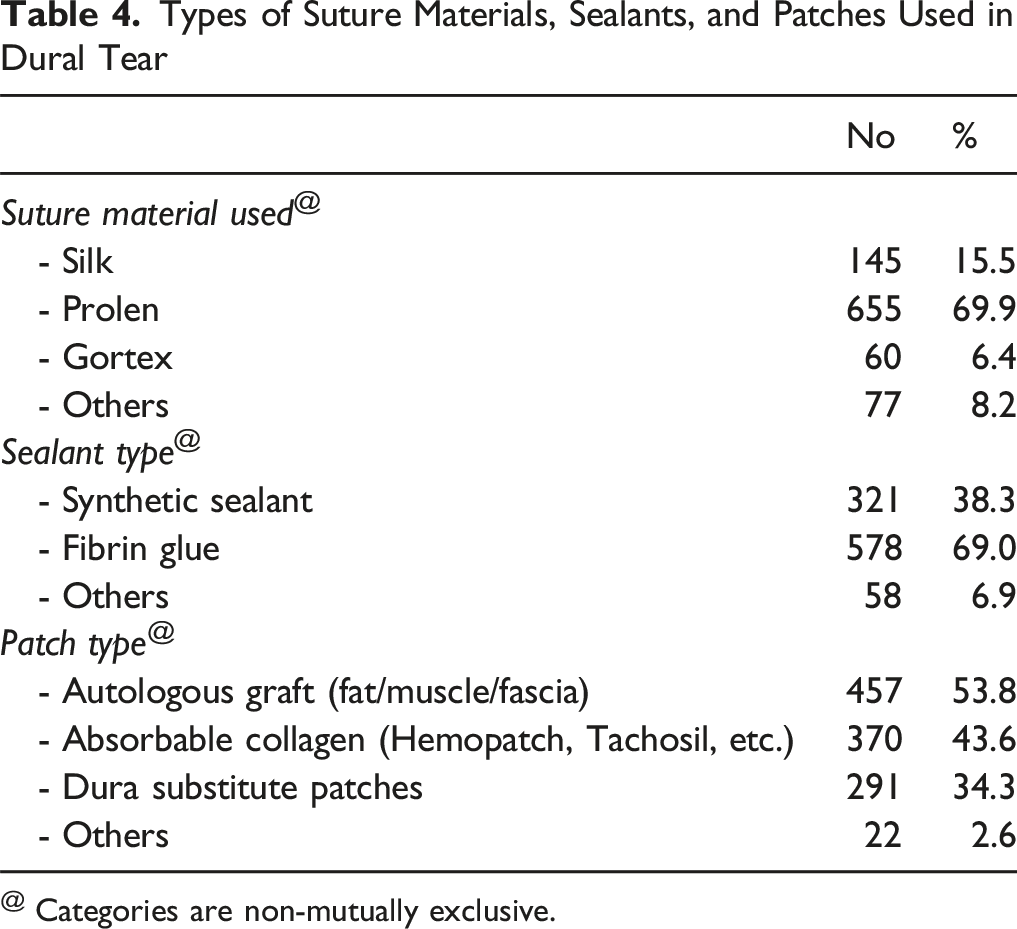
@ Categories are non-mutually exclusive.
Prevalence of Frequent Dural Tears (>5% of Surgeries) and Associated Factors
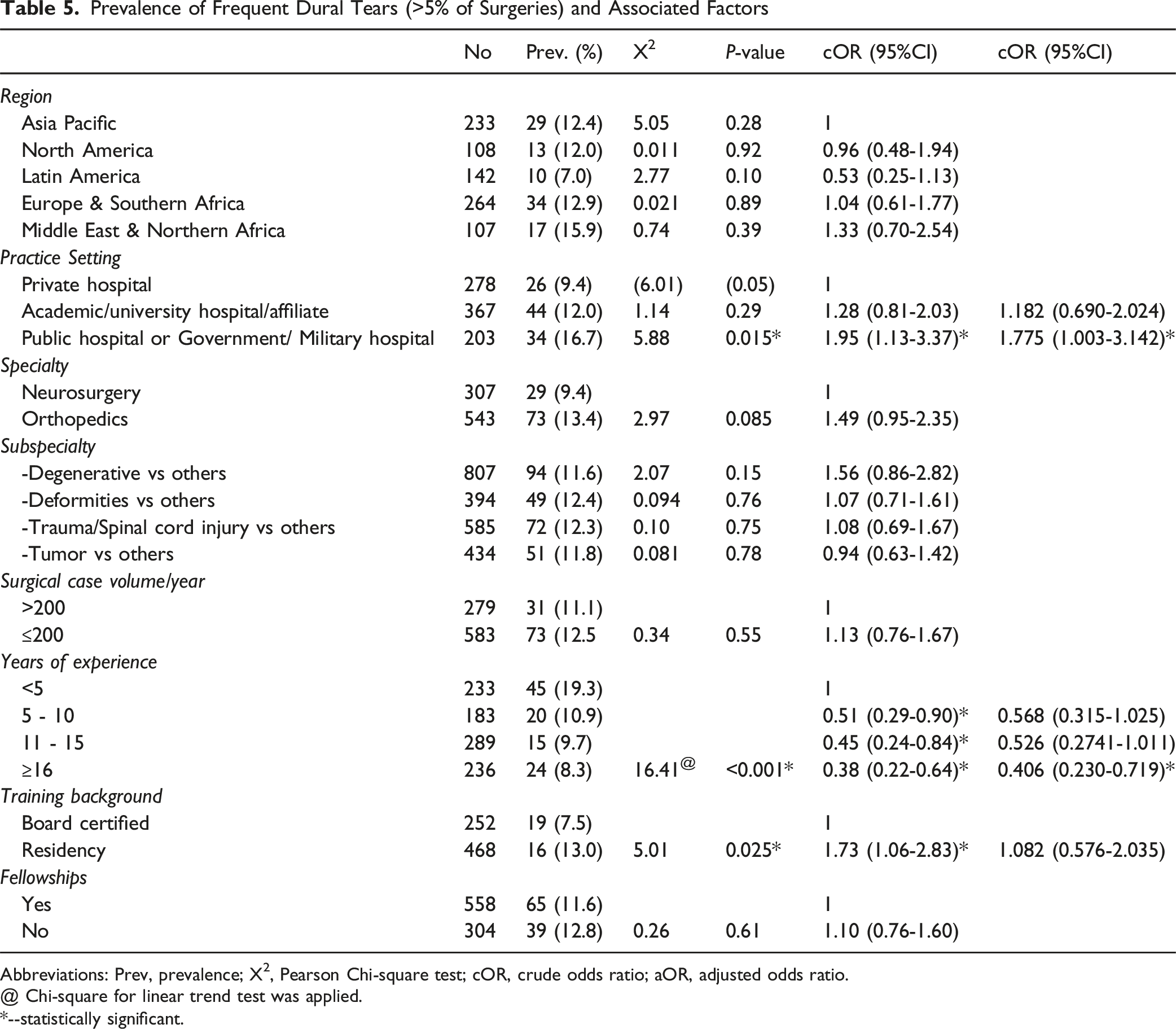
Abbreviations: Prev, prevalence; X2, Pearson Chi-square test; cOR, crude odds ratio; aOR, adjusted odds ratio.
@ Chi-square for linear trend test was applied.
*--statistically significant.
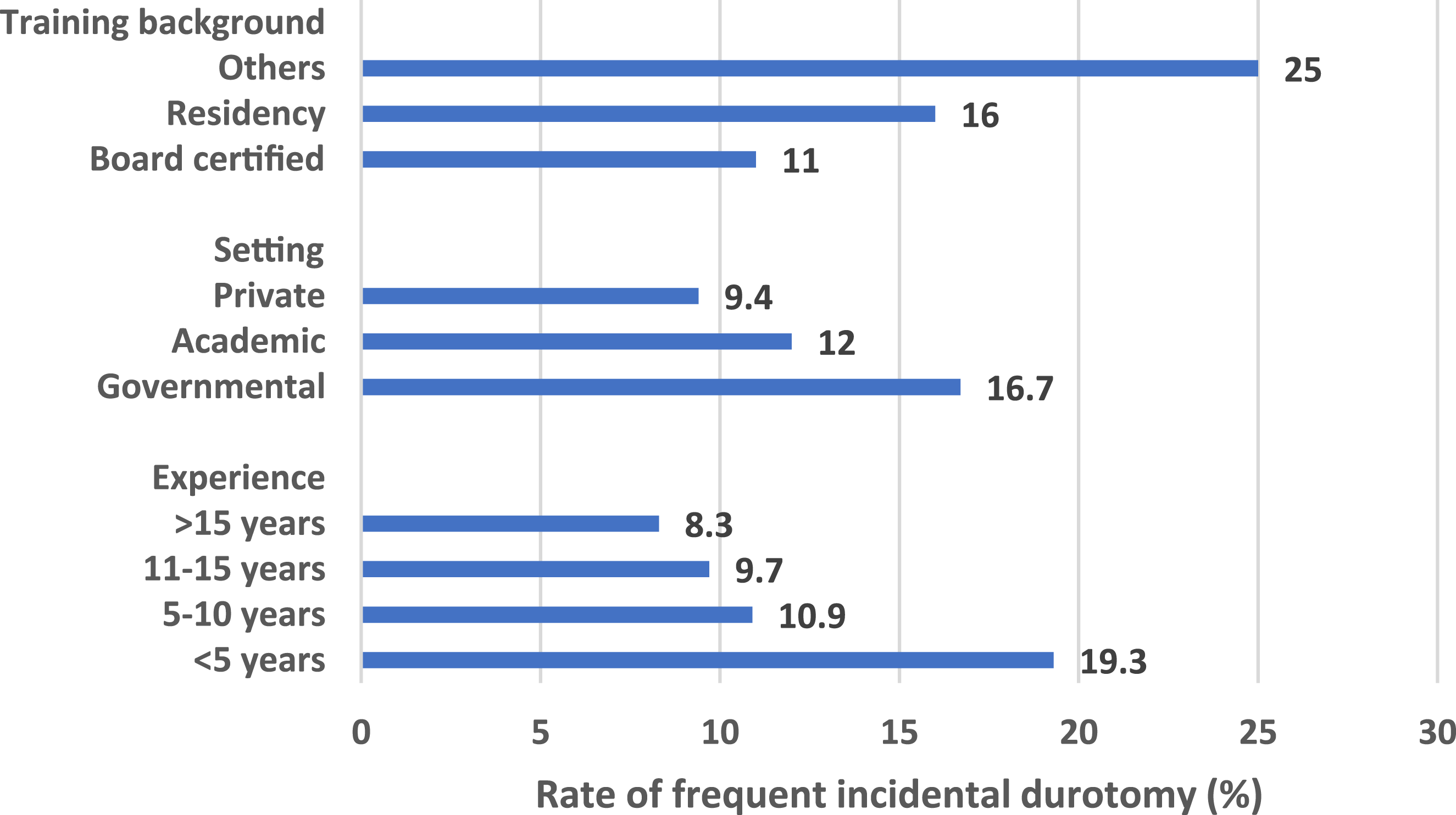
Rate of Frequent Incidental Durotomy according to Surgical Experience, Setting, and Training Background
Surgeons with five or more years of experience in spine surgery exhibited a higher prevalence of frequent tears than their counterparts with less than five years of experience. The prevalence of frequent tears decreased significantly from 19.3% in the less experienced group to 10.9%, 9.7%, and 8.3% in the groups with 5-10 years, 11-15 years, and 16 years or more of experience, respectively (X2 LT = 16.41, P < .001), as illustrated in Figure 3. After adjusting for confounders, longer surgical experience of 16 years or more was significantly associated with a lower rate of frequent ID (OR = 0.406, 95% CI 0.230-0.719, P = .031). Regarding the surgeon’s training background, individuals with residency training reported a higher prevalence of frequent tears than those board certified (13.0% vs 7.5%, OR = 1.73, 95% CI 1.06-2.83, P = .025), as illustrated in Figure 3. However, after adjustment, this significant association disappeared.
Association of Incidental Durotomy Repair Techniques With the Rate of Post-incidental Durotomy Complications, Adjusting for Some Potential Confounders
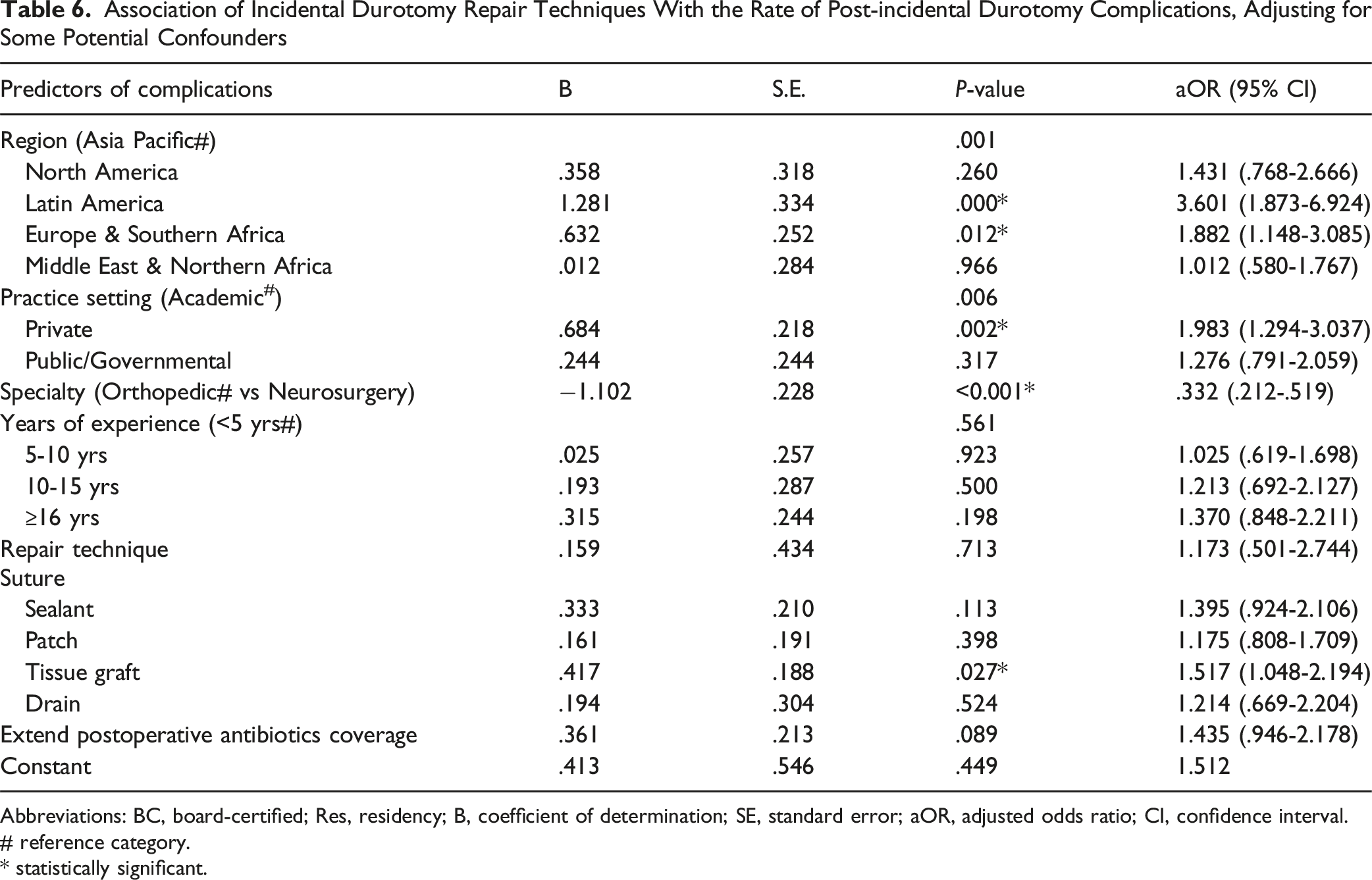
Abbreviations: BC, board-certified; Res, residency; B, coefficient of determination; SE, standard error; aOR, adjusted odds ratio; CI, confidence interval.
# reference category.
* statistically significant.
Discussion
Incidental durotomy is a recognised complication of spine surgeries, occurring with greater frequency in surgical practice due to the rising incidence of both primary and revision spine procedures globally.1511 The overall incidence of dural injuries in a prior study was 2.3%, with a higher incidence rate of 16.6% observed in revision surgery cases, 16 which aligns with the current literature.17-20 In this study, surgeons reported the frequency of dural tears to range from 1% to over 20% throughout their careers, with the majority indicating a 1-5% (56.3%). This figure would align with the frequency of 5.8% reported in a meta-analysis of 23 studies. 3 Only 1.8% of surgeons indicated experiencing more than 10% durotomies over their careers, whereas a prior study found that 70% of durotomies were reported by 20.4% of surgeons. 21
In our study, most surgeons indicated experiencing one or more complications from dural tears. Pseudomeningocele was the most common complication of incidental durotomy, occurring in more than half of the cases, followed by CSF fistula, meningitis, arachnoiditis, and epidural abscess. In a prior study, 21 CSF fistulas occurred in 0.025% of all patients. Radiculopathy with dysesthesia was reported by 12.4% of surgeons, sensory loss by 3.4%, and motor weakness by 2.2%. Higher rates of ID complications were associated with orthopedic surgeons, surgeons working in Latin America, Europe & North Africa, surgeons in the private sector, and with ID repair using dural graft.
It has been reported that more than half of surgeons did not engage in any repair or closure, while 40% utilized sealants, and 7.8% attempted endoscopic sutures. 21 In our study, no interventions were performed for 17.6%, 2%, and 1.2% of small, medium, and large-sized tears, respectively. Sutures and sealants were utilized for most medium-sized and large-sized tears, and nearly half of the small-sized tears. A survey of Canadian spinal surgeons 11 revealed a lack of consensus on closure methods for pinhole-sized tears, with a notable trend towards sealant fixation at 36.7%. In our study, medium- and large-sized tears are primarily closed using sutures and sealant. Patch and sealant were more frequently used in ID repair in North America, while they were the least frequently used in the Middle East and North Africa. There was no significant geographical difference in the use of sutures in repair.
Traditionally, direct repair has been considered the optimal approach for managing dural tears. Suture materials such as monofilament polypropylene and braided nylon are utilized for their hydrostatic strength.22,23 In this study, fibrin glue emerged as the predominant sealant, accounting for more than half of the cases, while synthetic sealants comprised one-third. Synthetic grafts have emerged as an alternative to autologous fat and muscle grafts for dural repair. 16 The identified benefits encompass the capacity to establish a secure seal and the potential for use in dural defects of various irregular shapes and sizes. 16 In our study, using a dural graft for ID repair was associated with a higher rate of complications. The patch effect, dead space-filling effect, adherence, and interstice-filling effect are significant properties of these substitutes. 24 Prolene was utilised as the suture material by most surgeons, accounting for two-thirds of usage. Most surgeons utilised autologous grafts (fat/muscle/fascia) as the primary type of patch, followed by absorbable collagen and dura substitute patches. In a prior investigation, 21 DuralSeal emerged as the predominant brand of commercially available sealant, accounting for over one-third of usage. Additional sealants utilised included Tisseal, Evicel, and generic sealants.
In a clinicopathological study of synthetic dural grafts conducted by Narotam et al, 25 the collagenous matrix demonstrated advantages via its chemotactic interaction with dural fibroblasts. A retrospective review of 110 patients indicated that collagenous grafts effectively sealed the tear in over 95% of cases. 26 Grannum et al 27 found that non-suturing repair techniques, such as autologous and synthetic grafts, effectively address dural tears in lumbar spine surgery, with no reported adverse events or complications. In this study, the most frequently utilized patch was an autologous graft of fat/muscle or fascia, accounting for 53.8%, followed by an absorbable collagen patch at 43.6%. The study revealed no significant differences in complication rates among the different dural repair techniques. This aligns with findings from other studies.16,28 Therefore, a patch may be utilized solely as a repair option when there are constraints regarding primary dural repair, such as the defect’s location and configuration. A prior study involving Canadian spinal surgeons indicated that Tisseal was favored by most of the respondents compared to other sealants. 11
The literature lacks a clear consensus on the use of drains. A limited number of authors have advocated for the routine placement of drains in all patients with dural tears.29-31 In contrast, several other studies18,32 have supported the decision against the placement of drains, as the epidural hematoma typically serves as a tamponade for the dural rent. Additionally, drains may introduce a risk of contamination and the potential development of a duro-cutaneous fistula at the drain site. Our study found that one-third to one-half of surgeons reported not placing a drain for varying-sized tears. The predominant type of drain utilized for all dural tear sizes was a subfascial drain without suction. In a prior study, 16 the authors found no significant differences in immediate postoperative complications or infection rates between groups with and without drain placement. The decision to place drains should be based on individual cases, dural repair adequacy, and the surgical site’s anatomical dead space.
Traditionally, literature has advocated for prolonged bed rest to prevent persistent dural leaks and decrease hydrostatic pressure at the site of dural tear repair. 24 Complications of prolonged immobilization in patients with dural tears have been documented. 33 Previous studies indicated no significant differences in complication rates between early (<24 h) and late (>24 h) mobilization in patients with dural tears. A systematic review indicated that early mobilization significantly reduced complications such as headaches, tinnitus, nausea, and vomiting.34,35 In our study, 48 hours of bed rest was the predominant management strategy for large tears, whereas 24 hours was the most frequently utilized approach for medium-sized tears. Immediate ambulation or ambulation the following day was the most common management approach for small-sized tears, while it was the least common for large-sized tears. One-half of surgeons advised 48 hours of bed rest, while 40.4% suggested less than 24 hours. 21 In a prior investigation involving Canadian spinal surgeons, it was found that, aside from pin-hole-sized tears, most respondents advised bed rest for a minimum of 24 hours in cases of medium and large dural tears. 15
Before a procedure, the surgeon must communicate the advantages and possible risks associated with the surgical treatment to the patient. Surgeons must maintain transparency with patients regarding their care to prevent confusion and potential self-incrimination as complications occur. 36 In our study, almost all surgeons indicated that they disclose the occurrence of incidental tears to patients at all times, or they do so sometimes. An orthopedic surgery department established a confidential, real-time reporting system for intraoperative adverse events and conducted analyses of these events during structured morbidity and mortality conferences. 37 While physicians believed this process enhanced patient care, it led to a notable rise in reported error rates, which, as indicated by the authors, may have contributed to diminished quality ratings for the department. 37 Our study showed that longer surgical experience was a protective factor for frequent ID. This could be attributed to technical expertise or case selection. Natural tension exists between the surgeon’s objective of elucidating the potential causes of errors and the need to empathize with the patient, their family, or other carers while mitigating legal risks. 36 In our study, public/governmental hospitals increase the risk of frequent IDs, perhaps due to resource constraints or patient complexity.
Strengths and Limitations
This questionnaire differs from prior assessments by being a detailed survey encompassing work-related characteristics, enquiries regarding the frequency of durotomy, complication rates, types of complications, and disclosure of tears. It also includes questions about management strategies, materials, sealant types, patch types, drain types, and postoperative management practices. This study linked the kind of repair to the size of durotomy, an essential aspect for advancing future research. The sample size is substantial, encompassing diverse spine surgeons across various subspecialties, including neurosurgeons and orthopedic surgeons from multiple global regions. The response rate is satisfactory, allowing for a thorough examination of the uncertainties associated with managing dural tears. This would enable the generalization of our study’s conclusion.
The study presents several limitations. Methodological differences in studies across disciplines, predominantly retrospective, constrain comparisons within the general population. The anonymous nature of the survey limited the ability to compare responder and non-responder populations, thereby introducing the potential for selection bias. The reliance on self-reported data may introduce recall or social desirability bias, as surgeons might underreport complications or overreport adherence to best practices.
Future studies could mitigate this limitation by targeted follow-ups or demographic comparisons. This cross-sectional study cannot establish causality; thus, the causal relationship between the outcome (frequent dural tears) and potential risk factors such as hospital type, training background, and years of experience remains uncertain. Lastly, although the questions presented in this survey assist in pinpointing areas of uncertainty, we cannot ascertain the optimal closure methods for different types of dural tears due to the absence of individual patient data with follow-up.
Conclusion
This research employed a questionnaire to assess the prevalence of intraoperative dural tears globally among spinal surgeons and the contentious elements of their management. This study clarifies the uncertainties surrounding the management of iatrogenic dural tears. There is a lack of consensus on managing small-sized dural tears, specifically concerning the necessity of hospital admission or bed rest for patients following such an event. Standardized protocols for small tears or guidelines for deciding between repair and non-repair are recommended. However, potential barriers to their implementation, such as variations in healthcare systems and surgeon preferences, must be considered. A robust comparative research study of dural repair strategies is necessary.
The primary area of uncertainty is managing small, medium, and large dural tears. Repairs are primarily conducted using a combination of sutures and sealants. Respondents concur that a period of bed rest, along with hospital admission, is generally advisable. As tear size diminishes, consensus on optimal management decreases, with outcomes leaning towards “no repair” or sealant-only fixation for more minor tears.
Randomized controlled trials for closure techniques and longitudinal studies are recommended to assess long-term outcomes of different bed rest durations. Conducting cost-benefit analyses of different strategies would be highly beneficial, particularly considering the strain on healthcare systems, especially in pinhole-sized tears.
Footnotes
Acknowledgment
This survey was organized and funded by AO Spine. AO Spine is a clinical division of the AO Foundation, an independent, medically guided, not-for-profit organization.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest concerning this article’s research, authorship, and/or publication.