
Abstract
Study Design
Systematic Review.
Objective
Endoscopic cervical spine surgery (ECSS) has emerged as a minimally invasive alternative to traditional open surgery for certain cervical spine disorders. ECSS may offer potential advantages such as reduced tissue trauma, shorter hospital stays, and accelerated functional recovery. Technological advancements have further enhanced its feasibility. The purpose of this article is to review current ECSS approaches, systematically review ECSS for cervical stenosis, and explore future directions of ECSS.
Methods
The PubMed, Embase, and Google Scholar databases were searched systematically until October 20, 2024, adhering to PRISMA guidelines. We searched keywords associated with cervical stenosis, including “endoscopic cervical surgery”, “endoscopic cervical discectomy”, “endoscopic cervical foraminotomy”, “cervical endoscopic unilateral laminotomy for bilateral decompression”, and “unilateral bilateral endoscopy”. We excluded duplicate publications, review articles, preprints, and studies without clinical outcomes or incomplete information. Clinical outcomes and complications were collected.
Results
A total of 12 studies were included with 2 studies being reported twice for having two different ECSS approaches. Each study reported postoperative improvement in clinical outcomes compared to preoperative measurements. The most common complications included dural tears, transient hypesthesia, and CSF leakage.
Conclusion
ECSS is an emerging alternative for treating select cases of symptomatic cervical stenosis and other cervical conditions. Complications differed depending on the approach. Advancements in endoscopic instruments, navigational technologies, and artificial intelligence hold promise for improving preoperative planning, surgical precision, and patient outcomes. The true value of ECSS will require carefully conducted prospective, controlled studies with rigorous assessment of outcomes and complications.
Keywords
Introduction
The global population is currently seeing an upward trend of its age structure and a significant increase in health burden due to spinal disorders, specifically in the elderly population. 1 With an aging population in which comorbidities are more prevalent, spine surgery is undergoing a paradigm shift from traditional open surgical procedures to minimally invasive techniques in order to potentially improve surgical outcomes. 2 Among these surgical advancements, endoscopic spine surgery is emerging as a potential alternative. Endoscopic spine surgery offers a number of potential benefits compared to traditional open surgery including minimal bony and soft tissue disruption, better visualization of the surgical field, improved blood loss mitigation, and diminished postoperative pain.3,4 Advancements in technology have enabled endoscopic surgery to expand treatment to certain spinal pathologies such as spinal stenosis, prolapsed intervertebral disc, and degenerative disc disease.5,6
Development of an endoscopic anterior cervical approach was attempted in the past with both an animal model and in patients with herniated cervical discs, but the technique did not gain widespread adoption due to potential complications in high-quality instruments.7,8 Percutaneous techniques were also gaining popularity during this time with the inception of percutaneous nucleotomy, and Tajima et al. was the first to detail the procedure of an anterior percutaneous endoscopic cervical discectomy.9,10 The advent of a full-endoscopic cervical technique did not occur until 2007, after the maturation of endoscopic techniques for the lumbar spine. 11 From then on, anterior and posterior endoscopic cervical approaches have been steadily refined, demonstrating improvement in clinical outcomes and reduction in complication rates.12,13
Endoscopic cervical spine surgery (ECSS) is evolving as an alternative procedure in the treatment of select cervical spine conditions. With the integration of advanced imaging systems, robotics, and artificial intelligence, endoscopic spine surgeries are only further advancing their capabilities to enhance precision and outcomes. Given the swift advancements, this manuscript intends to explore the current state and future prospect of ECSS by examining the various endoscopic techniques and equipment and addressing its impact on successful surgical interventions. Understanding the trajectory of cervical spine surgery paves the way for continued innovation that will ultimately improve the patient’s well-being.
Methods
Search Strategy and Criteria for Selection
A systematic review following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines was conducted to identify articles related to endoscopic cervical surgeries and cervical stenosis. Three databases were examined from their inception through October 20, 2024, including PubMed, Embase, and Google Scholar. The following query terms were used in combination and adjusted accordingly for each specific database: “endoscopic cervical surgery” OR “endoscopic cervical discectomy” OR “endoscopic cervical foraminotomy” OR “cervical endoscopic unilateral laminotomy for bilateral decompression” OR “unilateral biportal endoscopy” AND “cervical stenosis.” Inclusion criteria were retrospective or prospective cohort studies, as well as comparative studies that incorporated a type of endoscopic surgical technique for patients with cervical spinal stenosis. Exclusion criteria were case reports, systematic reviews, preprints, review articles, non-English publications, or articles that reported no clinical outcomes (Figure 1). PRISMA Flow Diagram. Screening and Selection Process of Endoscopic Cervical Surgery for Cervical Stenosis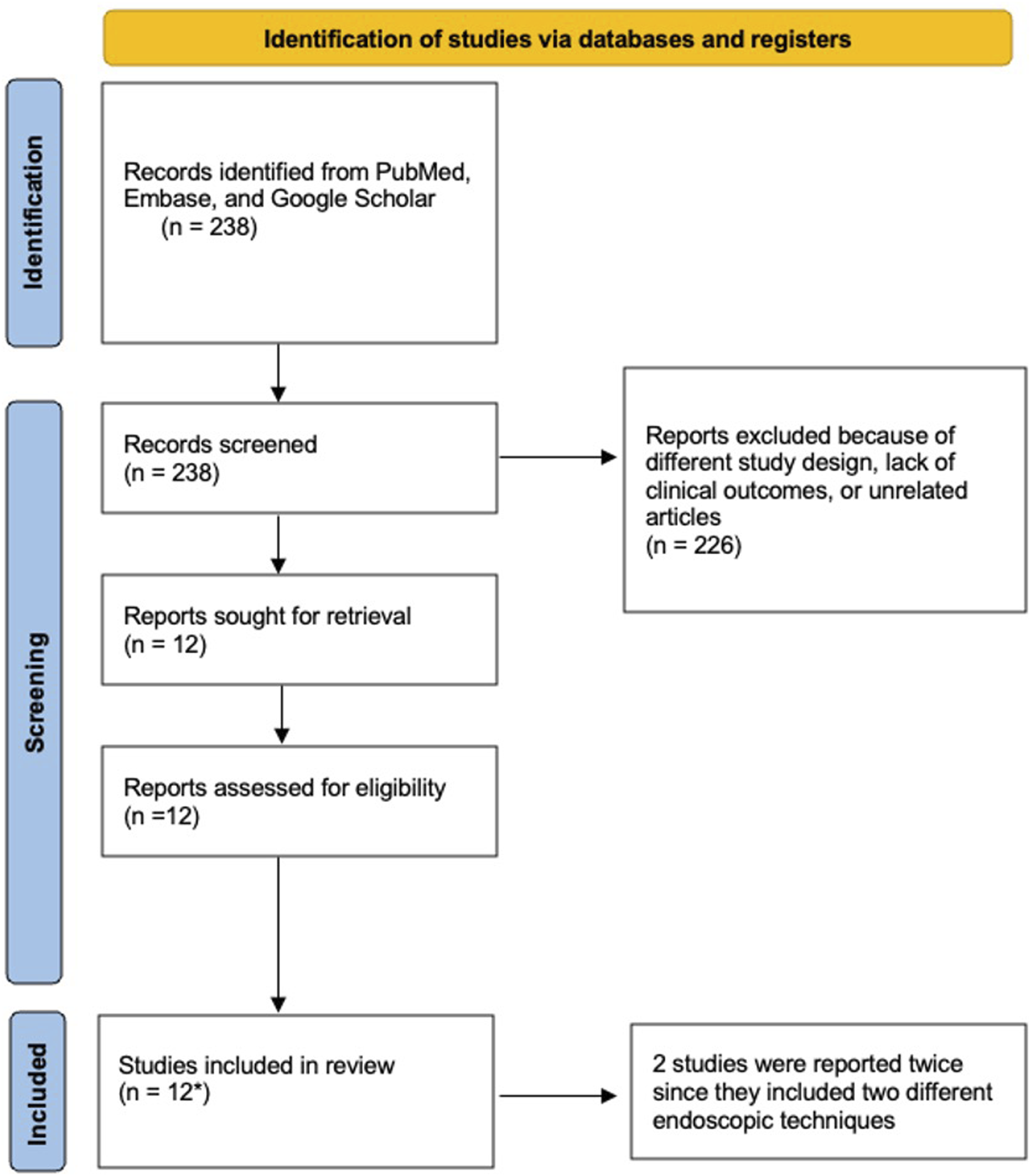
Data Extraction
Demographics
Postoperative Outcomes
Complications
Results
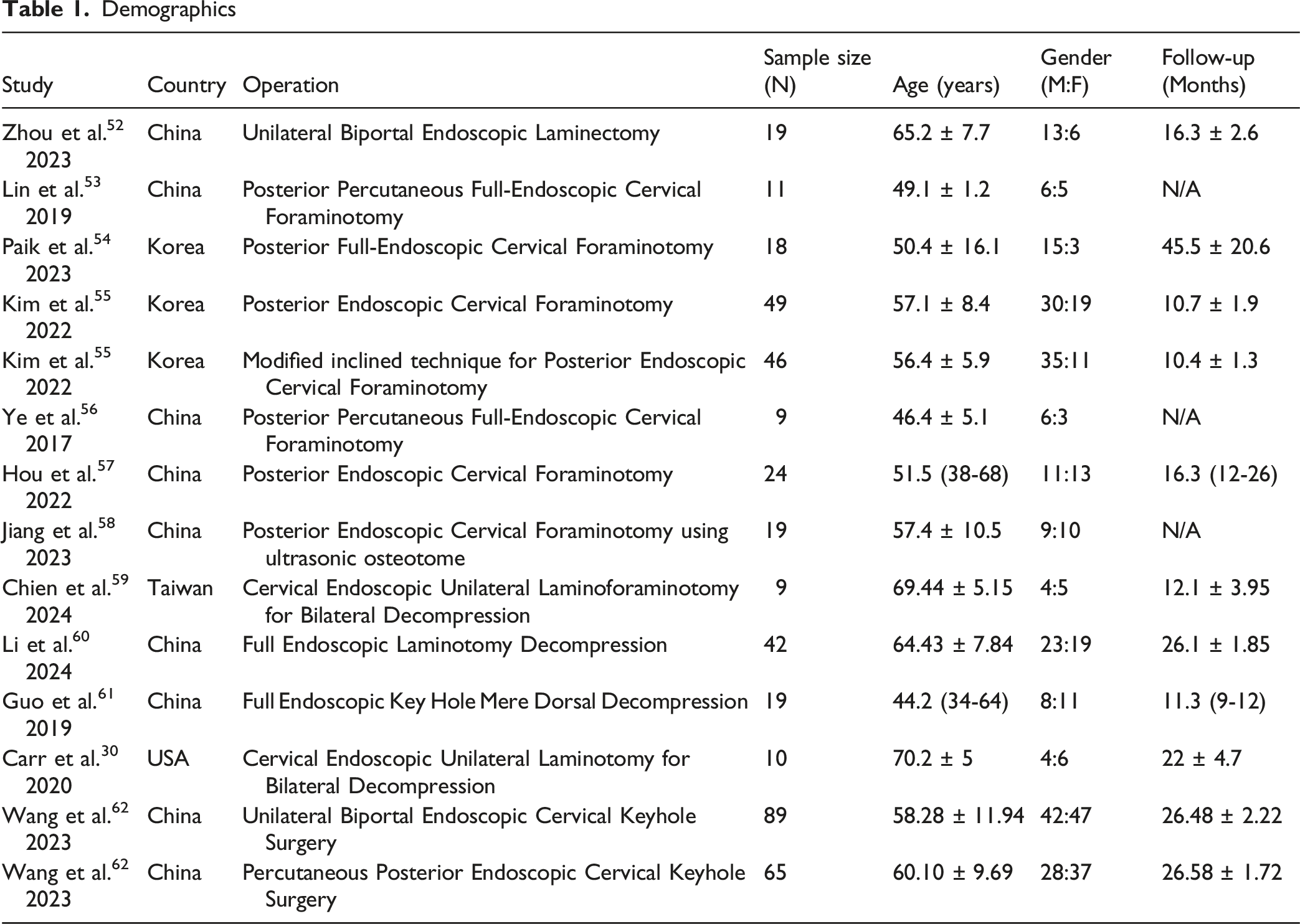
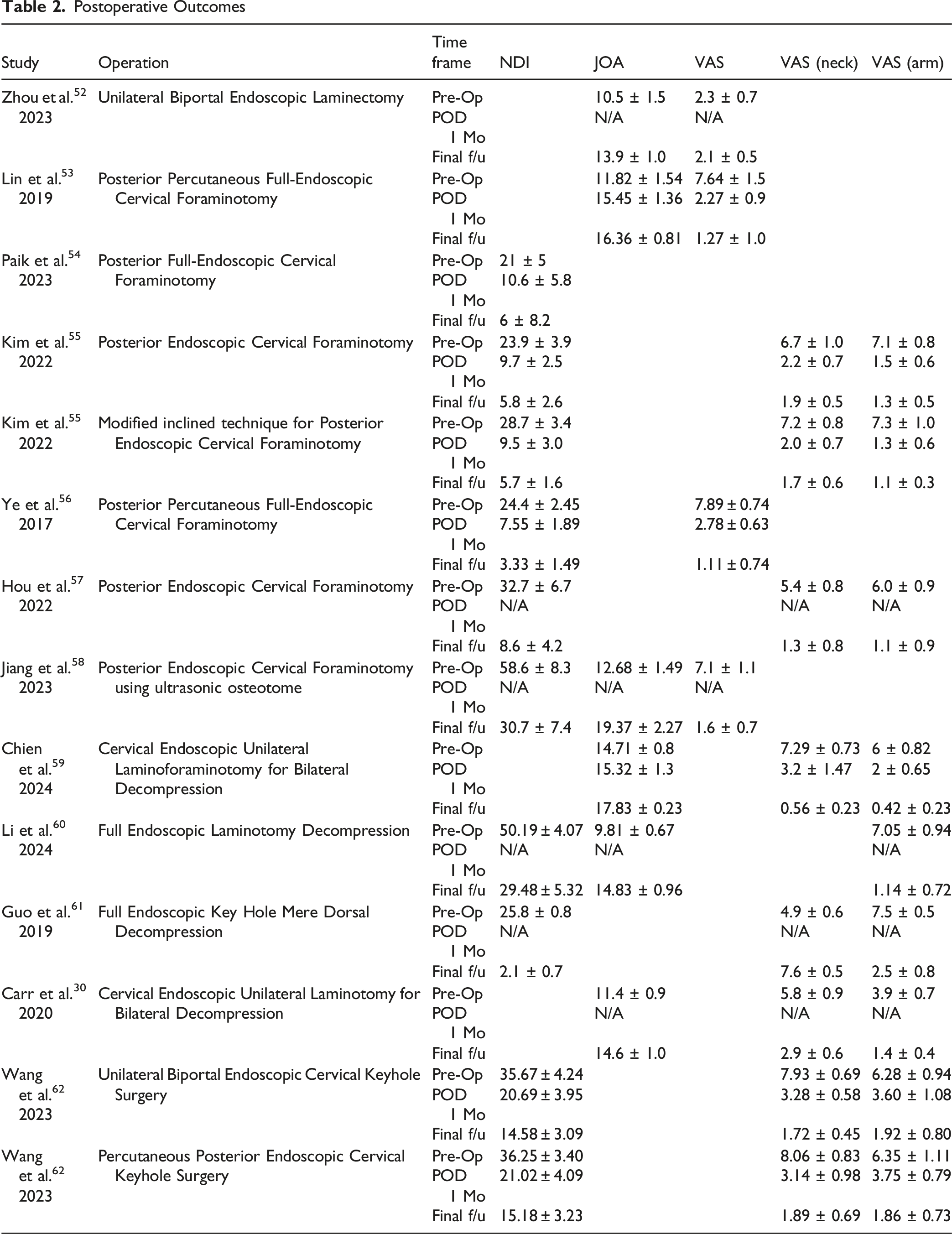
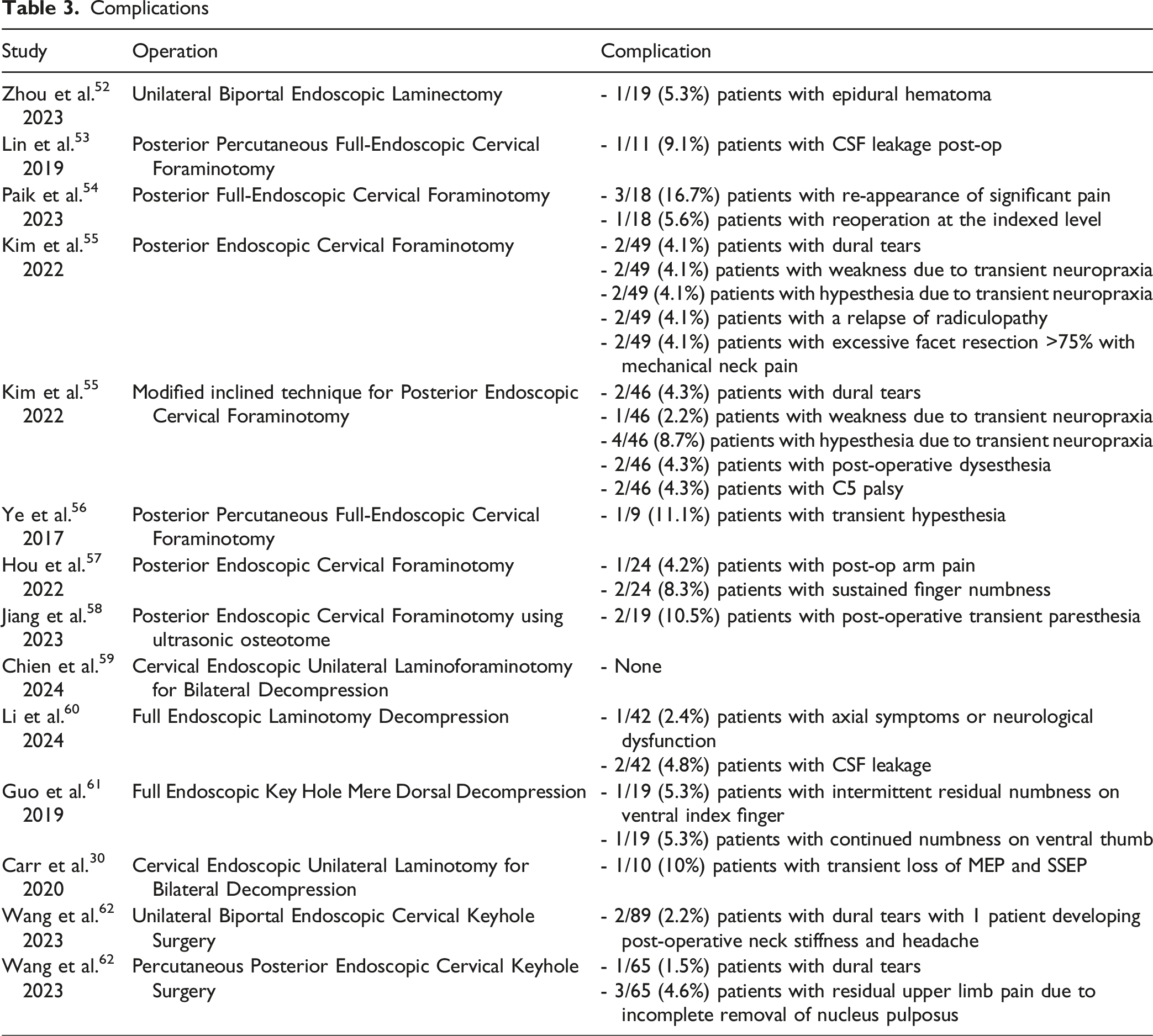
Using the screening criteria, 12 total studies were identified, and 14 endoscopic cervical surgical cohorts were reported since two studies described two different endoscopic operative techniques. A total of 226 articles were excluded during the screening because the surgical approach was not endoscopic, or cervical stenosis was not the primary condition being treated. All the studies reported improvement in clinical outcomes compared to preoperative assessment. The top complications noted are as follows: four of the fourteen studies reported a postoperative complication of dural tears, three of the fourteen studies reported transient hypesthesia, and two of the fourteen studies reported cerebrospinal fluid (CSF) leakage (Tables 1-3).
Discussion
The growing recognition of endoscopic cervical spine surgery on surgical outcomes highlights their role as promising alternatives to conventional open approaches for select cervical spine pathologies. Our findings demonstrated consistent postoperative improvement in pain and functional outcomes across all studies, affirming the therapeutic potential of ECSS in select patients. However, the analysis also revealed that complications varied by surgical technique, underscoring the need for a deeper understanding of their etiology and mitigation strategies.
The most frequent complications included dural tears, transient hypesthesia, and CSF leakage. Dural tears are often attributed to limited visualization or overaggressive bone resection, particular in severe cervical stenosis. 14 Careful anatomical planning with navigation technology and drilling or suturing in a water-based field can help prevent dural tears. Transient hypesthesia may be linked to neural irritation during decompression either through mechanical manipulation or thermal injury. Preventive strategies include gentle and precise decompression under continuous visualization and use of intraoperative neuromonitoring to detect early signs of nerve compromise. CSF leaks typically arise from unintended dural tears during decompression. It can be managed with primary closure of the dural defect with a dural substitute and sealant. As these complications are become better understood and techniques continue to evolve, it is essential to contextualize these outcomes within the broader development of cervical spine surgery.
With continued refinement, ECSS holds potential to expand its applicability. A growing body of evidence supports its benefits and advancements in instrumentation and visualization may further enhance its safety and efficacy. To guide future adoption and optimization of patient outcomes, it is essential to examine the clinical applications and limitations of current endoscopic techniques.
Current Endoscopic Cervical Techniques
Anterior Endoscopic Cervical Discectomy
The anterior endoscopic cervical discectomy (AECD) is the classical minimally invasive alternative to traditional anterior cervical discectomy and fusion (ACDF) and involves accessing the cervical disc space anteriorly with an endoscope.15-17 This technique is indicated clinically for pathologies such as cervical radiculopathy and myelopathy, symptomatic cervical disc herniation, and persistent symptoms despite 3 months of conservative management. 15 AECD offers many advantages including clearer operative visualization, shorter operative time, and accelerated rehabilitation with lower postoperative costs. 18 The surgical procedure initially places the patient in a supine position with their neck slightly extended. A small incision is made on the anterior aspect of the neck after confirmation of the level. A tubular retractor creates a working channel by dilating and maintain a corridor through the soft tissue. It is placed in the cervical disc space through a tract medial to the carotid sheath and lateral to the trachea and esophagus. Under endoscopic visualization, the surgeon drills down the uncinate joint and removes the herniated disc material with endoscopic forceps, decompressing the affected nerve root. Studies with AECD have reported minimal complications and improvement in postoperative neck pain and functional outcomes using the VAS and Nurick grading system, respectively.19,20
However, despite its benefits, several barriers hinder the widespread adoption of AECD. The steep learning curve, coupled with a lack of formal mentorship, has limited surgeon proficiency with inadequate training and fear of complications as primary obstacles. 21 Furthermore, concerns about limited indications in multilevel pathologies and anatomical constraints with small foraminal dimensions further restricts AECD’s application. 22 There is also concern for recurrence of disc herniation and progressive disc degeneration due to the disc-preserving nature of this procedure. The anterior approach itself introduces risks specifically to perforation and vascular damage given the proximity to the trachea, esophagus and carotid artery. These risks underscore the importance of careful patient selection and use of intraoperative navigation and neuromonitoring. Addressing these concerns through standardized training and meticulous techniques will be essential to establishing AECD as a safe and efficacious option.
Posterior Endoscopic Cervical Foraminotomy and Discectomy
The posterior endoscopic cervical foraminotomy and discectomy (PECFD) is another minimally invasive technique indicated for patients ideally presenting with cervical radiculopathy from lateralized disc herniation, osteophyte compression, and foraminal stenosis. 23
Compared with anterior approaches, the risk of injury to critical structures such as the trachea, esophagus, and carotid artery is significantly reduced with posterior approaches. 24 Moreover, PECFD utilizes smaller incisions and minimizes soft tissue disruption relative to open procedures, resulting in decreased postoperative pain and faster recovery. 25 In the procedure, the patient is placed in a prone position with the neck flexed and secured using a 3-point pin fixation or craniocervical traction system. The flexed neck widens the interlaminar window and reduces facet joint overlap. After identification with fluoroscopy, a small incision is made above the medial junction of the inferior and superior facet joint. Continuous irrigation with normal saline is maintained throughout the procedure. An obturator is then positioned at the V-point, which is the junction between the facet joint and superior and inferior lamina. A working channel and endoscope are inserted, and bone drilling occurs around the interlaminar space depending on the size and location of the herniated disc material. The ligamentum flavum is removed and ruptured fragments are discarded after an incision in the annulus. Decompression is performed and confirmed visually. 26 Studies with PECFD have reported significant clinical improvements in reducing pain scores and improving neck disability.25,27 In patients with cervical lordosis, PECFD also improved cervical curvature and neck extension. 28
Nevertheless, the implementation of PECFD is constrained by requiring specialized training, with only a few surgeons proficient in the procedure and inapplicability to certain patients, particularly those with advanced degenerative changes necessitating more extensive decompression. 29 In the context of foraminal stenosis, there is risk of excessive facet resection which can compromise segmental stability and accelerate degeneration at the index level. Imprecise bone removal can also contribute to neural injury and inadequate decompression. To mitigate these risks, detailed preoperative imaging to access facet preservation and careful drilling under continuous endoscopic visualization can help reduce the iatrogenic instability.
Cervical Endoscopic Unilateral Laminotomy for Bilateral Decompression
The cervical endoscopic unilateral laminotomy for bilateral decompression (CE-ULBD) is another emerging minimally invasive technique for treating cervical spinal stenosis and degenerative cervical myelopathy.
30
This technique involves placing the patient in a prone position with the head slightly flexed while avoiding excessive head inclination and shoulder traction. A small unilateral incision is made to introduce the endoscope and expose the lateral aspects of the lamina and posterior facet joint. The V-point, where the two laminae meet, serves as the main anatomical landmark. Decompression is performed by removing portions of the cranial and caudal lamina with a diamond burr and Kerrison punches. Ipsilateral and contralateral flavectomy fully decompresses the thecal sac and fluoroscopic imaging is utilized to verify the procedure. If foraminal stenosis is present, a foraminotomy is added to ensure adequate decompression while preserving the facet joint.
31
Studies with CE-ULBD have reported positive clinical outcomes with improvement in pain scores and neurological function and when compared with a standard ACDF, patients had significantly shorter hospital stays.30,32,33 Similar to other endoscopic procedures, however, CE-ULBD requires a higher learning curve and has relative limitations when addressing multi-level cervical pathologies.
34
Additionally, iatrogenic injury from misjudgment of decompression extent are possible complications can be addressed through intraoperative imaging and preservation of key anatomical landmarks such as the V-point and ligamentum flavum. Figure 2 presents the preoperative images, intraoperative endoscopic views, and postoperative images from a CE-ULBD. Supplemental Video 1 demonstrates the intraoperative technique of a CE-ULBD. Unilateral Endoscopic Cervical Laminotomy and Decompression. Preoperative (A) and Postoperative Magnetic Resonance Images (B). Operative View of the Lamina (C), Contralateral Lamina (D), Proximal Edge of Ligamentum Flavum (E), and Distal Edge of Ligamentum Flavum (F). All Images Were Provided by Dr Ji Soo Ha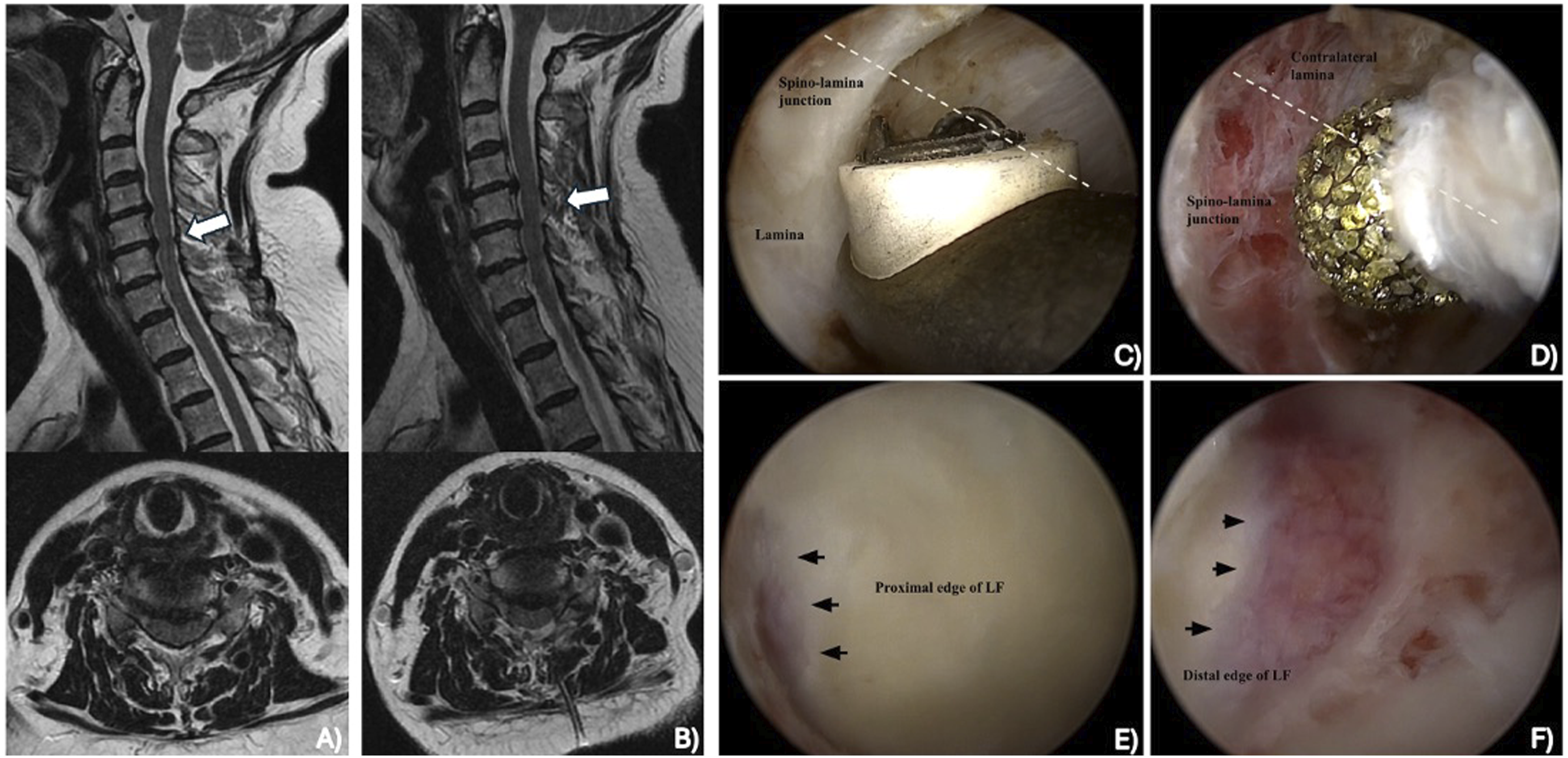
Unilateral Biportal Endoscopy
The unilateral biportal endoscopy (UBE) for the cervical spine is a minimally invasive alternative to traditional open cervical surgeries, allowing access to the cervical spine through two small portal sites with an endoscope and working channel. UBE has demonstrated effectiveness in treating cervical disc herniation, cervical stenosis, cervical spondylotic radiculopathy, and degenerative cervical myelopathy using a variety of procedures including cervical foraminotomy, cervical diskectomy, and cervical laminectomy.35-38 Like other endoscopic techniques, UBE provides continuous endoscopic saline irrigation, which enables high-definition monitoring of a transparent surgical field.
38
When compared with traditional posterior endoscopic foraminotomy (PEF), one study reported a shorter operating time with UBE-PEF (71.97 ± 10.87 min vs 80.12 ± 15.19 min), while still improving clinical outcomes compared to preoperative assessment.
39
The disadvantage of UBE surgery, unfortunately, is its relative difficulty and long learning curve for surgeons to gain proficiency.
40
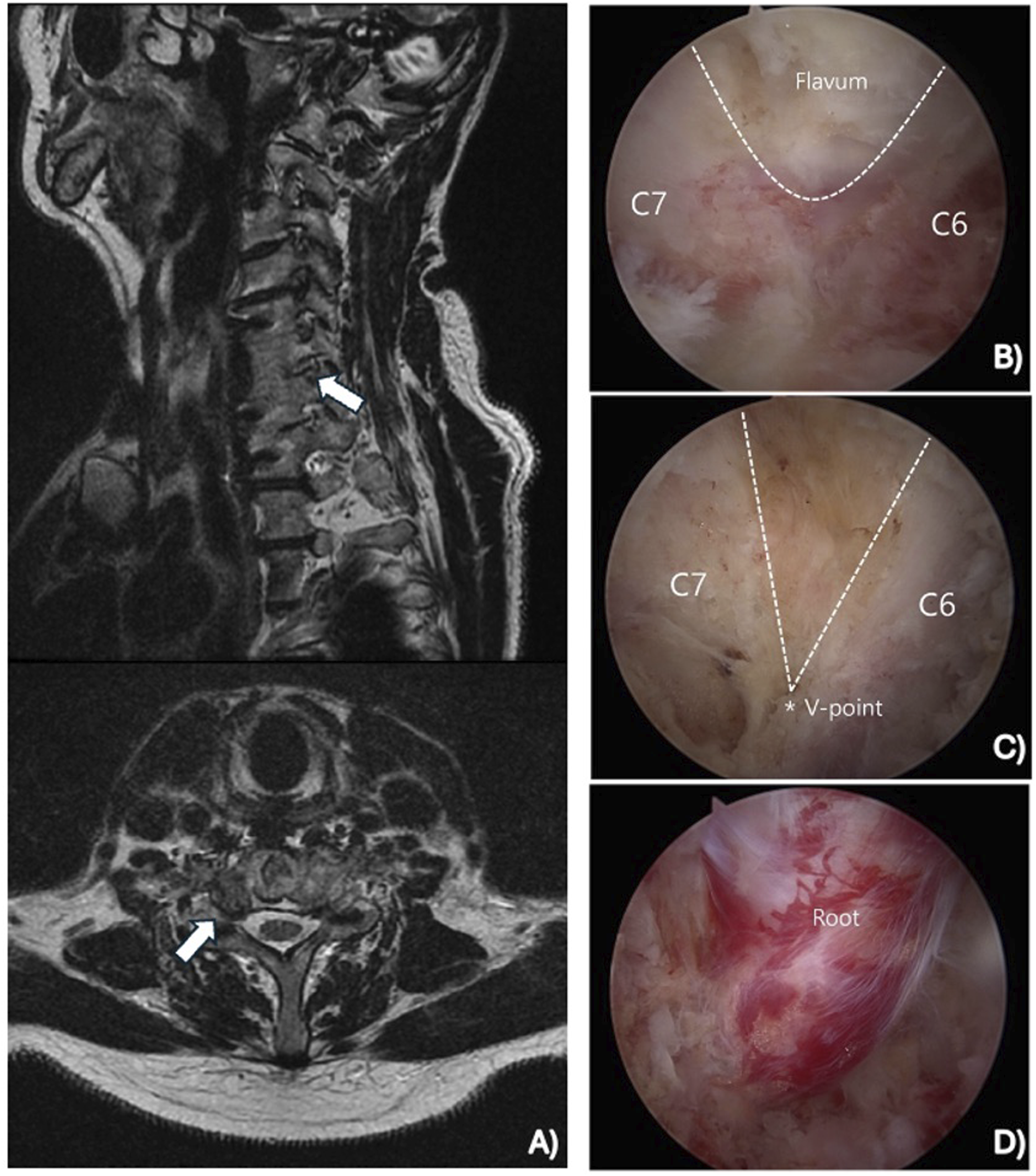
Figure 3 illustrates the preoperative images, intraoperative endoscopic views, and postoperative outcomes from a UBE cervical discectomy. Supplemental Video 2 highlights the intraoperative technique of a UBE cervical discectomy. Figure 4 illustrates the preoperative imaging and intraoperative endoscopic views from a UBE cervical foraminotomy and decompression. Supplemental Video 3 highlights the intraoperative technique of a UBE cervical foraminotomy and decompression. Unilateral Biportal Endoscopic Cervical Discectomy. Preoperative (A) and Postoperative Magnetic Resonance Images (B). Operative View Before the Discectomy, (C) During the Discectomy (D), and After the Discectomy (E). All Images Were Provided by Dr Ji Soo Ha Unilateral Biportal Endoscopic Cervical Foraminotomy and Decompression. Preoperative Magnetic Resonance Images (A). Operative View of the Flavum (B) and V-Point (C) During the Foraminotomy at the C6-C7 Level. Operative View of the Nerve Root After Decompression (D). All Images Were Provided by Dr Ji Soo Ha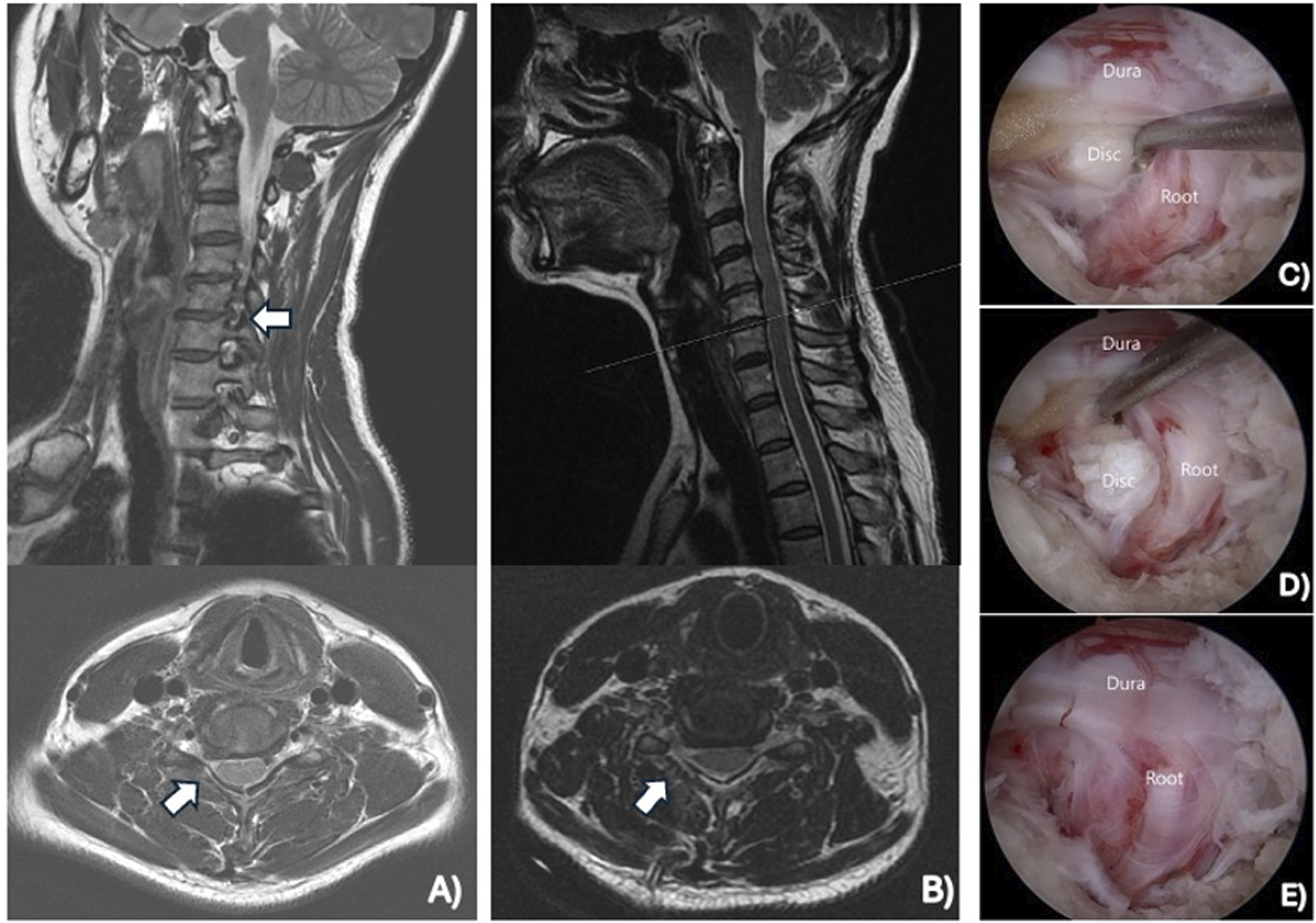
Although ECSS has demonstrated clinical efficacy, its widespread adoption is limited by challenges such as steep learning curves and reliance on tactile feedback in an anatomically constrained corridor. These limitations contribute to variability in outcomes and complications across different techniques. Emerging technologies directly address these barriers by enhancing preoperative planning, improving intraoperative visualization, and enabling more precise decompression. Integrating these innovations into ECSS has the potential to not only reduce complications, but also broaden its indications and improve reproducibility.
Future of Endoscopic Cervical Spine Surgery
As medical technology progresses, numerous recent innovations have significantly impacted the field of ECSS, with ongoing developments promising even greater advancements in the future. These advancements span various areas, including endoscopic, imaging, and navigational technologies, surgical tools, minimally invasive approaches, and specific innovative procedures. Moreover, the incorporation of artificial intelligence and machine learning into surgical planning and execution may further revolutionize the field, leading to more personalized and effective care for patients suffering from cervical spine conditions. The future of ECSS lies in the refinement of these innovations, potentially expanding their applications and improving patient outcomes.
Endoscopic, Imaging, and Navigational Technologies
Higher resolution camera lens technology can now clearly reveal previously hidden microstructures under magnification, refining dissection techniques and enhancing bleeding control. For instance, Kwon et al illustrated how a 4K ultra-high resolution endoscope enabled the straightforward visualization of structures like the foraminal ligaments, which are typically challenging to observe. 41 Three-dimensional (3D) endoscopic instruments offer detailed visualization of surgical anatomy, including clearer views of the dura and nerve roots. 42 Color representation in surgical imaging enables surgeons to distinguish between different important structures and adjust procedures as needed. The quality of color representation is dependent on the camera sensor integrated within the camera head. Complementary Metal-Oxide-Semiconductor (CMOS) sensors have gained widespread popularity among manufacturers for their cost effectiveness and higher resolution in comparison to Charge-Coupled Device (CCD) sensors, the previous gold standard. 43 Camera sensors can also be differentiated by whether they use a one-chip or three-chip system. While a three-chip system, which uses separate sensors for red, blue, and green, provides superior imaging capabilities, it is less cost-effective compared to a one-chip system that captures all three primary colors with a single sensor. 43 In their study, Kaliya-Perumal et al utilized image data merging (IDM) within a spinal navigation system to create a coherent image of screw heads during L1-L5 minimally invasive long-construct posterior instrumentation. This method addresses the challenge of visualizing screw heads, allowing precise placement of screws and rods. 44 This advanced imaging approach could similarly be applied to ECSS by improving intraoperative navigation and facilitate precise decompression with reduced risk of neurovascular injury. Similarly, a retrospective study by Hanna et al of over 19 years highlighted the advantages of integrating intraoperative CT scanning and image-guided surgery for thoracoscopic procedures. Their findings demonstrated benefits such as direct decompression without neural manipulation, enhanced 3D spatial orientation, and improved localization of complex spinal anatomy. 45 These innovations hold significant potential for advancing ECSS by enhancing precision, reducing intraoperative risks, and improving surgical outcomes.
Surgical Tools
Robot-assisted spine surgery and navigation systems both offer features that aid surgeons during procedures. However, robot-assisted surgery provides more precise physical guidance for executing preoperatively planned surgeries. This technology enhances a surgeon’s control and mobility through narrow portals while minimizing physiological tremors. 46 A study by Hyun et al 47 compared the impact of robotic guidance in minimally invasive spine surgery (MIS) to a fluoroscopy-guided open approach in lumbar fusions, revealing that the robotic-guidance group experienced less radiation and shorter hospital length of stay without compromising patient outcomes. 47 However, the study was constrained by a limited sample size, and the reported length of stay may have been impacted by the healthcare system in the author’s country. Similarly, Lonjon et al 48 evaluated the accuracy of pedicle screw placement using the ROSA robotic assistance system (Medtech S.A., Montpellier, France), finding that the robotic-guidance group achieved a 97.3% accuracy rate compared to 92% in the freehand conventional technique group. 48 In endoscopic spinal surgeries, drills need specific features that differ from those used in other endoscopic procedures. Conducted in a water-based environment, these surgeries require drills that can efficiently expel bone dust to maintain a clear field of view. This is often achieved with drills that have a separate suction for water out-flow and thin shafts for high stability at high speeds. Additionally, waterproofing, particularly in the handpiece, is crucial for durability and preventing potential tool malfunctions. Advancements in these areas are expected to lead to more effective and selective tissue removal tools, improving the overall efficiency of ECSS. 43
Artificial Intelligence and Machine Learning
In the future, the field of ECSS anticipates the integration of novel technologies such as artificial intelligence (AI) and machine learning. These technologies are expected to enhance preoperative planning, improve surgical execution, and optimize patient selection, ultimately leading to better postoperative outcomes and increased patient satisfaction. 49 Zhu et al developed an AI-based MRI segmentation technique to construct a 3D model of lumbosacral structures, to help identify an appropriate approach for percutaneous endoscopic lumbar discectomy (PELD). This model offers detailed 3D anatomical information for preoperative evaluation and surgical planning, achieving high dice scores of 0.921 for L5 vertebrae bone, 0.924 for S1 vertebrae bone, 0.885 for discs, 0.808 for lumbosacral nerves, 0.886 for iliac bone, and 0.816 for skin. The high accuracy of this model suggests its potential application in endoscopic cervical spine surgery (ECSS) procedures. 50 Goedmakers et al developed a deep learning algorithm to predict Adjacent Segment Disease (ASD) using only preoperative cervical MRI scans in patients undergoing single-level ACDF. ASD poses a risk for patients having surgery for cervical radiculopathy and identifying those who will develop ASD remains a challenge for clinicians. The model demonstrated high performance on 93 test images, achieving an accuracy of 88 out of 93 (95%; 95% CI: 90, 99), sensitivity of 12 out of 15 (80%; 95% CI: 60, 100), and specificity of 76 out of 78 (97%; 95% CI: 94, 100). In comparison, predictions made by a neuroradiologist and a neurosurgeon were less accurate, sensitive, and specific than those of the algorithm. 51 These studies underscore the potential of AI and machine learning to enhance the precision and efficiency of ECSS.
Limitations
Despite the increase in literature on endoscopic cervical spine surgery, several limitations must be acknowledged. Research analyzing patient outcomes and complications remains scarce, with most studies being retrospective in nature and there being an absence of high-quality randomized control trials. Furthermore, significant heterogeneity in surgical technique, follow-up durations, and outcome measures complicate direct comparison and synthesis of findings. The lack of standardized reporting limits the feasibility of a meta-analysis, as data from studies with different methodologies may introduce potential bias and diminish the reliability of the conclusion. To establish ECSS as a comparable standard to open techniques, further research prioritizing randomized control trials with standardized methodologies is required to generate higher-level evidence supporting its usage.
Conclusion
Endoscopic cervical spine surgery is emerging as an alternative approach in the treatment of various cervical spine pathologies. This approach offers a number of potential advantages over traditional open procedures such as, reduced soft tissue damage, quicker recovery, and improved clinical outcomes. The refinement of techniques such as anterior endoscopic cervical discectomy, posterior cervical foraminotomy, and unilateral laminotomy for bilateral decompression has supported ECSS as a minimally invasive alternative for many patients. With technological innovations such as advanced imaging systems, robotic-assisted tools, and the integration of artificial intelligence, the future of ECSS is set for substantial advancements. These innovations will potentially enhance surgical precision, optimize patient selection, and improve postoperative outcomes, making ECSS a key player in evolving the landscape of cervical spine surgery. As research and development in this field continues, ECSS will likely expand its indications and capabilities, potentially leading to better patient care and long-term health benefits.
Supplemental Material
Supplemental Material - Clinical Outcomes and Future Directions of Endoscopic Cervical Spine Surgery: A Systematic Review With Narrative Insights
Supplemental Material for Clinical Outcomes and Future Directions of Endoscopic Cervical Spine Surgery: A Systematic Review With Narrative Insights by Ryan Wang, Satheeshram Tamilselvan, Ji Soo Ha, Aditya Vedantam, C. Rory Goodwin, Nathan Evaniew, Uzondu F. Agochukwu, Konstantinos Margetis, Yoon Ha, Michael Fehlings, Jefferson R. Wilson, and Ankit I. Mehta in Global Spine Journal.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This supplement was organized and financially supported by AO Spine through the AO Spine Knowledge Forum Spinal Cord Injury, a focused group of international spine experts, and AO Spine North America. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization based in Davos, Switzerland.
Supplemental Material
Supplemental material for this article is available online.