
Abstract
We present a case of a dural tear associated with nerve root herniation following unilateral biportal endoscopic decompression (UBED) that was successfully treated using a computed tomography-guided epidural blood patch. A 60-year-old man underwent UBED for radicular pain because of spinal stenosis at L4–5. A left partial hemilaminectomy and flavectomy were performed; however, the left dorsolateral side dura mater was torn during the procedure. TachoComb® was applied at the dural tear site, and the pain was relieved following UBED. However, 3 weeks post-UBED, the patient reported severe pain with an electric shock-like sensation in the left buttock and posterior thigh region with no other neurologic symptoms. The pain was aggravated by standing and spinal motion. Follow-up lumbar spinal magnetic resonance imaging was performed. Axial images indicated protrusion of the left S2 nerve root through the left dorsolateral side of the dura mater. The patient was further diagnosed with nerve root herniation following a dura mater tear. A computed tomography-guided epidural blood patch was performed, with successful therapeutic results. The outcome of this study indicates that a small dural tear that occurs during minimally invasive spinal surgery can be efficiently treated using an epidural blood patch prior to open surgery.
Keywords
Introduction
Minimally invasive spinal surgery has been an effective treatment strategy for patients diagnosed with a variety of lumbar spinal diseases for over 20 years.1–3 These surgeries have rapidly evolved from mini-open to tubular or percutaneous endoscopic techniques,1–3 with numerous advantages such as smaller wounds, reduced blood loss, less postoperative wound pain, and a shorter hospital stay. 2 Additionally, minimally invasive spinal surgery avoids the possibility of injuring paraspinal muscles and posterior stabilizing structures (interspinous ligaments, facet joint, and capsule), which in turn helps maintain spinal stability. 2 Unilateral biportal endoscopic decompression (UBED) is a percutaneous, full-endoscopic surgical technique used in the treatment of spinal stenosis. 4 This procedure is performed by the introduction of two small surgical incisions on either side of the spinous process. 4 UBED does not rely on a working tube or channel. Surgeons can perform decompression accurately and in a magnified operative field using continuous high-pressure normal saline irrigation and high-definition endoscopy.
Dural tears are the most common complication associated with the UBED procedure, with an incidence rate of 5%.5,6 Open spinal surgery using an endoscopic technique such as UBED is often required for the treatment of dural tears. 6 Previous studies have shown that an epidural blood patch is an effective treatment method for managing post-dural puncture headaches. 7 Furthermore, we hypothesized that an epidural blood patch could also be used to effectively control dural tears.
In this study, we report a case of successful treatment of a dural tear with nerve root herniation following UBED with an epidural blood patch. This report will provide knowledge for pain physicians regarding the treatment of dural tears. The case reported in the study is in accordance with the CARE guidelines. 8
Case presentation
A 60-year-old man presented with left lateral thigh and calf pain because of spinal stenosis at L4–5 and underwent bilateral biportal endoscopic decompression at the department of neurosurgery in a local spine hospital. The patient’s left L5 nerve root was impinged between the herniated lumbar disc and juxtafacet cyst at the level of the L4–5 disc (Figure 1a). A left partial hemilaminectomy and flavectomy were also performed. However, a tear in the dura mater occurred on the left dorsolateral side during the procedure. The neurosurgeon applied TachoComb® (CSL Behring GmbH, Marburg, Germany) at the dural tear site. Following bilateral biportal endoscopic decompression, the patient had mostly recovered from the left lateral thigh and calf pain. The patient was discharged based on the schedule.

(a) Axial T2-weighted lumbar spine magnetic resonance imaging (MRI) before unilateral biportal endoscopic decompression revealed spinal stenosis at L4–5. The left L5 nerve root was impinged between the herniated lumbar disc and juxtafacet cyst. (b) Axial T2-weighted lumbar spine MRI performed 3 weeks after unilateral biportal endoscopic decompression showed that the left S2 nerve root was protruding through the left dorsolateral side dura matter (red arrow) and (c) Axial T2-weighted lumbar spine MRI performed 2 days after the epidural blood patch procedure showed no protrusion of the left S2 nerve root through the dura mater.
It should be noted that 3 weeks after endoscopic decompression, the patient reported severe pain (numeric rating scale: 7, 0: no pain, 10: the worst pain imaginable) with an electric shock-like sensation in the left buttock and posterior thigh. The pain was aggravated in a standing position or by spinal motion and was relieved in the supine or prone position. A physical examination revealed no sensory abnormalities or motor weakness. Follow-up lumbar spinal magnetic resonance imaging (MRI) was performed. Axial MRI demonstrated protrusion of the left S2 nerve root through the left dorsolateral side of the dura mater (Figure 1b). The MRI findings and clinical symptoms indicated that the patient’s pain was caused by left S2 root herniation as a result of a torn dura mater.
A computed tomography (CT)-guided epidural blood patch was performed, during which the patient was placed on a CT table. Using intermittent CT fluoroscopy for guidance, a 22-gauge Tuohy needle was introduced into the soft tissues of the lower back at the L4–5 disc level following skin anesthesia with 1% lidocaine. The needle was progressively advanced until the tip was placed into the left dorsolateral epidural space via an interlaminar approach (Figure 2a). Aspiration was performed to detect the presence of any cerebrospinal fluid leakage, and approximately 2.5 mL of cerebrospinal fluid was aspirated (Figure 2b). Subsequently, 5 mL of the patient’s blood was extracted under sterile conditions from an arm vein and slowly injected into the dorsal epidural space (Figure 2c).
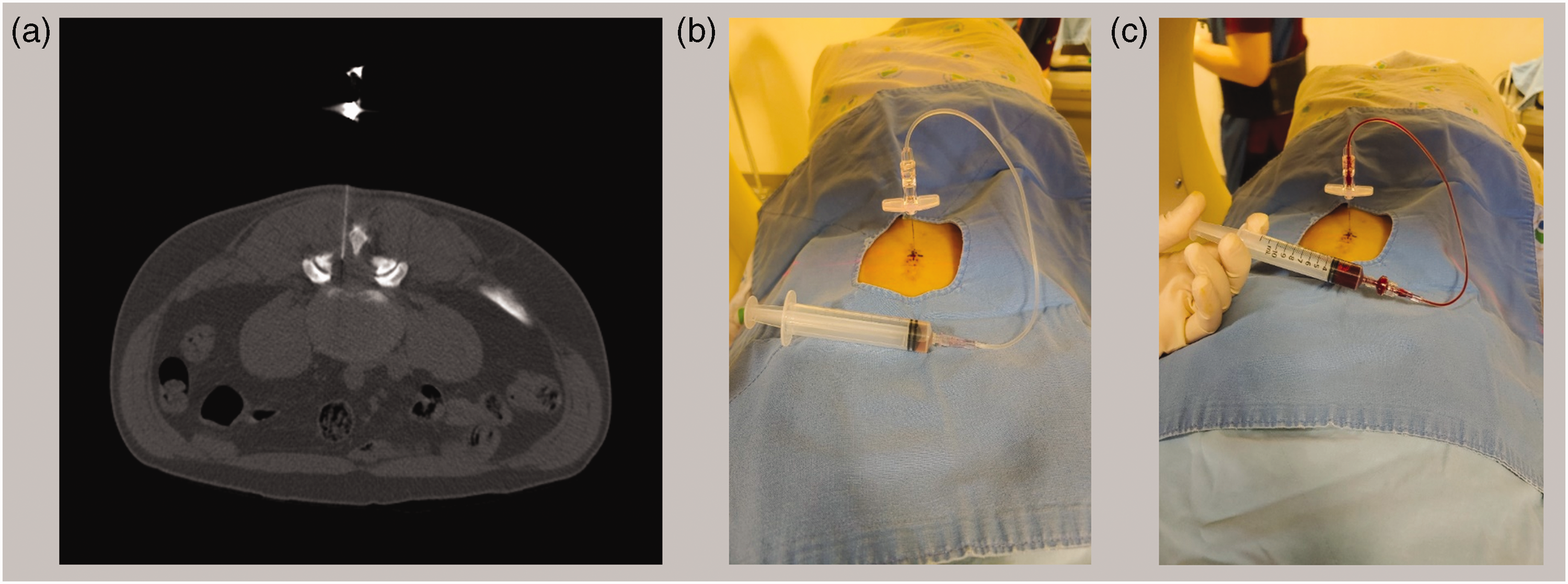
(a) Administration of a computed tomography-guided epidural blood patch was performed with a 22-gauge Tuohy needle; (b) cerebrospinal fluid was aspirated and (c) the patient’s blood was extracted from an arm vein and slowly injected into the dorsal epidural space.
Two days after the epidural blood patch procedure, the patient reported a 50% reduction in left buttock and posterior thigh pain. In a follow-up lumbar spinal MRI procedure performed 2 days after the epidural blood patch procedure, there was no indication of protrusion of the left S2 nerve root through the dura mater (Figure 1c). One month after the epidural blood patch procedure, the patient’s pain gradually subsided. At the 1-month follow-up after the epidural blood patch, the patient’s left buttock and posterior thigh pain had nearly disappeared.
Discussion
In the current study, we report the successful treatment of a dural tear combined with nerve root herniation caused by UBED with a CT-guided epidural blood patch.
Although dural tear is a frequently occurring complication in minimally invasive spinal surgery, it is rarely associated with nerve root herniation. To date, only a few cases of dural tear have been previously reported to be associated with nerve root herniation.9–11 In all of these cases of dural tears associated with nerve root herniation following minimally invasive spinal surgery, the torn dura was repaired with open surgery.9–11 To the best of our knowledge, our study is the first to report successful treatment of a dural tear by minimally invasive spinal surgery using an epidural blood patch. Entrapment of the nerve root at the dural defect site is associated with a neurologic deficit accompanied by pain that is non-responsive to any conservative treatment. 9 However, the patient in the current study did not exhibit any neurological symptoms. In addition, the pain was relieved in the supine or prone position. The clinical features of the patient along with the MRI findings indicated a small dural tear and that the nerve root entrapment could potentially be reversed. Therefore, we hypothesized that a blood patch could seal the tear in the dura mater. A CT-guided approach was chosen instead of fluoroscopy to accurately inject a blood patch into the dural tear site and prevent it from entering the intra-thecal space.
A high success rate and low likelihood of complications have established the epidural blood patch as the standard to treat dural puncture. 12 However, in the case of a dural tear, an epidural blood patch might induce the formation of adhesion tissue around the herniated nerve root. Moreover, there is also a possibility of worsening of the symptoms because of deformation and displacement of the thecal sac by a blood patch. Case reports and clinical trials demonstrating positive therapeutic effects are required to verify the effectiveness and safety of the epidural blood patch.
The outcomes of this study demonstrated the effectiveness of a conservative treatment technique involving the use of an epidural blood patch in the treatment of radicular pain in a patient because of a dural tear with nerve root herniation. Therefore, an epidural blood patch could potentially be an effective conservative treatment option for small dural tears that occur during minimally invasive spinal surgery and have no associated neurological deficit.
Footnotes
Author contributions
YMC, SHL, KSM, and MCC contributed to the study conception and design and wrote the manuscript. MCC supervised the study. All authors have read and approved the manuscript. The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Data availability statement
The datasets generated during the current study are available from the corresponding authors upon reasonable request.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Ethics and patient consent statement
Written consent for treatment was obtained from the patient. Written informed consent was also obtained from the patient for the publication of this study and the relevant images. This study was approved by the Institutional Review Board of Yeungnam University Hospital.
Funding
The authors disclose receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Research Foundation of Korea Grant funded by the Korean government (Grant No. NRF-2019M3E5D1A02069399).