
Abstract
Study Design:
Longitudinal cohort.
Objectives:
Posterior spinal fusion (PSF) using all-pedicle screw constructs has become the standard procedure in the treatment of adolescent idiopathic scoliosis (AIS). However, there have been several reports that all-pedicle screw constructs or the use of pedicle screws at the upper instrumented vertebrae (UIV) increases the incidence of proximal junctional kyphosis (PJK). We aimed to evaluate the impact of instrumentation type on the incidence of PJK following PSF for AIS.
Methods:
We performed a stratified random sampling from 3654 patients enrolled in a multicenter database of surgically treated AIS to obtain a representative sample from all Lenke types. Patients were then allocated into 3 groups based on the instrumentation type: all-pedicle screw (PS), hook at UIV with pedicle screws distally (HT), and hybrid constructs (HB). We measured proximal junctional angle (PJA) and defined PJK as PJA ≥ 10° and PJA progression of >10° at the final follow-up.
Results:
Fifteen (4.3%) of 345 cases had PJK. PJK was significantly more common in PS (11%) compared with HB (1%) and HT (0%) (P < .001). PJK patients were similar to non-PJK patients regarding age, sex, curve type, UIV, and preoperative coronal Cobb angle. Thoracic kyphosis was significantly higher in the PJK group before surgery. Patients who developed PJK had a statistically significantly larger negative sagittal balance compared with the non-PJK group.
Conclusion:
The incidence of PJK was 4.3% and was more common in all-pedicle screw constructs. Using hooks at UIV might be a treatment strategy to limit PJK.
Keywords
Introduction
Posterior spinal fusion (PSF) with all pedicle screw constructs has become the standard surgical treatment for adolescent idiopathic scoliosis (AIS). Pedicle screws have a mechanical advantage over hooks that allow for increased deformity correction, 1,2 by enabling surgeons to control the spine in 3 dimensions.
Proximal junctional kyphosis (PJK) is a common complication after PSF with a reported incidence of 7% to 46%. 3,4 Some studies have shown that the incidence of PJK was equivalent regardless of instrumentation type. 5 -7 Other studies have shown that hook or hybrid constructs are superior to all-pedicle screw constructs in terms of PJK. 8 -10 Wang et al 10 reported that the use of hooks at upper instrumented vertebrae (UIV) had a significantly lower PJK incidence than the use of pedicle screws at the UIV; however, the instrumentation type in the distal vertebrae was not associated with PJK. 10 Other studies showed that all-pedicle screw constructs had higher PJK incidence than all-hook or hybrid constructs. 8,9 Although there have been a number of articles on the topic, no consensus has yet been reached. This may be because there have been few large studies. 6,8,9 In addition, no studies have compared between all-pedicle screw, hybrid, and UIV-hook distal pedicle screw constructs with sufficient sample size. To obtain strong evidence, an analysis with clear-cut grouping using large sample size is necessary. The purpose of this study is to investigate the impact of the three instrumentation types on the incidence of PJK following PSF for AIS.
Methods
Subjects
The data on AIS patients enrolled in the Prospective Pediatric Scoliosis Study (PPSS) database from March 2003 to December 2009 was used for this study. The PPSS is a multicenter database of surgically treated AIS managed by the Spinal Deformity Study Group. A stratified random sampling was done as previously described 11 to obtain a representative sample from all Lenke types (1-6), subtypes (A, B, and C) and thoracic curve modifiers (N, −, and +). In brief, random numbers were assigned to each subject. Then, the first 10 subjects from each of the 42 Lenke curve subtypes were selected and their 36-inch films were evaluated. This was done through 3 iterations. Since there is an unequal distribution of cases among the 42 Lenke subtypes, no type 4, 5, or 6 subjects were left to randomize in some iterations. After the stratified sampling, patients were included if they underwent PSF, and if immediate postoperative and final follow-up posteroanterior and lateral whole-spine upright radiographs were available. Minimum 1-year follow-up was required. Patients who had revision surgery were excluded. Patients with all-hook constructs were also excluded from the analysis because there were only 12 patients. Institutional review board approval was received prior to enrollment of the subjects into the database. Institutional review board approval was also received prior to initiation of this secondary analysis.
Patients were then divided into 3 groups based on the instrumentation type: all-pedicle screw constructs (PS), hook at UIV with distal all-pedicle screw constructs (HT), and hybrid constructs (HB). The HT group included bilateral hooks, or one hook and one pedicle screw at UIV, and screws at the rest levels. Patients with other constructs including hooks and screws were included in the HB group.
Radiographic Measurement
Radiographic measures including Cobb angle, thoracic kyphosis (T5-12), and Lenke curve type were extracted from PPSS database. Proximal junctional angle (PJA) was measured using the Surgimap software by an independent reviewer who was not involved in the surgical treatment. PJA was defined as the caudal endplate of the UIV to the cephalad endplate of the UIV+2 vertebrae. 9 PJK was evaluated using lateral whole-spine upright radiographs immediate after surgery and at the final follow-up based on following criteria as previously described 12 : PJA ≥ 10° and PJA progression of ≥10° at the final follow-up. Spinal levels were assigned a number increasing caudally with C0 being 1 and T1 being 8.
Statistical Analysis
Categorical variables were analyzed using the Fisher exact probability test. Analysis of variance (ANOVA) was used to assess the difference of continuous measures across the groups. Multiple logistic regression model yielding odds ratios (ORs) and 95% confidence intervals (CIs) was used to identify significant predictors of PJK. Variables with a P value of <.05 in univariate analyses were entered into the multiple logistic regression model. All statistical analyses were performed using SPSS Statistics 25 (IBM Corp). A statistical significance was defined as P value <.05.
Results
Patient Demographics
We performed a stratified random sampling from 3654 patients to pick up a representative sample from all Lenke types (1-6), subtypes (A, B, and C) and thoracic curve modifiers (N, −, and +). After a random sampling, 345 patients were included. Patient demographics are shown in Table 1. The PS, HT, and HB groups included 128 111, and 106 patients, respectively. There was no significant difference in age, sex, thoracic kyphosis, sagittal balance, and curve type among the groups. Preoperative Cobb angle of the main curve was slightly higher in the HB group than in the PS group. UIV was slightly caudal in the PS group than in the HB group. Although statistically significantly different, this may not be clinically relevant.
Background Characteristics in Each Group.
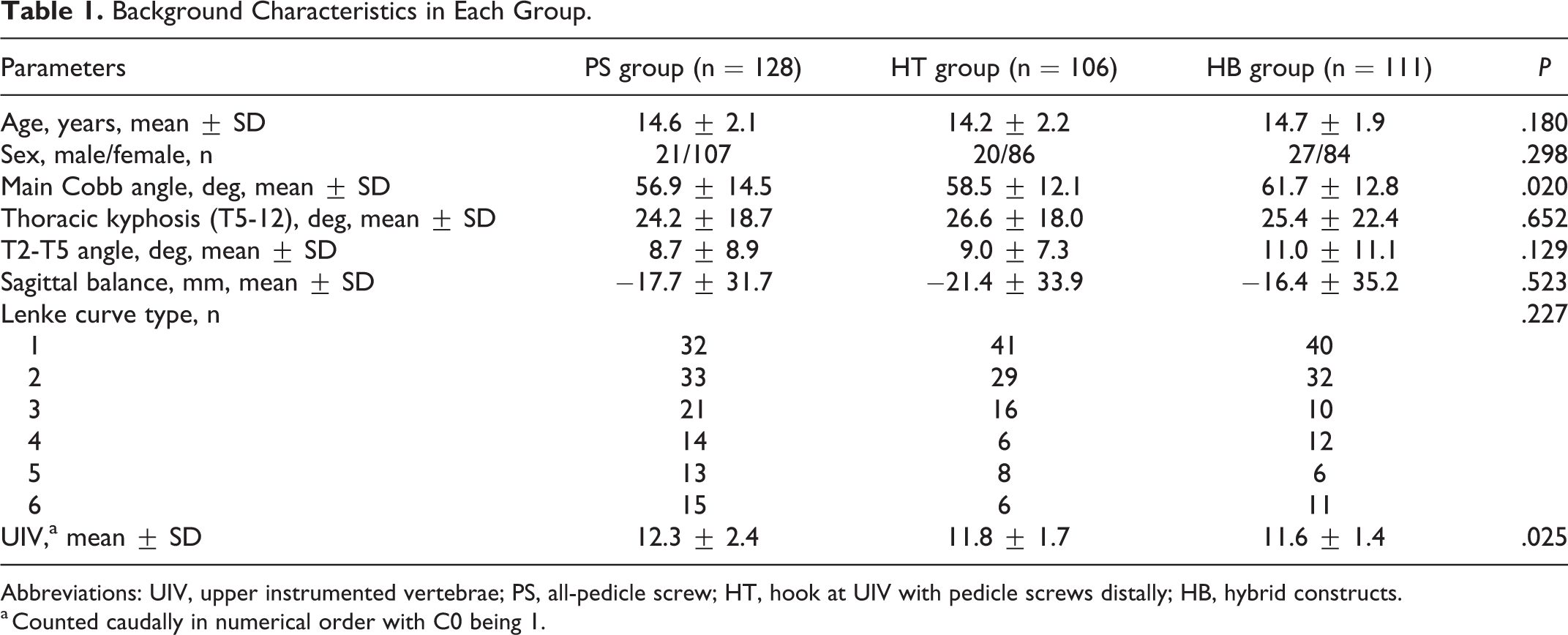
Abbreviations: UIV, upper instrumented vertebrae; PS, all-pedicle screw; HT, hook at UIV with pedicle screws distally; HB, hybrid constructs.
a Counted caudally in numerical order with C0 being 1.
Incidence of PJK and Postoperative Radiographic Parameters in Each Group
Fifteen patients (4.3%) were diagnosed as PJK at the latest follow-up (average 2.2 years). Fourteen out of 15 were in the PS group (11%) and the other was in the HB group (1%). There was no PJK in the HT group. The incidence of PJK was significantly higher in the PS group than other groups (Table 2). No revision surgery was required during the follow-up period.
Comparison of Clinical and Radiographical Data Between PJK and Non-PJK Groups.
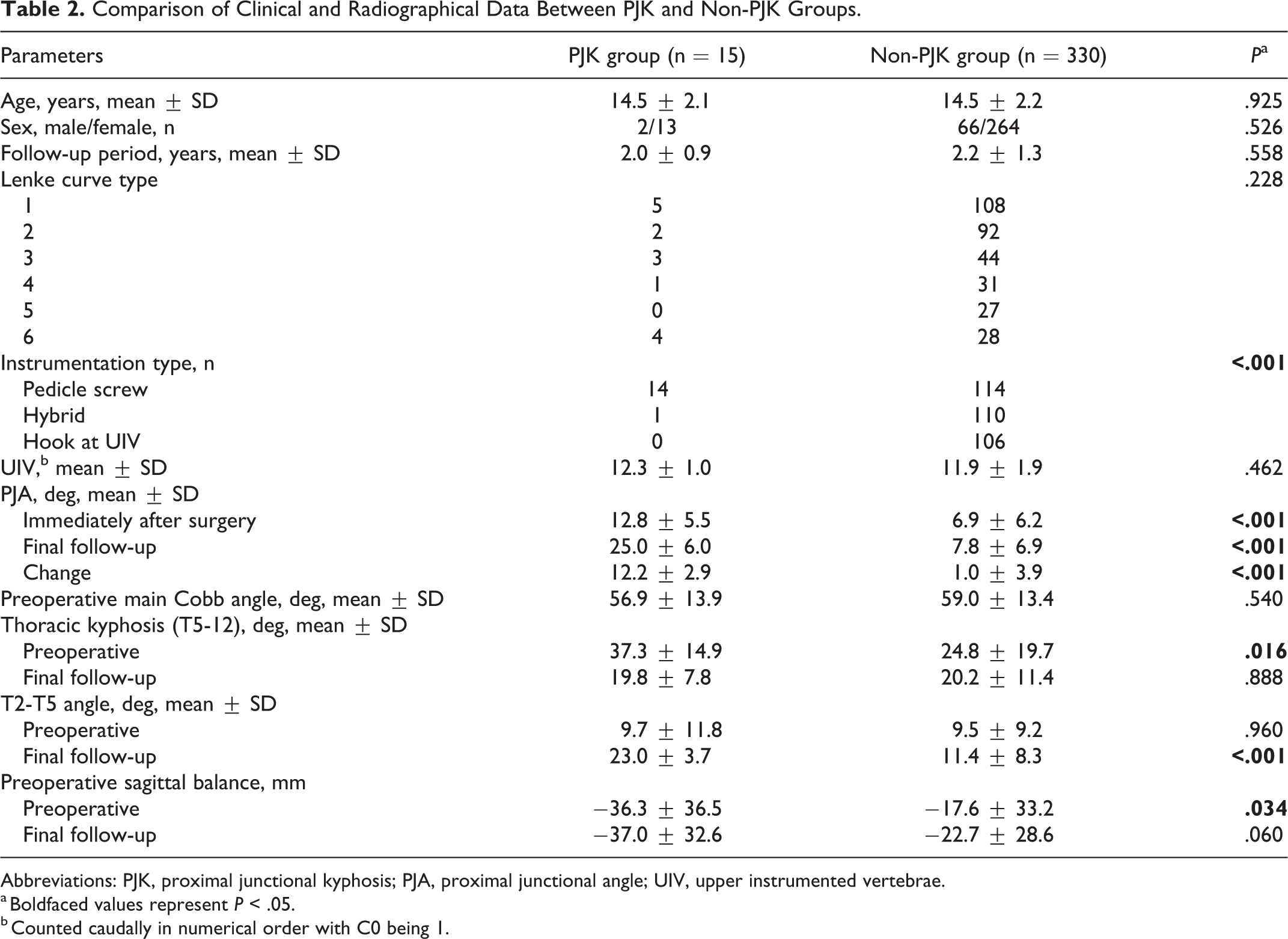
Abbreviations: PJK, proximal junctional kyphosis; PJA, proximal junctional angle; UIV, upper instrumented vertebrae.
a Boldfaced values represent P < .05.
b Counted caudally in numerical order with C0 being 1.
Comparison of Background Data and Radiographic Parameters in PJK and Non-PJK Patients
Then, we compared clinical and radiographic data between the PJK and non-PJK groups (Table 2). Fifteen PJK patients were not significantly different from non-PJK patients regarding age, sex, curve type, UIV, and preoperative main Cobb angle.
PJA at final follow-up was higher in the PJK group. PJA immediate after surgery was also significantly larger in the PJK group (12.8°) than the non-PJK group (6.9°).
Preoperative T2-5 angle was not different between patients with and without PJK. Postoperative T2-5 was significantly greater in PJK group. Thoracic kyphosis was significantly larger in the PJK group preoperatively although they were equivalent at final follow-up; thoracic kyphosis was significantly decreased in the PJK group after surgery.
The PJK group had significantly larger negative sagittal balance compared to the non-PJK group preoperatively. The trend was maintained at final follow-up although there was no statistical difference.
Multivariate Logistic Regression Analysis of the Variables for PJK
Considering the results of univariate analyses, instrumentation type, preoperative thoracic kyphosis and sagittal balance were considered as dependent variables (Table 3). An all-pedicle screw construct was a significant risk factor for PJK. Hybrid and hook at UIV constructs had ORs of 0.06 and 0, respectively. Preoperative larger thoracic kyphosis and negatively larger sagittal balance were also significant risk factors even in the multivariate logistic regression analysis.
Multivariate Logistic Regression Analysis of the Variables for PJK.
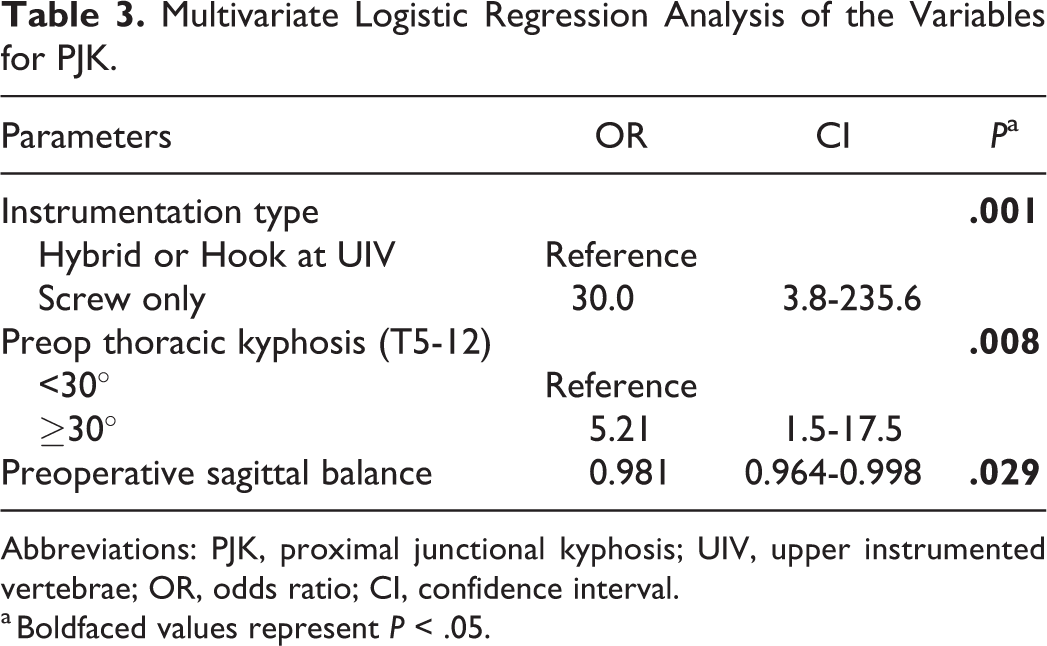
Abbreviations: PJK, proximal junctional kyphosis; UIV, upper instrumented vertebrae; OR, odds ratio; CI, confidence interval.
a Boldfaced values represent P < .05.
Discussion
We examined the incidence of PJK following PSF for AIS. The overall incidence was 4.3%. This was lower than previously reported incidence at 7% to 46%. 3,4,6,8 -10,12 This discrepancy may be due to the difference of PJA/PJK definition, which varied among studies. Some studies measure the difference between pre- and postoperative radiographs, while others, similar to this study, measure the difference between the immediate postoperative and latest follow-up film. Another possibility is the difference in instrumentation type. Several studies showed lower PJK incidence in hook or hybrid constructs. 8 -10 Our cohort included higher percentage of patients using hooks (217/345), which may attribute to lower PJK incidence in our study.
PJK can include fracture of the upper instrumented vertebrae (UIV) or UIV +1, soft tissue failure and implant pull-out. 13 The type of failure depends on the level of the UIV. Soft tissue failure is more common for upper thoracic UIV while fracture is more common for thoracolumbar UIV. 14 Fracture or implant pull-out is less common in AIS as adolescent patients have better bone quality than patients with adult spinal deformity. In fact, pull-out or fracture was not recognized in our study. All PJK patients in our cohort were classified into soft tissue failure type. Given this finding, instrumentation type, especially anchors at UIV, may play an important role in PJK.
Although hook or hybrid constructs may reduce PJK, a consensus has not been reached. Some studies showed that the incidence of PJK was equivalent among all-pedicle screw, all-hook and hybrid constructs. 5 -7 Liu et al 7 compared postoperative PJA change between all-pedicle screw and hybrid constructs in Lenke 1 curve and showed no significant difference. A systematic review comparing all-pedicle screw with hybrid constructs also showed no significant difference in PJK incidence. 5 Pahys et al 6 compared all-pedicle screw with hooks at UIV with distal all screw constructs and demonstrated that the incidence of PJK was equivalent.
On the contrary, several studies reported that all-pedicle screw constructs had higher PJK incidence than all-hook or hybrid constructs. 8 -10 Kim et al 9 conducted a large-scale study comparing all-pedicle screw (97), all-hook (210), and hybrid (103) constructs. They noted a lower rate of PJK in patients with all-hook constructs compared with all-pedicle screw and hybrid constructs. There was no difference between all-pedicle screw and hybrid constructs in the study. The authors did not define their hybrid constructs or identify a specific cohort with hooks at the UIV. 9 Helgeson et al 8 compared all-pedicle screw (37), all-hook (51), hybrid (177), and hooks at UIV (18) constructs. They reported higher rate of PJK in all-pedicle screw constructs than all-hook and hybrid constructs. Their grouping is reasonable and similar to our study; however, each group includes relatively less patients other than the hybrid group. 8 Wang et al 10 compared the incidence of PJK between hooks at UIV and screws at UIV constructs. They found that hooks at UIV constructs had significantly lower PJK incidence. However, sample size is relatively smaller, and they focused on only UIV anchor type. The concept of hooks at UIV differs from that of hybrid constructs. To obtain a solid evidence, we used appropriate criteria for grouping with more than 100 patients in each group.
Our study showed that all-pedicle screw constructs had significantly higher incidence of PJK incidence compared with hybrid and hook at UIV constructs. This finding is similar to some of the previous reports. 8 -10 The reason why all-pedicle screw constructs increase PJK remains unclear. However, 2 hypotheses have been proposed. First, increased rigidity and decreased thoracic kyphosis after PSF using screws may be related to PJK. Pedicle screw constructs have greater correction ability than hook constructs but result in less thoracic kyphosis. 15 PJK may be a compensation for the decreased thoracic kyphosis to restore global sagittal balance. 9,10 This is seen in our cohort, where a postoperative decrease in thoracic kyphosis was significantly larger in the PJK group compared with non-PJK group. Sagittal balance was also more negative in the PJK group than the non-PJK group postoperatively. These findings are consistent with the hypothesis that increased PJA is a compensatory mechanism for decreased thoracic kyphosis and subsequent negative sagittal balance. There is another study to support this hypothesis. Rhee et al 16 investigated the difference of sagittal plane radiographical parameters between ASF and PSF; ASF was kyphogenic while PSF was lordogenic within fusion area, which they attributed to anterior compression force in ASF. They also showed PSF was associated with greater increases in PJA than anterior surgery in AIS. 16 These findings suggest that PJK is a compensatory mechanism; decreased kyphosis or increased lordosis within fusion area leads to negative sagittal balance after PSF, resulting in proximal kyphosis to restore global sagittal balance.
The second hypothesis is soft tissue disruption. Pedicle screw placement at the UIV often violates the supra-adjacent facet capsules. The incidence of facet violation was reported at 8% to 47% when using pedicle screws. 17 -19 In addition, a broad range of soft tissue dissection is necessary when inserting screws. Capsular disruption in addition to ligamentous and muscular disruption in PSF could increase susceptibility to PJK. We compared all-pedicle screw with hook at UIV with distal all screw constructs. The only difference between the 2 constructs is the anchor at UIV. However, the incidence of PJK was much lower in hook at UIV constructs (0%) than pedicle screw alone constructs (11%). This finding implicates that violation of supra-adjacent facet capsule largely contributes to PJK. To our knowledge, 3 studies have focused on UIV anchor type. Wang et al. demonstrated that the incidence of PJK in the group using screws at UIV was higher than that in the group using hooks at UIV. They speculated that hooks at UIV decrease overall rigidity and lessened the likelihood of PJK. 10 On the contrary, Pahys et al 6 showed that there was no significant difference in PJK incidence between screw alone and hooks at UIV with rest all screw constructs. They excluded patients with one-hook/one-screw at UIV from the HT group and their criterion of PJK was 15° or more increase in PJA. We included one-hook/one-screw and bilateral hooks at UIV in the HT group and our threshold was 10°. These factors may be related to their different result from our study. Interestingly, in our study, one-hook/one-screw at UIV had no PJK with average 2.2 years follow-up. Ferrero et al 12 analyzed the incidence of PJK in AIS and reported one-hook/one-screw was equivalent to bilateral hooks at UIV in terms of PJK 12 . We speculate that one-hook/one-screw constructs reduced the rate of PJK by allowing us to keep at least one facet capsule away from violation. To our knowledge, there has been no report where pedicle screw constructs were superior to hook or hybrid constructs in terms of PJK. Given the high incidence of PJK with all-pedicle screw constructs, bilateral hook or one-hook/one-screw placement at UIV would be a practical method to avoid PJK.
There are limitations in this study. First, this was a retrospective study with a relatively short follow-up period. Evaluation with long-term period is necessary to confirm our findings. Second, this is a multicenter database study, which includes different surgeons and techniques. The procedure was at the discretion of each surgeon. Third, all our treatment groups are not equal. We did not create matched cohort groups because this would have limited the sample size and have reduced the study’s power. In addition, we excluded all-hook constructs from the analysis because our cohort included much less patients with all-hook constructs. A larger sample size would be necessary to better evaluate all-hook constructs. Last, patients in this study underwent surgery before 2009. If the PJK in the patients with an all-screw construct resulted from postoperatively developed hypokyphosis, our conclusion might not be applicable to current patients. Recently, there have been many attempts to restore thoracic kyphosis using pedicle screws. 20 -22 Modern correction techniques can better restore kyphosis and might change the incidence of PJK in patients with an all-screw construct. A study comparing the patients in the present study with recently operated patients would be necessary to confirm our findings.
In conclusion, the overall incidence of PJK following PSF for AIS was 4.3%. The use of bilateral pedicle screws at UIV might PJK. Bilateral hooks or at least one hook at the UIV might prevent PJK.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.