
Abstract
Study Design:
Prospective randomized controlled trial.
Objective:
To study the effect of local steroids in the retropharyngeal space after anterior cervical discectomy and fusion (ACDF) in reducing prevertebral soft-tissue swelling (PSTS) and complications associated with it.
Methods:
A total of 50 consecutive patients operated with ACDF were double-blinded randomized into 2 groups: steroids (25) and control (25). Triamcinolone in collagen sponge was used in the steroid group and normal saline in gelatin sponge in the control group. Patients’ lateral radiographs were taken on the immediate postoperative day; days 2, 4, and 6; at 2 weeks; and 2 and 6 months postoperatively. The PSTS ratio at C3 to C7 and PSTS index were calculated. Patients were clinically evaluated using the Visual Analogue Scale (VAS) score for odynophagia and radiating pain, modified Japanese Orthopedic Association Score (mJOA), and Neck Disability Index (NDI).
Results:
PSTS showed a significant reduction in the steroid group as compared with the control group on the immediate postoperative day; days 2, 4, and 6; and at 2 weeks. However, at 2 and 6 months, PSTS remained the same. VAS score for odynophagia also showed a significant difference between the 2 groups on the immediate postoperative day; days 2, 4, and 6; and 2 weeks postoperatively, with no significant difference at the 2- and 6-month follow-up. mJOA and NDI showed no significant difference between the 2 groups at the 2- and 6-month follow-up.
Conclusion:
Use of retropharyngeal steroids helps in reducing the postoperative odynophagia on a short-term basis without any complication.
Keywords
Introduction
Anterior approaches to the cervical spine are needed for decompression of the neural elements when there is anterior neural compression. Among the various complications associated with the anterior approach, injury to the trachea resulting from iatrogenic causes, hematoma, angioedema leading to dyspnea or respiratory distress, and injury or compression on the esophagus leading to dysphagia and odynophagia are the most common ones. 1,2
Dysphagia and odynophagia are among the most commonly experienced complications following ACDF, with incidence ranging from as low as 1% to 71% in the literature. 3,4 Intraoperative excessive retraction, laryngeal nerve palsy, and soft-tissue swelling are among the proposed causes of dysphagia. 5 -7 Prevertebral soft tissue swelling (PSTS) is the swelling of the soft tissues lying anterior to the cervical spine vertebrae. Surgical inexperience, improper soft-tissue handling, surgery period of more than 2 to 3 hours, blood loss more than 300 ml and more than 3 level cervical spine surgery 4,8,9 are the various factors that can lead to this complications.
Corticosteroids inhibit the prostaglandins and cytokines that are responsible for the inflammatory process. This inflammatory process is responsible for the soft-tissue swelling, which ultimately leads to compression of the trachea and esophagus. Use of local steroids in the spine is not a new technique. There are reports of local application of steroids in the epidural space following lumbar discectomy, which is known to significantly reduce pain in the immediate postoperative period. 10 Use of intravenous (IV) steroid for management of PSTS has been described in the literature with various conflicting results. 11,12 However, there are very few reports about the use of localized steroids in anterior cervical spine surgery in the recent literature. 13 -15 The purpose of our study was to analyze the effect of local steroids in the retropharyngeal space following ACDF.
Materials and Methods
We conducted a prospective randomized double-blinded parallel study at a tertiary care center, with a study duration of 2 years (2017-2018). Institutional Ethics Committee approval was taken prior to commencement of the study. After taking informed valid consent, 50 consecutive patients operated with anterior cervical discectomy and fusion (ACDF) with anterior cervical plating and who satisfied our selection criteria were included in our study (Table 1). These patients were randomized into 2 groups, with 25 in each group: the case study (steroid) group and control (nonsteroid) group.
Selection Criteria.
Abbreviations: ACDF, anterior cervical discectomy and fusion; IV, intravenous; RA, Rheumatoid Arthritis.
Randomization
Randomization was done by a person who did not participate in patient clinical care using a computerized random number generator. Patients were blinded for their cohort randomization. Data interpretation was performed by an investigator blinded to the treatment that the patient was receiving, to prevent any bias during the surgery.
Procedure
All surgeries were performed in the supine position under general anesthesia. All patients underwent ACDF of 1 to 2 level with the conventional Smith and Robinson approach, with autologous corticocancellous bone grafting and anterior cervical plating. A transverse incision along the medial border of the sternocleidomastoid was taken on the left side in all cases. Subcutaneous dissection was done till the platysma. The platysma was divided vertically to see the medial border of the sternocleidomastoid properly. A space was created medial to the sternocleidomastoid between the carotid sheath and medial structure by blunt dissection. This exposed the longissimus colli muscles and pretracheal fascia. After fluoroscopic confirmation of the involved segment, discectomy was done. The cartilage and the end plates were removed using a burr till the subchondral bone was exposed. The tricortical iliac crest bone graft was used for fusion with the anterior cervical plate. Saline irrigation and meticulous hemostasis was done throughout the procedure. Collagen sponge with triamcinolone (40 mg)—that is, steroid—was introduced in the retropharyngeal space. Then, the platysma layer was closed, and subcutaneous and skin closure was done with a closed suction drain. A thin sterile dressing was applied.
A total of 25 patients who were included in the study as cases were the patients in whom we administered local steroid—that is, triamcinolone (40 mg)—in the collagen sponge in the retropharyngeal space, whereas the other 25 were selected as controls and saline was given in the collagen sponge. IV antibiotics—namely, injection cefuroxime 500 mg—twice a day for 2 days were given postoperatively.
Radiographic Assessment 13
To measure the extent and change of PSTS, simple cervical spine lateral radiographs were taken preoperatively; immediately after the operation; at postoperative days 2, 4, and 6; and at 2 weeks, 2 months, and 6 months. On the radiographs, we calculated PSTS ratio based on the ratio of the prevertebral soft-tissue thickness measured to the anteroposterior (AP) diameter of each vertebral body. The AP diameter of the vertebral body from C3 to C7 was measured between the center of the anterior and posterior cortex of each vertebral body. In the vertebral body where anterior plating was done, we measured from the anterior most point of the plate and the posterior most point of the pharynx, which is the PSTS. The vertebral body AP diameter was taken in the same was as we for the nonplated vertebral body (Figure 1). To compare the overall PSTS of the 2 groups, the average value of PSTS ratio at C3, C4, and C5 where edema is observed most clearly was defined as the prevertebral soft-tissue swelling index (PSTSI). Plain radiographs and computed tomography (CT) scans were used in the evaluation of postoperative union after 1 year of follow-up for every patient. Evidence of radiological union included the presence of bony extension into the space between the graft and the absence of segmental motion. Disconnection of the bony trabeculae with a radiolucent line around the instrument was considered pseudo-arthrosis.
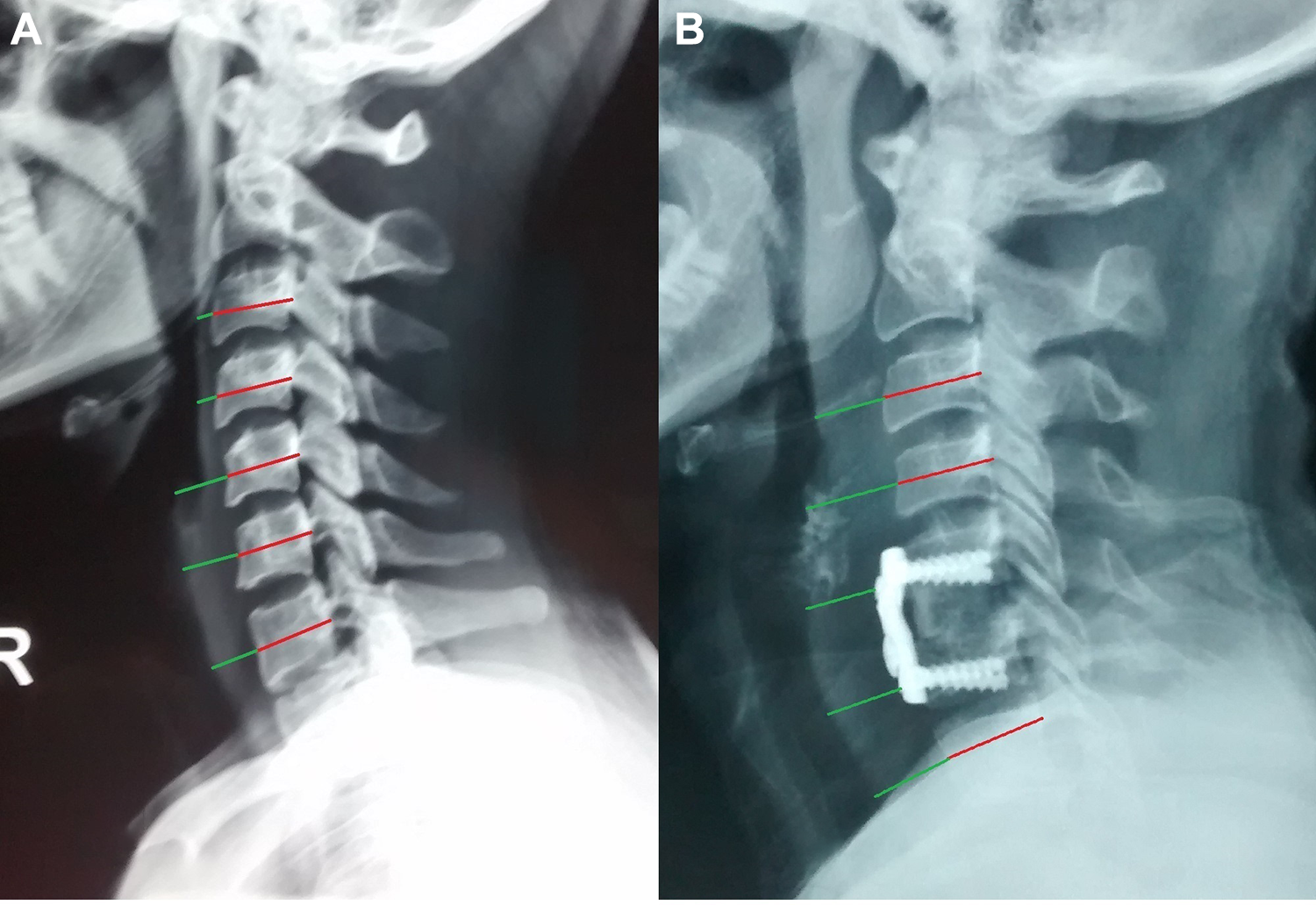
PSTS ratio calculation: A. PSTS in preoperative lateral X-rays. B. PSTS calculation with anterior cervical plating cervical plate.
Clinical Assessment
In the laboratory study for inflammatory response, changes in white blood cell (WBC) count were analyzed on postoperative days 2 and 4. The total amount of postoperative drainage was measured on postoperative days 2 and 4, and changes in odynophagia were measured immediately after operation and on postoperative days 2, 4, and 6, and at 2 weeks, 2 months, and 6 months using the Visual Analogue Scale (VAS). At 6 months, clinical outcomes were analyzed using the Neck Disability Index (NDI), modified Japanese Orthopedic Association Score (mJOA), and VAS score for radicular pain.
Statistical Analysis
Quantitative data is expressed in terms of mean values with corresponding SDs. The independent 2-sample t-test was used for comparisons of variables; statistical significance was defined as a P value of <.05.
Results
Demographic Results
A total of 50 patients were included in our study. The mean age of the patients was 50.4 years, with a minimum follow-up of 12 months. There were 38 male and 12 female patients. The average time required for each surgery was 2 hours and 21 minutes. In all, 8 patients underwent 2-level discectomy, and 48 patients underwent 1-level discectomy. Both the groups were comparable.
Radiographic Results
The PSTSI was lower in the patients who received retropharyngeal steroids as compared with the control group in the immediate postoperative period and day 2, day 4, day 6, and 2 weeks (P values: .0390, .018, .0060, .0440, .0190, respectively). However, no statistical difference was seen at 2 months and 6 months (P = .06 336 and .05 791). At baseline (preoperative), no significant difference was observed in the PSTS ratio and PSTSI between both groups (Table 2).
PSTS of Each Cervical Vertebra.
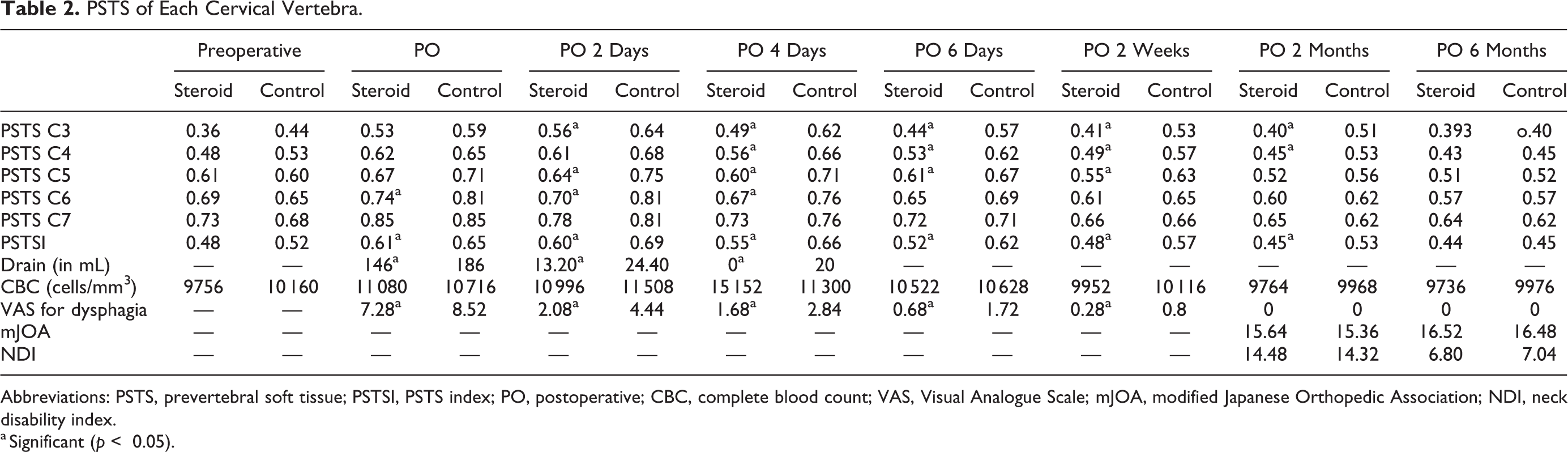
Abbreviations: PSTS, prevertebral soft tissue; PSTSI, PSTS index; PO, postoperative; CBC, complete blood count; VAS, Visual Analogue Scale; mJOA, modified Japanese Orthopedic Association; NDI, neck disability index.
a Significant (p < 0.05).
Immediate Postoperative Period
Patients showed significant statistical difference of PSTS ratio at the C6 level (P = .0088), whereas PSTS ratios at C3, C4, C5, and C7 were not statistically significant (P = .0552, .2251, .2945, and 1, respectively; Figure 2)
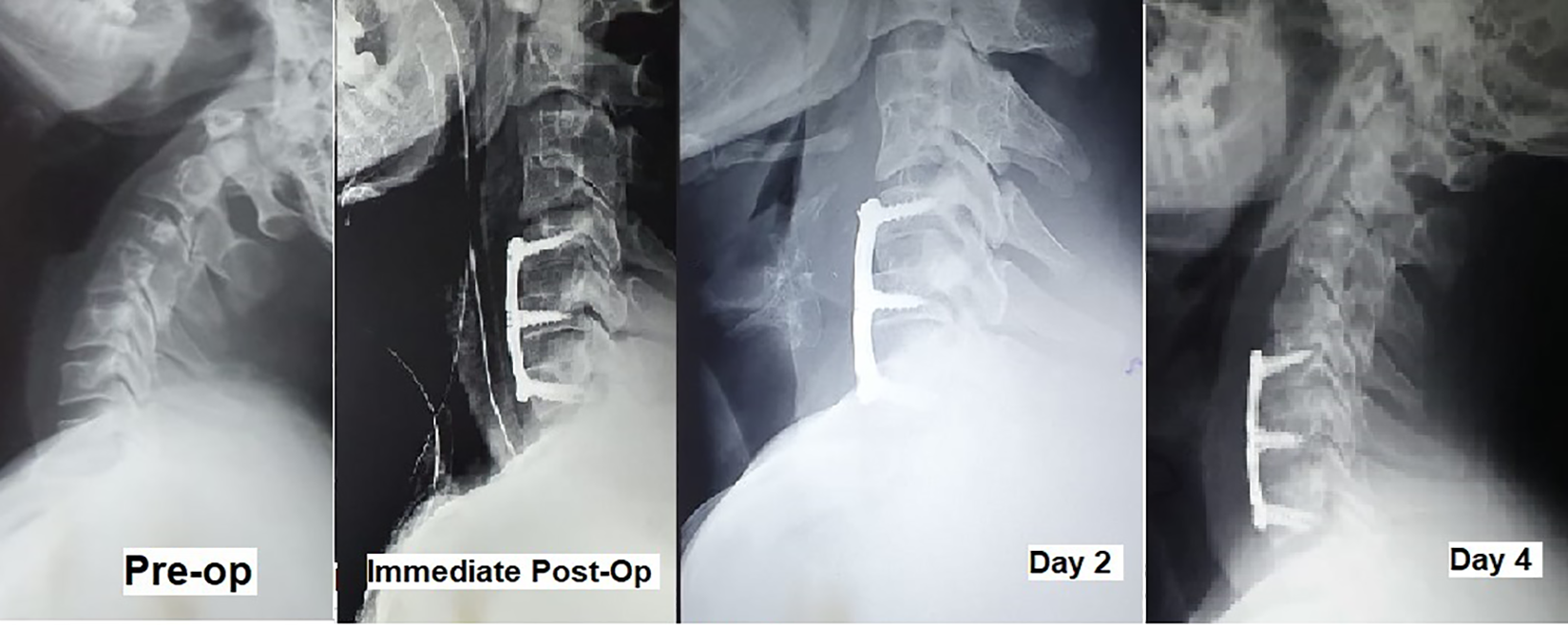
PSTS on preoperative and postoperative days.
Day 2, Postoperative Period
There was a statistically significant difference of PSTS ratio at C3, C5, and C6 (P = .0075, .0010, and .0003, respectively), whereas the data suggest no significant difference at C4 and C7 levels (P = .0536 and .3307, respectively).
Day 4, Postoperative Period
Showed statistical significance difference of PSTS ratio at C3, C4, C5, and C6 and no significant statistical difference at the C7 level (P = .0001, .0051, .0003, .0027, .3694, respectively).
Day 6, Postoperative Period
PSTS ratio showed significant statistical difference at cervical levels C3, C4, and C5 (P values: <.0001, .0091, and .0225, respectively) and no statistical difference at C6 and C7 levels (P = .0706 and .7381, respectively).
2-Week Postoperative Period
PSTS ratio at C3, C4, and C5 levels showed statistically significant difference, whereas at C6 and C7, there was no statistically significant difference seen (P = .0001, .0167, .0006, .0512, and 1, respectively).
2-Month Postoperative Period
C3, C4 (P = .0002 and .0138) showed statistical significance of PSTS ratio, whereas no significant statistical difference was seen at C5, C6, and C7 (P = .4553, .2508, and .0689, respectively).
6-Month Postoperative Period
No significant difference was seen at any level.
Clinical Results
The immediate postoperative period showed a statistical difference in the VAS score for odynophagia (P value = .0001) between the 2 patient groups, but there was no significant difference for radicular pain. Mean drain output in group 1 was 140 mL, and in group 2, it was 186 mL, which is statistically significant (P = .0001).
VAS score for odynophagia showed a statistical significant difference between the 2 groups on day 2, day 4, and day 6 and at the 2-week postoperative period (P = .0001, .0002, .0001, and .0003, respectively). However, VAS score for radiculopathy showed no significant difference during the whole study period. Drain output in the immediate postoperative period and on days 2 and 4 showed statistical significance (P = .0001, .0499, .0001).
However, mJOA and NDI showed no statistically significant differences between groups at 6 months (P = 1.000 and .3886, respectively). Similarly, WBC counts failed to show any statistically significant difference between the 2 groups.
All patients, except 2 in whom 2-level fusion was done, achieved bony union at the end of 12 months of follow-up, which was confirmed with a CT scan, and no complications were seen during the study period. The 2 nonunion patients remained asymptomatic for that 1 year, and a decision was made to continue monitoring these 2 patients.
Discussion
ACDF is a common surgery done nowadays for anterior cervical spine pathology mostly for cervical myelopathy or radiculopathy because of disc prolapse anteriorly or any other compressing structures. Among the many complications while doing anterior cervical spine surgery, postoperative dyspnea and dysphagia are the most common, 1,2 with one of the reasons being soft-tissue edema leading to compression and dysphagia. Various methods have been advised to prevent or reduce the overall severity of this complication. These include delayed extubation, use of IV steroids, and use of local steroid in the retropharyngeal space.
Jeyamohan et al 11 showed a significant reduction in postoperative swallowing function and airway edema after using IV dexamethasone in the perioperative period. In the prospective study conducted by Emery et al, 12 33 patients received 3 doses of IV steroids, whereas 33 patients received only saline, and no significant differences were found between the 2 groups.
Lee et al 13 used 40 mg local triamcinolone over morcellized collagen sponge, whereas saline was used in the control group, and recommended use of local steroids in ACDF because it tends to reduce PSTS and postoperative dysphagia. Koreckij et al 14 conducted a similar study for multilevel ACDF, where they used localized methylprednisolone in the steroid group and control group; they found reduction in dysphagia in the immediate postoperative period. However, in a randomized trial conducted by Haws et al, 15 where the authors divided 104 patients into 2 groups of local steroid and control, no significant difference was found between the 2 groups. This has led to a debate regarding the use of local steroids in ACDF.
Suk et al, 8 in their study, had maximal PSTS on day 3, whereas our study had maximal PSTS on day 2 in the control group and immediate postoperative period in the steroid group, with decreasing trend later. However, PSTSI showed a significant difference between the 2 groups in the immediate postoperative period; on the second, fourth, and sixth days; and 2 weeks postoperatively suggesting that there is reduction in the PSTS following ACDF in patients when a local retropharyngeal steroid was used (Figure 3). Particularly on postoperative day 2 and day 4, there was significant reduction in the PSTS in the steroid group compared with the control group, when the risk of prevertebral soft-tissue related complications are highest. The PSTSI nullifies the differences seen among individuals, such as width of the vertebral body or any other abnormality of the neck or retropharyngeal space. Hence, the PSTSI helps us compare with other postoperative patients and also with themselves.
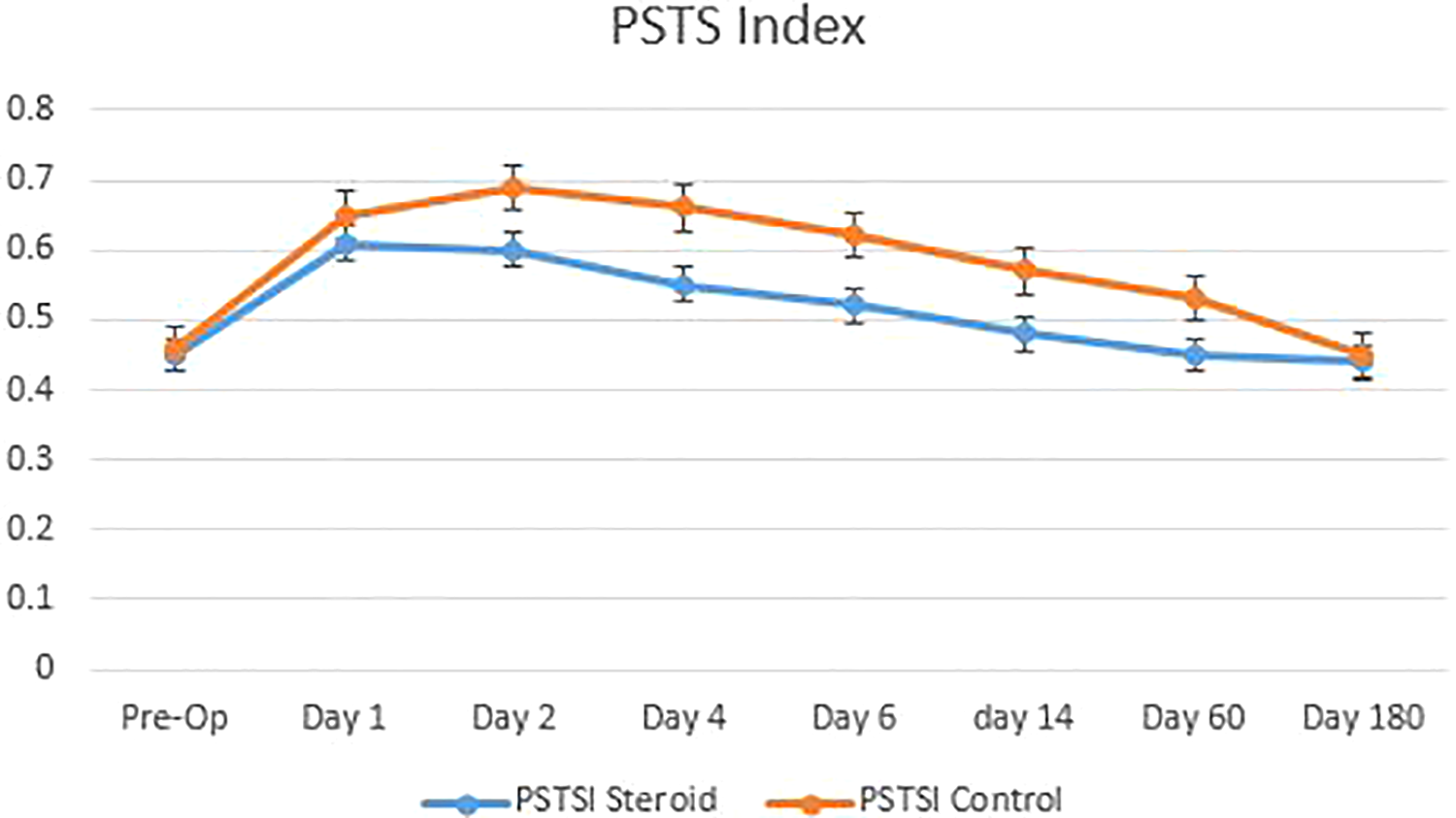
Line diagram showing decrease in PSTSI with decreasing trend.
In our study, we found that the VAS score for odynophagia in the immediate postoperative period; on days 2, 3, 4, and 6; and at 2 weeks was less in the steroids group compared with the control group (Figure 4). These results were comparable to those of Lee et al 13 and Koreckij et al, 14 which showed similar outcomes. In our study, the mJOA and NDI were not statistically significant during the follow-up at 2 weeks, 2 months, and 6 months postoperatively between the 2 groups. This suggests that local steroids do not have significant effects on long-term results. Lee et al found a reduction in drain output between the 2 groups, but it was statistically insignificant. However, in our study, we found a statistically significant reduction in drain output on postoperative days 2 and 4. 13 This suggests that locally available steroids reduce the inflammation and effusion during the postoperative period, leading to reduced drain output.
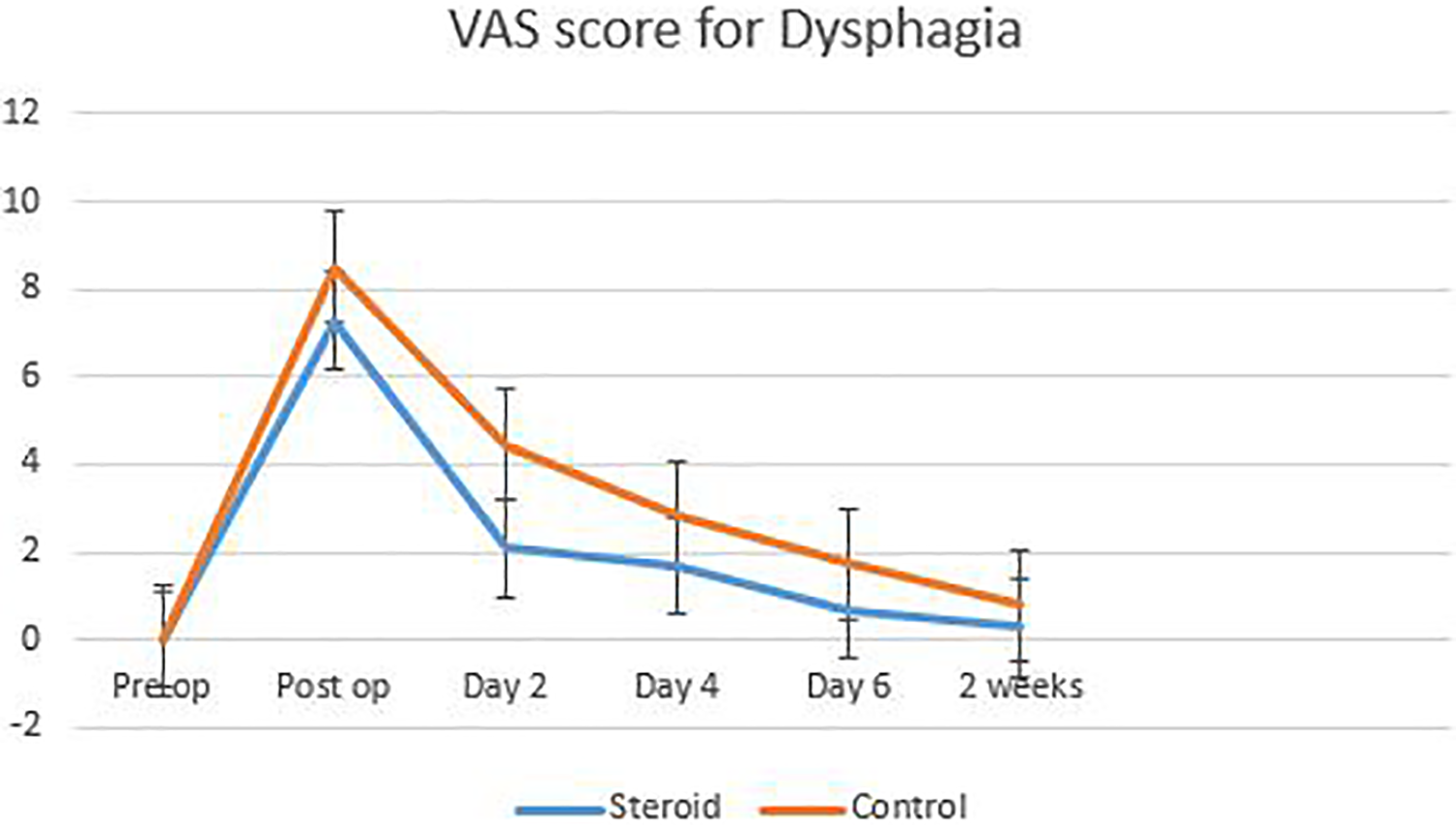
Line diagram showing decrease in dysphagia with decreasing trend.
Major concerns regarding the use of local steroids were nonunion and increased chances of esophageal perforation. In a recent study, conducted by Jenkins et al, 16 where they randomized patients into IV steroid and local steroid groups, they found 2 cases of pseudoarthrosis in 2 patients in the local steroid group after a period of 1 year. In our study, at the 1-year follow-up, CT scans showed that 2 patients from each group (ie, the steroid and control groups) had signs of nonunion, making both the groups comparable and ruling out the effect of steroids on union.
Esophageal perforation is one of the most dreadful complications of ACDF, with an incidence of 0.02% to 1.52%. 17 Local steroid use decreases the potential for soft-tissue injury to heal on its own and increases the chances of perforation. Two cases have been reported in the literature of esophageal perforation after local retropharyngeal steroid use, though these patients were on chronic steroids, which we have excluded in our study. 18 Limitations of our study are a small sample size, use of only VAS score for assessment of dysphagia, the fact that it was a single-institute study, short-term follow-up, radiation exposure, and no involvement of multilevel discectomy (more than 2-level discectomy).
In conclusion, we would like to remark that use of a local steroid in the retropharyngeal space reduces the PSTS in ACDF and reduces postoperative odynophagia in the short-term, thus helping in early recovery of patients, without any complications.
Supplemental Material
Supplemental Material, CONSORT_2010_Checklist - Prospective Randomized Controlled Trial to Study the Effect of Local Steroids in the Retropharyngeal Space After Anterior Cervical Discectomy and Fusion
Supplemental Material, CONSORT_2010_Checklist for Prospective Randomized Controlled Trial to Study the Effect of Local Steroids in the Retropharyngeal Space After Anterior Cervical Discectomy and Fusion by Aditya Dahapute, Sandeep Sonone, Shubhanshu Bhaladhare, Kuber Sakhare, Nandan Marathe, Sai Gautham Balasubramanian and Swapnil Keny in Global Spine Journal
Supplemental Material
Supplemental Material, CONSORT_2010_Flow_Diagram - Prospective Randomized Controlled Trial to Study the Effect of Local Steroids in the Retropharyngeal Space After Anterior Cervical Discectomy and Fusion
Supplemental Material, CONSORT_2010_Flow_Diagram for Prospective Randomized Controlled Trial to Study the Effect of Local Steroids in the Retropharyngeal Space After Anterior Cervical Discectomy and Fusion by Aditya Dahapute, Sandeep Sonone, Shubhanshu Bhaladhare, Kuber Sakhare, Nandan Marathe, Sai Gautham Balasubramanian and Swapnil Keny in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplementary Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.