
Abstract
Study Design:
A systematic review and meta-analysis.
Objectives:
Cervical total disc replacement (CTDR) can preserve range of motion (ROM) of the operated spinal segment in cadaver studies. Evidence is less clear in clinical trials. The present study aims to investigate the differences in cervical biomechanics before and after CTDR and its association with heterotopic ossification (HO) development.
Method:
Articles that reported the rate of HO and ≥1 difference in cervical biomechanics were included in quantitative analyses. We pooled the mean difference (MD) of cervical biomechanics before and after CTDR. Subgroup analyses and metaregression analyses were conducted to identify potential contributors to heterogeneity.
Results:
Of the 599 studies screened, 35 studies were included in the final analysis. In comparison with preoperative values, ROM of the spinal segment inferior (MD: 0.38; 95% CI: 0.02 to 0.74) and superior (MD: 0.43; 95% CI: 0.12 to 0.75) to the surgical spinal segment, functional spinal unit (FSU) angle (MD: 2.23; 95% CI: 1.11 to 3.35), and C2/C7 Cobb angle (MD: 3.49; 95% CI: 1.73 to 5.25) significantly increased after CTDR. In contrast, FSU and cervical ROM at baseline were no different from follow-up. On multivariable meta-regression analyses, HO and ROM-limiting HO were not associated with changes in cervical biomechanics. Single-level CTDR and duration of follow-up were associated with changes in cervical biomechanics.
Conclusion:
Our study reported the pooled mean of biomechanics at baseline and final follow-up and their differences. The changes in biomechanics were not associated with the rates of HO and ROM-limiting HO.
Introduction
Anterior cervical discectomy and fusion (ACDF) is the gold standard treatment for refractory cervical degenerative disc disease. Although ACDF is effective in alleviating signs and symptoms of patients and has a low rate of complications, 1 symptomatic adjacent segment disease (ASDisease) can develop in the long run. 2 The pathogenesis of ASDisease is unknown. The most widely accepted theory is that fusion of spinal segments significantly reduces motion of the operated spinal segment and, thus, increases intradiscal pressure at the adjacent segments and accelerates degeneration at these levels. 3,4
Cervical total disc replacement (CTDR) has been developed as an alternative to ACDF. The theoretical advantage of CTDR over ACDF is the preservation of segmental motion at the operated level; it may, therefore, reduce the risk of adjacent segment degeneration and ASDisease. 5,6 Although the motion preservation benefit of CTDR has been confirmed by previous in vitro studies, 7,8 a consensus on whether CTDR can preserve cervical biomechanics cannot be reached in clinical trials. 9 -12 Moreover, the development of heterotopic ossification (HO), a known complication of CTDR, 13 may reduce range of motion (ROM) of the operative spinal segment, especially in severe forms (grade III and IV). 14 However, no review, to our best knowledge, has yet examined whether biomechanical parameters are preserved after CTDR and its association with HO formation. It has been postulated that HO is induced by the altered cervical biomechanics after CTDR. 15,16 The primary aim of our study is to investigate if the changes in biomechanical measures before and after CTDR, if any, are attributable to the formation of HO.
Methods
Study Selection
This systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analysis protocols (PRISMA-P) guideline and the guidelines for academic neurosurgeons. 17 -19 Medical subject headings (MeSH) and search terms that were related to CTDR and HO were used in data searches, including heterotopic ossification, heterotopic bone, cervical, arthroplasty, total disc/disk replacement, artificial disc/disk replacement, and disc/disk prosthesis.
Published articles in MEDLINE (OVID interface, 1948 onward), EMBASE (OVID interface, 1980 onward), the Cochrane Central Register of Controlled Trials (Wiley interface, current issue), and PubMed databases were searched up to April 2018. The reference lists of publications retrieved in the initial literature search were screened for potential studies. We further supplemented the searches by contacting the corresponding authors if there were incomplete data or the rate of HO was expressed in number of patients but not in number of spinal segments.
After the removal of duplicated articles and screening of titles and abstracts, 2 reviewers assessed the eligibility criteria of the full-text articles. Any discrepancy in the data collection process was first resolved by discussion between the 2 reviewers, then by consulting the senior author if a consensus could not be reached.
The inclusion criteria were as follows: Reported ≥1 difference in biomechanical factor before and after CTDR Reported the rate of overall HO Patients ≥18 years of age who underwent TDR in the cervical spine There was no restriction on the number of radiologists/spine surgeons who graded and diagnosed HO, or the type of prosthesis used in CTDR Articles published in English
The exclusion criteria were as follows: Nonclinical studies such as letter to the editor, review articles, case reports, or cadaver tests or editorials Rates of overall HO expressed in number of patients Duplicated publications Radiological follow-up shorter than 1 year
Data Extraction
The primary outcomes measures were the differences in biomechanics of the cervical spine before and after CTDR: functional spinal unit (FSU) height (in millimeters), C2/C7 Cobb angle, FSU angle and ROM of the operative segment and its superior and inferior spinal segment, disc/shell angle, and cervical ROM. To ensure consistency, the rate of HO was expressed in the number of spinal segments, but not in the number of patients. If a data set involved the same study location and study population was published more than once, only the more recent article with the more comprehensive data would be included.
Assessment of Methodological Quality
The methodological quality of the included randomized controlled trials (RCTs) was appraised in accordance with the guideline published by the Cochrane Back and Neck Group (CBNG) in the Cochrane Handbook for Systematic Review of Interventions. 21 Item 11 of the CBNG guideline, which assesses compliance of intervention, was not applicable because CTDR is a single-session intervention. The methodological quality of the included non-RCTs was appraised in accordance with the Methodological Index for Non-randomised Studies (MINORS). 22
Statistical Analysis
Statistical analysis was conducted using OpenMetaAnalyst and R software. Heterogeneity between included studies was calculated using Q tests and the I2 statistic. A significant heterogeneity was defined as I2 ≥50% or P value <.10, in which a random-effect model was used. 23 Otherwise, the fixed-effects model was used.
We pooled the differences in biomechanics of the cervical spine using mean difference (MD) and 95% CIs. Subgroup analyses were conducted stratified by the type of prosthesis and the length of follow-up. Meta-regression analyses were run using the Restricted Maximum Likelihood model to identify possible associations of the differences in biomechanics of the cervical spine after CTDR with a combination of variables, including HO, ROM-limiting HO, length of follow-up, and the proportion of single-level CTDR. Multivariable meta-regression analyses were performed if the number of studies was larger than 10.
Results
Characteristics of Included Studies
A total of 599 articles were initially identified in searching the databases, of which 35 met the inclusion criteria and were included in the present meta-analysis (Figure 1). Table 1 summarizes the characteristics of the included studies. 9,11,24 -56 Two were RCTs, and 33 were nonrandomized trials, with a mean follow-up of 3.68 years (ranging from 1 year 52 to 15.5 years 25 ). Among a total of 1674 patients who underwent CTDR, mean age was 45.6, 55% were male, 76.9% underwent single-level CTDR, 17.3% were operated at the C4/C5 level, 52.3% were operated at the C5/C6 level, and 21.4% were operated at the C6/C7 level.
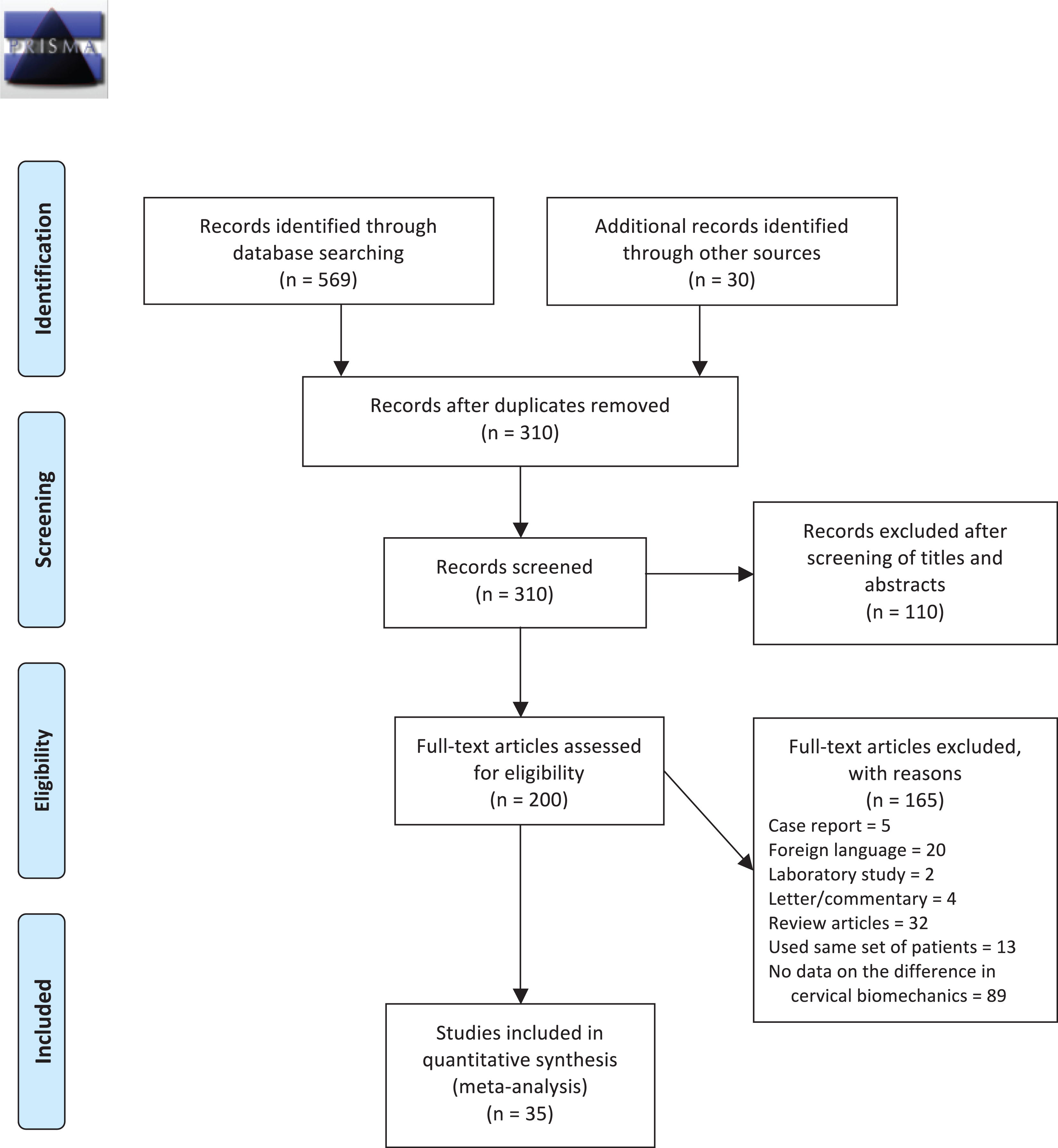
PRISMA 2009 flow diagram.
Study Characteristics.a
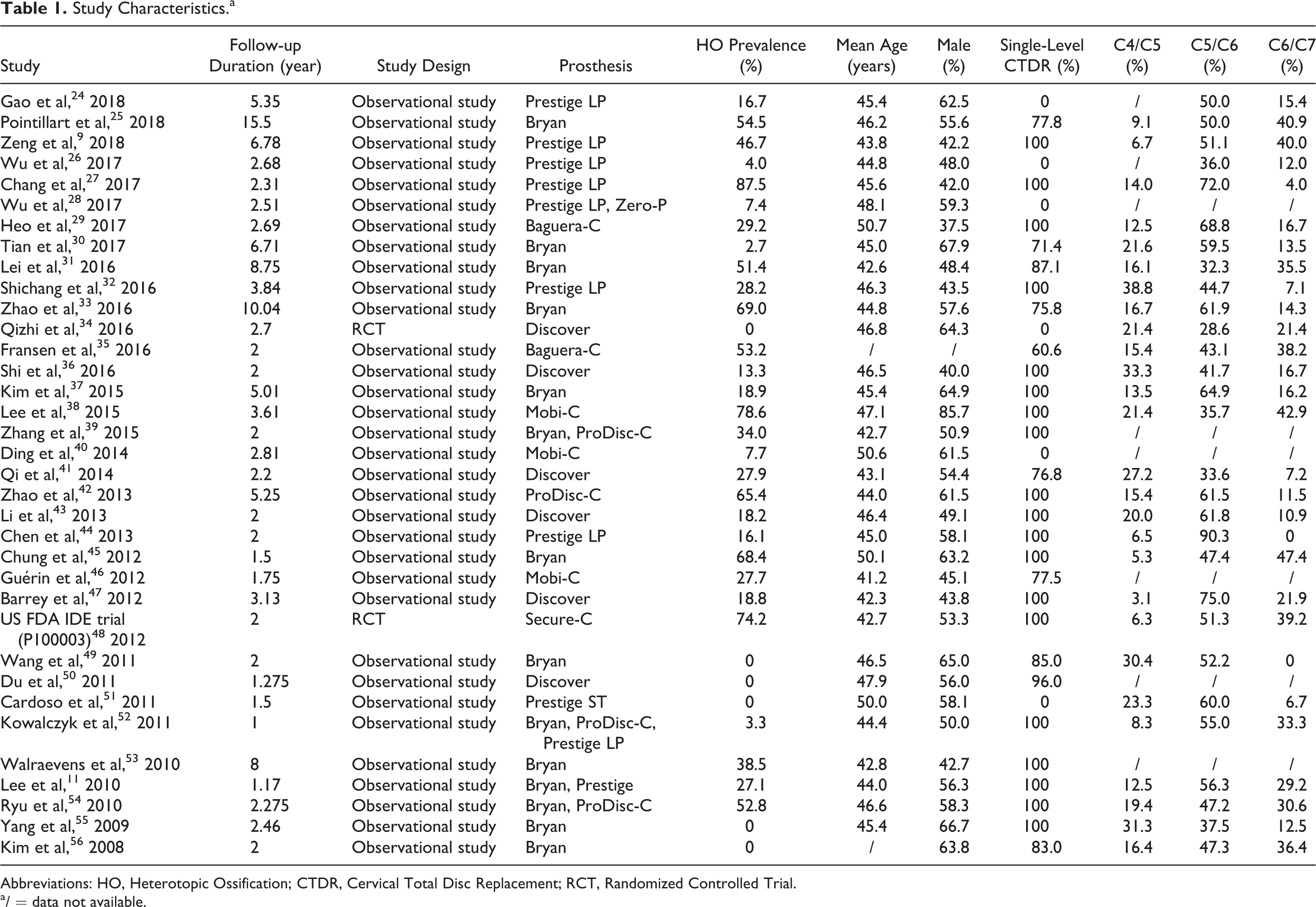
Abbreviations: HO, Heterotopic Ossification; CTDR, Cervical Total Disc Replacement; RCT, Randomized Controlled Trial.
a / = data not available.
Only 2 RCTs were included in the review. According to the CBNG guideline, both studies did not adopt intent-to-treat analysis and did not have information on the use of random sequence generation and allocation concealment (Figure 2). Otherwise, most of the other criteria were met. The average MINORS score for comparative studies was 17.6 (out of 24, ranging from 16 to 19), whereas the MINORS score for noncomparative studies was 9.4 (out of 16, ranging from 6 to 12).
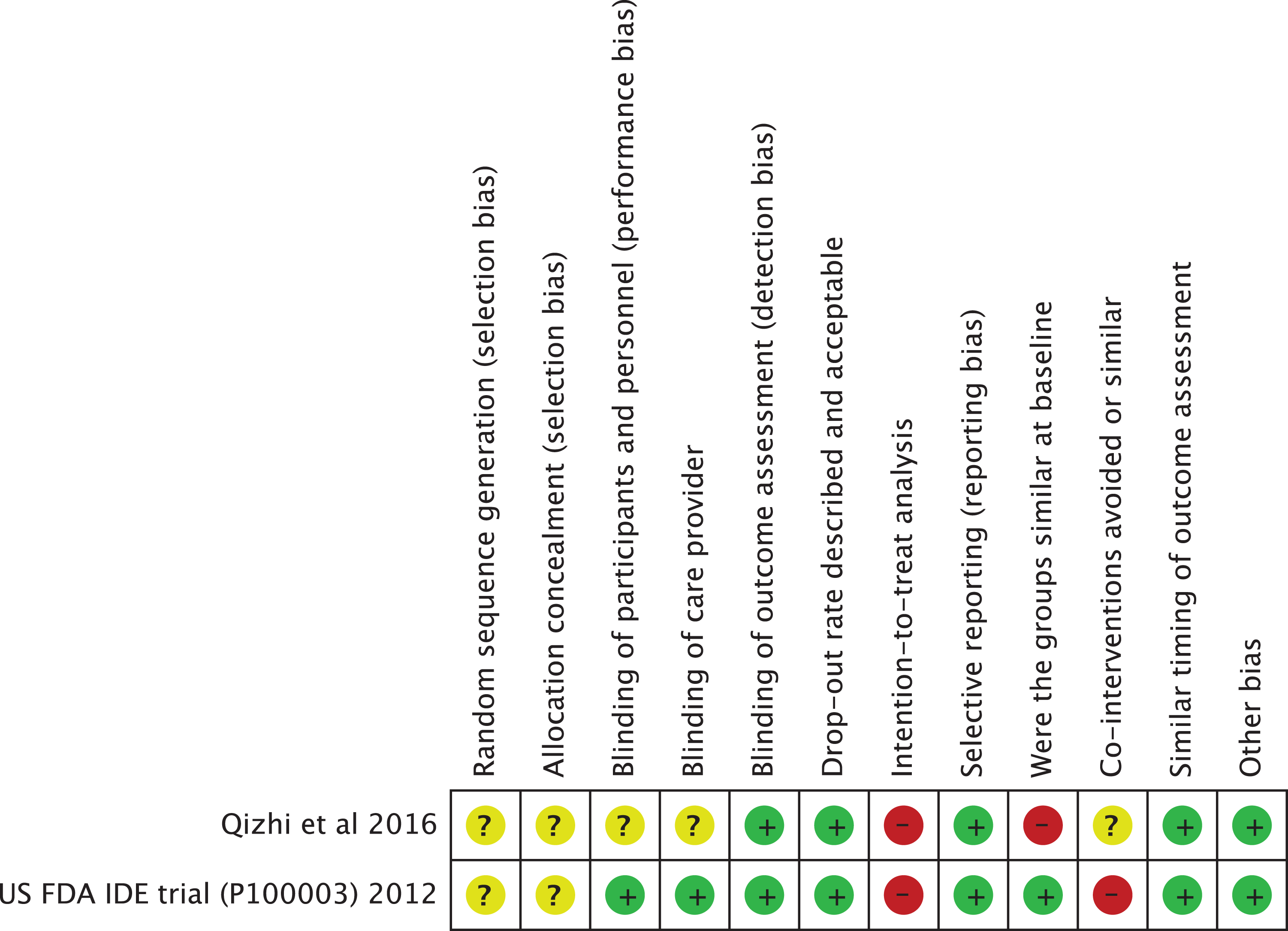
aRisk of bias summary table.
Biomechanical Measures
Table 2 summarizes the pooled mean of biomechanical measures before and after CTDR and their differences. Compared with the baseline values, ROM of the cervical segment inferior (MD: 0.38; 95% CI: 0.02 to 0.74) and superior (MD: 0.43; 95% CI: 0.12 to 0.75) to the surgical spinal segment, FSU angle (MD: 2.23; 95% CI: 1.11 to 3.35), and Cobb angle (MD: 3.49; 95% CI: 1.73 to 5.25) significantly increased at final follow-up. In contrast, FSU and cervical ROM were comparable between baseline and follow-up. Forest plots of the results in Table 2 are available in Supplementary File.
The Biomechanics of the Cervical Spine Before and After CTDR and Their Differences.
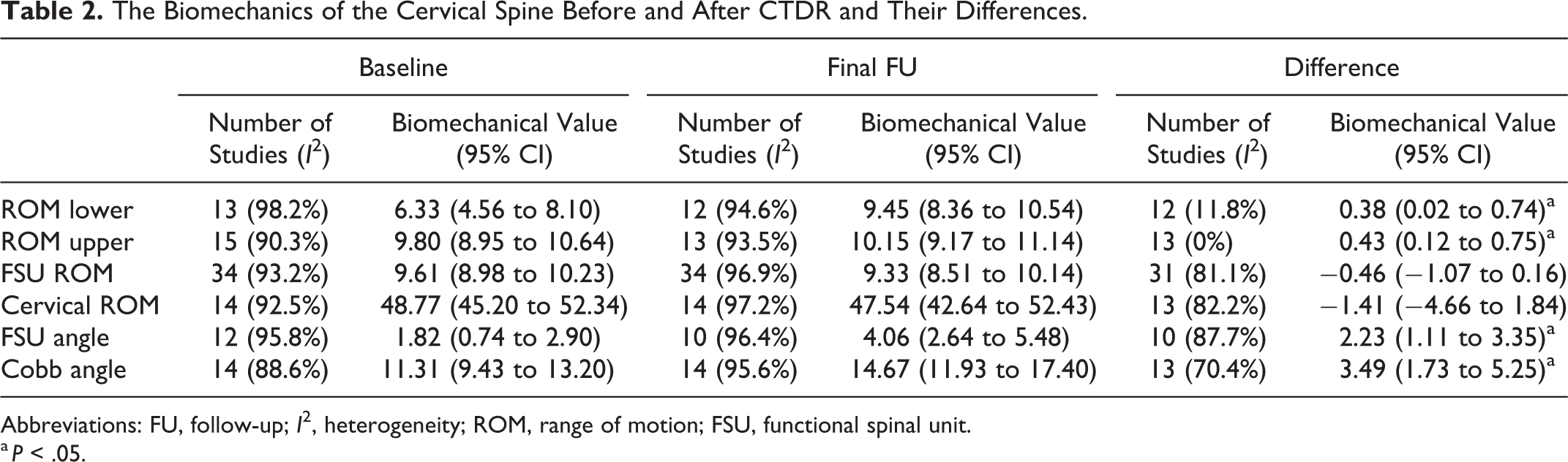
Abbreviations: FU, follow-up; I2, heterogeneity; ROM, range of motion; FSU, functional spinal unit.
a P < .05.
Subgroup Analyses
In light of the significant heterogeneity, we stratified the biomechanical measures based on the length of follow-up to identify potential effect modifiers (Table 2). As shown in Table 3, subgroup analyses revealed that the decrease in FSU ROM was significantly higher in studies with >6 years of follow-up (MD: −2.15; 95% CI: −2.97 to −1.33) compared with that in studies with 1 to 2 years of follow-up (MD: −0.03; 95% CI: −0.90 to 0.84). The difference in Cobb angle before and after CTDR was comparable between studies with 1 to 2 years and 2 to 3 years of follow-up. When stratified based on the type of prosthesis, the difference in FSU ROM was comparable between different types of prostheses. The limited number of studies in other biomechanical factors did not permit subgroup analyses. Forest plots of the results in Table 3 are available in Supplementary File.
Subgroup Analysis of the Difference in Biomechanics Stratified by the Length of Follow-up.a
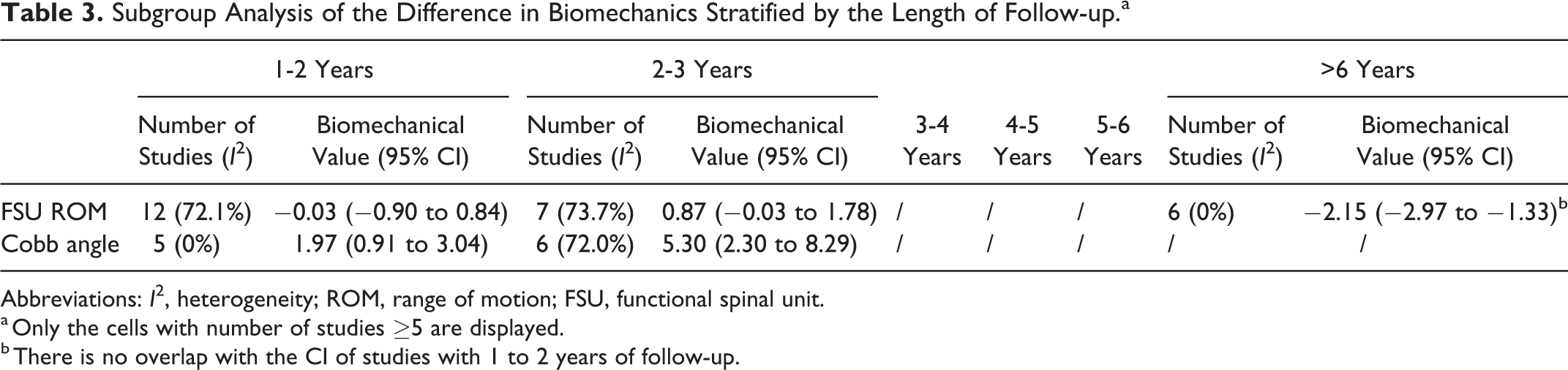
Abbreviations: I2, heterogeneity; ROM, range of motion; FSU, functional spinal unit.
a Only the cells with number of studies ≥5 are displayed.
b There is no overlap with the CI of studies with 1 to 2 years of follow-up.
Metaregression
Metaregression analyses were conducted to identify the association between various baseline and outcome variables with differences in biomechanics (Table 4). On multivariable regression analyses, HO was not associated with any differences in biomechanical factors. Because grade III and IV HOs are classified as ROM-limiting HOs, 20 we replace HO with ROM-limiting HO in the analyses. Similarly, ROM-limiting HO, and CTDR at C5/C6 and C6/C7 level was also not associated with any differences in biomechanical factors. On the other hand, single-level CTDR was inversely associated with the difference in ROM of the inferior segment but positively associated with the difference in cervical ROM. Moreover, the length of follow-up was associated with changes in FSU ROM.
Multivariable Metaregression of the Effects of Various Variables on the Changes in Cervical Biomechanics.
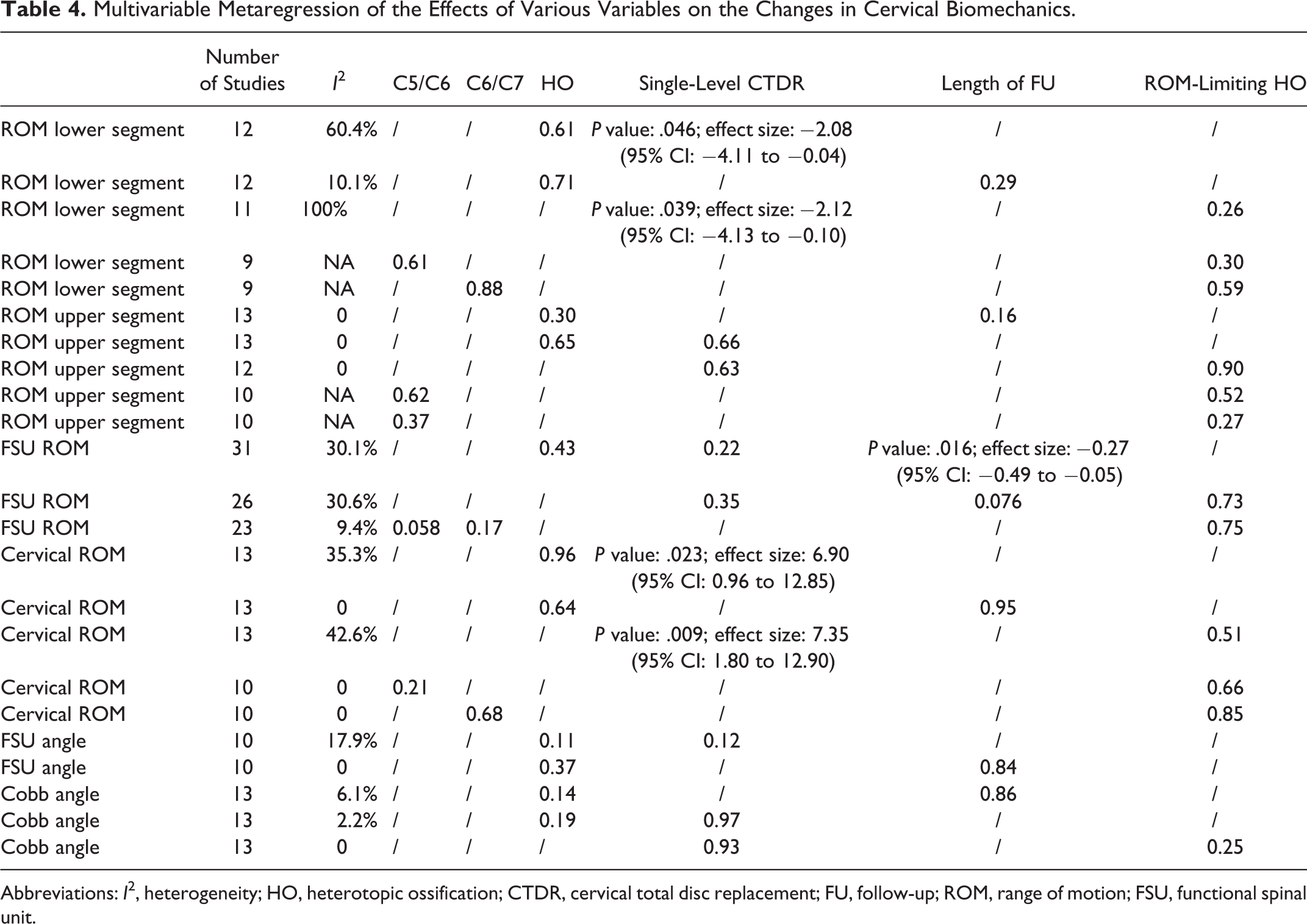
Abbreviations: I2, heterogeneity; HO, heterotopic ossification; CTDR, cervical total disc replacement; FU, follow-up; ROM, range of motion; FSU, functional spinal unit.
Discussion
The pathogenesis of HO formation after CTDR remains elusive. A recent meta-analysis of 82 studies estimated that the prevalence of HO after CTDR was 32.5%, which is comparable to the prevalence of 29.1% reported in our study. 13 A number of risk factors for HO have been proposed. For example, a multivariable Cox regression analyses demonstrated that male gender and obesity are positively correlated with a higher incidence of HO. 57 Other potential risk factors include operation level number 41,58 and older age. 59 However, the evidence is inconclusive in some observational studies. 45,46,60 Many theories have been proposed in an attempt to describe the pathophysiology of HO, the most noticeable of which is that HO is a self-defense physiological reaction in response to the nonphysiological biomechanics of the spine after CTDR. 15,16 Finite-element analyses demonstrated that shear and compressive forces on the cervical spine each induced a unique pattern of ectopic bone formation. 61,62 Although the cervical biomechanics significantly changed after CTDR, our study is the first to report that HO and ROM-limiting HO formation were not associated with changes in biomechanics of the cervical spine, which may seem to contradict the results in preclinical studies. One of the explanations is that the spine is a dynamic structure, and other spinal segments and muscular structures may adapt to the changes in cervical biomechanics after CTDR, minimizing biomechanical insult on the cervical bone. In fact, our study showed that some of the biomechanics of the spinal segments adjacent to the operative segment changed significantly at final follow-up. Because only some biomechanical factors were examined in our study, whether other biomechanical factors such as center of rotation have an association with HO development is worth future investigation.
The aim of CTDR, in theory, is to preserve ROM of the surgical spinal segment and minimize the risk of ASDisease. 6 Even though cadaver studies support the preservation of cervical biomechanics after CTDR 63,64 ; results from clinical trials are conflicting. 9 -12 Although various prostheses have their unique design and biomechanical properties, our study found no significant differences in the changes in FSU ROM between different types of prostheses. Also, we found that FSU ROM could be preserved up to 3 years after CTDR. Reasons for the modest, yet significant, decrease in FSU ROM in studies with follow-up longer than 6 years could be multifactorial, such as degeneration and age. 65 Whether the preservation of FSU ROM in the intermediate-term can transform into the benefit of preventing ASDisease in the long run remains unknown.
Our study, to our knowledge, is also the first to meta-analyze biomechanics of the cervical spine before and after CTDR. In comparison with our pre-operative results, healthy individuals have higher segmental and cervical ROM 66,67 but similar Cobb angles. 68 Moreover, the FSU ROM in healthy individuals with degenerative spine changes and spinal cord compression is two times higher than the pooled pre-operative mean of our study. 69 These results reflect the fact that the spine biomechanics of patients who were about to undergo CTDR is significantly dysfunctional compared with that of healthy individuals. Although CTDR, based on our results, successfully preserved FSU ROM for 5 years, the preoperative biomechanics is impaired in relation to that in healthy individuals. Hence, it raises the question of whether the aim of CTDR is to preserve preoperative biomechanics of the spine or reverse it to the values in healthy individuals.
A number of limitations are worth considering when interpreting the results of our study. First, the included studies are heterogeneous with a mixture of different lengths of follow-up, prostheses implanted, and operated spinal levels. We tried to account for the heterogeneity by conducting subgroup analyses. Second, even though the overall number of included studies is moderate, the number of studies in each subgroup is small and did not permit the analyses of some contributing factors. Third, there is observer bias in diagnosing and grading HO in the included studies. Although most studies used experienced radiologists and neurosurgeons to diagnose HO, blinding of observers was lacking. Fourth, there were a number of studies that had data on biomechanical factors but expressed the rate of HO in number of patients. Inclusion of these studies could potentially provide a more accurate estimate, with narrower CIs than in the current data. Finally, most of our included studies are observational studies. A synthesis of RCTs will provide a more unbiased estimate.
Conclusion
In conclusion, this meta-analysis provides information on various biomechanical factors of the cervical spine before and after CTDR. Patients who opt for CTDR clearly have significantly different cervical biomechanics from healthy individuals or even from those with cervical degeneration. However, there is no association of HO or ROM-limiting HO with the changes in cervical biomechanics. This gives insight into the pathophysiology of HO formation after CTDR.
Supplemental Material
Supplemental Material, Forest_plots_baseline_biomechanics - The Changes in Cervical Biomechanics After CTDR and Its Association With Heterotopic Ossification: A Systematic Review and Meta-analysis
Supplemental Material, Forest_plots_baseline_biomechanics for The Changes in Cervical Biomechanics After CTDR and Its Association With Heterotopic Ossification: A Systematic Review and Meta-analysis by Nicholas Hui, Kevin Phan, Mei-Yi Lee, Jack Kerferd, Telvinderjit Singh and Ralph J. Mobbs in Global Spine Journal
Supplemental Material
Supplemental Material, Forest_plots_biomechanics_followup - The Changes in Cervical Biomechanics After CTDR and Its Association With Heterotopic Ossification: A Systematic Review and Meta-analysis
Supplemental Material, Forest_plots_biomechanics_followup for The Changes in Cervical Biomechanics After CTDR and Its Association With Heterotopic Ossification: A Systematic Review and Meta-analysis by Nicholas Hui, Kevin Phan, Mei-Yi Lee, Jack Kerferd, Telvinderjit Singh and Ralph J. Mobbs in Global Spine Journal
Supplemental Material
Supplemental Material, Forest_plots_differences_in_biomechanics - The Changes in Cervical Biomechanics After CTDR and Its Association With Heterotopic Ossification: A Systematic Review and Meta-analysis
Supplemental Material, Forest_plots_differences_in_biomechanics for The Changes in Cervical Biomechanics After CTDR and Its Association With Heterotopic Ossification: A Systematic Review and Meta-analysis by Nicholas Hui, Kevin Phan, Mei-Yi Lee, Jack Kerferd, Telvinderjit Singh and Ralph J. Mobbs in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material is available online with this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.