
Abstract
Femoral neck fractures are one of the most common fractures in the elderly population. Due to frequent complications of the fixation of these fractures, patients are more and more often eligible for hip replacement surgery. One of the most frequently mentioned postoperative complication is the formation of heterotopic ossification. This case report describes as a 70-year-old male patient that presented with an old hip fracture accompanied by a mild craniocerebral trauma. The patient underwent total cementless hip arthroplasty followed by rehabilitation. At 8 months after surgery, the patient was diagnosed with Brooker IV° heterotopic ossification in the area of the operated hip joint. Due to the persistent pain and complete loss of mobility in the operated joint, computed tomography imaging was performed and the patient was recommended for a revision surgery. The procedure was performed 14 months after the original surgical treatment, resulting in a significant improvement in the range of motion and reduction of pain.
Introduction
Hip arthroplasty is currently one of the most frequently performed elective surgeries in the world.1,2 The main indication for hip arthroplasty is progressive osteoarthritis of the hip joint. Other indications also include non-fused hip fractures, which are very common in the elderly and are among the ten most common causes of disability in this population. 3 Despite the very good results of hip arthroplasty, the complications should not be forgotten.4,5 One of the complications is heterotopic ossification, which according to the latest meta-analysis reported in 2015 may affect up 30% of hip replacements. 6 The definition of heterotopic ossification is the uncontrolled formation of ossification foci within soft tissues. Heterotopic ossification can take many forms. In extreme cases, it leads to the involvement of large areas of soft tissue, osteochondrosis or stiffening of the joints. The aetiology of the disease is multifactorial. 7 The most common causes include previous musculoskeletal injuries (including perioperative injuries), spinal cord injuries and craniocerebral injuries, especially those resulting in long immobilization of the patient, such as coma, paresis or paralysis. 8 Among the factors reducing the risk of heterotopic ossification after surgical treatment of hip joints, the literature emphasizes the advantage of cementless arthroplasty over cemented prostheses and the treatment of hip fractures over elective procedures. Despite the relatively frequent occurrence of ossification, there are many ways to treat cases complicated by dysfunction of the operated joint. 9 According to the literature, the use of prophylaxis of heterotopic ossification does not fully protect against their occurrence. 10
The case report describes a patient that developed massive heterotopic ossification after treatment of an old femoral neck fracture with cementless arthroplasty despite a lack of risk factors.
Case report
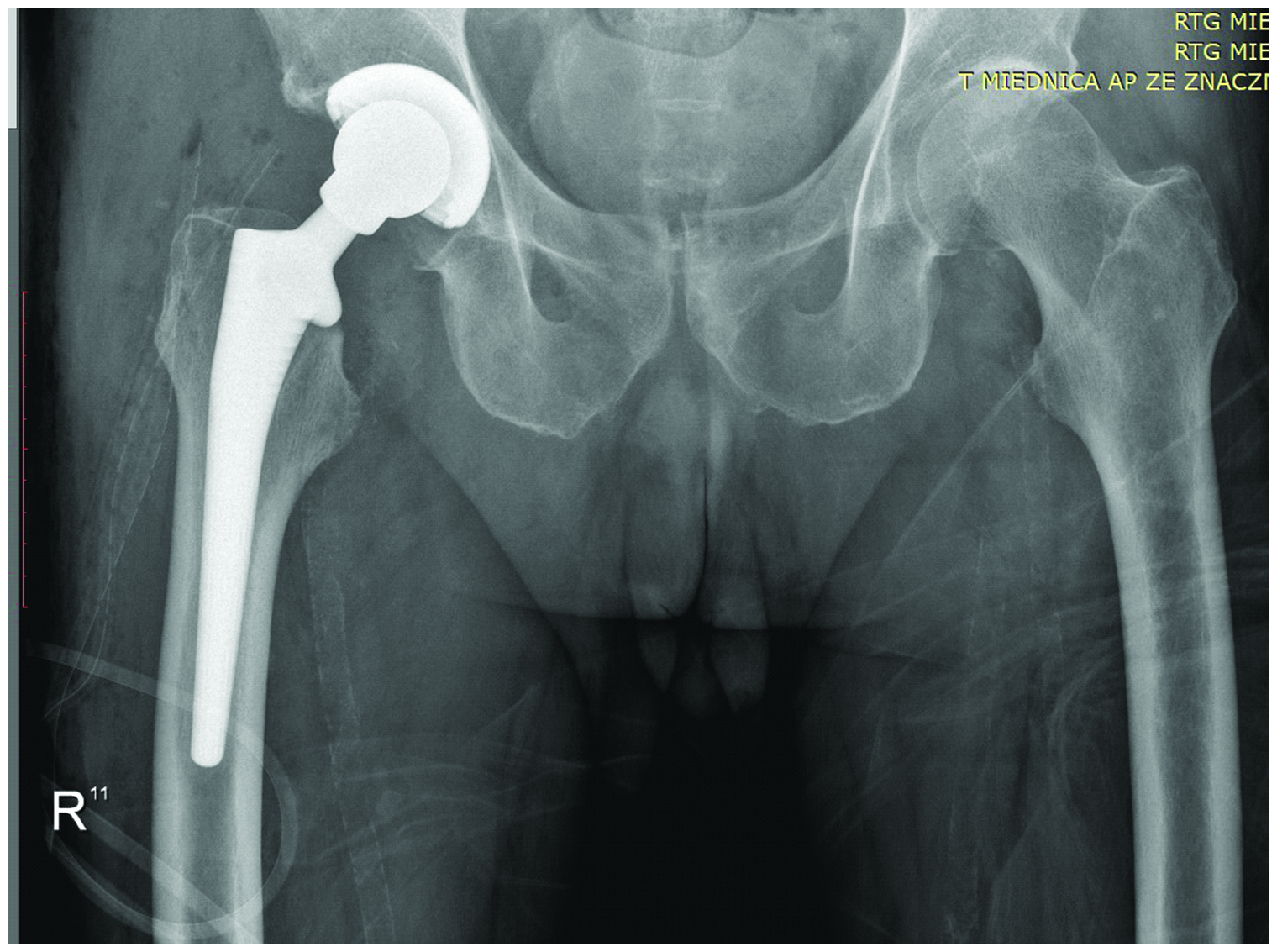
In July 2018, a 70-year-old male patient was beaten and suffered injuries to the right lower limb and a superficial head injury, during which there was no loss of consciousness. After the injury, there were no signs of damage to the central nervous system. After the incident, the patient was medically treated in the Accident and Emergency Department, City Hospital, Siemianowice Śląskie, Poland, where, after a computed tomography (CT) examination of the head, a contusion of the head was diagnosed and, additionally, a contusion of the right knee joint. After 2 weeks, due to the persistence of pain in the lower right limb, especially in the area of the hip and knee joint, and the inability to put weight on the limb, the patient was examined by a physician in the Department of Adult Orthopaedics, District Hospital of Orthopaedics and Trauma Surgery, Piekary Śląskie, Poland. A physical examination revealed painfully limited mobility of the right hip joint with a visible bloody streak during pigmentation changes and resorption in the area of the hip and right thigh. An anteroposterior X-ray of the pelvis with the hip joints revealed an old fracture of the neck of the right femur (Figure 1).

An anteroposterior X-ray of the pelvis with the hip joints of a 70-year-old male patient that presented with injuries to the right lower limb and a superficial head injury without loss of consciousness shows an old fracture of the neck of the right femur.
The patient qualified for surgery for which informed and written consent was given. The procedure was performed 15 days after the injury. Due to the good quality of bone tissue and the accompanying degenerative changes, total cementless arthroplasty of the hip joint was undertaken using the anterolateral approach (equipment used: J&J Pinnacle 52 mm cup, Marathon polyethylene 32/52 mm insert, J&J Corail No. 12 stem, 32 mm + 13 metal head) (Figure 2).
An anteroposterior X-ray of the pelvis with the hip joints of a 70-year-old male patient that presented with injuries to the right lower limb and a superficial head injury without loss of consciousness shows the status after total cementless right hip arthroplasty.
Early rehabilitation on the ward was implemented after surgery. The patient received 100 mg ketoprofen orally every 12 h for 8 days and 400 mg ibuprofen orally every 8 h for 8 days. The patient performed the prescribed exercises (breathing, circulatory, isometric) and learned to walk on crutches. On day 7 after the surgery, the patient was in good condition so he was transferred to the Department of Motor Rehabilitation, District Hospital of Orthopaedics and Trauma Surgery, Piekary Śląskie, Poland for further rehabilitation treatment. In the Department of Motor Rehabilitation, the instructions from the Department of Adult Orthopaedics’ discharge card regarding the pharmacological prophylaxis of extraskeletal ossification (ibuprofen) was not continued. During his stay on the rehabilitation ward, the patient underwent rehabilitation treatment, which included passive, active and isometric exercises and assisted exercises. The patient was discharged from the Department of Motor Rehabilitation after 14 days. Four weeks after discharge from the hospital, the patient presented at the Department of Adult Orthopaedics, District Hospital of Orthopaedics and Trauma Surgery, Piekary Śląskie, Poland for a scheduled appointment, where he did not report any symptoms of the operated hip joint and showed no signs of a previous head injury. The patient did not come to the next scheduled appointment 8 weeks after the surgery for unknown reasons. After 8 months, the patient reported for a medical appointment at the Trauma and Orthopaedic Clinic, Department of Adult Orthopaedics, District Hospital of Orthopaedics and Trauma Surgery, Piekary Śląskie, Poland due to a limp and significant limitation in the range of motion in the operated joint despite rehabilitation. An X-ray examination of the pelvis with the hip was performed, which revealed the presence of massive heterotopic ossification (IV° according to Brooker) (Figure 3). An angio-CT examination of the pelvis with three-dimensional imaging was performed in order to accurately assess the morphology of the ossifications and to assess the course of the neurovascular bundle and their anatomical relations (Figure 4).

An anteroposterior X-ray of the pelvis with the hip joints (A) and an axial X-ray of the right hip joint (B) of a 70-year-old male patient that presented with injuries to the right lower limb and a superficial head injury without loss of consciousness show the status after total cementless right hip arthroplasty with a visible massive IV° heterotopic ossification according to Brooker.
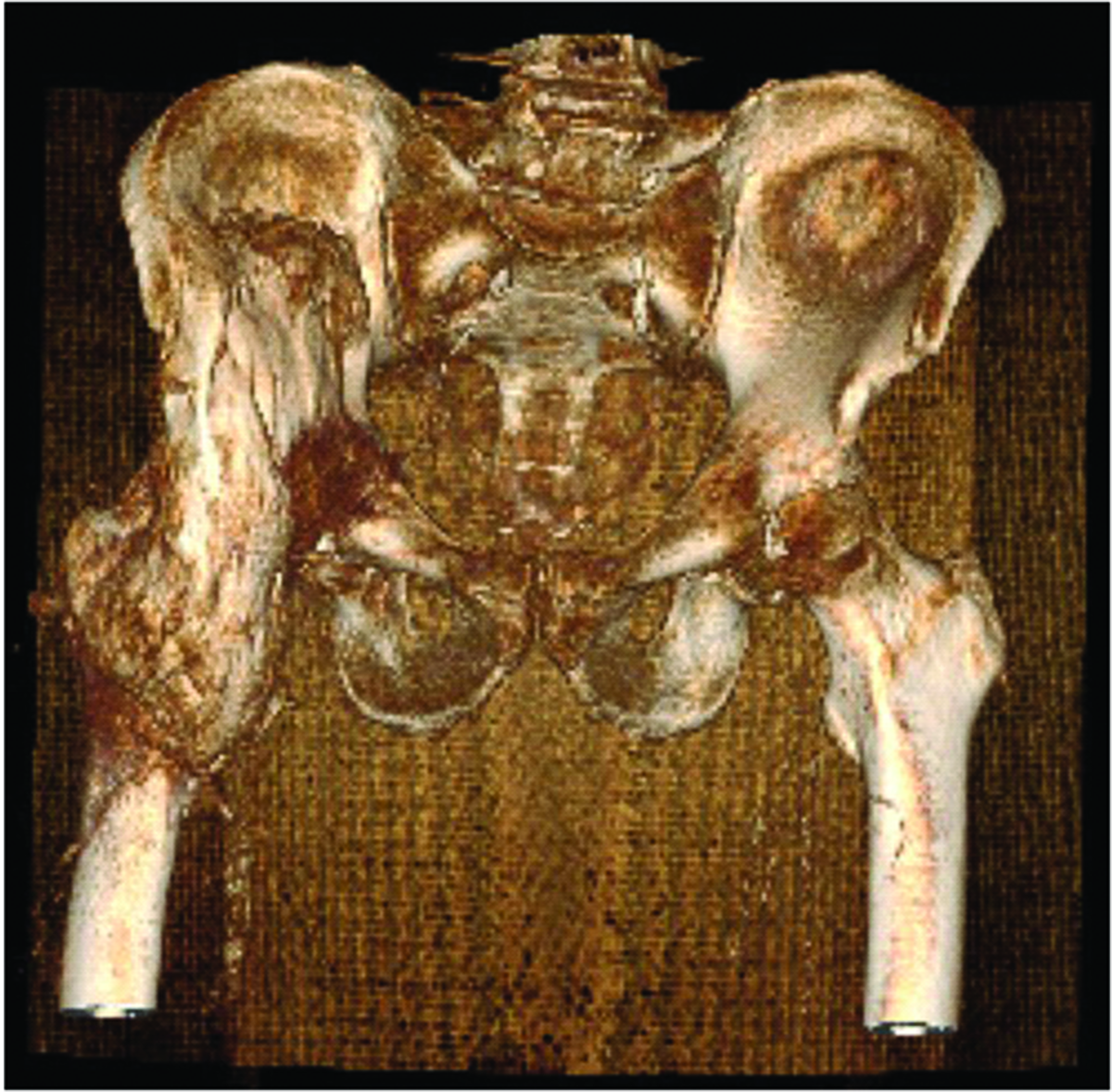
An angio-computed tomography examination of the pelvis with the hip joints of a 70-year-old male patient that presented with injuries to the right lower limb and a superficial head injury without loss of consciousness shows a visible massive IV° heterotopic ossification according to Brooker.
After the analysis of the CT imaging and correlation with the clinical picture, the patient was scheduled to undergo a surgical ossification resection. Before the planned surgery, the patient was referred for a consultation to the Department of Radiotherapy, National Research Institute of Oncology, Gliwice, Poland, where he was considered eligible for a one-time preoperative radiotherapy of the ossification of the right hip joint with 6XMV photons at a dose of 7 Gy. In October 2019, 1 day after the local radiotherapy, the patient underwent revision surgery of the right hip with surgical removal of a massive heterotopic ossification of the right hip joint (Figure 5).

An anteroposterior X-ray of the pelvis with the hip joints of a 70-year-old male patient that presented with injuries to the right lower limb and a superficial head injury without loss of consciousness shows the status after resection of the massive ossifications and revision surgery.
After 5 days, the patient was discharged from hospital in a very good general and local condition with the recommendation to continue further rehabilitation. The patient was rehabilitated initially on an outpatient basis; and 2 months after the revision surgery, as part of the Department of Motor Rehabilitation, District Hospital of Orthopaedics and Trauma Surgery, Piekary Śląskie, Poland. During the follow-up at 6, 12 and 18 months after the revision surgery, no recurrence of ossification and no pain in the operated hip joint were observed. The patient was capable of functioning independently. The reporting of this case conforms with the CARE guidelines. 11
Discussion
Femoral neck fractures are one of the most common injuries among the elderly population and their frequency, due to the aging population, will gradually increase, according to various estimates.12,13 There are several methods of surgical treatment of a femoral neck fracture and when the final treatment decision is made the following parameters should be taken into account: patient's age, activity level, bone tissue quality, additional diseases, type of fracture according to Garden and Pauwels classification as well as the related risk of complications.13,14
This current case report describes an independent, fit and active person, hence the decision to implant a cementless total prosthesis, which is recommended and more and more often used in such patients, giving the chance of a better functional outcome.15–17 Additionally, there are reports showing a higher rate of complications in the case of arthroplasty after unsuccessful fixation of hip fracture in relation to the primary treatment of the injury with arthroplasty. 18 For the above reasons, no attempt was made to fix the fracture and a decision to perform cementless hip arthroplasty was made.
Despite the beneficial results of the surgical treatment of diseases of the hip joints with the use of arthroplasty, possible complications should not be forgotten, among which heterotopic ossification is one of the most common. 6 They can take various forms, from small bone islets to massive ossification and bone bridges leading to limitation of joint mobility. A commonly used scale for assessing the extent of ossification of the hip joint area is the four-grade Brooker scale and many authors point out the clinical significance of grade III and IV ossifications. 19
The aetiopathogenesis of the development of heterotopic ossification is not clear. 7 Heterotopic ossification can be categorized as traumatic, neurogenic or genetic. The current case was considered to be either traumatic or both traumatic and neurogenic. Craniocerebral injuries, soft tissue injuries, burns and previous surgical procedures may be a factor causing the development of ossification.20,21 Complex cellular processes as well as tissue mediators and factors, such as insulin-like growth factor, interleukin (IL)-6, IL-10, monocyte chemotactic factor, protein induced by interferon 10 or macrophage inflammatory protein 1α, are important for the development of heterotopic ossification. 22 It has also been shown that local hypoxia secondary to tissue damage is a potent factor contributing to heterotopic ossification at the molecular level. 23 Hypoxia promotes the stability of the hypoxia-induced factor regulating gene expression, e.g. bone morphogenetic proteins, vascular endothelial growth factor or neuropilin-1, associated with bone formation. 23 However, despite numerous studies, the significance or role of these substances and processes in the prevention and prophylaxis of heterotopic ossification has not been clearly established. 9 All of these cellular mechanisms are important since the cell differentiation in the current case started 14 days prior to operative treatment favouring heterotopic ossification.
There are several factors predisposing to the development of heterotopic ossification. 6 The main factors are male sex, history of ossification, use of cemented hip prostheses and dual-mobility bearings. 6 Also, surgery for osteoarthritis is associated with a higher incidence of ossification than procedures for fractures of the proximal femur.24,25 In this current patient, apart from their male sex, there were no other risk factors. However, the fact that the procedure was performed on the 15th day after the injury should be considered a disadvantage. There are reports of an increase in the risk of ossification with the passage of time from the injury to the operation. 26 Nevertheless, we had no influence on this parameter as the patient was admitted to our hospital on the 14th day after the injury, and additionally, it was not listed among the high-risk factors. 9
The main methods of preventing the occurrence of heterotopic ossification include the use of oral pharmacotherapy, radiotherapy and physical rehabilitation. For example, pharmacological prophylaxis mainly involves nonsteroidal anti-inflammatory drugs (NSAIDs), which act both selectively and non-selectively. Numerous studies have shown their effectiveness in reducing ossification.27,28 Considering the possible side-effects of NSAIDs, some authors recommend their reasonable use and the need for their use to be dependent upon the presence of risk factors. 29 Radiotherapy is also widely described as a prophylactic method, both as preoperative and postoperative therapy, with good efficacy in reducing the risk of ossification in various dose ranges. 30 The last factor positively influencing the formation of ossification is the early mobilization of the patient, maintaining the mobility of the operated area and rehabilitation.31,32
In this current patient, despite the presence of only a few, non-modifiable risk factors (male sex, delayed surgical treatment) and an ambiguous position regarding the use of prophylaxis, the decision to implement pharmacological prophylaxis and rehabilitation was made. During the patient’s stay in the Department of Adult Orthopaedics, the patient received NSAIDs in the immediate perioperative period, which were ordered for further use after discharge and transfer to the Department of Motor Rehabilitation. However, for unknown reasons, this prophylaxis was not continued. Despite the lack of the main risk factors for the occurrence of heterotopic ossification and the short-term use of oral medications, as well as rehabilitation treatment, the patient developed massive heterotopic ossification in the area of the operated hip joint. Due to the symptomatic nature of the lesions, the patient qualified for surgery. The maturity of heterotopic ossifications is one of the elements taken into account during the presurgical planning. 33 The delayed removal of heterotopic ossification until after it has reached maturity reduces the risk of bleeding complications and the risk of recurrence. 33 On the other hand, delaying the operation for too long may lead to joint ankylosis. 33 In addition, there is no clear indication of the time when the ossification reaches maturity. In our opinion, waiting too long could be detrimental to the prognosis in terms of improvement after surgery and could further aggravate the patient's disability resulting from persistent pain and limited mobility of the joint. In this current patient, the ossification resection and the release of the affected joint were performed 14 months after the initial surgery, without ordering additional tests to confirm the maturity and lack of metabolic activity of the ossicles.26,27
As one of the main risk factors for the occurrence of heterotopic ossification is their formation after previous operations it was decided to introduce preoperative radiotherapy as a preventive measure. In our opinion, radiotherapy in the preoperative period is easier for the patient than transporting him/her in the first days after the surgery. After consultation with the Department of Radiotherapy, the patient underwent a single local radiotherapy with 6XMV photons at a dose of 7 Gy with good tolerance. The next day after radiotherapy, the osseous resection was performed, followed by rehabilitation in order to maintain the joint efficiency. At further follow-up of up to 18 months, there was no evidence of any recurrence of ossification.
The current case shows that despite the numerous factors mentioned in the literature that increase the risk of heterotopic ossification after hip arthroplasty, their absence or elimination does not necessarily result in no heterotopic ossification. Moreover, even the use of preventive treatment does not completely eliminate the risk of heterotopic ossification. In this current patient, a history of head trauma may be considered as an additional risk factor, but it was completely asymptomatic. On the other hand, the literature emphasizes the impact of major craniocerebral injuries and spinal cord injuries, which lead to significant restrictions in the patient's mobility, paresis and paralysis. 34
Despite many studies on the phenomenon of heterotopic ossification, there remains a lot of ambiguity. It is impossible to find a specific cause of their development and thus an effective method of their prevention. The final clinical result of the presented case confirms that the gold standard for heterotopic ossification therapy is surgical resection and prophylaxis with NSAIDs.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605221095225 - Supplemental material for Are there really specific risk factors for heterotopic ossifications? A case report of ‘non-risk factor’ after total hip replacement
Supplemental material, sj-pdf-1-imr-10.1177_03000605221095225 for Are there really specific risk factors for heterotopic ossifications? A case report of ‘non-risk factor’ after total hip replacement by Tomasz Stołtny, Jarosław Pasek, Dominika Rokicka, Marta Wróbel, Michał Dobrakowski, Paweł Kamiński, Rafał Domagalski, Szymon Czech, Krzysztof Strojek and Bogdan Koczy in Journal of International Medical Research
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from funding agency in the public, commercial, or not-for-profit sectors.
Author contributions
TS – study design, data collection, data interpretation, manuscript preparation; JP – study design, data collection, data interpretation, manuscript preparation; DR – data collection, manuscript preparation, literature search; MW – data collection, literature search; MD – data interpretation, manuscript preparation; PK – data collection, data interpretation, manuscript preparation; RD – data interpretation, manuscript preparation; SC – study design, data collection, manuscript preparation; KS – study design, data collection, data interpretation; BK – study design, data collection.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.