
Abstract
Study Design.:
A retrospective multivariate analysis.
Objective.:
To analyze clinical outcomes of surgical treatment and prognostic factors of local failure after stereotactic body radiation therapy (SBRT) in patients with spinal metastatic non–small-cell lung cancer (NSCLC).
Methods.:
This study included patients with metastatic spinal cord compression (MSCC) from spinal NSCLC after radiotherapy who received massive spondylectomy for circumferential decompression of spinal cord and reconstruction of spinal stability in our center between May 2006 and February 2017. Neurological function was evaluated using the Frankel score. Overall survival (OS) was estimated by the Kaplan-Meier method. Factors with Pvalues ≤.1 were subjected to multivariate analysis for OS by proportional hazard analysis. Values of P<.05 were considered statistically significant.
Results.:
The mean age of the 55 included patients (36 male and 19 female) was 57.76 ± 8.94 (median 58, range 36-77) years, with a mean postoperative OS of 14.98 ± 14.81 (median 10.0, range 1-84) months. Neurological function was improved in 46 (83.6%) of the 55 patients after surgery. Prognostic analysis suggested that preoperative frankel score (FS) score, visceral metastasis, D-dimer (D-D) level, and neutrophil/lymphocyte ratio (NLR) were independent prognostic factors for selected patients.
Conclusions.:
Massive spondylectomy could provide circumferential decompression and improve the neurological function of patients with MSCC from spinal NSCLC after radiotherapy. A preoperative FS score of C/D, no visceral metastasis, D-D <1000 μg/L, and NLR <5 are predictors of better prognosis.
Introduction
Non–small-cell lung cancer (NSCLC) is the leading cause of cancer-related death worldwide. 1,2 More than 30% of NSCLC patients progressed to bone metastasis, with the spine predominating. 3,4 Unfortunately, the incidence of bone metastasis in NSCLC patients tends to increase because of prolonged survival of the patients receiving target therapy. 5 -7 Spinal metastasis is a significant problem in metastatic disease because it is associated with nonfunctional consequences because of spinal cord compression, resulting in decreased quality of life. 8 Therefore, effective treatment of cancer spinal metastasis is a critical clinical issue.
Radiotherapy is the most commonly used treatment in patients with spinal metastatic NSCLC for the sake of palliation and preservation of neurological function. 9,10 The incidence of local failure after radiotherapy in patients with spinal metastasis is about 5.7%. 11 Patients with local failure after radiotherapy are prone to spinal instability and neurological disorders. As a result, surgical treatment was recommended for patients with MSCC by spinal NSCLC after local failure of radiotherapy. Conventionally, separation surgery combined with postoperative radiotherapy was recommended for the treatment of patients with MSCC by spinal NSCLC. 12 However, patients with MSCC by spinal NSCLC after radiotherapy are usually unable to receive further radiotherapy because of inability to tolerate high doses of radiation. As a result, the surgical strategy for treatment of MSCC by spinal NSCLC after radiotherapy becomes a clinical dilemma.
Here, we report a series of patients who received massive spondylectomy for the treatment of MSCC after local failure of radiotherapy. Massive spondylectomy is defined as removal of all posterior elements and most of the vertebral body. The stability of the posterior column is ensured by reconstruction with pedicle screws and rods, and the anterior column, by using a titanium mesh filled with allograft bone. Bone cement is used to wrap the titanium mesh and enhance the stability of the anterior column. This study aims to analyze the effect of surgical treatment and prognostic factors of patients who suffered from MSCC by spinal NSCLC after local failure of radiotherapy, hoping that it could shed new light on the management of this challenging disease.
Methods
Study Design and Patients
A retrospective study was performed to investigate the prognostic factors in patients with radiotherapy failure and mobile spinal metastasis from NSCLC who received surgical treatment in our center between May 2006 and February 2017. The inclusion criteria were as follows: (1) patients with metastatic tumors involving the mobile spine, including the cervical, thoracic, and lumbar segments; (2) patients receiving radiotherapy on the metastatic vertebrae before surgery; (3) patients with local failure in the vertebrae after radiotherapy; (4) patients with spinal cord compression and neurological function deficits; and (5) patients whose diagnosis of NSCLC was pathologically confirmed by biopsy or surgery. The exclusion criteria were as follows: (1) patients with radiation myelopathy, (2) patients with local failure beyond the vertebrae that received radiotherapy, and (3) patients whose final pathological diagnosis was not NSCLC.
Follow-ups
The clinical and pathological data of all patients was collected from the previously maintained database in our center. The preoperative and postoperative neurological status of the patients were classified according to the Frankel score, and their general conditions were assessed using the Eastern Cooperative Oncology Group performance score (ECOG-PS). The individualized surgical strategies were decided according to WBB stage, Tokuhashi scores, and Changzheng scores for spinal metastatic NSCLC. 13,14 Progression-free survival (PFS) after stereotactic body radiation therapy (SBRT) was defined as the interval between the date of radiotherapy and the date of neurological function deterioration. Overall survival (OS) was defined as the interval between the date of the initial surgery and the date of death. Each patient was followed up on the outpatient basis at 3-month intervals until death.
Statistical Analysis
All statistical calculations were performed using PASW Statistics version 18.0. Qualitative data is described as percentages. Quantitative data is described as means and medians (range). The postoperative OS rate was estimated using the Kaplan-Meier method, and differences were analyzed using the log-rank test. Factors with P values less than .1 were subjected to multivariate analysis for OS by proportional hazard analysis. 15 P values less than .5 were considered statistically significant.
Ethical Considerations
The research was approved by the ethics committee of Changzheng hospital, and written informed consent was obtained from all patients.
Results
Characteristics of the Patients and Univariate Analysis of Prognostic Factors
The clinical characteristics of the patients are shown in Table 1. Altogether, 55 patients (36 male and 19 female) met the selection criteria. The mean age was 57.76 ± 8.94 (median 58, range 36-77) years. All the patients previously received 7 to 11 cycles of radiotherapy before local failure at a mean dose of 19 to 45 Gy. The mean PFS after radiotherapy was 20.11 ± 20.36 (median 17.0, range 0-107) months. A total of 23 patients suffered from vertebrae compression fracture (VCF); 19 patients suffered from tumor enlargement, and 13 patients suffered from both VCF and tumor enlargement. All the patients received massive spondylectomy and were followed up to death. The OS time was 14.98 ± 14.81 (median 10.0, range 1-84) months after surgery. No patient was found to have local recurrence after surgery in the follow-up period.
Patients’ Characteristics and Univariate Analysis of Prognosis Factors.
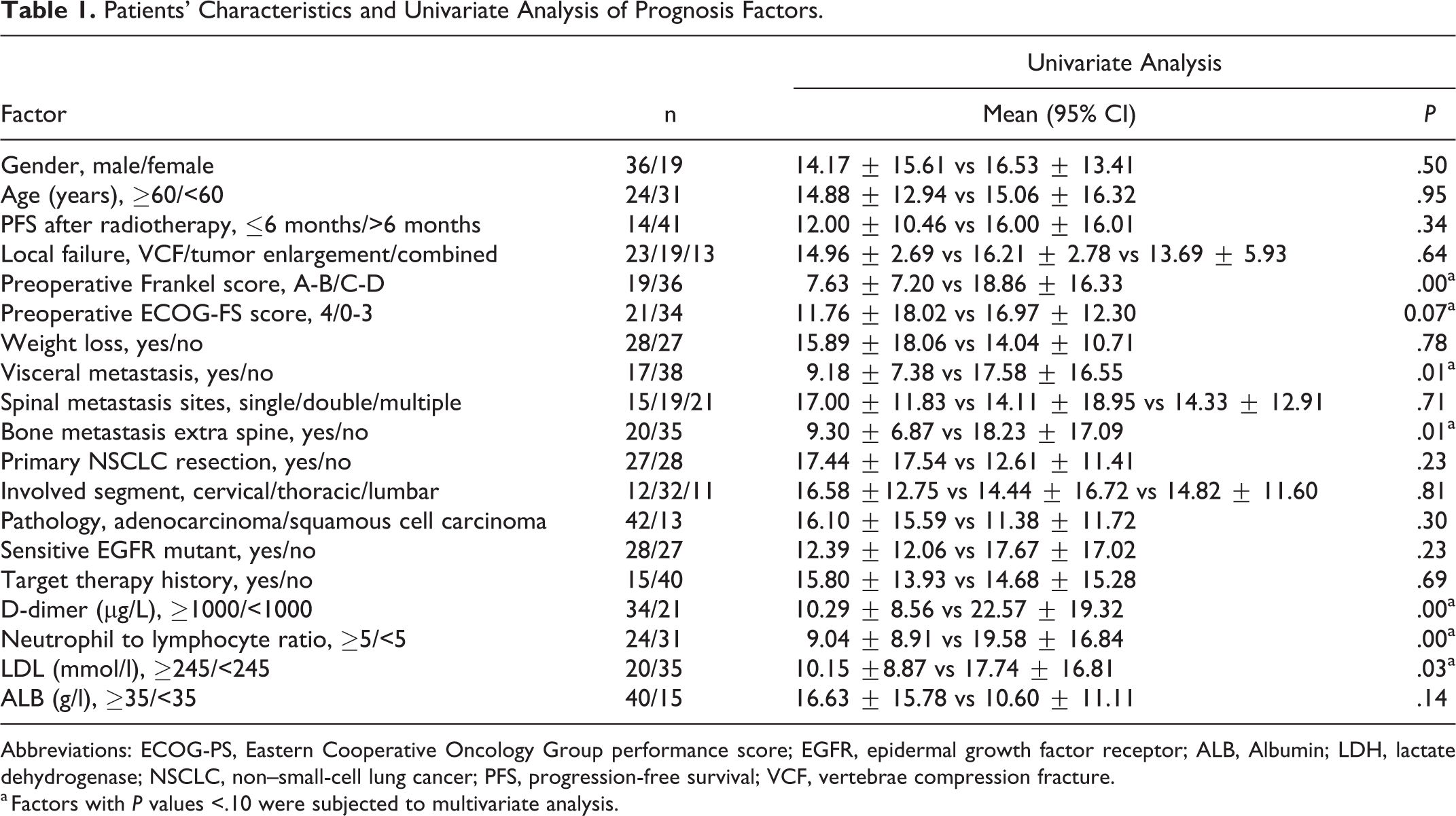
Abbreviations: ECOG-PS, Eastern Cooperative Oncology Group performance score; EGFR, epidermal growth factor receptor; ALB, Albumin; LDH, lactate dehydrogenase; NSCLC, non–small-cell lung cancer; PFS, progression-free survival; VCF, vertebrae compression fracture.
a Factors with P values <.10 were subjected to multivariate analysis.
Of the 55 included patients, 19 with a preoperative Frankel score of A/B survived 7.63 ± 7.20 months, and the other 36 with a preoperative Frankel score of C/D survived 18.86 ± 16.33 months. The OS of patients with a Frankel score of A/B was significantly shorter than that of patients with a Frankel score of C/D (P = .00). Of the 55 patients, 21 had a preoperative ECOG-PS score of 4, and the other 34 patients had a preoperative ECOG-PS score of 0 to 3. The OS of patients with an ECOG-PS score of 4 was 11.76 ± 18.02 months as compared with 16.97 ± 12.30 months in patients with scores of 0 to 3, showing a significant difference between the 2 groups of patients (P = .07). There were 17 patients with visceral metastasis, and 20 patients with extraspinal bone metastasis. The OS of patients with visceral metastasis was 9.18 ± 7.38 months, which was significantly shorter than 17.58 ± 16.55 months in patients without visceral metastasis (P = .01). Patients with extra-spinal bone metastasis had a mean OS of 9.30 ± 6.87 months, which was significantly shorter than 18.23 ± 17.09 months in patients without extraspinal metastasis (P = .01).
Of the 55 patients, 34 patients had a D-dimer (D-D) value >1000, 24 patients had a neutrophil/lymphocyte ratio (NLR) >5, and 20 patients had a lactate dehydrogenase (LDH) value >245 mmol/L. The OS of patients with D-D >1000 was 10.29 ± 8.56 months, which was significantly shorter than 22.57 ± 19.32 in patients with D-D <1000. The OS of patients with NLR >5 was 9.04 ± 8.91 months, which was significantly shorter than 19.58 ± 16.84 months in patients with NLR <5 (P = .00). The OS of patients with LDH >245 was 10.15 ±8.87 months, which was significantly shorter than 17.74 ± 16.81 months in patients with LDH <245.
Of the 55 patients, 28 reported weight loss, and the other 27 patients did not; OS was 15.89 ± 18.06 and 14.04 ± 10.71 months, respectively (P = .78). A total of 15 patients had metastasis at a single spinal site, 19 patients had 2 spinal metastatic sites, and 21 patients had multiple metastatic lesions; OS was 17.00 ± 11.83, 14.11 ± 18.95, and 14.33 ± 12.91 months, respectively (P = .71). In all, 27 patients received primary NSCLC resection, and the other 28 patients did not; OS was 17.44 ± 17.54 and 12.61 ± 11.41 months, respectively (P = .23). Metastasis involved the cervical vertebra in 12 patients, thoracic vertebra in 32 patients, and lumbar vertebra in 11 patients; OS was 16.58 ±12.75, 14.44 ± 16.72, and 14.82 ± 11.60 months, respectively (P = .81). A total of 42 patients had adenocarcinoma, and 13 patients had squamous cell carcinoma; OS was 16.10 ± 15.59 and 11.38 ± 11.72 months, respectively (P = .30).
Multivariate Analysis of Prognostic Factors
Univariate analysis demonstrated that the potential prognostic factors were preoperative Frankel score, preoperative ECOG-PS score, visceral metastasis, extraspinal bone metastasis, D-D, NLR, and LDH. They were submitted to the multivariate Cox regression model to identify the independent prognosis factors for patients with local failure after radiotherapy. The risk of death in patients with preoperative Frankel score of A or B was significantly increased in patients with C or D (P = .01), with a hazard ratio (HR) of 3.19 (95% CI = 1.28-7.94) for OS. Patients with visceral metastasis were significantly associated with poorer OS than those without visceral metastasis (P = .03), with a HR of 2.13 (95% CI = 1.09-4.19) for OS. The Kaplan-Meier curves of OS for preoperative FS score and visceral metastasis are shown in Figure 1. D-D >1000 significantly increased the OS as compared with D-D <1000 (P = .03), with a HR of 2.12 (95% CI = 1.08-4.17). The risk of death was significantly elevated in patients with NLR >5 as compared with that in patients with NLR <5 (P = .03), with a HR of 1.98 (95% CI = 1.08-3.62). The HR for preoperative ECOG-PS score, extraspinal bone metastasis, and LDH were 0.61 (95% CI = 0.23-1.60), 1.80 (95% CI = 0.89-3.62), and 1.00 (95% CI = 0.52-1.90), respectively, showing no significant difference within each factor (P = .31; P = .10; and P = 1.00). The Kaplan-Meier curves of OS for D-D and NLR are shown in Figure 2. Collectively, the survival analysis suggested that preoperative Frankel score, visceral metastasis, D-D, and NLR were independent prognostic factors for patients with local failure after radiotherapy in the mobile spine. Details are shown in Table 2.
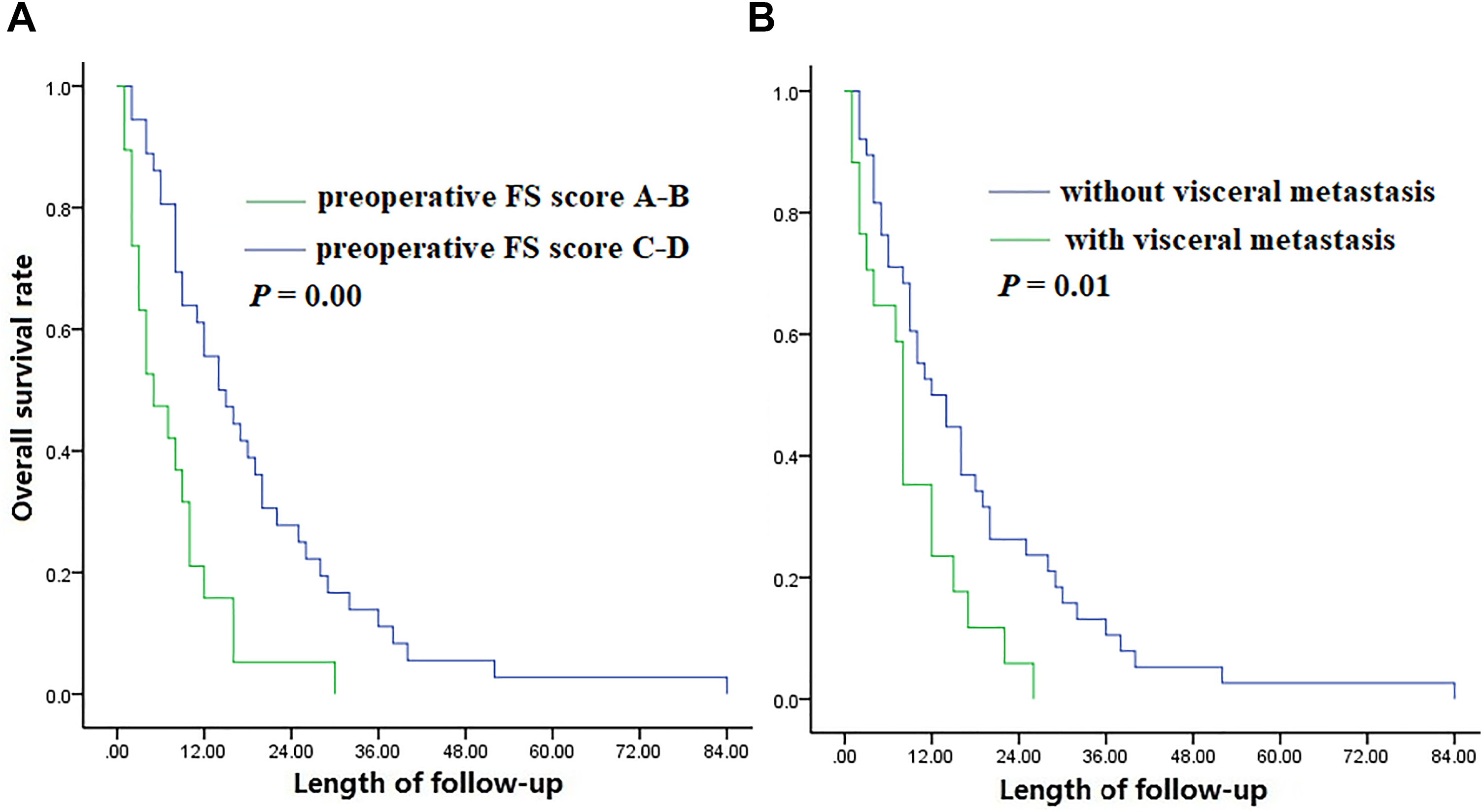
A. Kaplan-Meier curves for overall survival between patients with preoperative FS score A-B and C-D. B. Kaplan-Meier curves for overall survival between patients with visceral metastasis and without visceral metastasis.
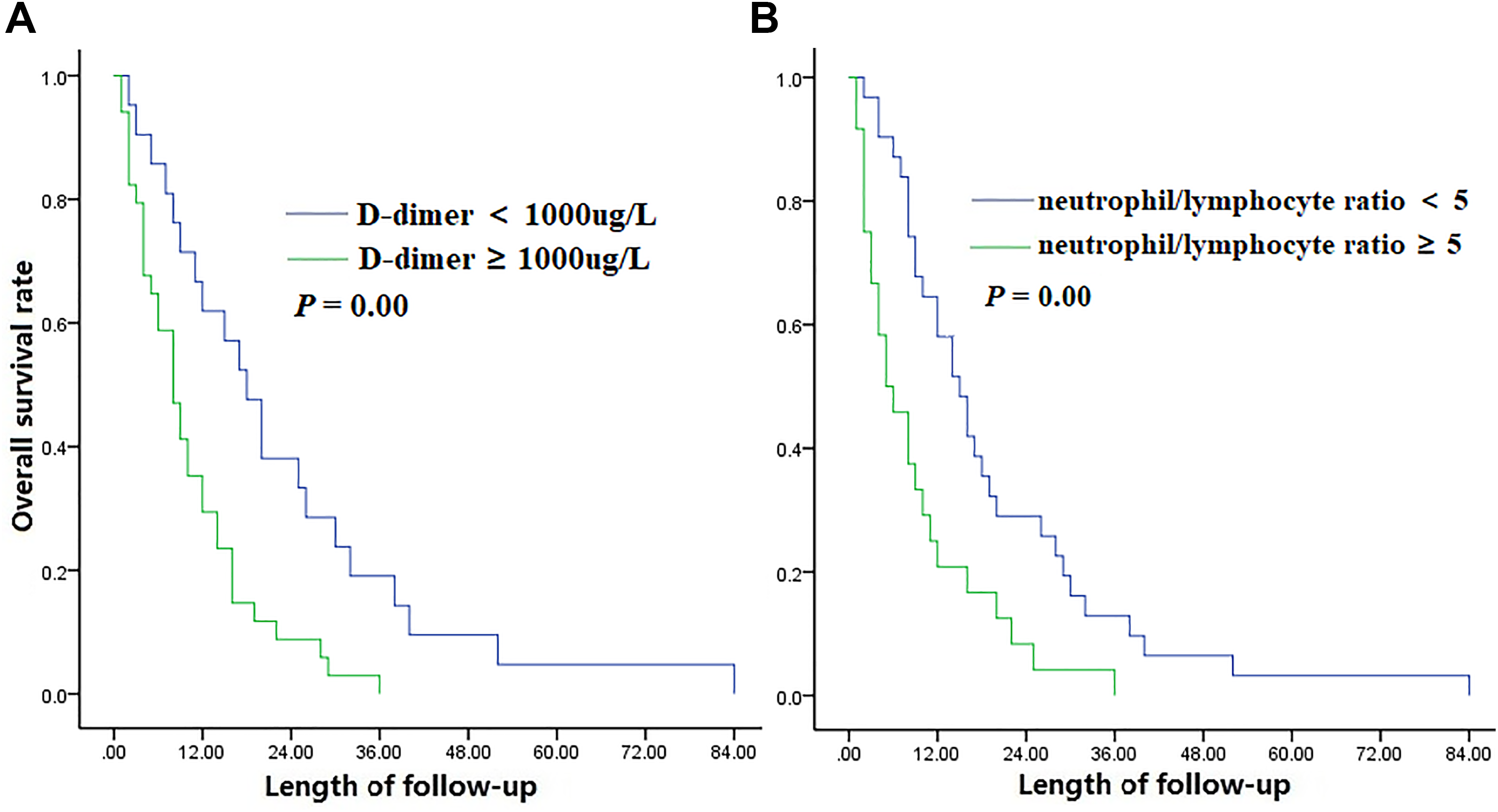
A. Kaplan-Meier curves for overall survival between patients with D-dimer <1000 μg/L and D-dimer ≥1000 μg/L. B. Kaplan-Meier curves for overall survival between patients with neutrophil/lymphocyte ratio (NLR) <5 and NLR ≥5.
Multivariate Analysis of Prognosis Factors.
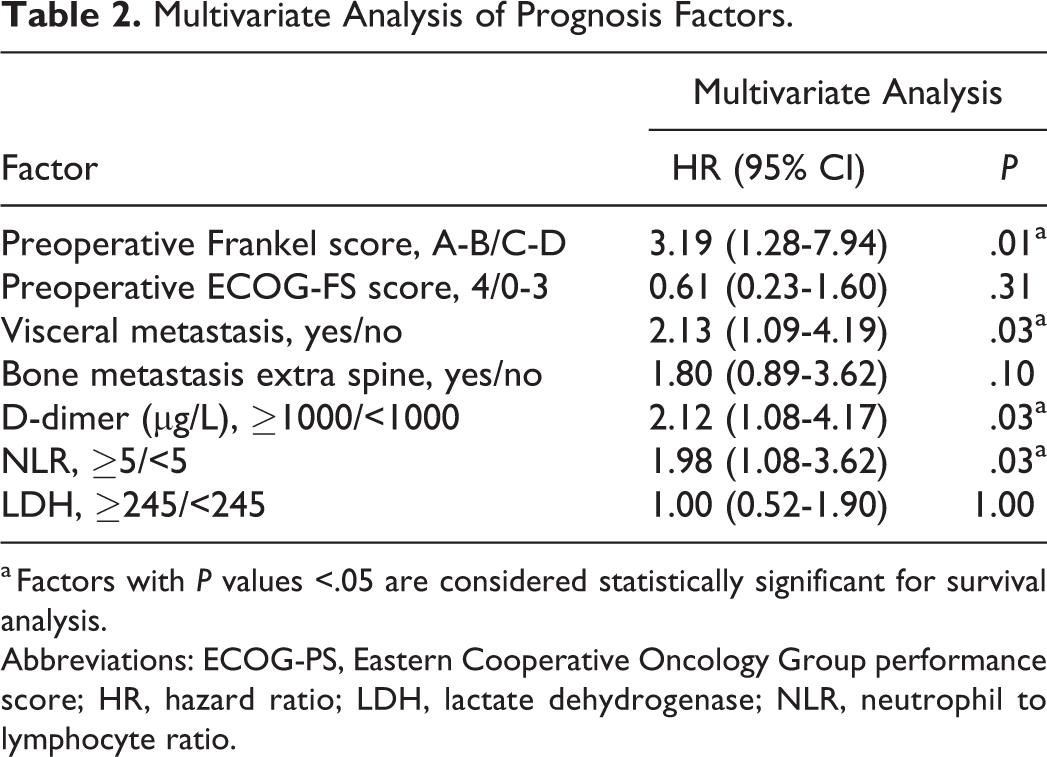
a Factors with P values <.05 are considered statistically significant for survival analysis.
Abbreviations: ECOG-PS, Eastern Cooperative Oncology Group performance score; HR, hazard ratio; LDH, lactate dehydrogenase; NLR, neutrophil to lymphocyte ratio.
Surgical Procedures and Neurological Function Conversion After Surgery
The posterior approach was applied in patients with thoracic and lumbar spinal tumors. The combined posterior-anterior approach was used in patients with cervical spinal tumors. All the patients received massive spondylectomy. We implanted pedicle screws at the superior and inferior 2 segments, respectively. The total posterior elements were removed. The vertebral body was resected mostly in order to release the spine cord adequately. The stability of the anterior column was reconstructed by a titanium mesh filled with allograft bone. Bone cement was also used to wrap the titanium mesh and enhance the stability of the anterior column.
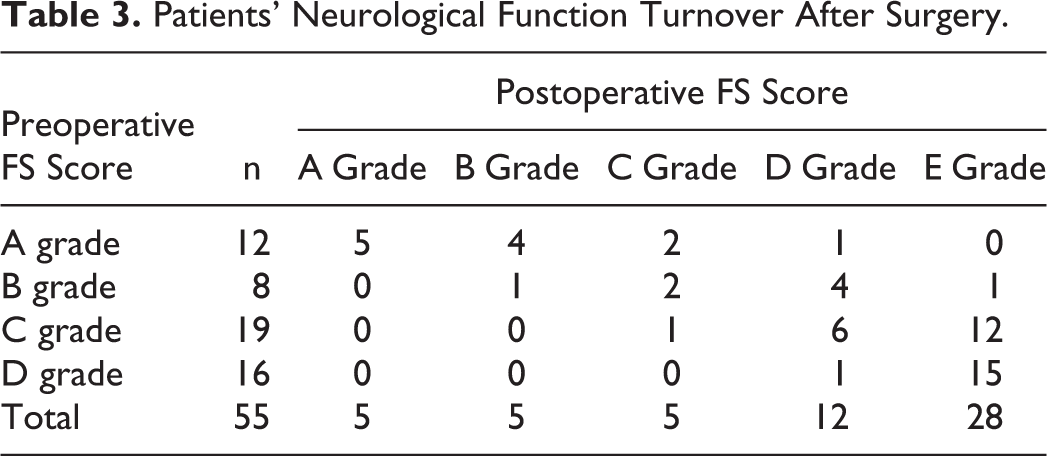
Among the 55 patients, neurological function improved in 46 (83.6%) after surgery. No postoperative deterioration of neurological function was observed in any of the patients in our series. Details about neurological function conversion after surgery are shown in Table 3. Among 12 patients with preoperative Frankel score A, neurological function was improved in 7 (58.3%) patients, including conversion to B in 4 patients, to C in 2 patients, and to D in 1 patient; among 8 patients with preoperative Frankel score B, neurological function was improved in 6 patients (75.0%), including conversion to C in 2 patients, to D in 3 patients, and to E in 1 patient; among 19 patients with preoperative Frankel score C, neurological function was improved in 6 patients, including conversion to D in 7 patients and to E in 12 patients; and among 16 patients with preoperative Frankel score D, neurological function was converted to E after surgery in 15 patients (93.8%).
Patients’ Neurological Function Turnover After Surgery.
Discussion
NSCLC is the most common type of cancer worldwide and the leading cause of cancer-related deaths. 1 About 30% to 40% of NSCLC patients eventually progressed to bone metastasis, mainly involving the spine. 16,17 Spinal metastasis is often associated to severe local pain, pathological fracture, spinal instability, neurological function deficits and even paralysis. Radiotherapy was reported to be a safe and effective treatment for spinal metastatic NSCLC because it is sensitive to radiation. 18 -20 However, local failure after radiotherapy remains a threat to some of these patients, especially in those with mobile spinal metastatic NSCLC. 11 To the best of our knowledge, few studies have reported surgical treatment of local failure after radiotherapy in patients with spinal metastatic NSCLC. In this study, we reported the effect of massive spondylectomy and prognostic factors in such patients.
Surgical treatment has been applied extensively in spinal metastasis. It was reported 21 that direct decompressive surgery combined with local radiotherapy could achieve better functional preservation compared with radiotherapy alone. It has been reported that separation surgery followed by postoperative radiotherapy were recommended for the treatment of patients with spinal metastasis. 12 However, the patients with local failure after radiotherapy are usually unable to receive further radiotherapy because of inability to tolerate high doses of radiation. As a result, separation surgery may not be a suitable strategy for the treatment of patients with local failure after radiotherapy.
We reported a series of patients who received massive spondylectomy. In this procedure, the spinal cord could be completely released because an adequate safe distance was provided by removal of total posterior elements and most of the vertebral body. In addition, spinal instability as a predominant risk factor for local failure after radiotherapy 21 could be reconstructed by surgical treatment. This procedure could provide reliable stability because the posterior and anterior columns were reconstructed simultaneously. In the current study, neurological function was improved in 83.6% of these patients after surgery, which is indication that massive spondylectomy is a viable option for local failure after radiotherapy in patients with spinal metastatic NSCLC.
The result of survival analysis suggested that a good Frankel score is an independent predictor of better prognosis. The function conversion analysis showed that patients with Frankel score C/D had better neurological function conversion than those with Frankel score A/B. The results suggested that the OS was prolonged in patients with better functional improvement after surgery, probably because good neurological function could prevent or defer the occurrence of paraplegia-related complications, such as susceptibility to infections, decubitus ulcers, or deep-vein thrombosis. 22 Also, patients with good neurological function could receive more effective systemic therapies. ECOG-PS was significant in univariate analysis but became insignificant in multivariate analysis, partly because the ECOG-PS score is mainly based on the bed-ridden duration of the patient. Therefore, there may be a bias when it is applied to patients with spinal metastasis and associated neurological function deficits. Knowing that visceral metastasis is considered an important factor affecting patient survival, it is included in the Tokuhashi, Tomita, and Bauer scoring systems as well as in the Changzheng Scale for spinal metastatic NSCLC. In this study, multiple spinal metastases were found to have no significant impact on patient survival, probably because all the included patients who received radiotherapy were only affected by single-site nerve compression and instability.
The results of all laboratory tests, including D-D, NLR, LDH, and Albumin (ALB), were analyzed in the present study. D-D and NLR were found to be independent prognostic factors for patients with local failure after SBRT in mobile spinal metastasis from NSCLC. D-D is a marker of hypercoagulation. A high D-D level is thought to be predictive of occurrence of venous thromboembolism, a frequent complication in cancer patients, and is associated with poor prognosis in patients with NSCLC. 23 For this reason, anticoagulants should be used in patients with local failure after SBRT who have high levels of D-D. The NLR is an important marker of systemic inflammation. Neutrophils, T-, and B-lymphocytes play a central role in antitumor immune responses. 24 The NLR has proven to be a prognostic factor for various types of cancer, including breast cancer, pancreatic cancer, esophageal cancer, and lung cancer. 25 -28 Some recent studies also suggested that NLR could predict the survival of patients with NSCLC who received PD-1 inhibitor therapy. 7,29,30
There are some limitations to this study. First, it was a retrospective study, although to the best of our knowledge, it is the first serial study to discuss local after radiotherapy in spinal metastatic NSCLC. In addition, the sample size is relatively small, and therefore, more studies are required to confirm the conclusion and suggestions of the present study.
Our study demonstrated that massive spondylectomy could improve the neurological function and provide stability in patients with local failure after radiotherapy in mobile spinal metastatic NSCLC. A preoperative FS score of C and D, no visceral metastasis, D-D <1000 μg/L, and NLR <5 are predictors for better prognosis.
Footnotes
Authors’ Note
The following authors contributed equally to this study: Wei Xu and Minglei Yang. This work was supported by grants from National Key Research and Development Program of China (2016YFC0902100), the National Natural Science Foundation of China (81 702 888), Shanghai Excellent Medical Talents Funding (2018YQ56), and Shanghai Youth Doctor Assistance Program (Wei Xu).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.