
Abstract
Study Design
Retrospective cohort.
Objectives
With rising cancer rates and survival, effective palliative treatments are crucial. For decades, conventional external beam RT (cEBRT) has been the standard for palliation but is dose-limited. The efficacy of postoperative radiotherapy for spinal metastases with stereotactic body radiation therapy (SBRT) in direct comparison to cEBRT remains understudied. We aim to compare clinical outcomes after treatment with cEBRT or SBRT for patients with spinal metastases.
Methods
Eligible patients included those who received palliative RT with cEBRT or SBRT between January 2017 and December 2022 at Massachusetts General Hospital. A matched cohort of 204 patients was created using propensity score matching. Reoperation, overall survival (OS), and postoperative complications were evaluated. Multivariable logistic regression was used to adjust for residual bias after propensity score matching.
Results
81 patients treated with cEBRT were matched with 123 patients treated with SBRT. Reoperation rate was 13.2%, with no significant difference between the cEBRT and SBRT groups (12.4% vs 13.8%, P = 0.76). Median OS was 15.9 months (IQR, 6.7-40.6 months). Kaplan-Meier analysis revealed no significant association between type of radiotherapy and either reoperation or OS (P = 0.40 and P = 0.56, respectively). When comparing reoperation by radiation modality, multivariable logistic regression analysis showed no significant difference.
Conclusion
We observed that SBRT does not reduce rates of reoperation or complications, nor does it improve overall survival. These findings suggest that conventional radiotherapy remains a viable postoperative treatment for spinal metastases, especially when SBRT is not available or feasible, or when cost is a significant concern.
Keywords
Introduction
Nearly all types of cancer can spread to the bone, with the spine being the most common site of metastasis. Around 30% of cancer patients develop spinal metastases. 1 With rising cancer rates and extended survival due to advanced therapies, the prevalence of spinal malignancy is expected to rise. 2
Treatment goals for metastatic spine disease are primarily palliative, focusing on pain control and preserving neurologic function using radiotherapy (RT), chemotherapy, and surgery. For decades, conventional external beam RT (cEBRT) has been the standard for palliation. 3 However, cEBRT is dose-limited due to its effects on the skin and relatively flat dose gradient, increasing the risk of radiation exposure to sensitive surrounding structures such as the spinal cord, nerve roots, bowel, and/or lung fields.
Contemporary stereotactic body RT (SBRT) may circumvent these limitations by delivering higher doses in fewer fractions (typically 1-5) to smaller, well-defined targets. 4 This may improve local control and reduce treatment-related toxicities.4,5 For spinal disease, the proximity of the spinal cord makes SBRT an attractive RT modality, achieving local control rates over 85%.6-8 SBRT also has a favorable safety profile and improves pain and quality of life when compared to conventional treatment.9-11 However, the limited availability of SBRT poses logistical challenges, making cEBRT necessary in some cases despite its potential risks, including delayed wound healing and mechanical complications with instrumentation.
To our knowledge, no previous studies directly compare SBRT to cEBRT from an orthopedic lens, focusing on surgical outcomes. Most research on SBRT centers on oncologic endpoints such as pain response, quality of life, and the optimal interval between surgery and the start of RT.10,12,13 Consequently, this study aims to investigate this gap by evaluating whether cEBRT is a viable alternative when SBRT is unavailable. We evaluated the effect of postoperative RT modality (cEBRT vs SBRT) on reoperation rate and overall survival for spinal metastasis. Secondarily, we assessed complication rates between the 2 treatment groups.
Methods
Study Design
Institutional review board approval was obtained to examine patients in our research data registry, and informed consent was waived for retrospective analysis of deidentified data. Patients were identified with International Classification of Disease 10th Revision (ICD-10) codes for secondary malignant neoplasm of bone and bone marrow (C79.5) or multiple myeloma without mention of complete remission (C90.0) and all CPT codes related to surgical procedures of the spine. A total of 2312 patients at Massachusetts General Hospital (MGH) between January 2017 and December 2022 were identified. Records were screened for the following inclusion/exclusion criteria: received surgical treatment for spinal metastasis and palliative postoperative RT.
Population
This study was a retrospective review of patients with spinal metastasis treated with both surgical resection and postoperative RT at our institution. Eligible patients included those who received palliative RT with either conventional external beam RT (cEBRT) or stereotactic body RT (SBRT). Participants with missing RT data or who received only pre-operative RT were excluded, as were patients treated with proton therapy or definitive RT for primary bone tumors (Figure 1). Sample population for retrospective analysis.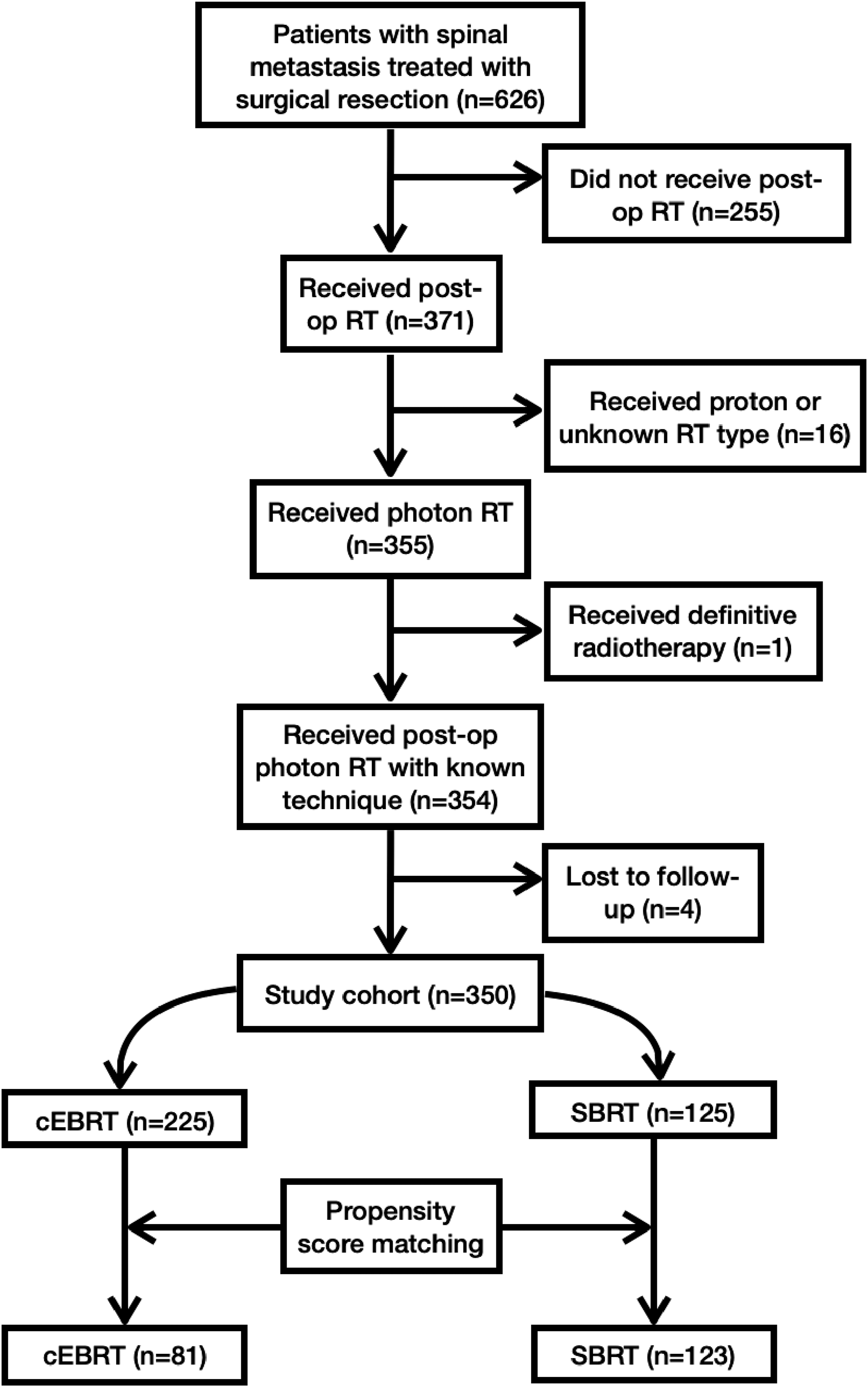
Data Extraction/Additional Explanatory Variables
In-depth manual record review was performed on demographic and clinical factors. We extracted demographic information including sex, age at surgery, race, and smoking history. Additional data on disease status and treatment were collected including primary tumor type, number of spinal metastases, other perioperative treatment, surgical site, and surgery type. Due to sample size concerns, primary tumor type was reclassified according to the revised Katagiri grading system and considered as an ordinal variable (slow growth, moderate growth, rapid growth). 14
Outcomes
The primary endpoint was reoperation, defined as surgical intervention to the same site due to tumor progression, instrumentation failure, delayed wound healing, or other complication from the index surgery. Overall survival was a secondary outcome. We also assessed short-term complications, defined as any complication occurring within 30 days of the index surgery including infection, pneumonia, pulmonary embolism, sepsis, instrumentation loosening, myocardial infarction, or unexpected ICU admission. Vital status was collected on postoperative days 30, 90, 180, 365, and 540, as well as at the time of final follow-up.
Statistical Analysis
Two groups of patients were identified: a cEBRT Group (patients treated with postoperative cEBRT), and an SBRT Group (patients treated with postoperative SBRT). Both groups received definitive surgical resection. Due to concerns of differences between treatment groups, a propensity score was created to mitigate bias from covariates. Significant variables in bivariate analysis were used in the propensity score model and included revised Katagiri score,
14
Charlson Comorbidity Index,
15
Eastern Cooperative Oncology Group (ECOG) performance status,
16
American Spinal Injury Association (ASIA) impairment scale,
17
number of spinal metastases, and smoking status, and time between surgery and the start of RT. As recommended,
18
calipers were set at 0.2 standard deviations of the logit of the propensity score. Unmatched patients were excluded, yielding a matched cohort of 204 patients with 81 patients in the cEBRT group and 123 patients in the SBRT group. The adequacy of the matching process was assessed by constructing density plots of the propensity scores before and after matching (Figure 2A and B). (A, B) Propensity score before and after propensity score matching.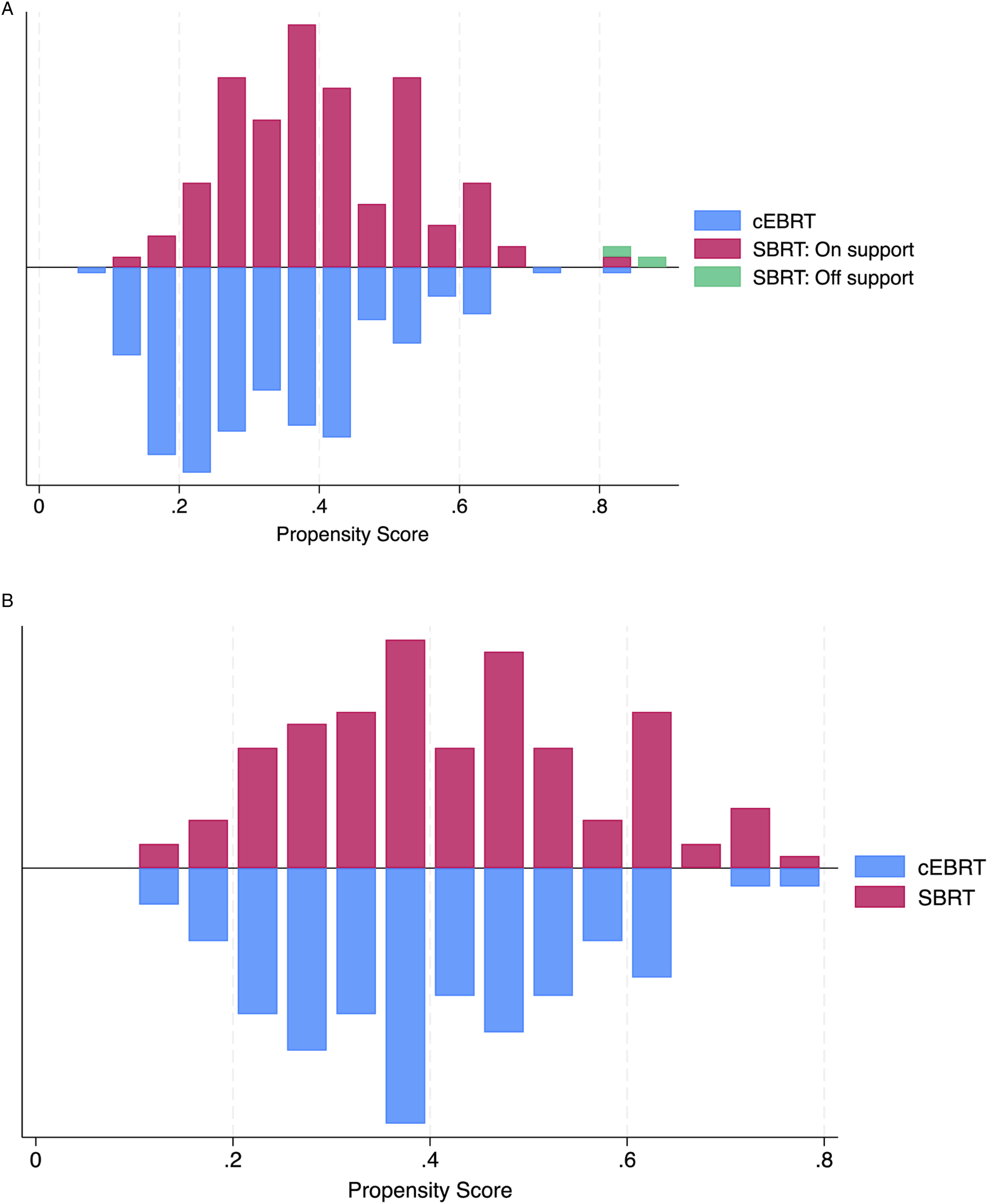
Data was analyzed from June 19, 2024, to July 24, 2024. Stata version 18.5 (StataCorp LLC, College Station, TX) statistical software was used for all analyses. P values were two-sided, and P < 0.05 was considered significant. For bivariate analysis, dichotomous and nominal variables were analyzed using the chi-squared test and the Fisher exact test when indicated. For continuous variables, Student’s t test assumptions were examined using the Shapiro-Wilk test, and data was deemed not normally distributed. Therefore, data are displayed as frequencies with percentages (%) or as medians with interquartile ranges (IRQ). Continuous variables were analyzed using Wilcoxon rank-sum test. Multivariable analysis was conducted using a logistic regression model. Factors that were considered clinically significant were selected as model covariables.
For each outcome, time to event (months) was calculated from the date of first radiation treatment to the date when the event occurred—either the date of reoperation, date of death, or date of last follow-up. Kaplan-Meier estimates of reoperation and overall survival were graphically displayed, stratified by RT technique, with outcome estimates compared using a two-sided log-rank P-value.
Results
Preoperative and Perioperative Data
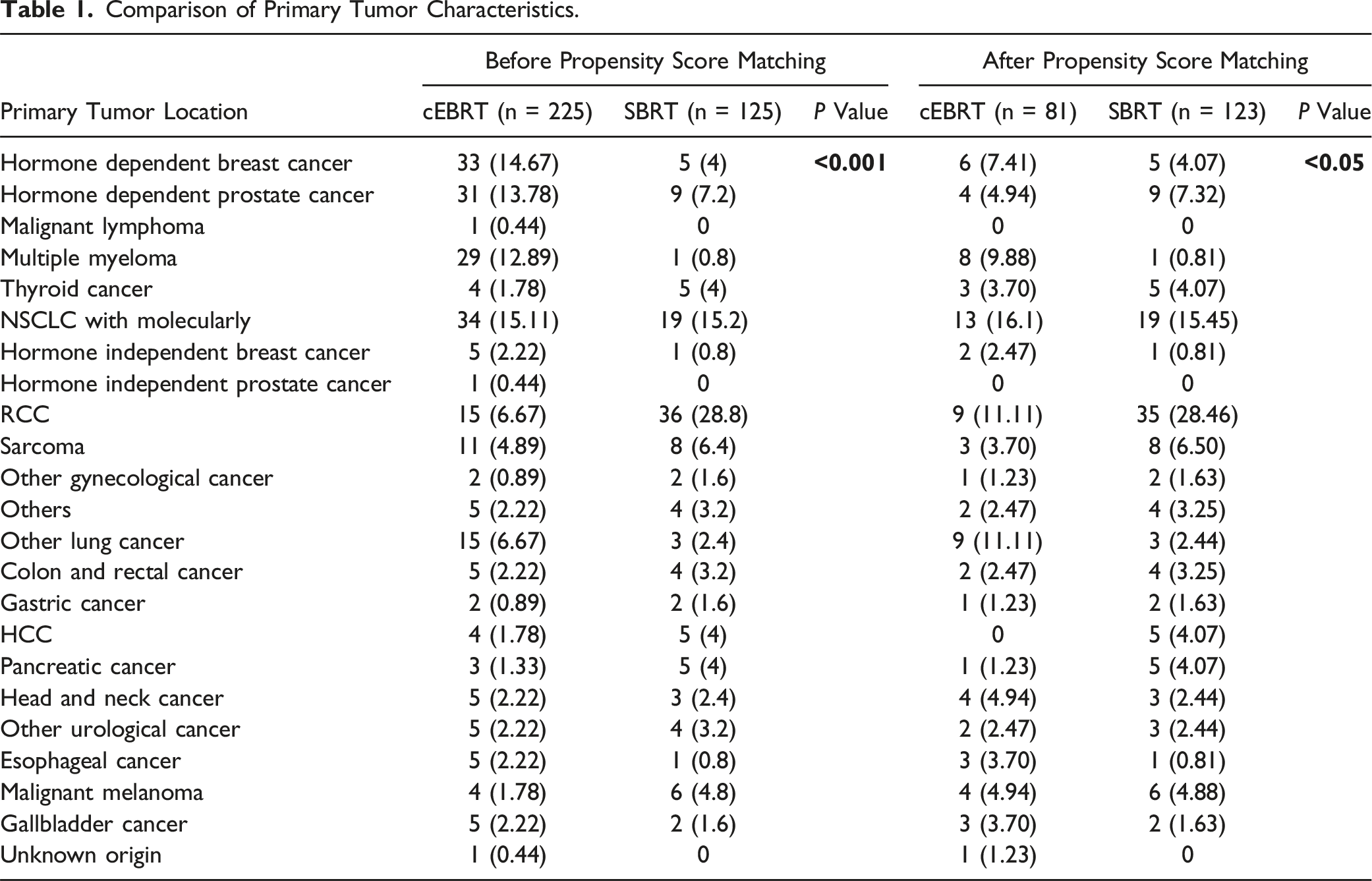
Comparison of Primary Tumor Characteristics.
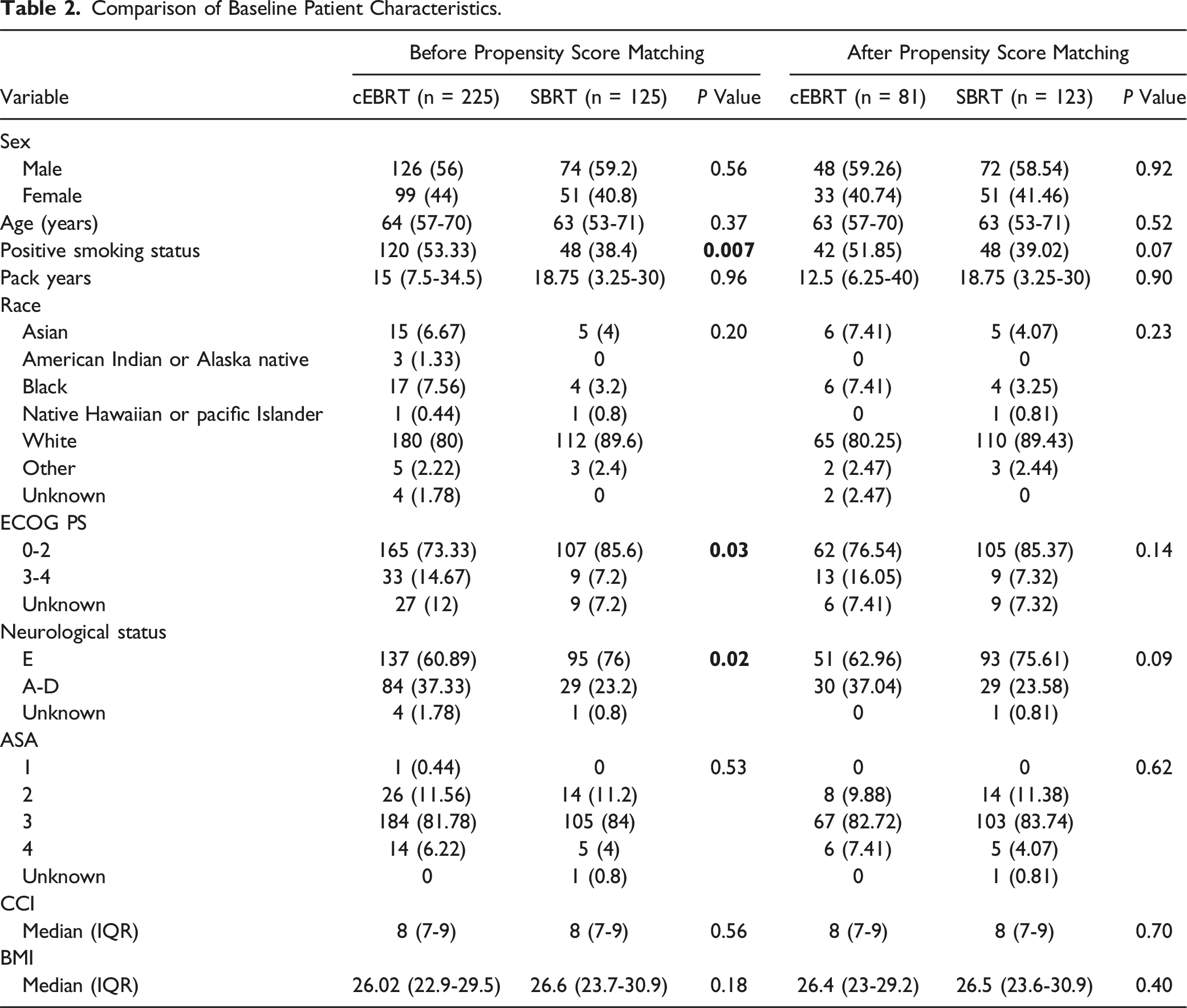
Comparison of Baseline Patient Characteristics.
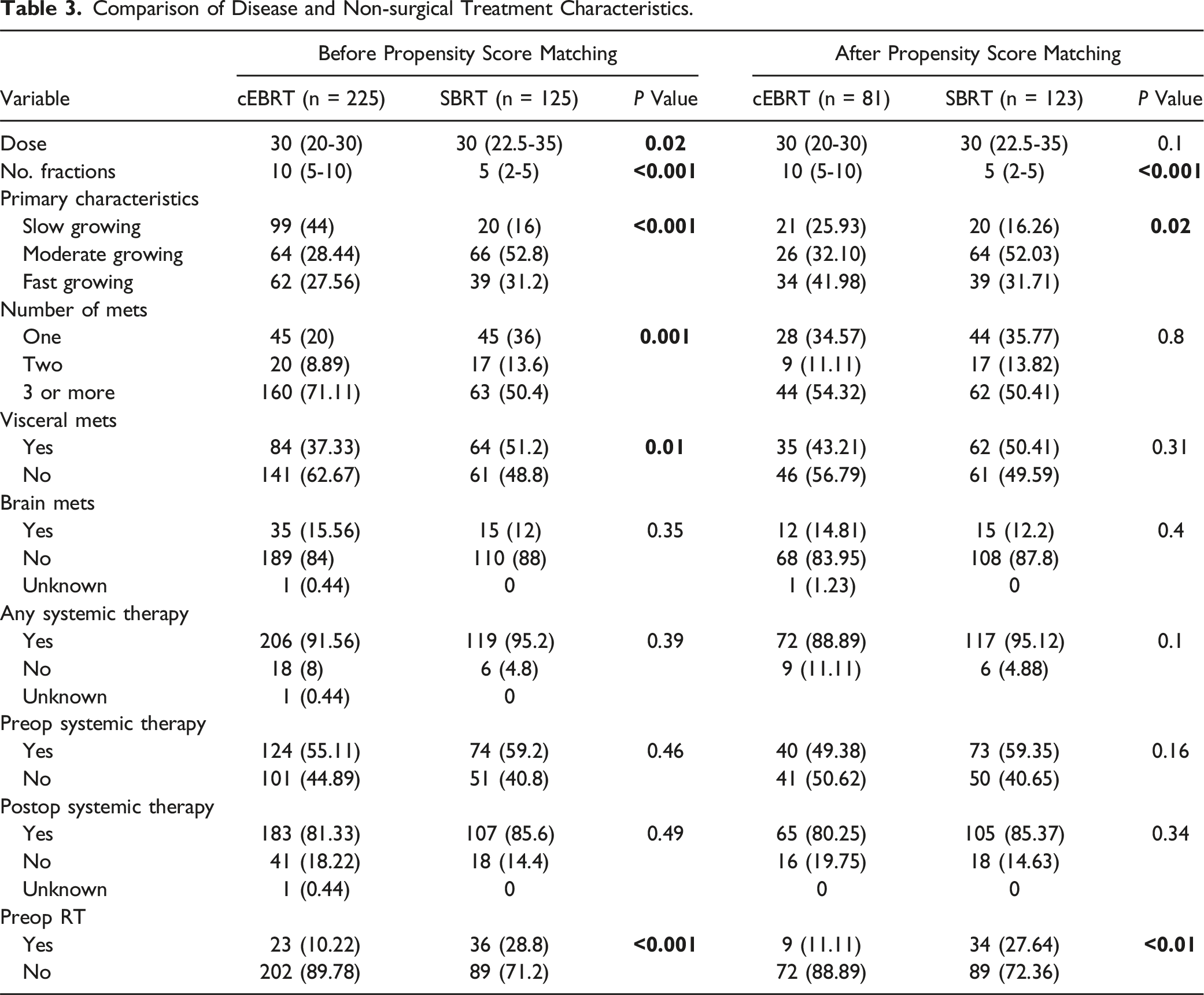
Comparison of Disease and Non-surgical Treatment Characteristics.
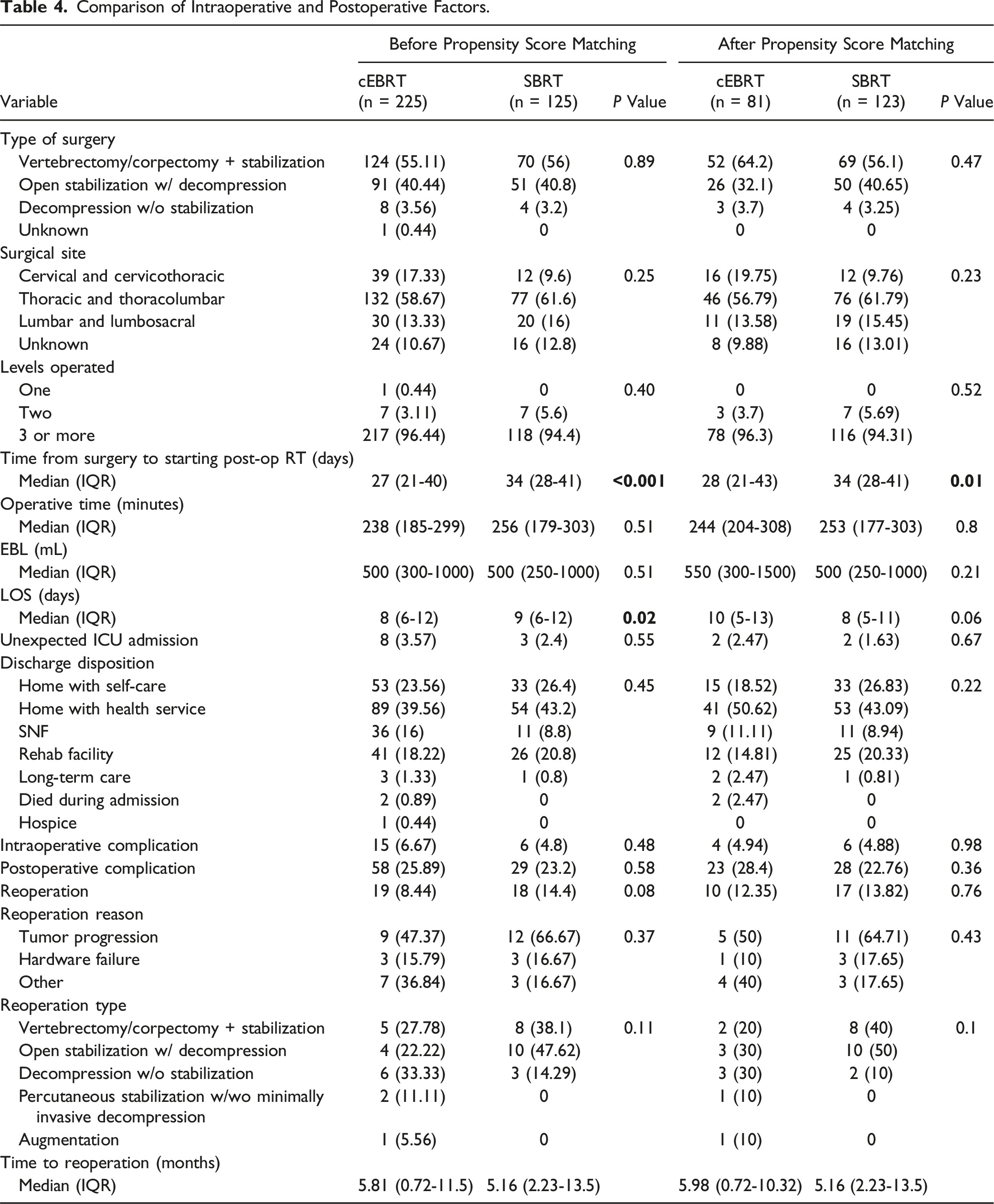
Comparison of Intraoperative and Postoperative Factors.
Reoperation
Twenty-seven patients had a reoperation after the index surgery (13.2%). The reoperation rate was 12.4% (10/81) in the cEBRT group and 13.8% (17/123) in the SBRT group (P = 0.76). Figure 3 shows the Kaplan-Meier curve for reoperation stratified by postoperative RT modality. The median time to reoperation was 6 months (IQR 1.4-11.5 months). Comparing cEBRT to SBRT, the median time to reoperation was 6 (IQR 0.7-10.3) vs 5.2 (IQR 2.2-13.5) months. Log-rank testing revealed no significant association between RT type and reoperation rate (P = 0.4). Most reoperations were due to tumor progression (55.6%), 11.1% were due to instrumentation failure, while 33.3% were due to other reasons. Kaplan-Meier curve depicting reoperation based on type of radiotherapy (cEBRT vs SBRT).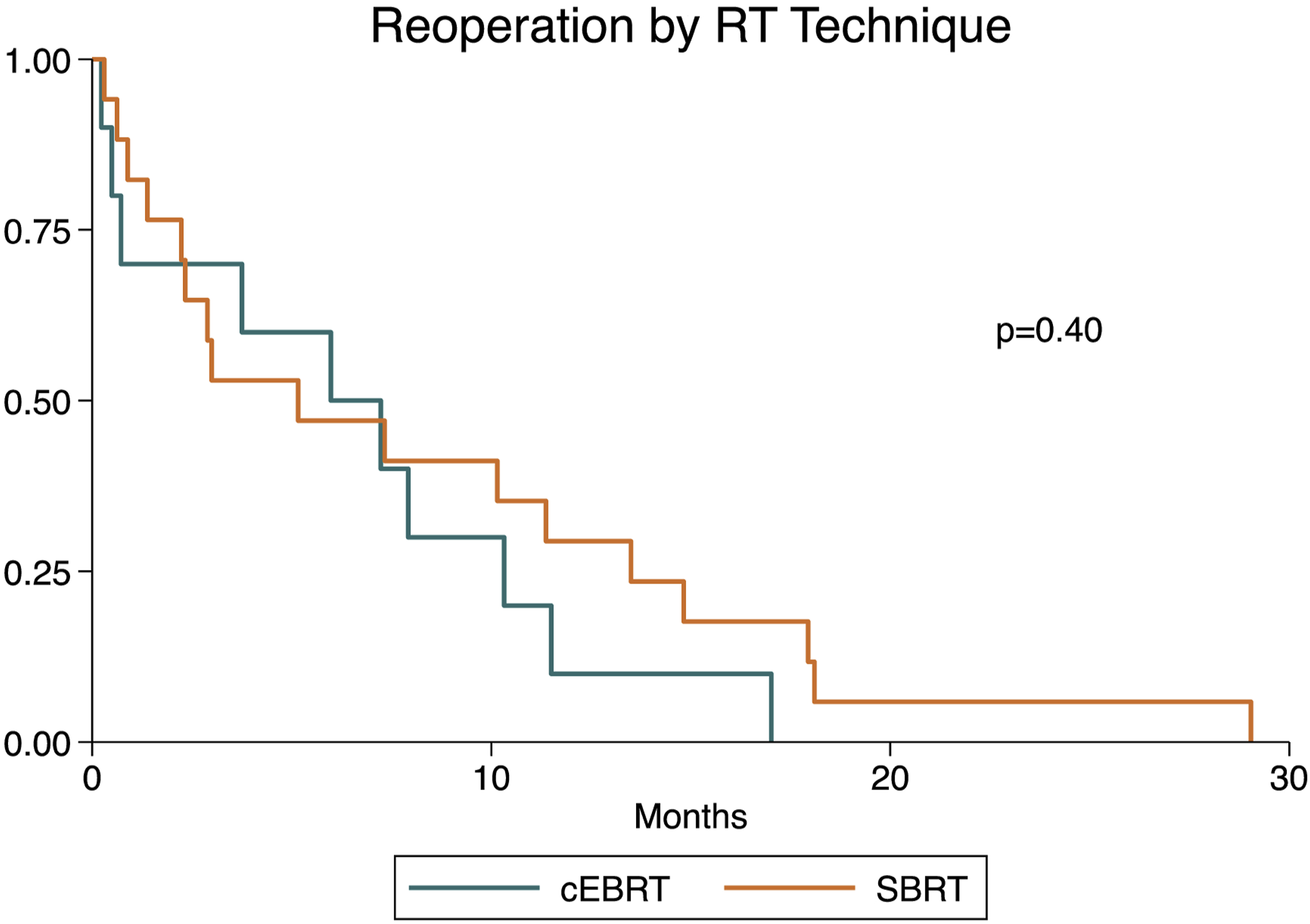
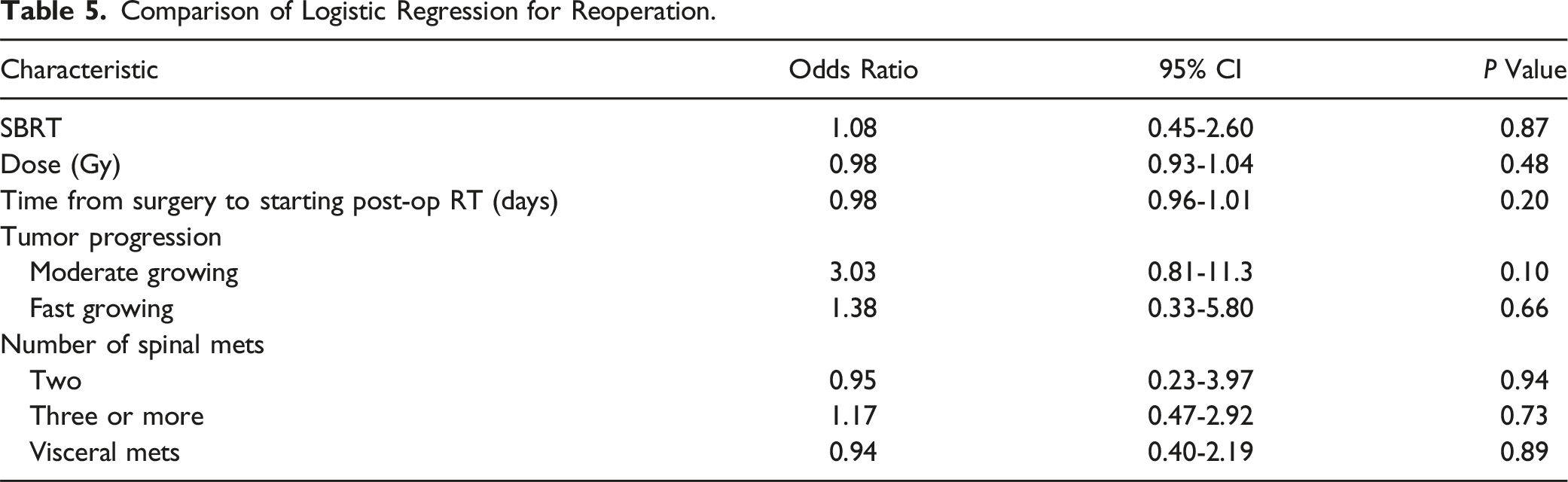
Comparison of Logistic Regression for Reoperation.
Secondary Outcomes
Median overall survival (OS) was 15.9 months (IQR 6.7-40.6 months). Log-rank testing revealed no significant association between RT type and OS (P = 0.56) (Figure 4). After 30 postoperative days, three patients had died. By 90 days postoperatively, 15 were deceased, while at 180, 365, and 540 days postoperatively 48, 88, and 104 were deceased, respectively. Pearson chi-square tests indicated no significant difference in vital status between RT modality for each time point. Similarly, there was no significant difference in postoperative complications between the 2 groups (P = 0.36). Kaplan-Meier curve depicting overall survival based on type of radiotherapy (cEBRT vs SBRT).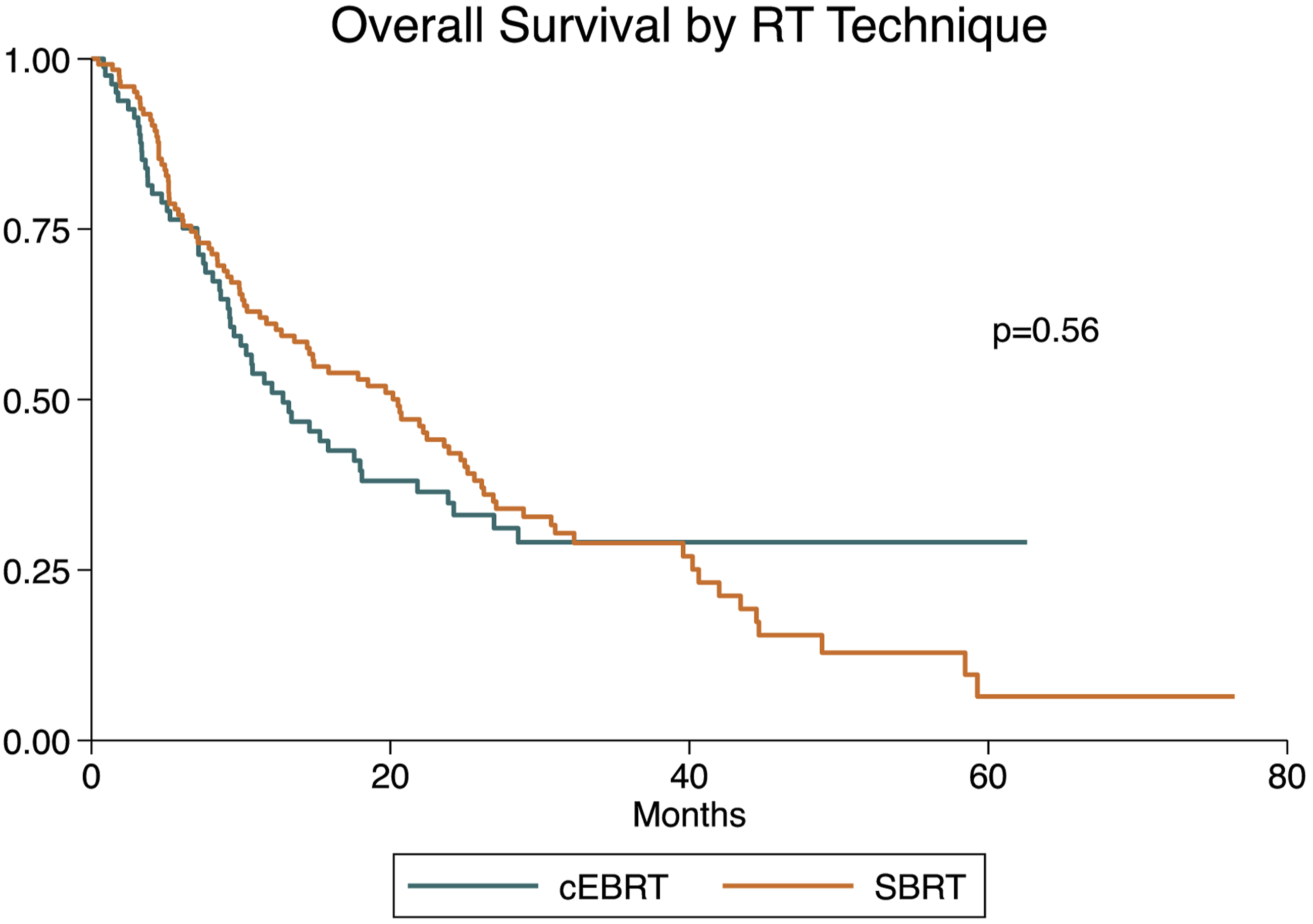
Discussion
The decision on how to postoperatively irradiate a patient with metastatic spinal disease is a common challenge in spine oncology, with an increasing number of clinicians opting for SBRT. A 2011 survey on SBRT usage found that two-thirds of respondents were already using SBRT, and among those who were not, the majority planned to adopt it. 19 Moreover, a substantial body of literature supports SBRT as a safe and effective treatment for local control and pain management in solid tumors following surgery.6-8,20,21 Similarly, other studies suggest excellent local control with adjuvant SBRT for spinal metastases compared to surgery alone.22,23 However, these studies primarily focus on SBRT in isolation, highlighting the need for a formal comparative study with conventional RT. Given the rapid adoption of SBRT and the relatively limited data directly comparing its efficacy to cEBRT, we aimed to evaluate the local control and overall survival outcomes of each treatment when used postoperatively in patients with spinal metastases.
Reoperation Rate and Overall Survival
Our results indicate that SBRT does not provide improved reoperation rates compared to cEBRT. Additionally, there was no significant difference in overall survival (OS) between the 2 groups, suggesting that conventional RT is equally effective as a postoperative treatment for spinal metastases. We also observed no significant difference in reoperation rates, which served as an indirect indicator of local control. While not all patients with recurrence undergo reoperation—due to factors such as oncologic deterioration, medical comorbidities, or patient preference—imaging can result in false positives and may not fully capture the clinical impact of recurrence. Reoperation conversely is a measurable marker of a clinically significant detrimental disease course and treatment failure.
To our knowledge, no study has directly evaluated the local control rates achieved from SBRT compared to cEBRT. A previous prospective study of postoperative spine SBRT demonstrates excellent local control with low toxicity and is most comparable to our retrospective investigation of the 2 modalities. 8 However, the patient population and variables are distinct from the methods of assessment and focus of this study. In the prior study, the authors did not assess SBRT in comparison to conventional RT. The study followed only 35 patients, while this present study includes an overall group of 350 and a matched cohort of 204 patients. Notably, Redmond et al evaluated local control based on postoperative CT and MRI scans, which may have captured a wider range of tumor progression. In contrast, our study uses reoperation as a surrogate for local control, since tumor progression requiring reoperation is a more significant setback in a patient’s oncologic care.
Similar to prior studies, our data suggest local control rates around 87%.6-8,20,21,24 We found that 87.7% and 86.2% of patients treated with postoperative spinal RT did not require repeat surgery in the cEBRT and SBRT groups, respectively. Additionally, we found a median overall survival of 15.9 months with no difference between the treatment groups. This result is consistent with the published literature on postoperative SBRT reporting median overall survival times between 14 and 29 months.6,8 Therefore, our data support the claim that SBRT is a safe and effective postoperative treatment for spinal disease.
Unlike prior efforts, our study directly compared the outcomes of SBRT and cEBRT, and our results indicate that SBRT did not result in lower reoperation rates. Therefore, if SBRT is unavailable due to logistical challenges, it would be reasonable for patients to receive cEBRT instead. For example, prior studies investigating travel distance for radiation treatment found that SBRT treatment was associated with greater travel distances.25,26 One such study concluded that the mean distance from SBRT was 63.6 miles compared to a mean distance of 5.1 miles for conventional RT. Travel distance may be a significant economic barrier to the receipt of appropriate care. Thus, the results of our study support alleviating some economic burden and facilitating the delivery of appropriate treatment, since conventional RT is an equally effective treatment as SBRT for postoperative spinal metastases.
Postoperative Complications
Literature on complications after postoperative RT with either cEBRT or SBRT is limited, but there seem to be 2 opposing perspectives regarding the effects of the 2 treatment modalities. The major concern is that higher doses are predictive of vertebral compression fractures and radiation myelopathy.27,28 Others have hypothesized that SBRT may reduce radiation-related surgical complications, as the dose distribution is more targeted, thus sparing the wound. 29 Still other groups have found no difference in wound complications for patients treated with either modality. 30 Likewise, we found no difference in short-term postoperative complications between the 2 treatment groups, suggesting that SBRT does not confer a benefit to post-surgical complications. In summary, our findings suggest that SBRT is safe and effective, as it demonstrates comparable overall survival and local control rates to those reported in previous studies. However, our findings also show that SBRT and cEBRT may yield similar outcomes concerning local control, reoperation rates, complications, and overall survival. Therefore, in situations where logistical challenges make SBRT difficult to access, it is reasonable to consider cEBRT as an alternative.
In the present environment of medical cost concerns, it is also important to consider the financial implications of this treatment choice. SBRT is associated with higher treatment costs.31,32 However, it may be associated with fewer toxicities 31 and becomes more cost effective with increased expected survival.32,33 For example, a study of single fraction radiotherapy by Kim et al. found that SBRT is economically reasonable only when the patient is expected to survive at least 11 months. 32 Given our findings of similar rates of local control and overall survival between cEBRT and SBRT, palliative cEBRT remains a viable option in resource-limited settings without concern that substandard care is being delivered.
Limitations
While our results support a less burdensome approach to the radiation treatment of spinal disease, they must be viewed within the limitations of the study. Primarily, the study is limited by its retrospective design, which introduces inherent biases such as indication bias. Outcomes may be influenced by factors not fully captured in the data, leading to potential confounding effects. Additionally, the study’s setting in a high-volume academic center that treats many spinal metastases introduces expertise bias, limiting the generalizability of the findings to other settings. This bias complicates our finding that spinal metastases may be effectively treated at community centers with cEBRT, and caution must be applied when interpreting these results. Future studies are essential to identify patients who are most likely to benefit from SBRT, potentially due to factors that increase their risk for toxicity from cEBRT. Additionally, our study assessed only short-term complications, which may insufficiently capture long-term deleterious effects of SBRT or cEBRT. Given these limitations, our recommendations should be interpreted with caution, as they may not fully account for confounding factors across different settings and longer time periods.
Conclusion
There was no demonstratable difference in overall survival in this cohort of surgical patients with metastatic spinal disease treated with either postoperative SBRT or cEBRT. These data suggest that cEBRT continues to be a valid treatment option, especially when logistical challenges or financial considerations limit access to more contemporary radiation modalities.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.