
Abstract
Study Design:
Retrospective cohort study.
Objectives:
The treatment of giant thoracic disc herniation (gTDH)remains challenging for surgeons worldwide because of its large volume and calcified or ossified nature and the limitations of the prior small-sample-size, single-center studies reporting comparative effectiveness. We aim to compare the anterior decompression and spinal fusion (ASF) and posterior circumspinal decompression and spinal fusion (PCDF) for patients with myelopathy due to gTDH in the largest study to date by sample size.
Methods:
Preoperative and postoperative functional status, surgical details, and complication rates were compared between the 2 groups.
Results:
A total of 186 patients were included: 63 (33.9%) ASF and 123(66.1%) PCDF. The PCDF group had significantly shorter operation duration (163.06 ± 53.49 min vs. 180.78 ± 52.06 min, P = 0.032) and a significant decrease in intraoperative blood loss(716.83 mL vs. 947.94 mL, P = 0.045), and also a shorter hospital length of stay (LOS) and postoperative LOS (6 vs. 7, P = 0.011). The perioperative complication rate (13.8% vs. 28.6%, P = 0.015) and surgery-associated complication rate(13.0% vs. 27.0%, P = 0.018) were significantly higher in the ASF group. A higher rate of complete decompression was achieved in the PCDF group. There were no observed significant differences in changes in functional status between the 2 groups.
Conclusion:
PCDF for central or paracentral gTDHs is a highly effective and reliable technique. It can be performed safely with a low complication rate. If either procedure can adequately excise a central or paracentral gTDH, a PCDF approach may be a better option.
Keywords
Introduction
Hott et al 1 defined such giant thoracic disc herniations(gTDHs) as those occupying at least 40% of the spinal canal’s diameter based on preoperative CT myelography, MR imaging, or both. Giant TDHs typically present with slowly progressive myelopathy and differ significantly from smaller thoracic disc herniations in clinical presentation, intraoperative morphology, and postoperative outcomes.1,2 Most surgeons recommend surgery for giant TDHs because those TDHs frequently lead to the development of myelopathy. However, gTDHs could be difficult to remove because of the large volume and calcified or ossified nature of the gTDHs and the inherent vulnerability of the thoracic cord.2-7 Therefore, their treatment remains challenging for surgeons worldwide.
The surgical approaches available for gTDHs include thoracotomy, mini-thoracotomy, thoracoscopic, costotransversectomy, transpedicular approaches, and posterior bilateral total facetectomies approach.1-3,5-9 Since the posterior approach via laminectomy is associated with high morbidity, and most authors recommend various modified transthoracic approaches as the preferred treatment.6,7,10 However, the anterior approach is technically demanding because it involves manipulating the ribs, pleura, or the diaphragm. Furthermore, higher complication rates, especially pulmonary and cardiac complications, increased in-hospital mortality, and longer hospital length of stay (LOS) in the anterior approach was reported.11-13 The endoscopic procedure is considered less invasive, requiring surgeons with solid experience, but a high proportion of revision surgery and neurological deficit is observed. 3
Surgeons are more familiar with posterior-based decompressions of the disc, and it would be ideal if sufficient visual effects could be obtained through the posterior midline approach. We have previously reported a bilateral circumspinal decompression technique that includes a laminectomy plus bilateral facet joints excision and transforaminal decompression for patients with thoracolumbar disc herniations (TLDH) and showed it was a highly effective and safe procedure for decompression, which is comparable to the anterior transthoracic approach for the surgical treatment of TLDH patients.14,15 We gradually applied this technique to treat patients with central or paracentral gTDHs. Thus, we present a retrospective analysis of 186 cases of gTDHs, which is the largest series reported to date, intending to overcome some of the gaps in knowledge of this rare and challenging diagnosis, compare the outcomes and complications between ASF and PCDF to provide another surgical option for the treatment of gTDH in the future.
Patients and Methods
Population
We retrospectively analyzed 186 patients, with at least a 12-month follow-up, who had undergone surgery for central or paracentral gTDHs between March 2006 and March 2019. All patients had neurologic symptoms that warranted surgery. CT and MRI were used to confirm the diagnosis. The exclusion criteria were diffuse idiopathic skeletal hyperostosis, spinal infections, spinal compression fractures, malignant tumors of the spine, thoracic kyphosis, and scoliosis rotational deformity. This study was approved by the Ethical Committee of our hospital and conducted according to the Declaration of Helsinki principles. The informed consent was waived because this was a retrospective study.
These patients include 145 males and 41 females, with an average age of 46.44 ± 13.24 years (range 20∼77 years). One hundred and sixty-five patients were operated on at a single level, and 20 patients were operated on at 2 levels, and one was at 3 levels. Of the 208 herniated discs with a mean canal occupancy of 58.78 ± 12.45%, 171 were excised central, and 37 were paracentral. That is, they were broad-based and extended across the midline significantly. Besides, 83.2% of them were “hard discs” with a significant calcified or ossified component compressing the dural sac. Of these patients, 134 were followed up after the operation, with a mean follow-up period of 75.82 months (range, 15-166 months). The distribution of the lesions is illustrated in Figure 1.
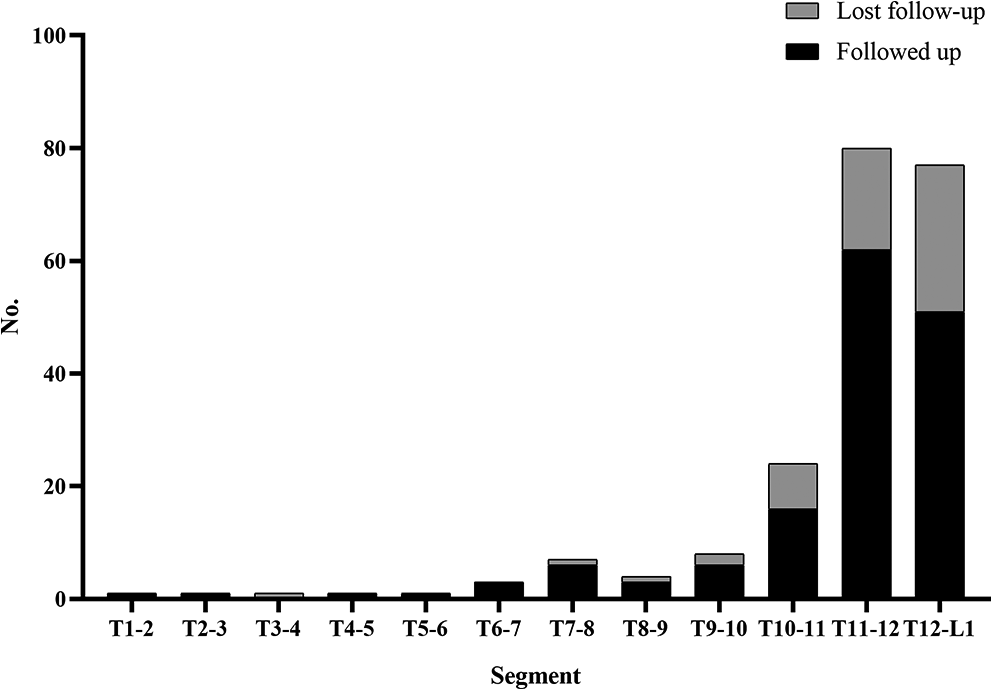
The distribution of the operated levels. A total of 208 discs were excised, and 52 patients (57 discs) did not attend the final follow-up.
Operative Technique
In all cases included in this study, meticulous surgeries were performed by the senior authors (Zhongqiang Chen, Chuiguo Sun, Zhongjun Liu, Xiaoguang Liu, and Weishi Li), who had at least 15 years of thoracic spinal surgery experience before. All surgical strategies and approaches were discussed and decided by these surgeons before the operation.
Posterior circumspinal decompression and spinal fusion
The PCDF technique was as we previously described.14,15 The posterior elements were exposed through a midline incision in the prone position. The bilateral pedicle screws were inserted at segments of decompression, and then laminectomy was performed. The ossification or hypertrophy of the ligamentum flavum, if present, was also removed. After that, the residual lateral facet joint (the entire inferior articular process and the superior portion of the superior articular process) was resected to manipulate the disc. At this time, the epidural venous plexus and the blood vessels accompanying the exiting nerve root usually bleed heavily. Therefore, it is necessary to carefully coagulate the blood vessels, identify the nerve roots, and protect them with a small cotton piece. After posterior laminectomy and facet joint excision, the posterolateral rim of the herniated disc was exposed. Next, we pushed the pleura (or peritoneum) away from the vertebra with a smooth gauze and inserted the gauze between the lateral side of the disc and the pleura to protect the pleura when exposed the disc’s posterolateral rim. Rongeurs and curettes were used to remove the lateral portion of the herniated disc first, leaving the middle portion of the herniated disc that is located directly ventral to the dura intact.
In most cases, the residual anterior midline compression was continuous with the adjacent vertebrae and resembled a “hard shell.” A neural dissector was inserted into the space between the base of the “hard shell” (the junction of the “shell” and the vertebral body), and the adhesion between them was gently separated. Next, we then put the cutting edge of an osteostome on the junction of the “hard shell” (the residual middle portion of the disc) and the vertebra and carefully knocked the hard shell off from the vertebra from an angle as parallel to the horizon as possible. When decompression was performed on one side in this step, a rod was contoured and set into the screw head on the other side for interim stability. After the “hard shell” was nearly isolated, with a neural dissector dissecting the compressive pathology off the dura, a rongeur was used to pull down the “hard shell” as well as the connected nucleus material into the intervertebral space before their removal. Mostly, successful ventral decompressions were achieved by alternative and interactive manipulation from both sides. A cage with autologous bone graft was packed in the disc space for the fusion. Then bilateral rods were set into the screw head.
Anterior transthoracic approach
In this group, 14 patients underwent a transpleural approach while the other 49 patients underwent the extrapleural or extraperitoneal approach, depending on the lesion level. Those 2 approaches’ surgical procedures were similar to those reported by Quraishi et al 10 and Otani et al 16 , respectively.
Clinical Outcomes
All patients were routinely received CT or MRI and X-rays of the surgical site at discharge. Based on postoperative radiological data, we classified decompression as complete decompression, disc remnant without compression, and disc remnant resulting in compression on the spinal cord and/or spinal root. 17
Only the patients who were followed up (92 in PCDF and 42 in ASF) were included in this part of the study. The pre/postoperative neurologic statuses of the patients were assessed by the modified Japanese Orthopedic Association (mJOA) scoring system (maximum 11 points) and the ASIA grading system, and the mJOA score was used to evaluate the spinal cord function improvement. Recovery rate [(postoperative score -preoperative score)/(11 − preoperative score) × 100%] was classified into 5 groups: excellent (75-100%), good (50-74%), fair (25-49%), unchanged (0-24%), and worse (less than 0%). 18 Pre/postoperative back pain and leg pain were assessed using the linear visual analog scale (VAS). Moreover, the Oswestry Disability Index (ODI) is used to measure function.
Statistical Analysis
SPSS software (version 22.0; IBM) was used for statistical analysis. Simple comparisons of continuous data between groups were carried out with the Student’s t-test or Mann Whitney U-test, depending on whether the distribution was normal or abnormal, respectively. Categorical variables were compared using the X2 test or Fisher’s exact test. An Enter multiple logistic regression analysis were fitted for perioperative complication development, prolonged length of postoperative stay(greater than the 75th percentile, i.e. 8 days.), and mJOA improvement (recovery rate ≥50%) after adjusting for age, sex, BMI, preoperative comorbidity, TDH type and canal occupancy and surgery duration in order to investigate the independent effect of the surgerial approach. An association was considered significant if P < 0.05.
Results
Demographic Data and Comorbidities
The demographic data were summarized in Table 1. The rates of preoperative comorbidities, combined OLF at the disc herniated same level, and the smoking in patients treated by PCDF were higher than those in the ASF group.
Patient Demographics and Comorbidities.
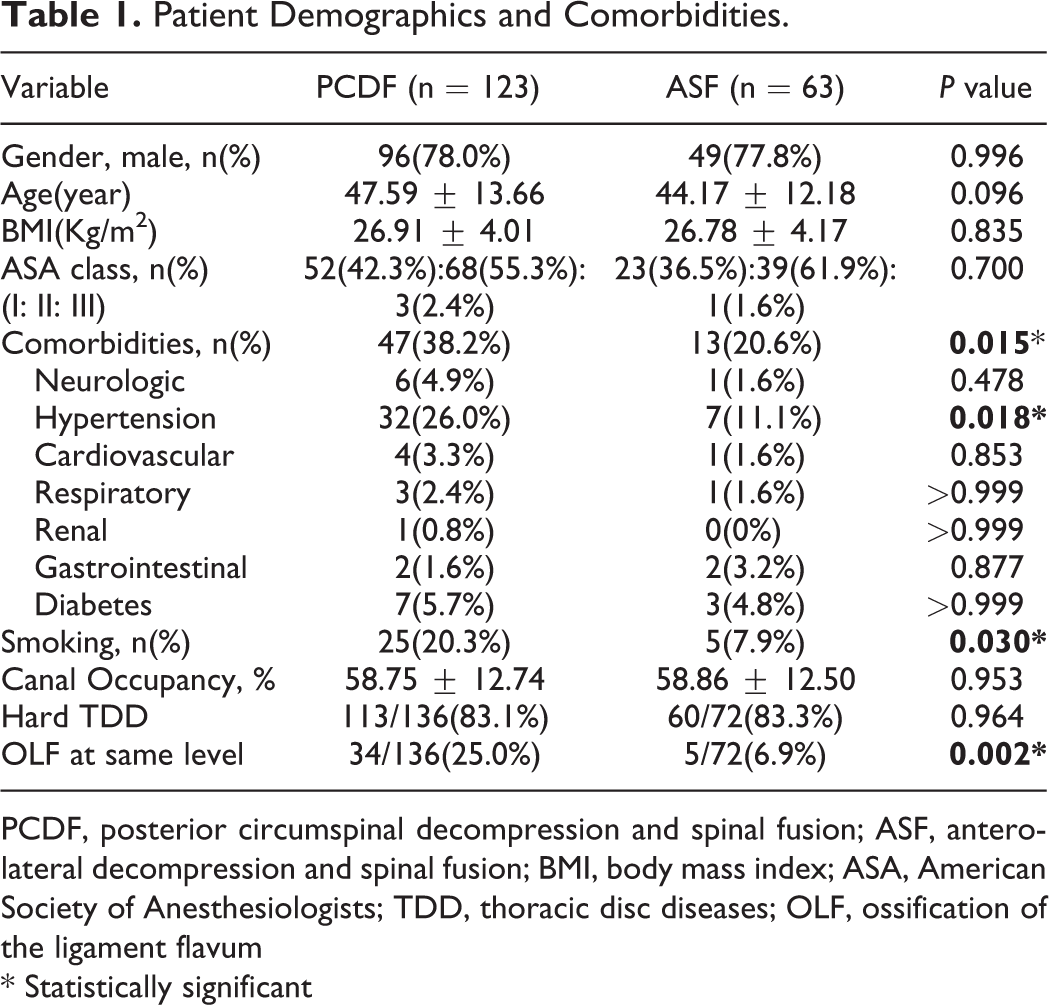
PCDF, posterior circumspinal decompression and spinal fusion; ASF, anterolateral decompression and spinal fusion; BMI, body mass index; ASA, American Society of Anesthesiologists; TDD, thoracic disc diseases; OLF, ossification of the ligament flavum
* Statistically significant
Surgical Characteristics and Complications
PCDF, either in total or per disc excised, had a shorter operative time and less intraoperative blood loss than the ASF group. All discs were successfully removed with no incidence of wrong-level surgery. Detailed descriptions of perioperative complications were outlined in Table 2. Overall, perioperative complications and surgery-associated complication rates were significantly higher for patients who received an ASF procedure than those receiving a PCDF.
Operative Variables and Postoperative Complication Development Across Surgical Groups.
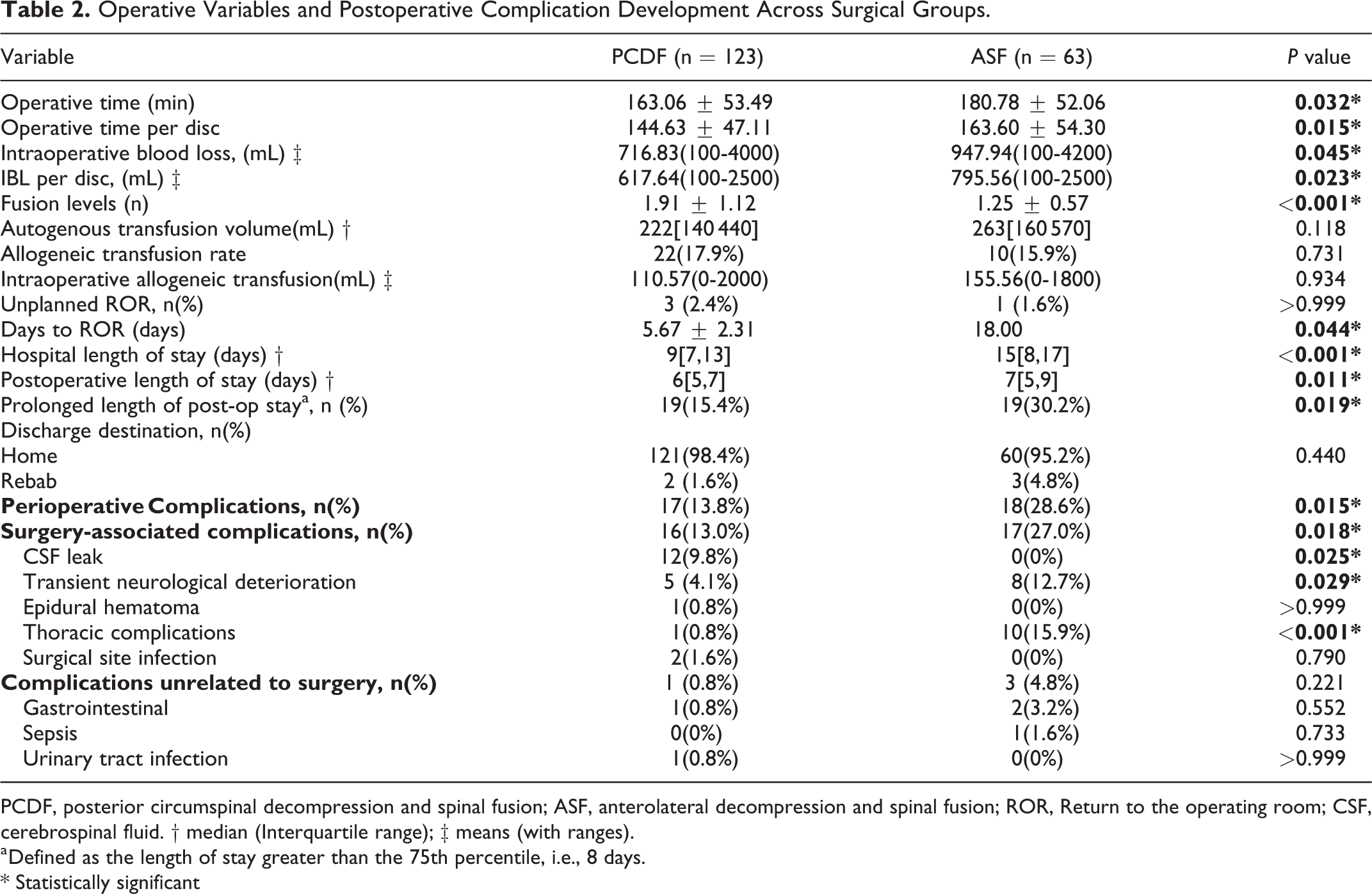
PCDF, posterior circumspinal decompression and spinal fusion; ASF, anterolateral decompression and spinal fusion; ROR, Return to the operating room; CSF, cerebrospinal fluid. † median (Interquartile range); ‡ means (with ranges).
a Defined as the length of stay greater than the 75th percentile, i.e., 8 days.
* Statistically significant
Patients undergoing ASF had significantly higher rates of transient neurological deterioration and thoracic complications than the PCDF group. Conversely, a significantly higher proportion of patients in the PCDF group developed the cerebrospinal fluid leak (9.8%) compared to the ASF group. Ten patients developed thoracic complications in the ASF group (1 pulmonary embolism, 3 pleural effusion, 1 pneumonia, 5 pneumonia with pleural effusion), and 1 patient in PCDF developed pneumothorax. Postoperative wound infections occurred in 2 patients and improved after the revision and antibiotic treatment. Hospital and postoperative length of stay (LOS) was significantly longer for patients in the ASF group.
Multivariable Regression Analysis
The results of the multivariable logistic regression analysis about perioperative complication development, prolonged length of postoperative stay, and mJOA improvement were shown in Table 3. The independent variable chosen in the multivariate regression analyses was noted in the notes below Table 3, which were chosen from the results of univariate analysis, the risk factors reported by previous studies, and the potential risk factors we think might influence the dependent variables. Patients undergoing PCDF had significantly lower odds of having perioperative complications (OR: 0.41, 95% CI:0.18–0.93, P = .032) and lower odds of prolonged length of stay (i.e., more than 8 days) (OR: 0.44, 95% CI:0.20–0.98, P = .043) compared to the ASF group. However, the effect of the surgical approach was not significant to reach an mJOA good recovery rate(≥50%). The analysis revealed that older patients were associated with an increased risk of perioperative complications and not reaching good mJOA recovery. Longer surgery duration increased risks of perioperative complications and prolonged length of postoperative stay. Higher ASA classification (class II and III) and hard discs increased the risk of missing good mJOA recovery.
Adjusted Odds Ratio of the Effect of Procedure Type on Perioperative Complication Development, Prolonged Length of Stay and mJOA Improvement.
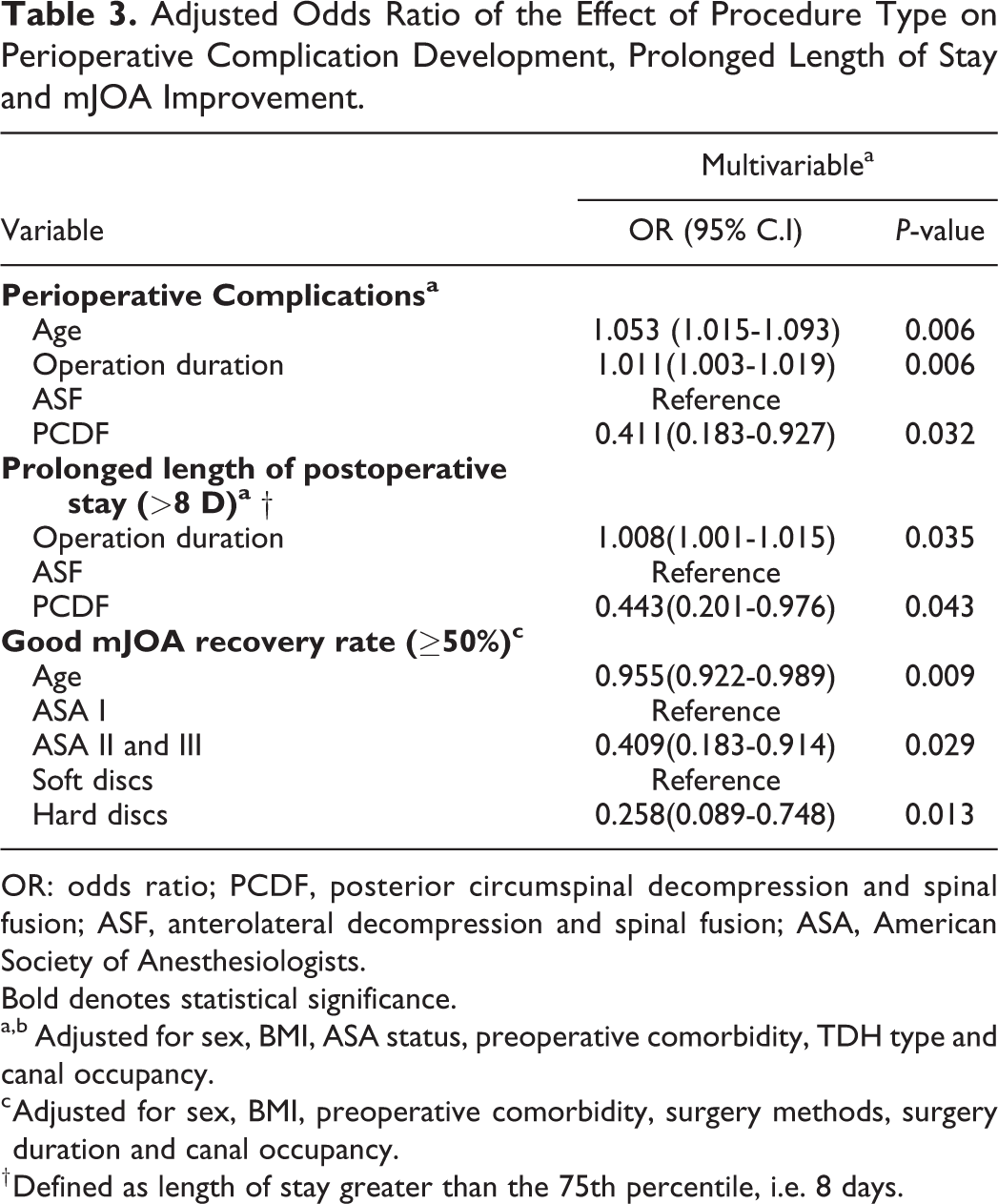
OR: odds ratio; PCDF, posterior circumspinal decompression and spinal fusion; ASF, anterolateral decompression and spinal fusion; ASA, American Society of Anesthesiologists.
Bold denotes statistical significance.
a,b Adjusted for sex, BMI, ASA status, preoperative comorbidity, TDH type and canal occupancy.
c Adjusted for sex, BMI, preoperative comorbidity, surgery methods, surgery duration and canal occupancy.
† Defined as length of stay greater than the 75th percentile, i.e. 8 days.
Clinical Outcomes
Complete resection and decompression was achieved in 127 discs (93.4%) in the PCDF group (Figure 2), which were significantly higher than ASF (93.4% vs. 62.5%, P < 0.001). 5.9% discs in PCDF and 36.1% in ASF had minimal disc remnants without a compressive effect either on the spinal cord or the nerve root. A disc remnant compressing the spinal cord was still present in 2 patients (1 in PCDF and 1 in ASF). Both of them were reoperated, achieving complete decompression. In the 134 patients who attended the final follow-up, all patients except one in the PCDF had a solid fusion at the final follow-up, and the fusion rate was 98.9% and 100% in PCDF and ASF group, respectively. The patient complained of numbness in his lower back and right lower extremity, intermittent claudication with a 400-meter walking distance, and back pain (VAS score 6) after he had long-distance travel by bus 1 year after his primary PCDF surgery. He was diagnosed as non-fusion and screw loosening because of discontinuous bone bridging and a radiolucent line around the screws in the axial CT image, which was confirmed in the revision surgery.
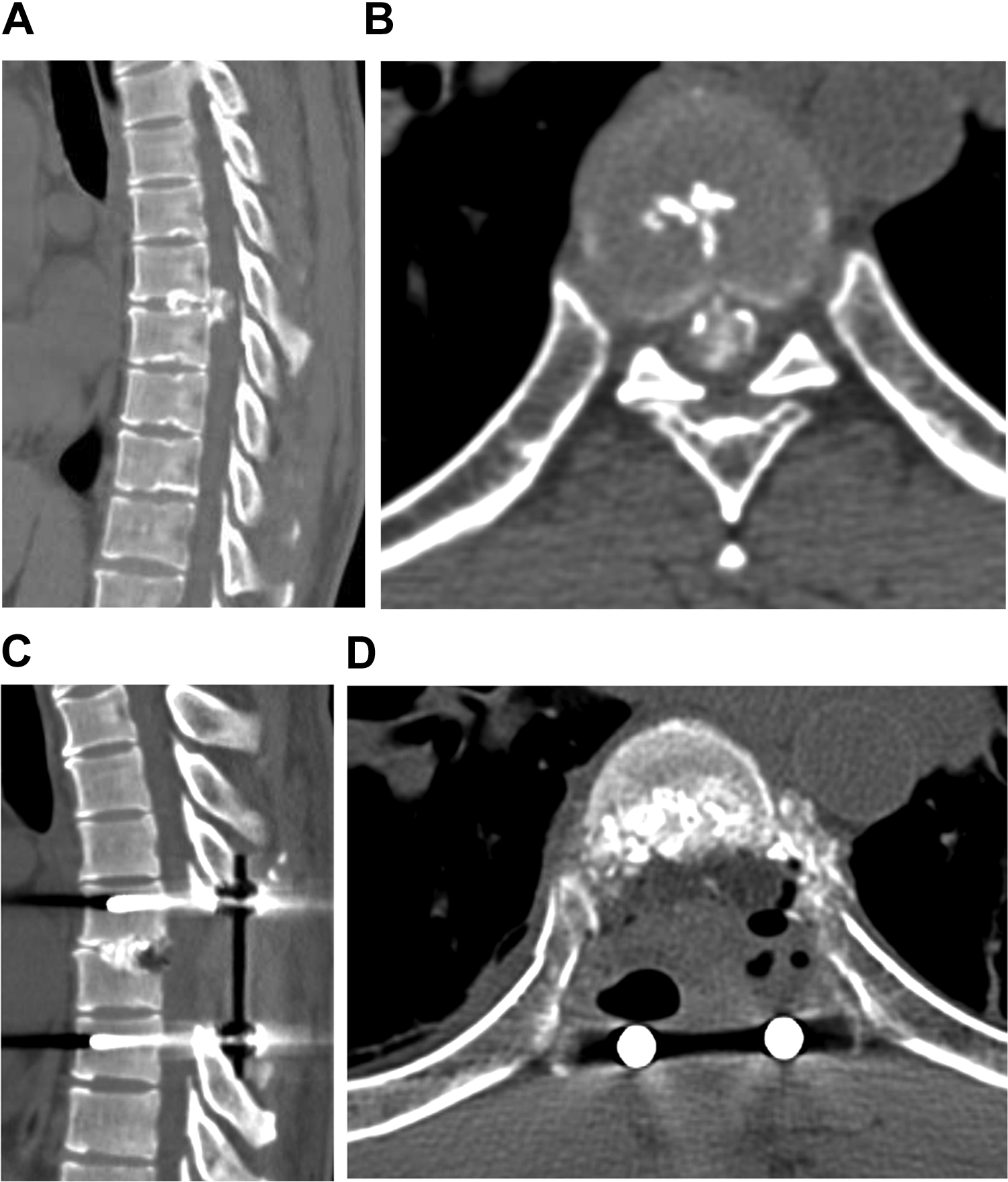
Case example: 43-year-old male patient presented with calcified disc herniation with motor and sensory disturbances, and after complete resection of the herniation by PCDF, mJOA scores improved from 3 to 11 points. Preoperative CT (A, B) showed the ventrally central compression of a “hard disc” of 80% canal occupation at T7-8; Postoperative CT image demonstrating that the herniated hard disc and the bilateral facet joints had been removed and satisfactory decompression (C, D).
A significant difference was detected between baseline and follow-up clinical scores in all the 134 patients who finished the final follow-up in both groups. However, there was no difference between the 2 groups in the improvements of those scores (Table 4). There were 70.7% and 64.3% of patients in the PCDF and ASF who reached a good or excellent mJOA recovery rate (P = 0.461). The preoperative and follow-up ASIA grades of patients in both groups were shown in Figure 3. In the final follow-up, 61 (66.4%) PCDF patients and 22 (52.4%) ASF patients improved by at least 1 grade, and neurology deteriorated by 1 ASIA grade in 4 (4.3%) patients in PCDF and 2 (4.8%) in ASF group.
Outcome Parameters Between the 2 Groups.
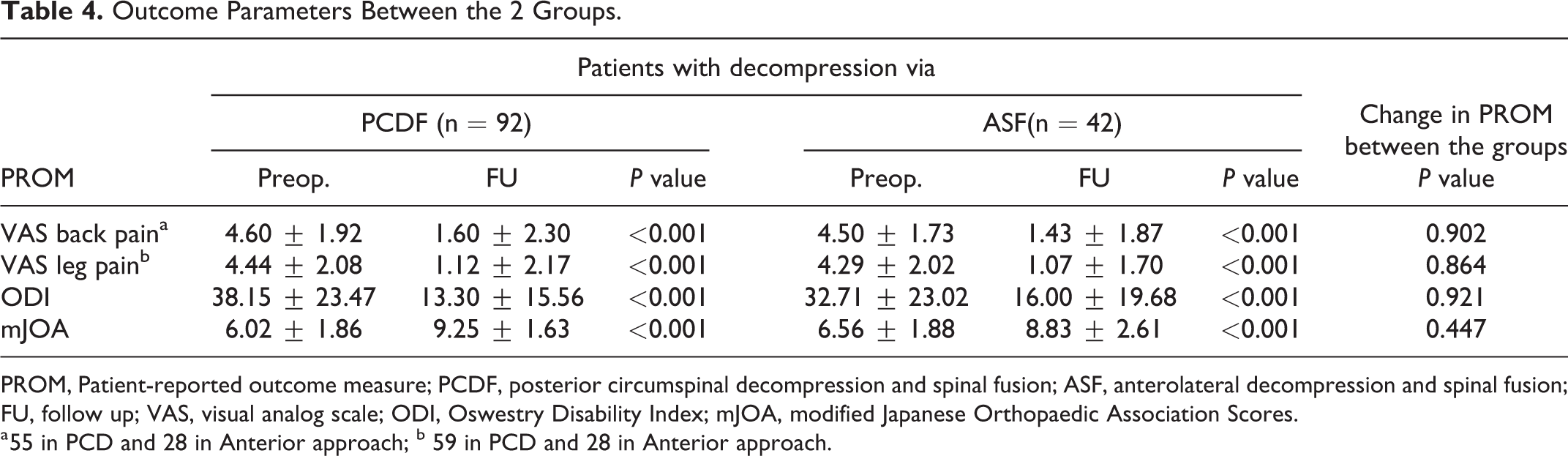
PROM, Patient-reported outcome measure; PCDF, posterior circumspinal decompression and spinal fusion; ASF, anterolateral decompression and spinal fusion; FU, follow up; VAS, visual analog scale; ODI, Oswestry Disability Index; mJOA, modified Japanese Orthopaedic Association Scores.
a 55 in PCD and 28 in Anterior approach; b 59 in PCD and 28 in Anterior approach.
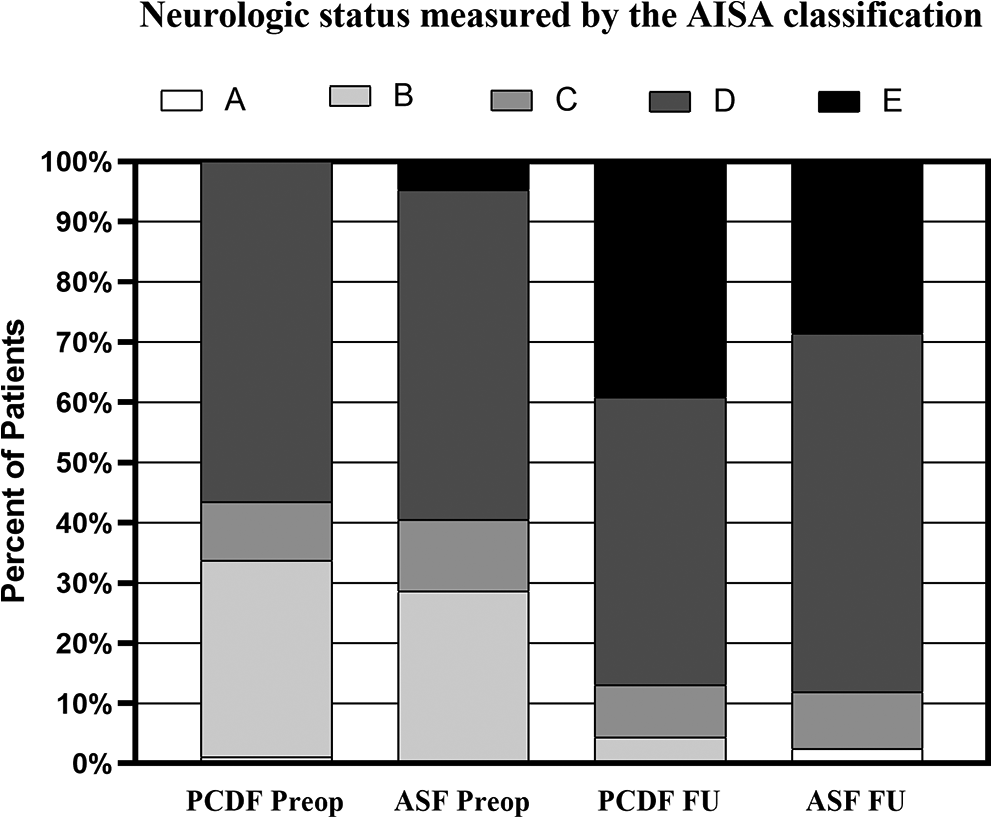
The preoperative and follow-up ASIA grades.
Discussion
This study retrospectively analyzed the outcomes of the surgical treatment of 186 patients with gTDH. To the best of our knowledge, we report the largest series of patients operated for gTDH. The results showed that the PCDF group had significantly shorter operative duration, less intraoperative blood loss, fewer perioperative complications, and shorter length of stay comparing with ASF. However, there were no observed significant differences in the recovery of the postoperative functional status of patients.
Both anterior and posterior surgical techniques have been described for the surgical management of gTDH.1-3,8-10,18-20 The anterior thoracotomy approach has advantages in proving a direct view of the herniated discs and the sheath. However, the visualization provided by the anterior transthoracic approach is still inadequate because that the neural elements on the other side of the spinal canal are not in direct view for most of the decompression process, and it is necessary to access the dura through the compressive lesion, predisposing the patient to inadvertent cord injury 14 . Furthermore, the anterior thoracotomy approach carries potential morbidity associated with thoracotomy, resulting in increased in-hospital morbidity and mortality rates and increased health care burden.9,19,21
Stillerman et al 22 first described the transfacet pedicle-sparing approach and demonstrated that it decreased operative time and blood loss and diminished perioperative pain. Machino et al 23 applied unilateral transforaminal thoracic interbody fusion (TTIF) using a single posterior approach to treat thoracic spine lesions. However, unilateral TTIF was insufficient for effective decompression in central and paracentral gTDH. In 2008, we developed a bilateral circumspinal decompression technique (PCDF) that resembles Machino’s technique and includes a laminectomy plus bilateral facet joints excision and transforaminal decompression for patients with thoracolumbar disc herniations (TLDH). 14 Furthermore, this study further confirmed its efficacy and safety in the surgical treatment of central and paracentral gTDH patients. In contrast, the greatest advantage of the PCDF technique is that it enables anterior decompression with sufficient vision without excess retraction of the neural elements.
The operative age of the PCDF approach patients was slightly older than that of ASF patients, and the proportions of preoperative comorbidities and smoking of the PCDF patients were also higher than that of ASF patients. The high risk of thoracic complications was associated with the anterior approach, which might make doctors more inclined to select younger, healthier patients for anterior surgery. Another possible reason for the results might be that the ASF was a small sample size. In this study, spinal surgeons performed all surgeries who were not as familiar with anterior surgical anatomy as the posterior approach, which may be one reason for the longer operation time and higher intraoperative blood loss of the ASF. Besides, the wide exposure provided by laminectomy and bilateral resection of the facet joints ensures that all the neural elements are under the surgeon’s direct view throughout the discectomy process in PCDF, which created conditions for the convenience and speed of the surgery.
A 13.8% (17/123) rate of perioperative complications was found in the PCDF group. By contrast, 28.6% (18/63) of the patients in the ASF group had perioperative complications, with most events related to the thoracic complications and transient neurological deterioration. In the PCDF procedure, after posterior laminectomy and facet joint excision, the posterolateral rim of the herniated disc was exposed. Next, we pushed the pleura (or peritoneum) away from the vertebra with a smooth gauze and inserted the gauze between the lateral side of the disc and the pleura to protect the pleura when exposed to the disc’s posterolateral rim. However, the pleura was stripped off the chest wall when exposing the thoracic vertebrae in the extrapleural/extraperitoneal approach, and this procedure needed adequate access to the front and the opposite side, and space should be able to insert a fingertip into the opposite side.16 PCDF obviously has a wider operating space than the extrapleural/extraperitoneal approach when performing the discectomy, providing convenience for the operation, and dealing with the bleeding. That might account for a shorter operative time and less intraoperative blood loss in the PCDF group. The protection of pleura and wider operating space, which might contribute to lower rates of pulmonary complications. The complication rate of TDH treated by the thoracic approach has been reported in the literature in the range of 11-38%, higher than PSF, especially pulmonary and cardiac complications.11-13,17 Our results corroborate previous literature demonstrating that anterior approaches are associated with higher postoperative morbidity than posterior approaches.
In this study, the incidence of cerebrospinal fluid leakage in the PCDF was 9.8%. This rate compares favorably with the recent literature rate, and the rate of dural tears during thoracic disc excision is approximately 10-15%. 24 A higher proportion of gTDH with OLF at the same level might account for a higher incidence of CSF leakage in the PCDF group. The Adamkiewicz segmental artery is anastomotic with the anterior spinal artery, which supplies blood to the spinal cord. The artery is located mainly on the left side of the lower thoracic vertebra. 25 Most thoracic disc herniations occur in the lower thoracic region. Unilateral segmental vessel ligation is routinely performed during anterior approaches. Therefore, there is a risk of spinal cord ischemia during segmental vessel ligation, including Adamkiewicz artery ligation, which may be why the proportion of patients with transient neurological deterioration of neurological symptoms after anterior surgery is higher than that of the PCDF surgery. In our long-term follow-up, we found that 4 (4.3%) patients in the PCDF and 2 (4.8%) patients in the ASF occurred neurological deterioration, similar to recent studies that report neurologic injury between 2-5% with no significantly increased risk with anyone approach technique.13,24,26
Our study had several limitations. First, its retrospective nature lends itself to limitations. However, prospective randomized controlled trials are difficult to conduct due to the low incidence of TDM and various surgical procedures. Secondly, there may be selection bias in the selection of anterior and posterior surgery. Although experts have carefully discussed all patients in the department before surgery, different surgeons have different proficiency in different surgical methods, and there is also a bias in the selection of surgical approaches. Finally, long-term follow-up is not available for all patients, affecting the final revision rates and long-term complications. However, improvements in neurological function were satisfactory in patients who completed follow-up.
Conclusion
This study showed that the circumspinal decompression procedure is an effective and safe technique for treating central and paracentral gTDH. Compared with ASF, PCDF had shorter operative duration, less intraoperative blood loss, fewer complications, and shorter length of stay. This procedure would be a particularly suitable option for gTDH patients with pulmonary morbidity that contradicts a thoracotomy or spine surgeons who are most familiar with the conventional posterior approach.
Footnotes
Authors’ Note
The survey data are publicly available on the internet for data users and researchers throughout the world. The device is approved by the corresponding national agency for this indication. Ethics approval was obtained from the Peking University Third Hospital Medical Science Research Ethics Committee (IRB00006761-M2020049) and registering in the Chinese Clinical Trial Registry (registration ID: ChiCTR2000032957. ![]() ).
).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.