
Abstract
Study design
Retrospective cohort study.
Objectives
Same-day discharge is widely used in many surgical specialities. If carefully planned, it can improve patient outcomes whilst using resources efficiently. We aimed to investigate the safety of same-day discharge following a posterior lumbar decompression and/or discectomy (PLDD).
Methods
This was a retrospective analysis of administrative data. We extracted data from the Hospital Episodes Statistics database for the 5 years from 1st April 2014 to 31st March 2019. Patients undergoing an elective one or two level PLDD aged 19-54 years during the index stay were included. The primary exposure variable was same-day discharge or post-surgery overnight stay and the primary outcome was emergency hospital readmission within 90 days post-discharge.
Results
Data were available for 45,814 PLDD performed across 103 hospital trusts of which 7914 (17.3%) were performed as same-day discharge. Same-day discharge rates varied from 87.7% to 0% across the 90 hospital trusts that operated on more than 50 patients during the study period. Fourteen (15.6%) trusts had same-day discharge rates above 30% and 57 (63.3%) trusts had same-day discharge rates below 10%. The odds of emergency hospital readmission within 90 days were lower for same-day discharge patients (odds ratio .72 (95% confidence interval .61 to .85). There was no difference in outcomes for patients seen at trusts with a same-day discharge rate of ≥30% compared to trusts with a same-day discharge rate of ≤10%.
Conclusions
Same-day discharge low-complexity elective PLDD is safe in adult patients below the age of 55 years. There is potential for many providers to substantially increase their rates of same-day discharge.
Introduction
The efficient running of any healthcare system requires the optimisation of patient outcomes within a finite budget. Within the National Health Service (NHS) in England, the Getting It Right First Time (GIRFT) programme has a remit to reduce unwarranted variation in clinical practice where this impacts negatively on patient outcomes or cost-effectiveness.
As the NHS recovers from the COVID-19 pandemic, one area of particular interest is whether more elective surgical procedures can be performed with shorter hospital stay without this negatively impacting on patient outcomes. Within the field of spinal surgery the GIRFT national report highlighted large variations in the use of same-day discharge protocols for posterior lumbar decompression and/or discectomy (PLDD) between NHS hospital trusts in England. 1 Some trusts routinely performed PLDD as same-day discharge, with post-surgery overnight stay being the exception, whilst others kept all patients in overnight.
There are limited previously published data on the safety of same-day discharge PLDD as identified in a recent systematic review. 2 The review identified 15 studies on the topic and concluded that same-day discharge PLDD was safe, acceptable to patients and could result in significant cost savings. However, the literature is dominated by studies from North America (eight United States, three Canada), with only four European studies (two from the United Kingdom (UK)). The largest study included 1652 same-day discharge patients. Different models of healthcare funding and delivery in other settings mean that findings may not be readily transferable. The anecdotal experience of UK hospital trusts that use same-day discharge PLDD as routine is that their patient outcomes have not been affected. 1 A small UK-based trial of 31 patients published in 2002 found that day-case discectomy patients mobilised faster post-surgery and had improved ambulation at two weeks; complication rates were similar. 3 A 2014 study reported on the introduction of day-case surgery for discectomy in a single site in Manchester, UK and also concluded that for carefully selected patients, day-case surgery was safe. 4
We aimed to use an administrative dataset to investigate the safety of same-day discharge PLDD by comparing outcomes for those discharged on the same-day as their procedure and those who stayed at least one night in hospital post-surgery.
Methods
Study Design
This was a retrospective analysis of administrative data from the UK Hospital Episode Statistics (HES) database. The HES database is collected by NHS Digital and includes data for NHS hospital activity in England. This includes patients admitted to non-NHS hospitals but funded by the NHS. The data is entered by trained coders within each trust.
Ethics
The presentation of data follows current NHS digital guidance for use of HES data for research purposes. 5 Consent from individuals involved in this study was not required for analysis of this administrative dataset. Data were accessed in a pseudonymised form.
Data Extraction
Setting
All NHS hospitals in England are run by trusts. Each trust covers a geographically defined catchment area of varying physical size and population. A single trust typically runs between one and four large secondary or tertiary care hospitals. Within a trust, spinal surgery will generally be performed at a single site or by a single surgical team covering a number of sites.
Time Period
1st April 2014 to 31st March 2019 for the index procedure, with follow-up to 1 year post-discharge.
Inclusion and Exclusion Criteria for Index Procedure
We identified PLDD using the following Office of Populations Censuses and Surveys Classification of Interventions and Procedures version 4 (OPCS-4) codes if used in the first position in the record of procedures conducted: V252, V254, V255, V256, V258, V259, V671, V672, V331, V332, V337, V338, V339, or any occurrence of the following codes in the first position of the procedural record: V351, V358, V359 if used in combination with any of the codes Z063, Z073, Z665, Z675, Z676, Z993. The procedure descriptions that these codes relate to are listed in Supplementary material Table S1. Data for decompression procedures with and without discectomy were analysed together. The coding of PLDD procedures by individual hospital trusts did not allow for discectomies to be differentiated from other decompression procedures in a consistent and reliable manner within HES.
In addition to the criteria set out above, patients were excluded where: 1. Surgery was non-elective. 2. Where a fusion had also been conducted during the hospital spell. These cases were identified where any of the OPCS-4 codes V251, V253, V382, V383, V384, V385, V386, V404 appeared in any position in the procedural record. 3. The patient was aged < 19 years or > 54 years. 4. Surgery was three or more spinal levels (OPCS-4 code V553).
These exclusion criteria were used to ensure that the selected patients were most likely to have received low complexity surgery and so would be likely candidates for same-day discharge. None of the included patients had moderate or severely frailty according to the Hospital Frailty Risk Score (HFRS). 6
To ensure all datapoints were independent of one another at a patient level, only the chronologically first recorded index procedure for anyone who had more than one procedure during the study period was included in the dataset. The data extraction process is summarised in Figure 1. Study patient flow diagram.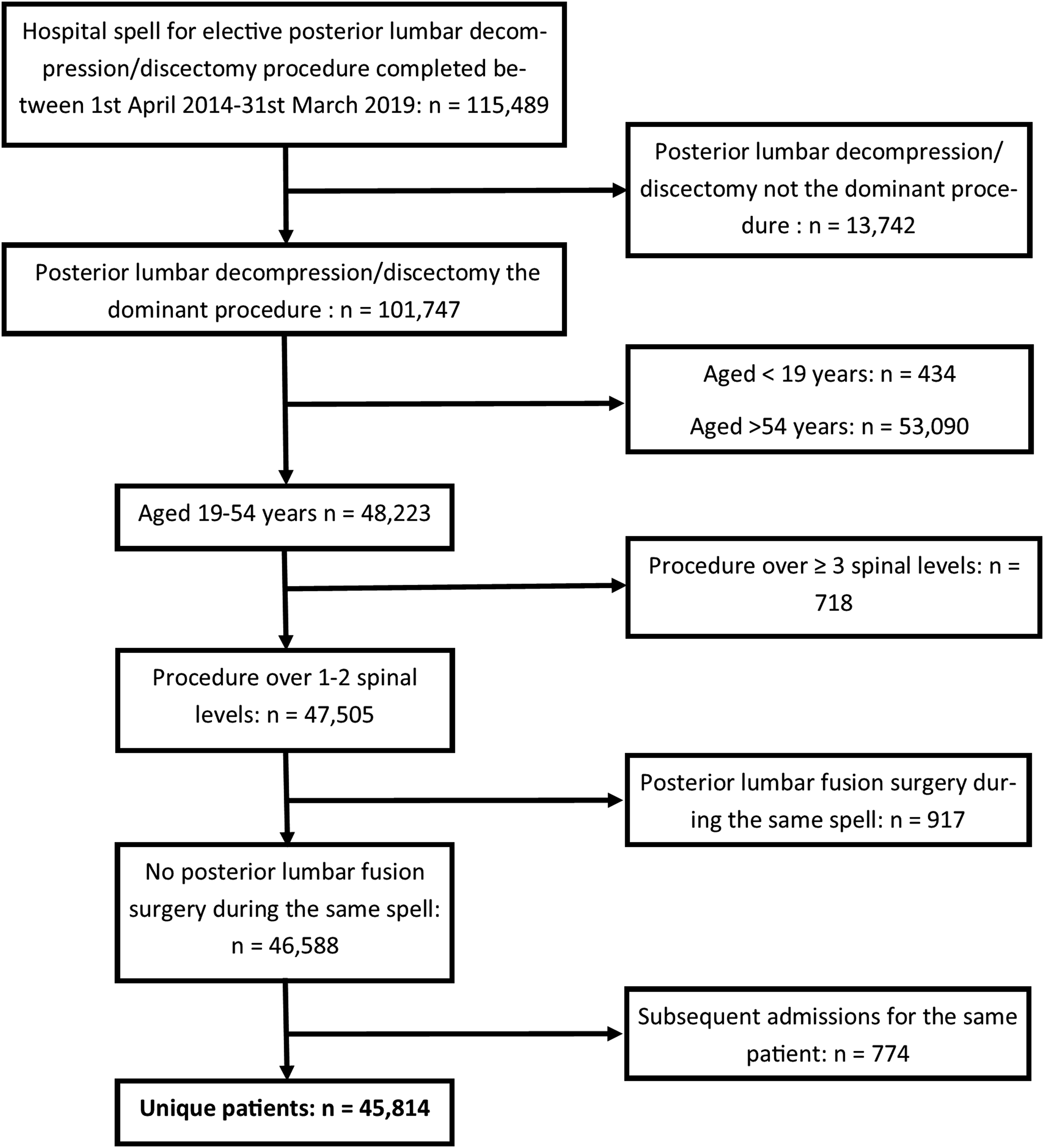
Primary Outcome
1. Emergency hospital readmission with at least one night’s stay within 90 days of discharge. This outcome was chosen to reflect the need for an early readmission related to a complication of surgery.
Secondary Outcome
1. Return for spinal surgery in any subsequent admission within 90 days and within one year of discharge from the index procedure. The OPCS-4 codes listed in Supplementary material Table S2 were used to define the spinal procedures considered as re-intervention procedures. 2. Mortality at one year post discharge. Mortality data were taken from the UK Office for National Statistics (ONS). 3. Back or spinal pain (ICD-10 code M54, R52) reported during emergency hospital admission at 90 days post-surgery. 4. Post-procedural haemorrhage (ICD-10 code T810) or infection (ICD-10 code T814) during emergency readmission within 90 days of discharge.
Exposure
Hospital discharge on the same-day as surgery was the exposure of interest (whether or not they were also admitted on the day of surgery). These patients were compared to those who stayed in hospital for at least one night following surgery. The number of patients who were seen as day case (admitted and discharge on the same-day) are also reported.
In secondary analysis, trusts undertaking these procedures on more than 50 patients during the study period were categorised into those with ≥30% of procedures conducted as same-day discharge and those with ≤10% of procedures conducted as same-day discharge. All other trusts were excluded. This analysis was performed to minimise potential bias due to the same-day discharge and overnight stay groups varying systematically according to unmeasured variables relating to clinical presentation or threshold for intervention or the outcome of surgery precluding same-day discharge. As an example, post-procedural complication identified prior to planned discharge are likely to lead to higher rates of overnight stay, regardless of the planned discharge pathway. As such post-procedural complication recorded during the index procedure are likely to be higher for patients staying overnight than those discharged the same day. Systematic variations in presentation would be less likely across groups of trusts after adjustment for covariates.
Covariates
1. Age in years 2. Sex 3. Financial year of admission 4. One or two spinal levels 5. Haemorrhage (ICD-10 code T810) or infection (ICD-10 codes T814) during the index admission 6. Revision surgery during the index stay. Revision surgery was defined using the OPCS-4 codes V262, V264, V265, V266, V268, V269, V681, V682, V688, V689, V341, V342, V347, V348, V349 7. Obesity (ICD-10 code E66).
Post-procedural haemorrhage or infection recorded during the index stay and revision surgery during the index stay were included as covariates as these are likely to preclude same-day discharge and are therefore potentially confounding.
Data Management and Statistical Analyses
Data were extracted from an encrypted SQL server controlled by NHS England and NHS Improvement and analysed within a secure information technology environment. Data were managed and analysed using standard statistical software: Microsoft Excel (Microsoft Corp, Redmond, WA, USA), Stata (Stata Corp LLC, College Station, TX, USA) and Alteryx (Alteryx Inc, Irvine, CA, USA). Standard descriptive statistics were used as appropriate to the level of the data. Age data were non-normally distributed and are summarised using the median and inter-quartile range (IQR).
Multilevel multivariable logistic regression modelling was used to investigate the association between the exposure variable and the outcomes specified above, with adjustment for the hierarchical nature of the data (patients nested within hospital trusts) and covariates. A two-level intercept only model was constructed with the hospital trust as the random effect. There was no evidence of non-linearity in the relationship between age and the log odds of the primary outcome and so age was modelled as a continuous variable without adjustment. All other variables were categorical. Each of the outcome variables was modelled with same-day surgery or post-surgery overnight stay as the exposure variable and adjustment for the covariates listed above. In secondary analysis the analysis was rerun with the exposure variable being trusts with ≥30% and ≤10% of procedures conducted as same-day discharge. The results of modelling are presented in terms of odds ratios (ORs), confidence intervals (CIs) and tests of significance.
Results
The data extraction process is summarised in Figure 1 identified 45,814 PLDD procedures. In total, 6116 (13.3%) were performed as day-case, 1798 (3.9%) were admitted on the day prior to surgery but discharge on the same-day as surgery, therefore a total of 7914 (17.3%) patients were discharge on the same-day as surgery. In patients not discharged on the day of surgery the median length of stay was 1 days (IQR 1 to 2 days).
The procedures were performed across 103 hospital trusts. Of the 90 trusts that performed more than 50 procedures during the 5 years the same-day discharge rate for each trust is summarised by surgical volume in Figure 2. Same-day discharge rates varied from 87.7% to 0% across trusts. Fourteen (15.6%) trusts had same-day discharge rates above 30% and 57 (63.3%) trusts had same-day discharge rats below 10%. Variation in the proportion of procedures conducted as same-day surgery by hospital trust volume in trusts operating on 50 patients or more during the study period.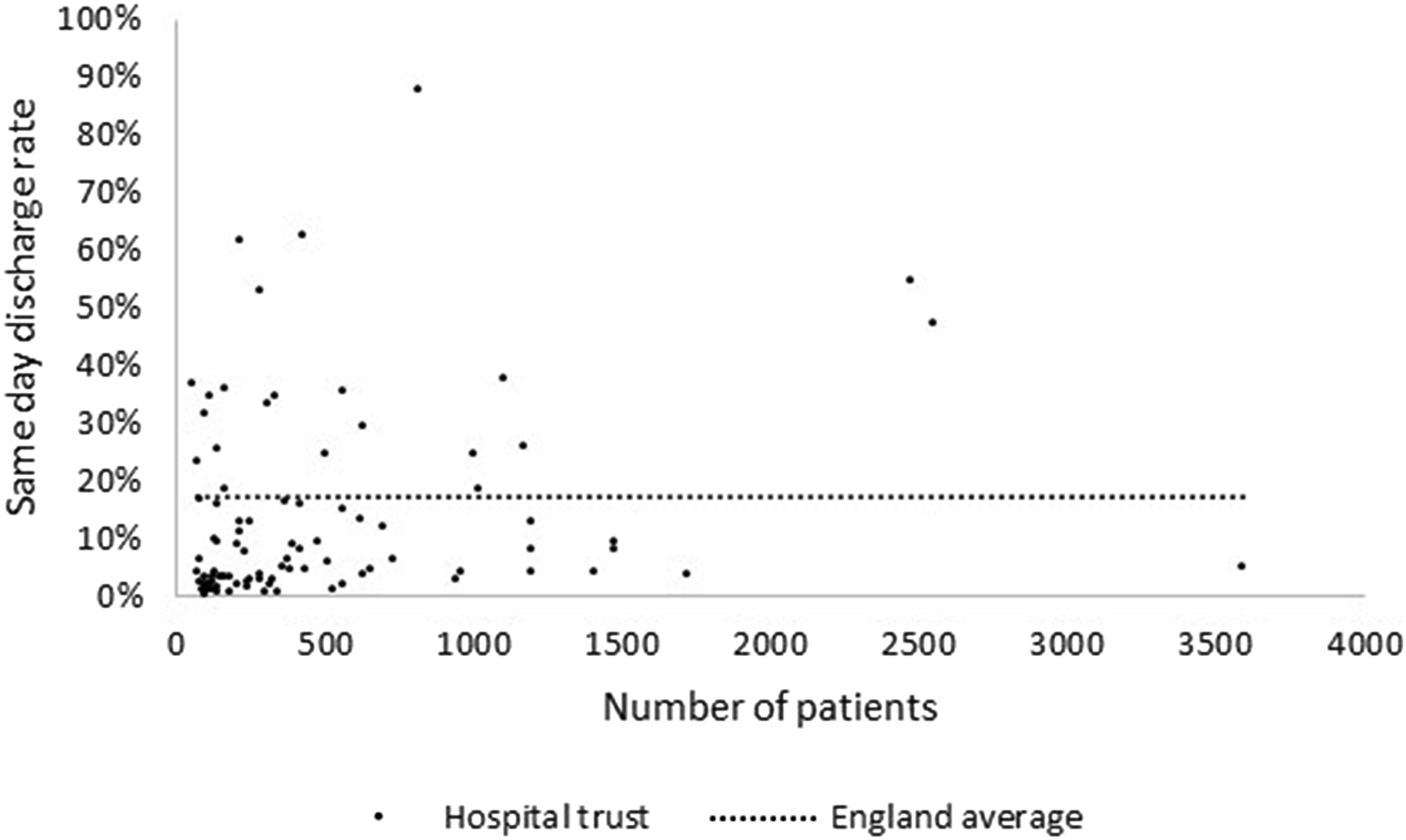
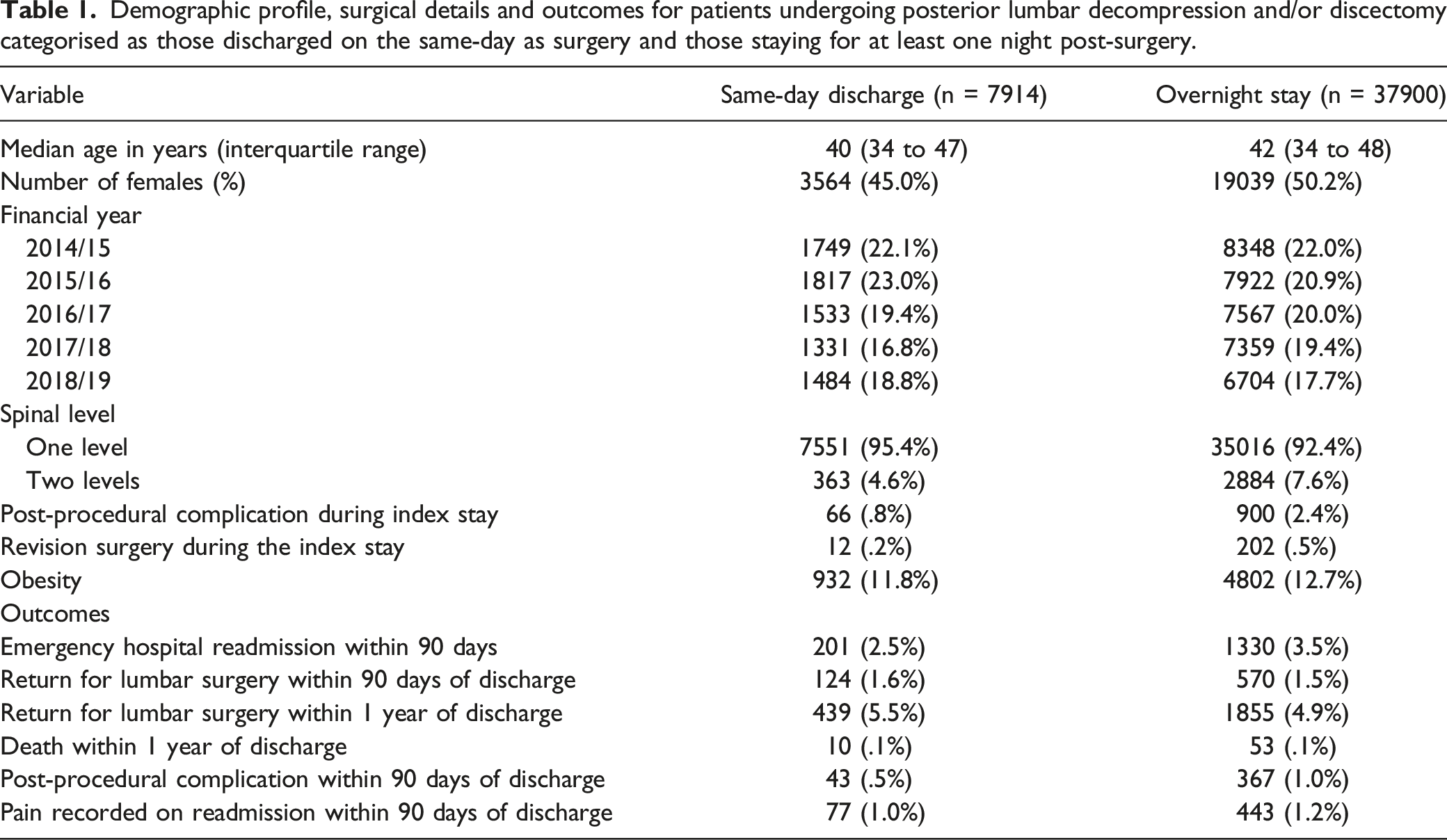
Demographic profile, surgical details and outcomes for patients undergoing posterior lumbar decompression and/or discectomy categorised as those discharged on the same-day as surgery and those staying for at least one night post-surgery.
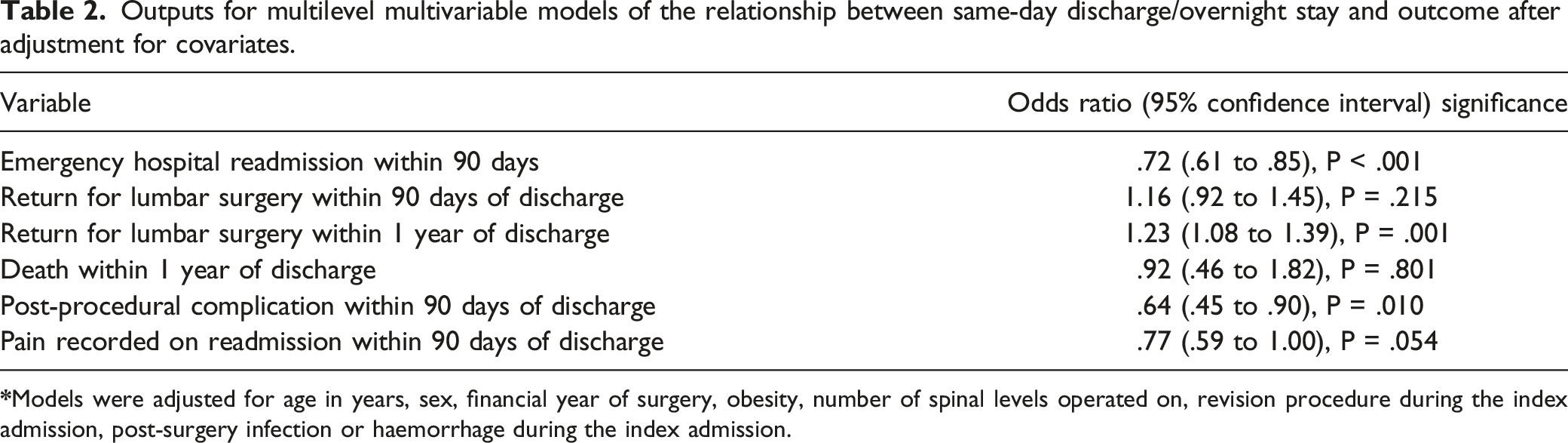
Outputs for multilevel multivariable models of the relationship between same-day discharge/overnight stay and outcome after adjustment for covariates.
Multivariable models of the relationship between trusts with ≥ 30% and ≤ 10% rates of same-day discharges and outcome after adjustment for covariates.
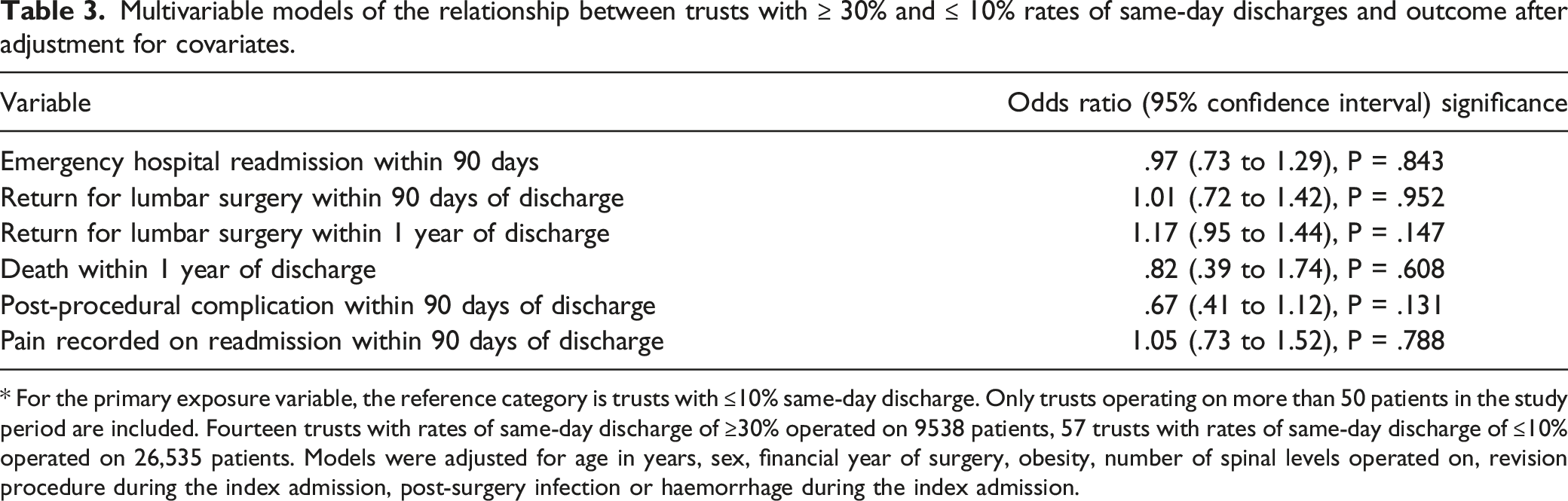
* For the primary exposure variable, the reference category is trusts with ≤10% same-day discharge. Only trusts operating on more than 50 patients in the study period are included. Fourteen trusts with rates of same-day discharge of ≥30% operated on 9538 patients, 57 trusts with rates of same-day discharge of ≤10% operated on 26,535 patients. Models were adjusted for age in years, sex, financial year of surgery, obesity, number of spinal levels operated on, revision procedure during the index admission, post-surgery infection or haemorrhage during the index admission.
Discussion
Reducing length of hospital stay following elective PLDD surgery has the potential to increase patient throughput, minimise risks of nosocomial infection and other adverse outcomes associated with prolonged hospital stay and promote early mobilisation.7,8 However, moving to a same-day discharge model of care, even for patients deemed low risk of adverse outcomes, is far from straightforward. Across all surgical specialties barriers to increasing same-day discharge rates identified in the GIRFT anaesthesia and perioperative medicine national report included a cultural reluctance to change current practice, a lack of same-day discharge infrastructure, a concern that outcomes would be compromised and a sense that same-day discharge rates were already 'optimal' for their patient population. 9 Given these concerns same-day discharge must be shown to be safe. Although same-day discharge is generally viewed favourably by patients, gains in throughput cannot be at the expense of patient safety.10,11
Our study is by far the largest study of its kind to look at the safety of same-day discharge PLDD. 2 It builds on the limited previous work on day-case/same-day discharge for PLDD 2 and other spinal procedures 12 Previous UK-based studies are few.3,4 We found substantial variation in rates of same-day discharge PLDD surgery across England, with a number of trusts performing more than half of PLDD for low risk patients with same-day discharge. We found no strong or consistent evidence that same-day discharge was unsafe in the cohort of patients studied. Although a higher emergency readmission rate for patients discharged earlier may have been expected, this does not appear to be the case, either in general or for specific complications. It is not clear why same-day discharge patients had a higher odds of repeat surgery within 1 year. However, it may be related to some aspect of presentation not accounted for by the covariates studied.
Outcomes for patients seen in trusts with high and low rates of same-day discharge were very similar. Same-day discharge will not be suitable for all patients. In rural areas, or where the surgery is conducted in a specialist centre, travel distances will preclude early discharge for some patients. Nevertheless, there appears to be potential for trusts with low rates of same-day discharge in low risk patients to substantially increase the number of patients discharge on the day of surgery. Increasing awareness of current same-day discharge practice and mechanisms and pathways used to achieve higher rates of early discharge may help more trusts meet these targets. Greater inter-trust collaboration and peer support via existing national clinical improvement initiatives (such as the GIRFT programme and Model Hospital) may be one way of achieving this.13,14 More broadly, improvement in same-day discharge surgery delivery will be dependent on further development of preoperative risk stratification and assessment frameworks, promoting an expectation of same-day-discharge where appropriate and creating the cultural ability and infrastructure to allow same-day discharge as default.
Our study has a number of strengths. By using a national database, we were able to link readmissions to different hospital trusts than the one that performed the index procedure. This is particularly important for specialist procedures such as PLDD which are often performed at some distance from the patient’s local emergency care hospital. The HES database is also relatively complete, with very few missing data, reflecting the link between data entry and provider payment.
The main limitation of our study is that we were unable to comment on clinical presentation directly. Same-day discharge patients could vary systematically from those staying overnight according to disease severity, time from symptom onset to intervention, degree and nature of functional impairment, imaging appearance or underlying health status. Our analysis of data for trusts with high and low rates of same-day discharge surgery will help to minimise such biases since it is unlikely factors related to clinical presentation will have varied systematically across these two groups of trusts. Another potential source of bias was that our definition of same day discharge was based on actual rather than intended management. The consequence of this is that patients with early post-procedural complications will have been more likely to stay in hospital overnight following surgery, and this is apparent in our data. Nevertheless, by employing post-procedural complications and revision surgery during the index admission as a covariate in modelling we have attempted to adjust for this potential bias. As noted above, our analysis of groups of trusts with high and low rates of same-day discharge also help overcome this potentially confounding factor.
Although the HES database includes data for all patient episodes, some data entry inconsistencies have been noted, mostly with regard to differences in coding practice for procedures across trusts. 1 With regard to the current study, we were unable to reliably identify PLDD procedures involving a discectomy and we accept this as a limitation. HES is limited in terms of the types of patient outcomes which can be studied. Data on patient quality of life and other patient reported outcomes would be valuable, allowing a deeper understanding of how procedure choice impacts on patient outcomes and experience. Although we report data on early return to hospital with pain, these are likely to be an under-report. We will only have captured the most severe cases of post-procedural pain; those requiring an emergency hospital admission. Finally, our study is observational and, for the reasons outlined above, is not definitive. A randomised controlled trial should be considered.
Conclusions
In summary, our analysis suggests that same-day discharge for patients undergoing PLDD deemed at low risk of adverse outcomes is safe. Most hospital trusts in England have potential to increase rates of same-day discharge PLDD and this will help to improve service efficiency. As elective spinal surgery in England recovers from the impact of COVID-19, more efficient ways of delivering surgery will help to reduce waiting lists and ensure patients are able to access surgery in a timely manner.
Supplemental Material
Supplemental Material - Safety of Same-Day Discharge Posterior Lumbar Decompression and/or Discectomy: An Observational Study Using Administrative Data From England
Supplemental Material for TSafety of Same-Day Discharge Posterior Lumbar Decompression and/or Discectomy: An Observational Study Using Administrative Data From England by William K. Gray, Jamie Day, Tim W. R. Briggs, and Mike Hutton in Global Spine Journal
Footnotes
Author Contributions
This study was designed and organised by MH, JD, TWRB and WKG. Data cleaning, analysis and writing of the first draft was by WKG, supported by JD and MH. All authors critically reviewed the manuscript and agreed to submission of the final draft.
Acknowledgments
We acknowledge The UK ONS and NHS Digital for permission to use their data in this report. We also thank all staff within individual NHS trusts who collected and entered the data used in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability
This report does not contain patient identifiable data. The data in this report are anonymised. Request for any underlying data will not be granted as the data are calculated from data under licence/data sharing agreement from NHS Digital and/or other data provider where conditions of use (and further use) apply. Copyright© 2013, 2014, 2015, 2016, 2017 re-used with the permission of the Health & Social Care Information Centre. All rights reserved.
Ethical Approval
Ethical approval was not sought for the present study because it did not directly involve human participants. This study was completed in accordance with the Helsinki Declaration as revised in 2013.
Informed Consent
Informed consent was not sought for the present study because it was an analysis of routine clinical data.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.