
Abstract
Study Design
Systematic Review.
Objectives
While substantial research has explored the impact of osteoporosis on patients undergoing adult spinal deformity (ASD) correction, the literature remains inconclusive. As such, the purpose of this study is to synthesize and analyze existing studies pertaining to osteoporosis as a predictor of postoperative outcomes in ASD surgery.
Methods
We performed a systematic review and meta-analysis to determine the effect that a diagnosis of osteoporosis, based on ICD-10 coding, dual-energy X-ray absorptiometry (DEXA) or computed tomography, has on the incidence of adverse outcomes following surgical correction of ASD. Statistical analysis was performed using Comprehensive Meta-Analysis (Version 2) using a random effects model to account for heterogeneity between studies.
Results
After application of inclusion and exclusion criteria, 36 and 28 articles were included in the systematic review and meta-analysis, respectively. The meta-analysis identified greater rates of screw loosening amongst osteoporotic patients (70.5% vs 31.9%, P = .009), and decreased bone mineral density in patients who developed proximal junctional kyphosis (PJK) (.69 vs .79 g/cm2, P = .001). The systematic review demonstrated significantly increased risk of any complication, reoperation, and proximal junctional failure (PJF) associated with reduced bone density. No statistical difference was observed between groups regarding fusion rates, readmission rates, and patient-reported and/or functional outcome scores.
Conclusion
This study demonstrates a higher incidence of screw loosening, PJK, and revision surgery amongst osteoporotic ASD patients. Future investigations should explore outcomes at various follow-up intervals in order to better characterize how risk changes with time and to tailor preoperative planning based on patient-specific characteristics.
Introduction
Adult spinal deformity (ASD) represents a complex constellation of spinal pathologies characterized by abnormal sagittal and/or coronal curvature of the spine. 1 These deviations can lead to significant functional impairment and decreased quality of life, often necessitating surgical correction. Amongst patients undergoing deformity correction, osteoporosis is a common comorbidity that predisposes patients to greater risks of postoperative complications as a consequence of compromised bone quality. 2
The intersection of osteoporosis and ASD surgery presents a significant clinical burden globally. The negative impact of osteoporosis on postoperative outcomes following surgical correction of ASD has been well-documented, spanning from increased risk of hardware failure and pseudarthrosis to postoperative vertebral fractures and reoperation.3,4 Dual-energy X-ray absorptiometry (DEXA) scans are therefore routinely incorporated into patients’ preoperative assessments such that they can be medically optimized with anabolic therapy prior to ASD surgery. 5
While a substantial body of research has explored the impact of osteoporosis on patients undergoing ASD surgery, reports within the literature taken in aggregate remain indeterminate.
The current understanding of osteoporosis as a risk factor in ASD surgery therefore remains inconclusive, further contributing to non-uniform clinical practices in detection and appropriate management. 4 As such, the purpose of this study is to synthesize and analyze the existing array of high-quality investigations pertaining to osteoporosis as a predictor of postoperative outcomes in ASD surgery. Doing so would better clarify contemporary knowledge surrounding the effect of osteoporosis, potentially underscoring the need for standardized preoperative optimization.
Methods
Following the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, we performed a systematic review to determine the effect of osteoporosis on the incidence of adverse outcomes following surgical correction of adult spinal deformities. Informed consent and IRB approval were not necessary given the nature of this study.
The first step involved querying the Medline (PubMed) database from 1990 through August 2022 using the following terms: “osteoporosis” AND “deformity” AND (“outcomes” OR “revision” OR “reoperation” OR “complication”). All English studies, both prospective and retrospective, were included initially that assessed patients with a diagnosis of osteoporosis and reported on the incidence of radiographic, surgical, clinical, and postoperative outcomes. Patients were defined as having a diagnosis of osteoporosis based on ICD-10 coding or a confirmed diagnosis of decreased bone density on DEXA or computed tomography (CT).
We began our initial exclusion filter by eliminating the following studies: systematic reviews, literature reviews, case reports, studies without osteoporotic patients, studies without relevant postoperative outcomes, technique/treatment comparisons, and those where vertebral surgery was due to specific indications such as trauma, neoplasia, or compression fractures. Furthermore, studies with limited sample sizes, which we defined as less than 20 patients, and those without a surgical intervention performed were also removed. After this preliminary exclusion, full-text articles were removed if they were unrelated to adult lumbar spine deformity, cement augmentation was utilized as part of the surgical intervention, or if the study was performed prior to 1990.
The electronic database search and screening were carried out by 2 independent reviewers. Papers were screened based on title, abstract, and full text, and duplicates were removed. Subsequently, the references of full texts were examined to identify any relevant studies missed within our initial query. These were also subjected to the aforementioned screening criteria, ensuring that only articles reporting on outcomes after surgery for ASD were included. After the study selection was finalized, data collection, systematic review, and meta-analysis were performed.
A data collection sheet was created using the Cochrane Consumers and Communication Review Group’s Data Extraction Template for Included Studies. 6 Eligible articles were reviewed by 3 authors who collected the following information: author name, publication year, study type, patient populations, indications for surgery, and the outcomes assessed. Moreover, study outcomes were further classified into the following groups: radiographic outcomes, surgical outcomes, patient-reported outcomes, and other complications. Finally, the risk of bias was assessed using the GRADE (Grading of Recommendations Assessment, Development, and Evaluation) method, and articles were assigned a GRADE of either very low, low, moderate, or high. 7
Statistical Analysis
Statistical analysis was performed using Comprehensive Meta-Analysis (Version 2). Differences in populations between studies were statistically taken into account by utilizing the random effects model. Factoring in standard deviations and sample sizes, the differences between means were calculated and compared between conditions. Categorical and continuous values with reportable standard deviations were included and P-values <.05 were considered significant.
Results
Study Characteristics
The PRISMA diagram outlines the process of study inclusion and exclusion, as well as the reasons for exclusion (Figure 1). Our initial query of the database yielded 1912 records, as well as 53 additional studies that were later identified through searching references of included papers. After the application of exclusion criteria, 1432 records remained, after which 528 were eligible for inclusion after title screening. Of these, 223 articles underwent full-text review, and 36 were ultimately included in this systematic review. 35 were retrospective studies, and one was a prospective study. 28 articles were included in the meta-analysis (Table 1). Study selection process. Characteristics of Studies Focusing on Outcomes After Surgery for Correction of Adult Spinal Deformity. * = included in meta-analysis. PJK/PJF, proximal junctional kyphosis/failure; SVA, sagittal vertical axis; PI-LL, pelvic incidence-lumbar lordosis; LL, lumbar lordosis; TK, thoracic kyphosis; PT, pelvic tilt; C7PL, C7 plumbline; SL, sacral slope; SRS-30, scoliosis research society deformity sequence questionnaire; ODI, Oswestry Disability Index.
Risk of Bias and Quality of Evidence
The level of evidence was determined for each study using the Journal of Bone and Joint Surgery schema. 8 One article was characterized by level II evidence, 24 by level III evidence, and 11 by level IV evidence. The GRADE guidelines were used to assess the quality of evidence, 7 wherein 25 studies were deemed to have very low-quality evidence, and 11 with low quality.
Radiographic Outcomes
Proximal Junctional Kyphosis and Failure
Summarized Results of Studies Focusing on Radiographic Outcomes.
* = included in meta-analysis.
┼ = statistically significant relationship between outcome and osteoporosis (P < .05).
PJK/PJF, proximal junctional kyphosis/failure; SVA, sagittal vertical axis; PI-LL, pelvic incidence-lumbar lordosis; LL, lumbar lordosis; TK, thoracic kyphosis; PT, pelvic tilt; C7PL, C7 plumbline; SL, sacral slope.
In their retrospective case series of 160 patients who underwent long spinal fusion to the sacrum for ASD, Park et al demonstrated that while osteoporosis was not a significant risk factor for the development of PJK, it was a significant predictor of PJF (P < .001). 15 In fact, all 4 articles that investigated PJF found that patients with poor bone stock were at higher risk for developing this complication.12,15,16,22 Kyrölä et al, Park et al, and Yagi et al all established a higher risk of PJF amongst patients with osteoporosis (P = .018, P = .03, and P < .01).12,16,22
Screw Loosening
Five studies assessed the relationship between osteoporosis and screw loosening after surgical correction of ASD, with 3 identifying low BMD as a risk factor.23-25 Yuan et al and Banno et al’s retrospective studies found that patients who experienced screw loosening had lower average T-scores (P = .002 and P = .005, respectively).23,25 Xu et al reported that 20.6% of patients had a diagnosis of osteoporosis in the non-screw loosening group compared with 75.0% in the screw loosening group in their cohort of patients who underwent instrumentation for degenerative lumbar scoliosis (P < .001). 24 In contrast, Kim et al and Nakazawa et al did not report differences in T-scores between patients with and without screw loosening in their respective retrospective studies.11,26
Fusion Rate and Pseudarthrosis
One study reported on the relationship between bone mineral density and fusion rates while the other reported rates of pseudarthrosis, with neither study successfully establishing significance.19,27
Implant Fracture
Two studies investigated the relationship between bone mineral density and the risk of rod fracture,12,28 while 1 study looked at pedicle screw fracture rates. 29 Neither Kyrölä et al nor Lertudomponwanit et al were able to establish an association between osteoporosis and rod breakage.12,28 O’Leary et al, however, found that osteoporotic patients were at significantly increased risk of pedicle screw fracture in their matched cohort analysis patients with long segmental pedicle screw constructs (T-scores: −1.73 ± .76 vs −.58 ± 1.12, P = .02). 29
Cage Subsidence and Adjacent Fractures
Kim et al conducted a study overviewing cage subsidence and adjacent fractures following surgical correction of lumbar degenerative kyphosis but found that neither outcome was more prevalent amongst osteoporotic patients. 27
Spinopelvic Parameters
Other radiographic outcomes assessed in 4 studies included coronal distance of C7 plumbline to the central sacral line (C7PL), pelvic incidence-lumbar lordosis (PI-LL), sagittal vertebral axis (SVA), pelvic tilt, thoracic kyphosis, sacral slope, and sagittal decompensation.22,26,27,30
The one study examining changes in C7PL was a single-center, retrospective review by Ploumis et al In this study, 54 patients who underwent long spinal fusion with ASD demonstrated that osteoporosis was a statistically significant factor for the changes of coronal C7PL (F = 4.99, P = .032). 30
Two studies studied the relationship between osteoporosis and PI-LL in patients with ASD. Nakazawa et al assessed sufficient correction, defined as postoperative PI-LL mismatch <10°, and found that patients with sufficient compared to insufficient correction had significantly different pre-operative BMDs (1.04 ± .31 vs .74 ± .17, P = .03), but not T-scores (−1.5 ± 1.3 vs −1.6 ± 1.0, P = .86). 26 The other study by Yagi et al did not find a difference in PI-LL between the mildly low BMD group and the severely low BMD group. 22
Three papers assessing SVA all determined that osteoporosis was not a significant risk factor for this postoperative radiographic parameter.22,26,27 In addition to SVA, Kim et al investigated other spinopelvic parameters such as lumbar lordosis, pelvic tilt, thoracic kyphosis, sacral slope, and sagittal decompensation in 40 patients with lumbar degenerative kyphosis, none of which were significantly associated with osteoporosis. 27 The other paper by Yagi et al that examined the relationship between pelvic tilt and osteoporosis was also unable to find a significant difference. 22
Complications
Overall Complications
Summarized Results of Studies Focusing on Rates of Various Complications.
* = included in meta-analysis.
┼ = statistically significant relationship between outcome and osteoporosis (P < .05).
Revision Surgery
In total, 4 studies assessed the impact of osteoporosis on rates of revision surgery.2,3,33,34 Gupta et al and Taliaferro both found that osteoporosis significantly increases the likelihood of revision surgery in patients with ASD (P = .013 and P < .001, respectively).2,34 In Puvanesarajah et al’s PearlDiver database review of 2293 patients who underwent ≥8 level primary thoracolumbar posterolateral fusion, osteoporosis was significantly more prevalent in patients who had revisions at 1, 2, 3, 4, and 5 years postoperatively compared to patients who did not undergo reoperation (P < .005 for all). 33 Varshneya et al’s regression analysis of a cohort of Medicare patients undergoing ASD correction identified osteoporosis as an independent risk factor for revision surgery within 1 and 2 years (P = .0036 and P < .001), but not at 90 days or 6 months after surgery. 3
Readmission Rates
Two studies examined the interplay between osteoporosis and readmission following surgery for ASD.3,34 Taliaferro et al’s univariate analysis identified osteoporosis as a significant risk factor for readmission within both 30 days and 90 days after index surgery (P < .01 for both), 34 while Varshneya et al was unable to establish a significant relationship between those who had osteoporosis compared to those who did not at 30, 60, and 90 days after discharge. 3
Neurologic Injury
Two studies assessed the relationship between osteoporosis and neurologic injuries following surgery for ASD.3,12 Neither Kyrölä et al nor Varshneya et al established a significant relationship between these 2 variables.3,12
Surgical and Patient-Reported Outcomes
Surgical Outcomes
Summarized Results of Studies Focusing on Surgical, Hospital, and Patient-Related Outcomes.
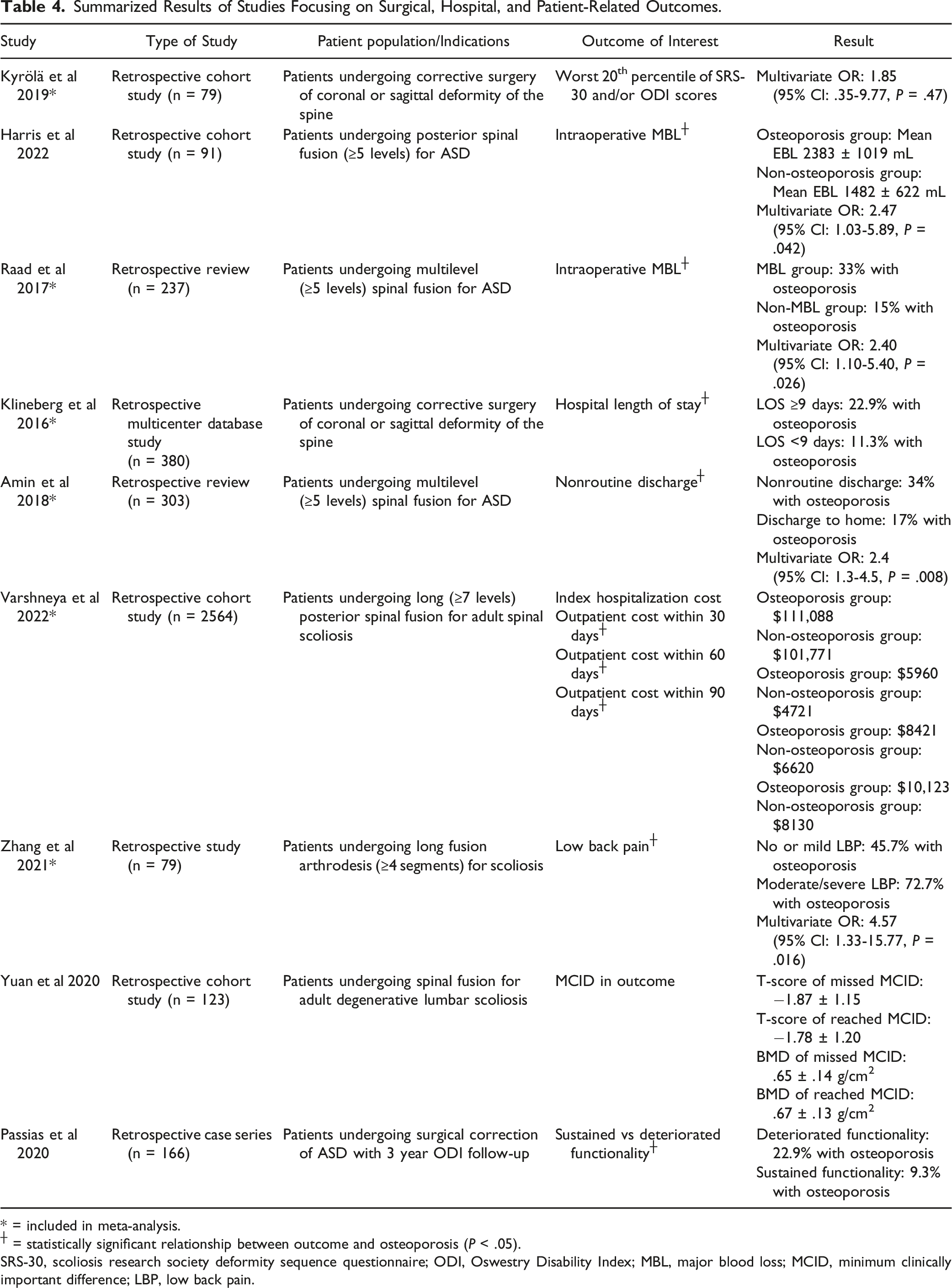
* = included in meta-analysis.
┼ = statistically significant relationship between outcome and osteoporosis (P < .05).
SRS-30, scoliosis research society deformity sequence questionnaire; ODI, Oswestry Disability Index; MBL, major blood loss; MCID, minimum clinically important difference; LBP, low back pain.
Intraoperative Blood Loss
Harris et al and Raad et al reported on the relationship between osteoporosis and major blood loss (MBL) during multilevel fusion for ASD, and both established that lower bone mineral density was predictive of increased risk of MBL intraoperatively (P = .042 and P = .026, respectively).37,38
Functional Outcomes
Four studies assessed clinical outcomes in patients with ASD including functionality, level of back pain postoperatively, clinical improvement, and patient satisfaction.12,39-41 Higher rates of osteoporosis were identified in patients with a decline in functionality postoperatively 39 and those with persistent moderate/severe low back pain. 40 However, Yuan et al did not find a difference in T-score or BMD between patients who missed and reached a minimum clinically important difference. 41 Lastly, being in the worst 20th percentile of scoliosis research society deformity sequence questionnaire (SRS-30) and/or Oswestry Disability Index scores were not associated with osteoporosis. 12
Meta-Analysis Results
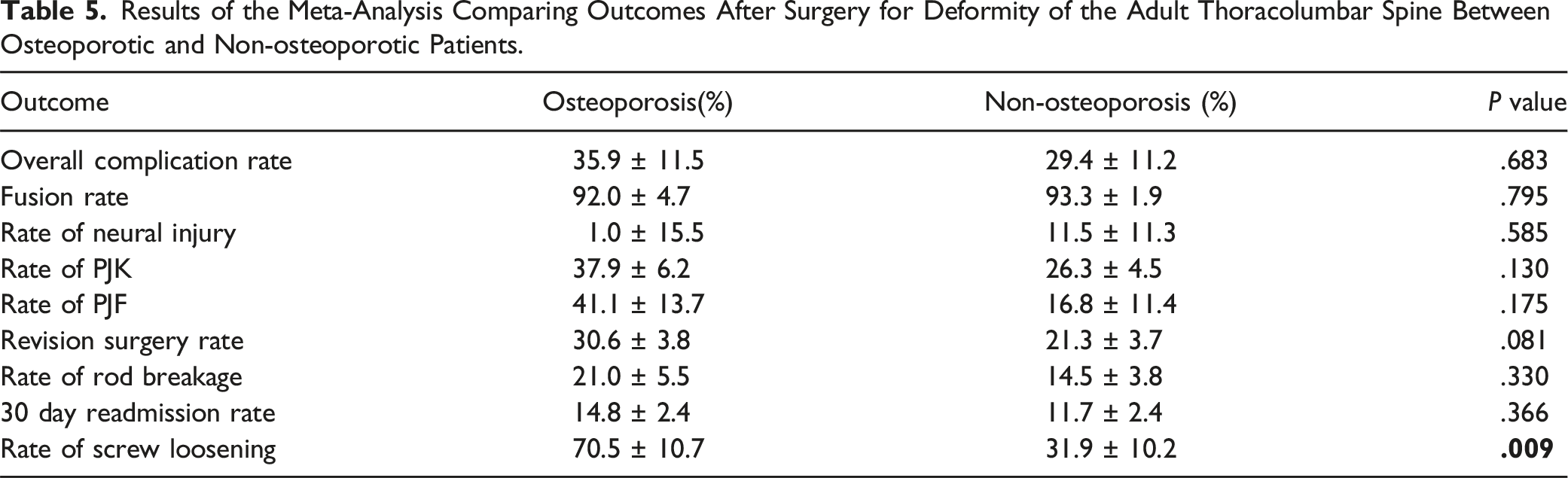
Results of the Meta-Analysis Comparing Outcomes After Surgery for Deformity of the Adult Thoracolumbar Spine Between Osteoporotic and Non-osteoporotic Patients.
Results of the Meta-Analysis Comparing Bone Quality Between Cases and Controls Where all Patients Underwent Pelvic Fixation.

Results of the Meta-Analysis Comparing Bone Quality Between Cases and Controls Where all Patients Underwent Fixation of T10 and Beyond.

Table 6 reports on the differences in bone quality between cases and controls for PJK and screw loosening using average T-scores. Included papers investigated patients who underwent fixation down to the pelvis to maintain consistency in comparisons. Two studies compared T-scores between PJK and non-PJK cohorts and found that patients who developed PJK had significantly lower T-scores (−2.597 ± .476 vs −1.796 ± .461, P < .001).10,11 Similarly, 2 studies were pooled to assess screw loosening and found that patients who developed this complication had significantly lower T-scores than their counterparts (−2.269 ± .169 vs −1.479 ± .165, P < .001).11,25,26
Table 7 demonstrates differences in T-scores between patients who developed PJK and those who did not after fixation of the T10 segment and beyond. There were an insufficient number of studies available to assess rates of screw loosening in this cohort. Across 4 studies, T-scores were significantly lower amongst patients who developed PJK than those who did not (−2.067 ± .045 vs −1.132 ± .048, P < .001).9,10,13,18
Discussion
Herein, we conduct a systematic review and meta-analysis to assess the impact of osteoporosis on outcomes following ASD surgery. In contrast with degenerative conditions, the management of spinal deformities often involves much lengthier and technically complex surgeries, often with significant complication rates both intraoperatively and postoperatively.3,31,44 Our meta-analysis identified a 30.6% revision rate in osteoporotic patients compared with 21.3% in non-osteoporotic patients across a pooled cohort of 5256 patients, but this difference was not statistically significant (P = .081). Notably, however, all 4 papers in the systematic review that reported on this outcome reported that osteoporosis was a risk factor for the reoperation of ASD.2,3,33,34 With the prevalence of osteoporosis ranging from 16%-61% across these 4 studies, and a reoperation rate between 4.2%-32.1% within a range of 90 days to 5 years, it is possible that these differences may have skewed the results of the meta-analysis. Moreover, Puvanesarajah et al investigated a cohort of 2293 patients who underwent multilevel (≥8 segments) thoracolumbar posterolateral fusion for ASD and found that a significantly greater proportion of patients who underwent reoperation at 1, 2, 3, 4, and 5 years after the index surgery were osteoporotic. Osteoporosis was furthermore a strong independent predictor of 5-year revision rates on their multivariate analysis (OR: 1.98, 95% CI: 1.60-2.46, P < .0001). 33 These results indicate that future investigations into not just reoperation rates, but any outcome after surgery, should be stratified by follow-up period.
Puvanesarajah et al also identified instrumentation failure as the most common reason for reoperation at 5 years, which was present in over 50% of patients who required reoperation. 33 This suggests that the impaired biomechanical strength of osteoporotic bone may present a significant surgical and financial burden. Osteoporosis is a metabolic bone disease that affects the microarchitecture and structural integrity of bone throughout the body, which often means that obtaining sufficient fixation is increasingly challenging in this population.45,46 A large review performed by Akinturk et al in 2022 of 79 articles with a total of 26 207 patients reported an overall complication rate of 34.5%, the most common being hardware failure, PJK, and distal junctional kyphosis. 47 In our study, 2 of 4 papers found that patients with osteoporosis were at significantly increased risk of developing any perioperative or postoperative complication,31,32 and the meta-analysis corroborated that 35.9% of osteoporotic patients experienced complications compared to 29.4% of non-osteoporotic patients (Table 5). In Varshneya et al’s large retrospective database study of 2564 patients, osteoporosis was identified in 61.0% of patients using ICD-9 coding. Although multivariate regression analysis ultimately did not identify osteoporosis as a significant risk factor for the development of postoperative complications, osteoporotic patients had significantly higher rates of select comorbidities, including cancer, history of cerebrovascular accident, and peripheral vascular disease, as well as an overall greater Charlson comorbidity index (P < .0001). 3 Though not directly related to outcomes after spine surgery, these findings highlight the unique challenges that both surgeons and patients face when faced with the interplay between reduced bone mineral density and surgical correction of ASD.
Though it remains unclear to what degree overall complication rates are affected by poor bone stock, we established that rates of pedicle screw loosening do significantly differ. Given the heterogeneity across results, screw loosening was analyzed 2 different ways: the first was based on rates between osteoporotic and non-osteoporotic patients (Table 5), and the second was based on differences in T-scores between patients with and without screw loosening (Table 6). We were able to identify differing rates of screw loosening between osteoporotic and non-osteoporotic patients (70.5% vs 31.9%, P = .009), which is consistent with the current literature.45,48-51 Nonetheless, the clinical significance of screw loosening has not been fully elucidated. In Yuan et al’s retrospective cohort study of 130 patients who underwent a minimum of 5-level fusion for lumbar scoliosis, osteoporosis was identified as a significant risk factor for pedicle screw loosening within the 12-month follow-up period (OR: 2.40, P = .001). However, patients experienced improvements in visual analog scale (VAS) back, VAS leg, SRS-22, and ODI scores after surgery irrespective of the presence or absence of pedicle screw loosening. 23 Several other investigations have shown that functional outcome scores were not affected by pedicle screw loosening.49,52 Other investigations have reported that functional outcomes may be affected by screw loosening, but these were in degenerative lumbar conditions which are distinct from ASD.48,50,53 However, Banno et al compared risk factors and outcomes of iliac screw loosening after ASD correction in 72 patients and reported that patients who developed loosening did not experience improvements in their ODI scores at the 2-year follow-up compared with patients whose screws remained appropriately fitted. 54 These findings indicate that more granular investigations into which patients are at higher risk of subpar clinical improvement are necessary, regardless of the presence or absence of certain radiographic signs.
In addition to screw loosening, our meta-analysis found that patients who developed PJK postoperatively had lower bone mineral densities (BMD) than their non-osteoporotic counterparts (.69 ± .03 g/cm2 vs .79 ± .01 g/cm2, P = .001). Proximal junctional kyphosis is a subtype of adjacent segment disease and is generally defined radiographically by the presence of kyphosis greater than 10° between the lower endplate of the upper instrumented vertebra (UIV) and the upper endplate of the vertebra 2 levels above the UIV.9,10 Proximal junctional kyphosis can result in persistent or recurrent postoperative pain, instability, and neurological deficit, and it is thought to be related to overly rigid instrumentation that results in increased load concentration at the UIV and subsequently accelerated degeneration and kyphosis.17,18,20 The diminished ability of osteoporotic bone to accommodate these increased forces, coupled with the fact that patients with osteoporosis are frequently comorbid with sarcopenia, often exacerbates preexisting propensity for developing adjacent segment disease, or specifically PJK.10,55 A 2022 systematic review and meta-analysis by Han et al overviewing 2388 patients who underwent surgical correction of ASD identified osteoporosis as a significant independent risk factor for the development of PJK (OR: 2.86, 95% CI: 1.64-4.99, P = .0002). 56 The authors also identified overcorrection of lumbar lordosis as a risk factor (OR: 2.20, 95% CI: 1.41-3.42, P = .0005). Specifically, a mismatch between pelvic incidence and lumbar lordosis is a known contributing factor to adjacent segment degeneration, as well as to reduced health-related quality of life scores, both of which are also more prevalent amongst patients with osteoporosis.57-59 These findings highlight the need for careful surgical planning informed by preoperative spinopelvic parameters to minimize the risk of adjacent segment degeneration while still attaining sufficient spinal alignment.
These spinopelvic parameters are frequently assessed pre- and postoperatively and include the coronal distance of C7 plumbline to the central sacral line (C7PL), pelvic incidence-lumbar lordosis (PI-LL), sagittal vertebral axis (SVA), pelvic tilt, thoracic kyphosis, sacral slope, and sagittal decompensation. Of these, 1 paper investigating C7PL established osteoporosis as a risk factor for coronal plane changes, 30 and another found that sufficient correction of PI-LL to <10° was associated with a higher preoperative BMD (P = .03), but not T-score (P = .86). 26 Although our 3 papers investigating SVA correction were unable to establish osteoporosis as a risk factor, sagittal alignment is known to be important for maintaining painless posture, and the compensatory biomechanical processes triggered by sagittal imbalance have been linked with reduced quality of life measures.12,60,61 Nakazawa et al reported that ODI scores at the final follow-up were significantly higher amongst patients who achieved a postoperative SVA increase of <40 mm compared to those with an increase of ≥40 mm. 26 Some investigations suggest that longer fusions may be more suitable for attaining favorable spinopelvic measurements, highlighting the complex interplay between bone quality, objective measurements of the spine, and functional outcomes.26,62,63 As such, it is difficult to draw conclusions regarding the impact of osteoporosis on postoperative spinopelvic parameters from this limited sample of patients, and future investigations utilizing a large cohort are warranted.
While our systematic review and meta-analysis pertaining to the impact of osteoporosis on outcomes after surgical correction of ASD highlights that reduced bone quality indeed may influence select outcomes, our study is not without limitations. Firstly, the retrospective nature of the majority of included studies limits conclusions that may be drawn given the reduced quality and grade of evidence. When performing the meta-analysis, different studies often tracked outcomes using different follow-up periods, which skewed the prevalence of these outcomes. For example, it is unsurprising that reoperation rates would significantly differ between a 90-day vs five-year postoperative period — therefore, more granular data from each study about the number of patients who underwent reoperation within each time interval would provide a more robust analysis of the role osteoporosis might play as a risk factor. To mitigate this concern, we sought to include papers with a minimum of 1-year follow-up or a mean follow-up interval of at least 1 year when this information was available. There were several papers that did not include this information, making uniform application of this criterion more difficult. For this reason, some of the results of the meta-analysis should be interpreted with caution, and this assessment highlights the need for a more uniform method of collecting outcomes based on follow-up length. Lastly, as there is no method in which T-scores and BMD can be retrospectively converted, individual analyses were performed based on measurement technique, which may have diminished the statistical power underlying some of the meta-analysis results given the inability to pool these patients. It may be helpful for future investigations to report both sets of measurements.
Conclusion
This systematic review and meta-analysis sought to determine the impact of osteoporosis as a risk factor for adverse outcomes following surgical correction of ASD. Reduced bone quality was significantly associated with an increased risk of screw loosening, and may also impact rates of reoperation, the development of PJF, and perioperative complications such as increased intraoperative blood loss. In contrast, osteoporosis did not seem to increase the risk of pseudarthrosis, PJK, or hospital readmission. Spinopelvic parameters such as pelvic incidence-lumbar lordosis and the sagittal vertical axis are frequently assessed pre- and postoperatively to determine whether surgical correction was sufficient, but we were unable to identify differences in these measurements between osteoporotic and non-osteoporotic patients. Our findings highlight the need for continued investigation into the magnitude of osteoporosis’s impact on surgical outcomes, especially at various follow-up intervals, with the goal of optimizing medical management and surgical techniques to reduce the frequency of complication events in this vulnerable population.
Supplemental Material
Supplemental Material - The Effect of Osteoporosis on Complications and Reoperation Rates After Surgical Management of Adult Thoracolumbar Spinal Deformity: A Systematic Review and Meta Analysis
Supplemental Material for The Effect of Osteoporosis on Complications and Reoperation Rates After Surgical Management of Adult Thoracolumbar Spinal Deformity: A Systematic Review and Meta Analysis by Elizabeth A. Lechtholz-Zey, Brandon S. Gettleman, Mina Ayad, Emily S. Mills, Hannah Shelby, Andy Ton, Ishan Shah, Michael M. Safaee, Jeffrey C. Wang, Ram K. Alluri, and Raymond J. Hah in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Elizabeth A. Lechtholz-Zey, Brandon S. Gettleman, Mina Ayad, Emily S. Mills, Hannah Shelby, Andy Ton, and Ishan Shah have nothing to disclose. Michael M. Safaee has received grant funding from ATEC, NuVasive, DePuy Synthesis for lectures and presentations, and financial support from USC for attending meetings. Jeffrey C. Wang has received intellectual property royalties from Zimmer Biomet, NovApproach, SeaSpine, and DePuy Synthes. Raymond J. Hah has received grant funding from SI bone, consulting fees from NuVasive, and support from the North American Spine Society to attend meetings. Ram K. Alluri has received grant funding from NIH, consulting fees from HIA Technologies, and payment from Eccentrial Robotics for lectures and presentations.
IRB Statement
Institutional review board (IRB) approval was not required as no patient information was collected for this study.
Supplemental Material
Supplemental material for this article is available online
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.