
Abstract
Study Design:
Retrospective case control study.
Objectives:
Adjacent-level ossification development (ALOD) is a distinct form of adjacent segmental degeneration that has been recognized to occur after anterior cervical discectomy and fusion (ACDF). It is unclear whether ACDF with plate versus standalone has an effect on rates of ALOD. This retrospective case-control study aims to assess the rate of ALOD in a large series of patients undergoing ACDF with and without plate and factors causing ALOD.
Methods:
Data was collected for patients undergoing ACDF from January 2009 to July 2016. Data collected was from multiple centers and included demographic data, surgical data, radiological imaging at time of surgery, and serial follow-up imaging. The radiology for ALOD was independently reviewed. Cohorts were divided into ACDF with plate (Group P = plate) and ACDF without plate (Groups S = standalone) and outcomes were compared.
Results:
There were 260 patients with 138 (53%) in Group P and 122 (47%) in Group S. ALOD was observed in 15.3% of patients overall, 29% in group P and 2.8% in group S (P < .001). Following multivariate adjustment, statistically significant association was found between use of plate and ALOD (odds ratio = 12.8, 95% confidence interval = 3.52-45.45, P < .001). Plate-to-disc distance <5 mm was significantly associated with ALOD (odds ratio = 13.5, 95% confidence interval = 3.83-47.62, P < .001).
Conclusion:
The use of anterior plate with ACDF was associated with ALOD. Plate-to-disc distance <5 mm was significantly associated with ALOD even after adjustment for confounding factors. We conclude utilization of standalone cages or cages with plate with more than 5 mm distance from adjacent disc to minimize ALOD.
Introduction
Adjacent segment disease (ASD) is a widely recognized pathology in anterior cervical spine surgery. Adjacent-level ossification development (ALOD) is a distinct type of adjacent segment pathology resulting in adjacent-level marginal bone osteophyte formation along the anterior longitudinal ligament (ALL) that has been recognized to occur after anterior cervical discectomy and fusion (ACDF). 1
ALOD was first described as early as the 1980s by Gore et al, 1 who noted anterior osteophyte formation was more frequent in their series of 90 patients who had undergone anterior cervical spine fusion surgery, although the modern terminology was termed by Park et al 2 in 2005. The underlying pathophysiology of ALOD is not well understood but has been postulated due to the proximity of placement of the plate or an oversized plate in relation to the adjacent intervertebral disc, 3 or due to excessive dissection along the anterior longitudinal ligament. 2,4 Some studies have suggested that ALOD is associated with recurrent pain and progression of spondylosis cephalad and caudal to the ALOD segments requiring additional surgery. 1
The literature has numerous studies assessing the incidence of ALOD in ACDF with a plate and its associated risk factors, but there are few studies on the incidence of ALOD in standalone ACDF (ie, without a plate). The popularity of the standalone ACDF has increased over the years. Plate placement is classically thought to result in higher fusion rates, better lordosis, greater disc height, and lower subsidence rates. 5 However the use of a plate system is not innocuous, with screw pullout, loosening of plate, hardware breakage, irritation of esophagus, and adjacent structures being reported. 6 Therefore, this study aims to identify and compare the rate of ALOD in patients undergoing ACDF with and without a plate.
Materials and Methods
The study was a retrospective analysis of prospectively collected data from multiple centers and involved 3 spine surgeons. It included all consecutive patients undergoing primary ACDF with and without plate between January 2009 and July 2016 for cervical radiculopathy and/or myelopathy not responding to conservative measures. The surgeons were using plate in the early part of the study and without plate in the recent years. The technique used by all 3 surgeons was a standard right-sided Smith-Robinson approach to the prevertebral space, and identification of the pathological level on X-ray. All 3 surgeons utilized retractors and Caspar pins for distraction. Two of the surgeons used microscope for magnification, while one of the surgeons used loupe magnification. Standard thorough discectomy was performed with combination of pituitary rongeur, curettes, and Kerrison rongeur with meticulous preparation of the endplates with curettes. The posterior longitudinal ligament was divided and dura fully visualized and placement of the implant.
Ethics approval was obtained and approved through the Human Research Ethics Committee as well as site-specific approval for the centers involved.
The exclusion criteria included surgery for trauma, diffuse idiopathic skeletal hyperostosis, ankylosing spondylitis, spinal malignancy, spinal infection, posterior fusion construct to support anterior cervical discectomy and fusion, and pregnancy. Any adjacent level with ALOD on preoperative imaging was not included, as this is not considered ALOD.
Data collection was conducted by the primary investigator and reviewed by 2 independent analysts including a statistician. Baseline demographics including sex, age, other medical conditions, and surgical data including cervical level ACDF performed, number of levels, plate used or not, type of cage and plate (if applicable), and bone substitute or graft type used.
With regard to the type of graft, the type of cage, and type of plate used, there were too many variables to make a statistically significant analysis and hence was excluded.
It was routine for the surgeons to obtain X-rays preoperatively and postoperatively at regular intervals. Radiographic data thus obtained was analyzed. The diagnosis of ALOD and grading was done by an independent senior neurosurgical trainee (CH) and an independent spinal fellowship–trained neurosurgeon (PR), and in cases where there were differences these were resolved by the senior spine surgeon (RM). The measurement of plate to the adjacent disc distance (PDD) was performed on lateral radiological imaging using measurements available on the radiology software.
Primary outcome aims to review the ALOD rates based on preoperative radiographic data and at follow-up at 3, 6, 12, and 24 months. The grading system for ALOD is as described by Park et al 2 (Figure 1).

Radiographs illustrating ALOD classification as described by Park et al. 2 Grades (left to right): 0, 1, 2, and 3.
Data analysis and statistical evaluation was conducted using IBM SPSS Statistics 22 (IBM Corporation, Armonk, NY), including age, cervical level, gender, and numbers of level fused. Descriptive statistics was performed for all parameters tested (mean ± standard deviation or percentage). Gaussian normality distribution was verified using the D’Agostino-Pearson omnibus test. Chi-square test was used for the comparison of categorical data. Multivariate logistic regression analysis identified independent risk factors correlated with ALOD. Statistical significance was assumed for a P value <.05.
Power Calculation
A power analysis was performed with primary endpoint of ALOD in ACDF with plate versus ACDF without plate. With an assumed event rate of 5% in the control group and for an absolute margin of 15%, 150 patients were required (75 patients in each group) to provide 80% power, assuming 5% attrition.
Results
There were 260 patients with 371 levels in the study from all the centers. A total of 51.2% were males and 48.2% were females. A total of 53.5% patients underwent ACDF with plate insertion and 46.5% underwent ACDF without plate insertion (Table 1). Of these, 174 patients were single-level (66.9%), 76 patients were 2-level (29.2%), and 10 patients were 3-level ACDF (3.8%).
Descriptive Statistics of Studied Population.
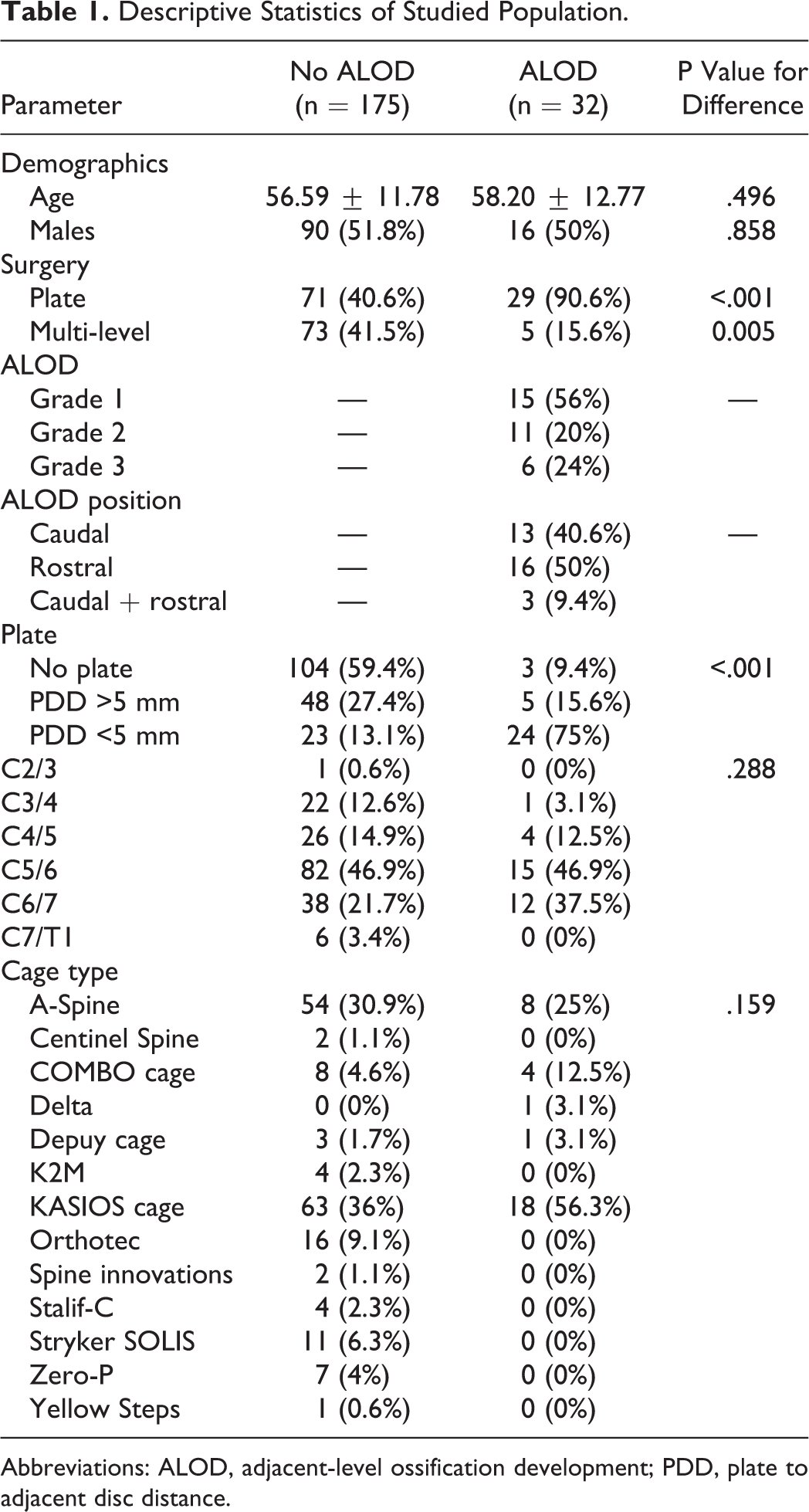
Abbreviations: ALOD, adjacent-level ossification development; PDD, plate to adjacent disc distance.
ALOD
Two hundred and seven out of the 260 patients had sufficient information for univariate and multivariate data analysis. The postoperative radiograph was obtained at a mean of 14.5months (SD = 8.2-25.3).
There was good interrater agreement on ALOD grading (Cohen’s κ interrater agreement was 0.88). This is the proportion of agreement over and above chance agreement. Based on guidelines from Altman 7 and adapted from Landis and Koch 8 , this represents almost perfect strength of agreement.
The total ALOD rate was 15.3% (32/207) with 46.9% Grade 1 ALOD (15/32 patients), 34.4% Grade 2 (11/32 patients), and 18.8% were Grade 3 (6/32 patients). Fifty percent of ALOD (16/32) present was rostral to the fused segment, 40.6% was caudal (13/32), while 9.4% was present both rostral and caudal (3/32).
ALOD was observed in 2.8% of patients undergoing ACDF without plate compared with 29% of ALOD observed in patients undergoing ACDF with plate, with the difference being statistically significant on univariate analysis (P ≤ .001; Table 2). Univariate analysis did not find any significant difference with regard to age, gender, or the level of surgery.
Univariate Analysis of ALOD Outcomes.
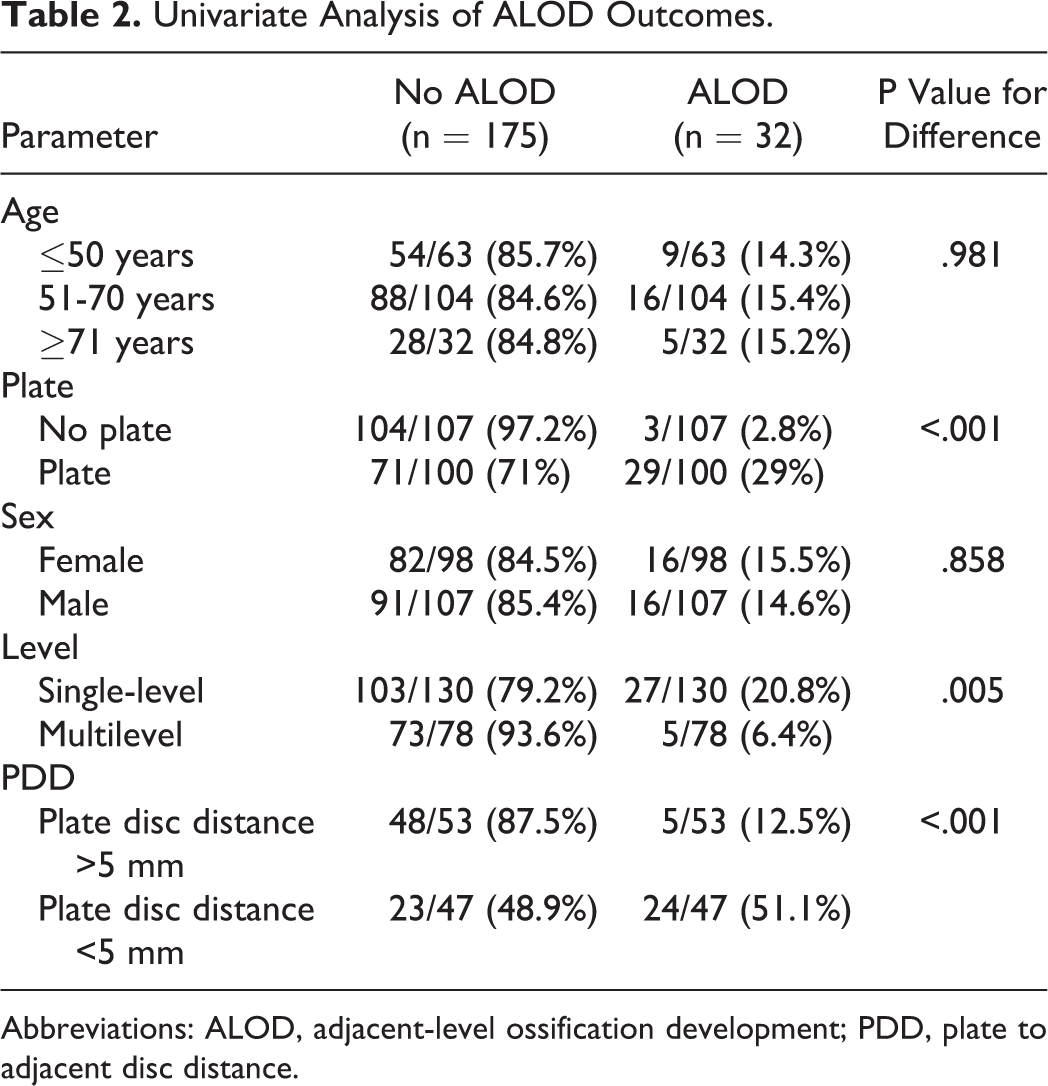
Abbreviations: ALOD, adjacent-level ossification development; PDD, plate to adjacent disc distance.
In ACDF without plate (total ALOD rate of 2.8%), 1 patient had ALOD Grade 1 (1/3), 2 patients had Grade 2 (2/3), and none had Grade 3.
In ACDF with plate (total ALOD rate 29%), 48.3% of ALOD was Grade 1 ALOD (14/29), 31% was Grade 2 ALOD (9/29), and 20.7% was Grade 3 ALOD (6/29; Table 4). Majority of the patients in this group with ALOD had PDD <5 mm (82.8%, 24/29), while only 17.2% (5/29) had PDD >5 mm.
We then divided into 3 groups: ACDF without plate, ACDF with plate with PDD <5 mm, and ACDF with plate with PDD >5 mm, and the respective rate of ALOD was 2.8%, 51.1%, and 12.5%, respectively (Figure 2).
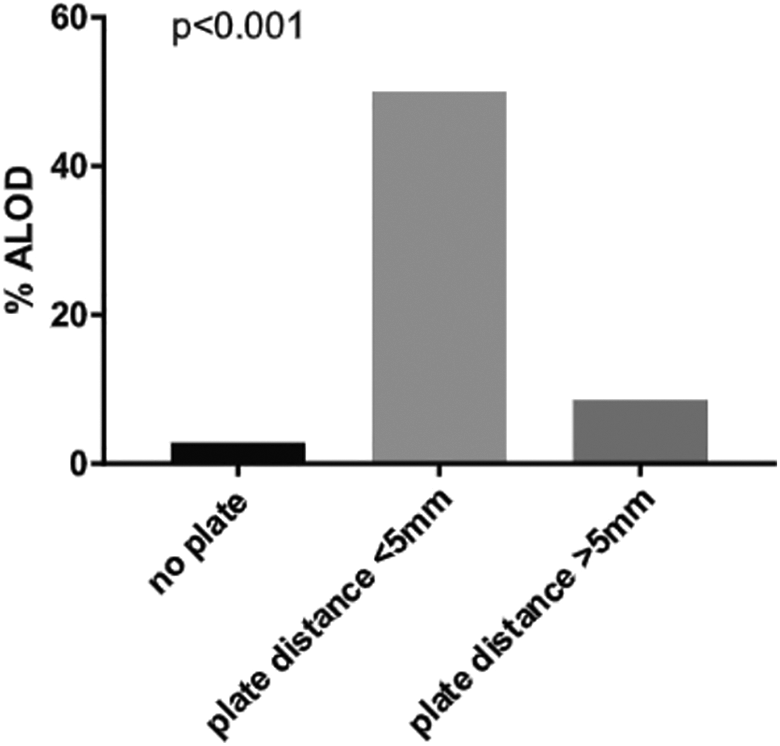
The rate of ALOD in groups with no plate, plate-to-disc distance <5 mm, and plate-to-disc distance >5 mm.
On multivariate adjustment for age, sex, and multilevel surgery, we found that use of plate was associated with ALOD (P = .001; Table 3). PDD was a significant factor in the development of ALOD in patients who had ACDF with plate (Table 4).
Multivariate Analysis of ALOD Outcomes.
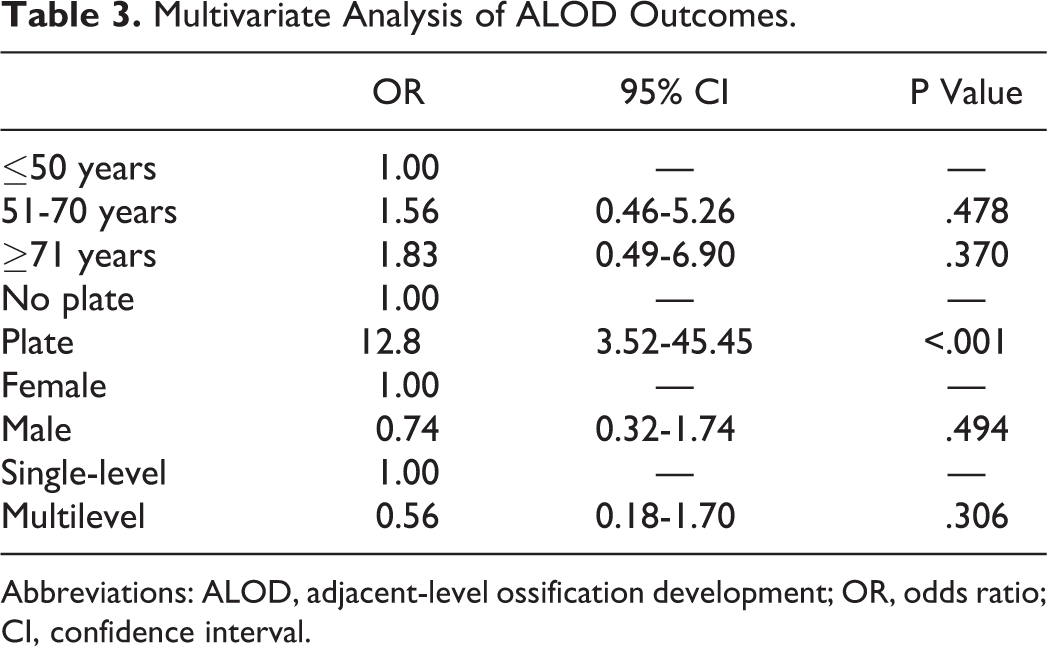
Abbreviations: ALOD, adjacent-level ossification development; OR, odds ratio; CI, confidence interval.
Comparison of ALOD Grades Between the 3 Groups (No Plate, PDD <5 mm, and PDD >5 mm)a.
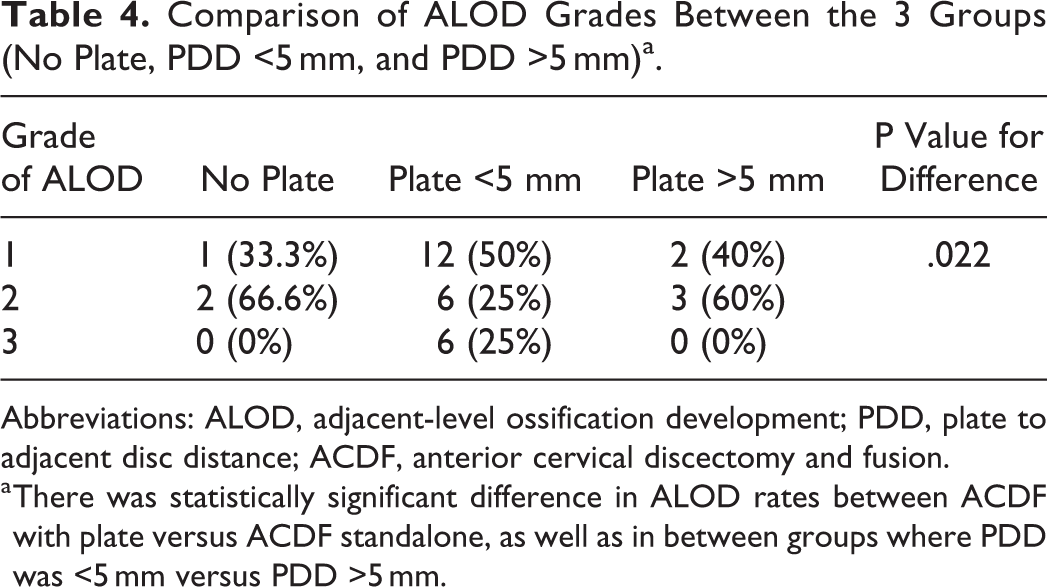
Abbreviations: ALOD, adjacent-level ossification development; PDD, plate to adjacent disc distance; ACDF, anterior cervical discectomy and fusion.
a There was statistically significant difference in ALOD rates between ACDF with plate versus ACDF standalone, as well as in between groups where PDD was <5 mm versus PDD >5 mm.
Although not all patients had radiologic follow-up to 24 months, statistical analysis showed there was no significance in ALOD rates in our cohort in patients with <12 months follow-up versus >12 months follow-up (Table 5).
Rate of ALOD in Patient With Follow-up <12 Months Compared to >12 Months.
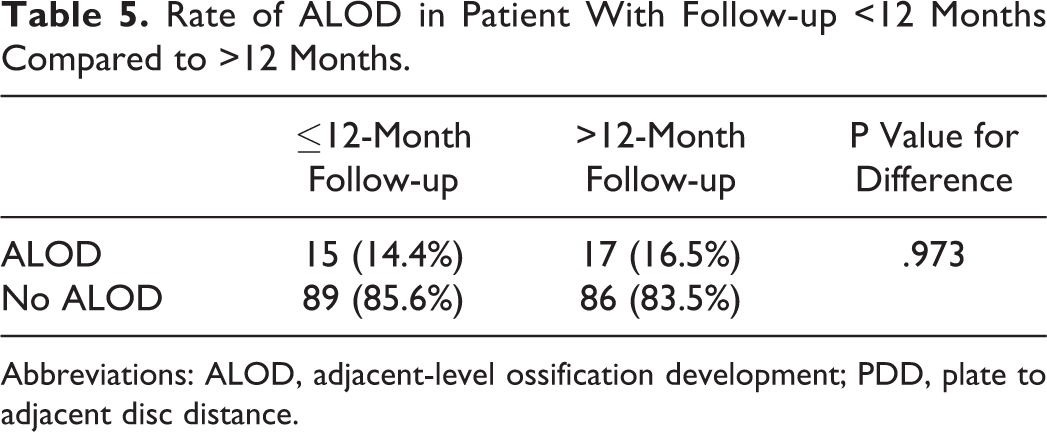
Abbreviations: ALOD, adjacent-level ossification development; PDD, plate to adjacent disc distance.
Discussion
A systemic literature review was performed by Kim et al 4 evaluating the risk factors for ALOD development in anterior cervical spine surgery and included 5 studies:
These studies have been summarized with other literature on ALOD including the current authors (Table 6).
List of Studies on ALOD to Date.
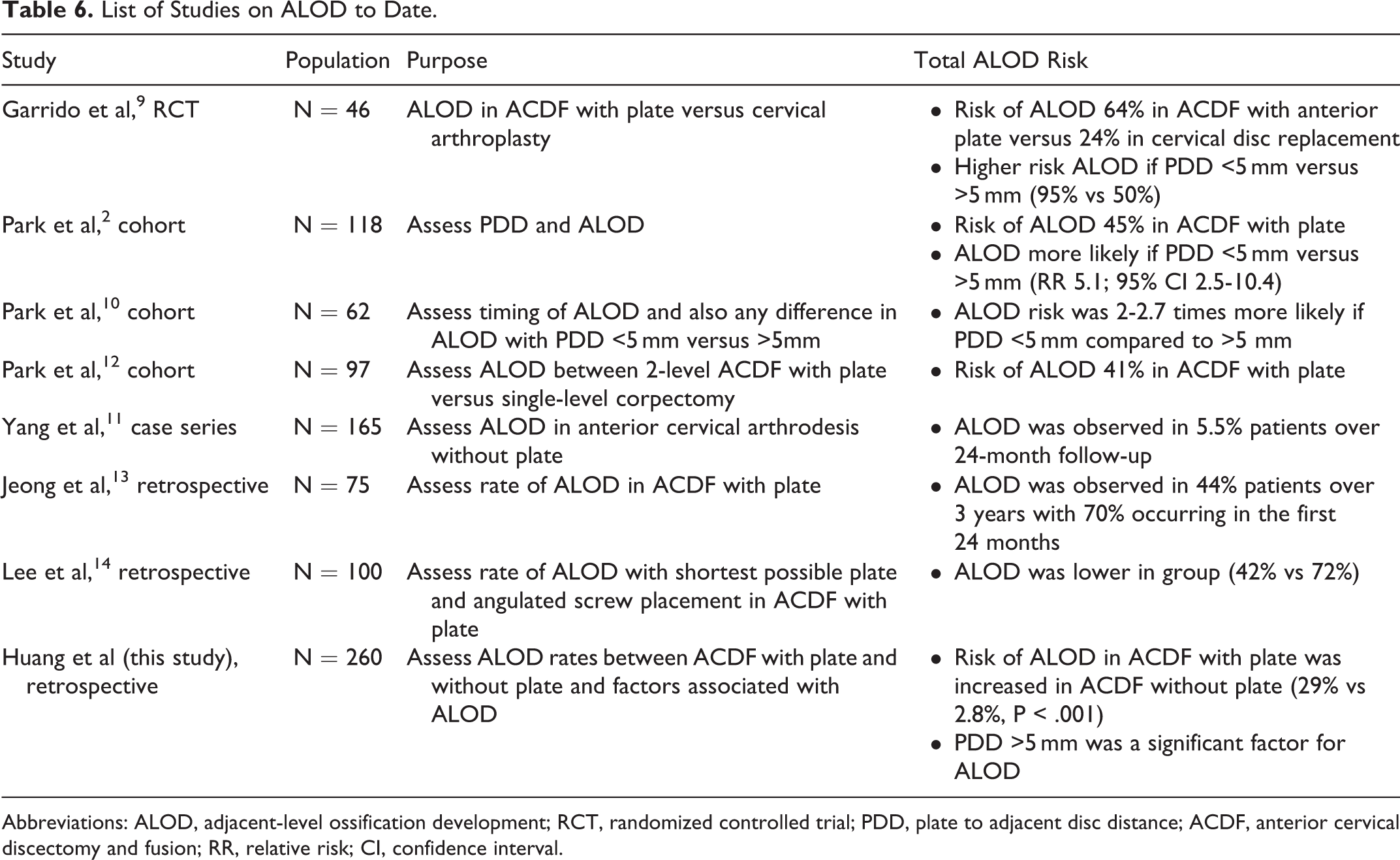
Abbreviations: ALOD, adjacent-level ossification development; RCT, randomized controlled trial; PDD, plate to adjacent disc distance; ACDF, anterior cervical discectomy and fusion; RR, relative risk; CI, confidence interval.
The ALOD risk ranged from 41% to 61% in the studies involving an anterior plate, 24% in the TDR group and 6% in the ACDF without plate group. The risk of ALOD was ranged from 41% to 64% at 24 months in the plate group versus a 6% to 24% risk at 24 months in the non-plate (ACDF and TDR) group. Their analysis observed a 2-fold higher risk of ALOD at the adjacent cranial segment with a PDD of <5 mm being a significant factor. They did not observe any significance between surgical procedure type (corpectomy vs discectomy or fusion) although they do comment that ALOD risk was higher in single-level anterior cervical, which was not statistically significant.
ALOD Risk in Anterior Cervical Surgery
In the original article by Park et al, 2 they retrospectively reviewed the lateral cervical radiographs of 118 patients following anterior cervical arthrodesis with a plate for the treatment of degenerative cervical disease. The follow-up was a mean of 25.7 months. They observed ALOD in 70/118 (59%) patients in the cephalad adjacent disc spaces and in 29/100 (29%) patients in the caudal adjacent disc spaces.
Jeong et al 13 also assessed ALOD rate in patients undergoing ACDF with plate. The ALOD rate was 44% (33/75) on follow-up of >2 years, with 40% (13/33) occurring in the second year. Garrido et al 9 in their randomized controlled trial found 64% risk of ALOD with plate when followed up for 24 months. But for TDR their rate was 24%. Park et al 10 in their study found 41% ALOD rate when the follow-up was a mean of 24 months.
In our study, ACDF with plate had ALOD rate of 29% with a mean follow-up of 15 months. This is similar but less than most of the studies and this could be because of the shorter follow-up. Jeong et al 13 found most of the ALOD development occurred during the first year, but also occurred during second and third years of follow-up; however, the length of follow-up was not statistically significantly related to ALOD development. Their cohort was heterogeneous with both trauma (25 patients) and degenerative (50 patients) included. In fact, Park et al 12 found that only 1.8% who had no ALOD at 12 months developed ALOD at 24 months. Hence, 12-month follow-up may capture majority of the ALOD development.
In standalone patients in our study the rate of ALOD was very low (2.8%), which is the similar to the rate of ACDF without plate in the study of Yang et al 11 but less than that of the TDR study of Garrido et al. 9
ALOD Development Risk Factors
Plate
Although there are studies looking at ACDF without plate and studies evaluating ACDF with plates, ours is the first study to compare the ACDF without plate cohort to with plate cohort. We found the rate of ALOD was reduced significantly without plate (29% vs 2.8%). In Garrido et al, 9 this difference is also apparent; however, there were 2 different kinds of surgeries, ACDF versus TDR
PDD
PDD <5 mm has been identified by a few studies as being a significant factor for ALOD development. In their analysis, Kim et al 4 observed a 2-fold higher risk of ALOD at the adjacent cranial segment with a PDD of <5 mm. In their study, Park et al 2 ALOD rate was 67% if PDD was <5 mm and 24% if PDD >5 mm. Garrido et al 9 found an ALOD rate of 95% if PDD was <5 mm and 50% if PDD >5 mm. In our study, we also found a statistically significant (P ≤ .001) reduction of ALOD rate if PDD >5 mm (51.1% vs 12.5%).
Lee et al 14 described a plating technique to prevent ALOD. In their retrospective matched cohort analysis of 100 patients (matched 1:1 for age, gender, number of levels fused, and comorbidities to either control or study group), they observed a reduction in Grade 2 or higher ALOD (6% vs 20%, P ≤ .05) with their technique—by using the shortest plate possible and placing the cranial and caudal screws at the corners immediately adjacent to their respective operative endplate level and angling the screws cranially and caudally for maximal purchase. The corner is also the strongest cortical bone and hence increases the strength of the screws. With their technique they were able to decrease the rate of ALOD, by increasing the PDD. One of the other factors was minimizing the dissection of the anterior longitudinal ligament along the vertebral body as the screws were placed in close proximity to the disc space.
Number of Levels Operated
There was low evidence data in Lee et al 14 to determine whether single-level or 2-level ACDF affected the rate of ALOD as well as the rate of ALOD in noninstrumented fusion. Yang et al 11 have identified younger age and increased number of levels fused as risk factors for ALOD and postulated that excessive dissection along the anterior longitudinal ligament may contribute for ALOD. In our study, surprisingly, we found more ALOD in the single level than in multilevel cases. This is being investigated further as to the cause for this result.
One of the criticisms raised with regard to ALOD is its clinical significance. There is conflicting data in the literature with some studies reporting no increase in pain or reoperation rates, 3,15 while others have reported increased adjacent segment degeneration disease. 1 Min et al, 16 in their retrospective study of patient radiographs, observed significantly reduced range of motion not only at the ALOD affected segment but also associated with increased motion at the next segment adjacent to the ALOD, thus suggesting it not only affects the immediate adjacent level of the fusion but also 2 levels from the fused level. 16 It is the fundamental belief, however, that if a surgeon and patient agree to fuse a certain level, any additional number of levels that are inadvertently fused or affected because of surgical technique is an undesirable outcome.
The alternative to placing a shorter plate and screws is a standalone cage, which has been reported to have the same fusion rate as ACDF with plate, 17,18 although this depends on multiple factors, including but not limited to patient medical background, number of levels approached, and underlying indication for ACDF. We observed decreased ALOD rates with standalone ACDF, which also has the benefit of not requiring additional anterior longitudinal ligament dissection.
Strengths
Our study is the largest study in the literature to the authors’ knowledge (260 patients). Second, ours is the first case-control study evaluating ALOD rated in ACDF without plate (standalone) versus ACDF with plate.
Limitations
The present study is constrained by several limitations. First, it is a retrospective study, which is susceptible to selection bias and other limitations of a retrospective study. Second, the follow-up rate was 80% for the patients included in the present cohort study, which although not perfect is in acceptable range. Although not all patients had radiologic follow-up to 24 months, there was no statistically significant difference in ALOD rates in our cohort in patients with <12 months follow-up versus >12 months follow-up (Table 5). There was also variation in the timing of follow-up scans to assess for ALOD, which contributes to heterogeneity of the present results. Thirty-two percent of patients did not have follow-up to 24 months, which is the detectable timeframe for ALOD. There is also the difference in cages and types of cages and plates utilized over time and between centers. The preoperative status of the adjacent levels that developed ALOD were not measured, but if ALOD was present preoperatively they were not considered as ALOD.
Conclusion
This is the first case-control study to evaluate ALOD rates in patients undergoing ACDF with and without plates. We observed a significant decrease in ALOD development in patients with standalone ACDF. However, the plate-to-disc distance <5 mm contributed also to the development of ALOD. The authors feel if ALOD prevention is a goal then either a standalone or a plate that is less than 5 mm from adjacent disc should be utilized. Further prospective studies are needed to evaluate if ALOD causes any significant clinical issues. Further research into ALOD and its role in adjacent segment degeneration and disease may present further insight into the pathogenesis underlying these pathologies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.