
Abstract
Study Design:
Retrospective analysis.
Objective:
We investigated whether complete correction of cervical sagittal malalignment is necessary during 4-level anterior cervical discectomy and fusion (ACDF) in patients with kyphosis.
Methods:
This retrospective study included 84 patients who underwent 4-level ACDF surgery at a university hospital between January 2010 and December 2015. Based on the degree of cervical lordosis correction, patients were categorized into the following groups: mild (0-10°), moderate (10-20°), and complete correction (>20°). The clinical outcomes, radiological parameters, and functional outcomes were analyzed.
Results:
We observed no significant intergroup differences in the baseline characteristics. The cervical sagittal vertical axis (CSVA) correction loss at the final follow-up was lesser in the mild- and moderate- than in the complete-correction group. The spinocranial angle (SCA) and T1 slope (T1 S) were significantly higher in the moderate- and complete-correction groups than in the mild-correction group, 3 days postoperatively. The cervical proximal junctional kyphosis (CPJK), adjacent segment degeneration (ASD), and ASD following CPJK rates were higher in the complete-correction group. We observed no significant intergroup differences in postoperative complications; however, 5 patients showed internal fixation failure in the complete-correction group; 4 of these patients required reoperation. No significant intergroup difference was observed in the Japanese Orthopedic Association and neck disability index scores at any time point.
Conclusions:
A mild-to-moderate correction of cervical lordosis is superior to complete correction in patients with kyphosis who undergo 4-level ACDF because this approach is associated with lesser axial stress and CSVA correction loss.
Keywords
Introduction
Anterior cervical decompression and fusion surgery, including anterior cervical discectomy fusion (ACDF), anterior cervical corpectomy and fusion, and anterior cervical hybrid decompression and fusion, which are widely performed for degenerative cervical spine disorders are associated with excellent results following optimal patient selection.1-4 However, internal fixation failure and adjacent segment degeneration (ASD) are commonly observed complications.4-12
The physiological cervical lordotic curvature is important to maintain spinal sagittal alignment and balance; the normal C2-7 Cobb angle measurements range from 16 ± 16° to 22 ± 16°.13,14 Persistent abnormal curvature of the cervical spine may result in neck pain, increased incidence of cervical myelopathy, spinal cord compression, and cord tension, which negatively affect patients’ quality of life.15-18 Moreover, cervical degenerative diseases often coexist and interact with abnormal cervical curvature. 19 Decompression alone may not reduce cord tension caused by abnormal cervical curvature, such as kyphosis, and surgical treatment of myelopathy should essentially include cervical lordosis correction. 19 Ferch et al 20 reported that cervical sagittal alignment correction may promote recovery of spinal cord function in patients with kyphotic deformity. Gum et al 21 suggested that better restoration of lordosis after ACDF was associated with improved health-related quality of life.
Reportedly, surgical correction of cervical lordosis improves clinical outcomes; therefore, most surgeons emphasize correction of cervical lordosis to the greatest extent possible. 22 However, the optimal extent of correction remains unclear. In this study, we investigated whether complete correction of cervical sagittal malalignment is necessary during 4-level ACDF in patients with kyphosis. Our findings may serve as guidelines to develop an optimal surgical strategy.
Methods
Study Design and Patients
This retrospective study included patients who underwent 4-level ACDF surgery between January 2010 and December 2015. Inclusion criteria were as follows: (1) diagnosis of cervical disc disease, such as cervical spondylotic myelopathy, cervical radiculopathy, and cervical disc herniation, (2) 4-level ACDF surgery at the C3-C7 level with at least 4 years of follow-up, (3) diagnosis of cervical kyphosis, (4) availability of complete clinical and radiological data, including anteroposterior (A/P), lateral and flexion-extension radiographs of the cervical spine preoperatively, 3 days postoperatively, and at final follow-up, along with magnetic resonance imaging (MRI) or computed tomography scans obtained preoperatively and at final follow-up and, (5) no preoperative ASD. Exclusion criteria were as follows: (1) diagnosis of cervical ossification of the posterior longitudinal ligament, tumor, metabolic diseases, cervical rheumatoid arthritis, and trauma and, (2) diagnosis of congenital spinal deformity and a history of cervical spine surgery.
Clinical and Radiological Evaluation
The following clinical and radiological data was analyzed: (1) patients’ demographic characteristics, including age at surgery, sex, body mass index (BMI), length of hospital stay, and duration of follow-up, (2) surgical variables, including postoperative complication and reoperation rates, (3) clinical outcomes, including the preoperative and postoperative Japanese Orthopedic Association (JOA) and neck disability index (NDI) scores, (4) radiographic parameters, including ASD both superior and inferior to the surgical segment, the proximal junctional sagittal Cobb angle, preoperative C2-7 Cobb angle (Pre-Angle A), preoperative and postoperative fused segment angles (Angle B), degree of cervical lordotic correction (Angle C), preoperative C2-C7 sagittal vertical axis (CSVA), the spinocranial angle (SCA), and the T1 slope (T1 S).
We compared preoperative radiographic findings with those observed at the final follow-up, and ASD was diagnosed in patients who met one of the following criteria: (1) osteophytes on plain A/P or lateral radiographs, (2) segmental hypermobility or newly developed instability detected on plain lateral radiographs (flexion and extension views) (slippage >3 mm), (3) clearly evident disc space narrowing on lateral radiographs (>3 mm reduction in disc space), (4) clearly evident reduction in the intervertebral disc signal intensity on MRI and, (5) newly developed cervical disc herniation or cervical canal stenosis on MRI.23,24
The C2-7 Cobb angle (angle A, Figure 1) was defined as the angle between the lines perpendicular to the lines parallel to the inferior endplates of the C2 and C7 vertebral bodies.25,26 The angle of the fused segment (angle B) refers to the angle formed by the lines parallel to the upper and lower planes of the fused segment. The degree of cervical lordosis correction (Angle C) was calculated as the difference between the pre- and postoperative angle B. The proximal junctional sagittal Cobb angle (angle D) was measured as the angle between a line parallel to the upper plane of the fused segment and that parallel to the inferior endplate of the adjacent upper vertebral body. The CSVA refers to the distance from the posterosuperior corner of C7 to the plumbline from the centroid of C2. 27 The SCA is defined as the angle between the C7 slope and a straight line that joins the middle of the C7 endplate and the middle of the sella turcica. 15 T1 S is defined as the angle between a horizontal reference line and a line parallel to the superior endplate of T1. 15 Cervical proximal junctional kyphosis (CPJK) was defined based on the following criteria: (a) proximal junctional sagittal Cobb angle <0° and, (b) absolute value of postoperative angle D >the preoperative angle D. JOA and NDI scores were recorded preoperatively, 1 year postoperatively, and at the final follow-up to evaluate neurological function. Radiographic parameters were measured by 3 independent clinicians using the Prospective Acquisition CorrEction system (a reliable and valid tool for quantitative spinal measurements) and were reviewed by the authors. The mean of 3 measurements was used for further analysis.
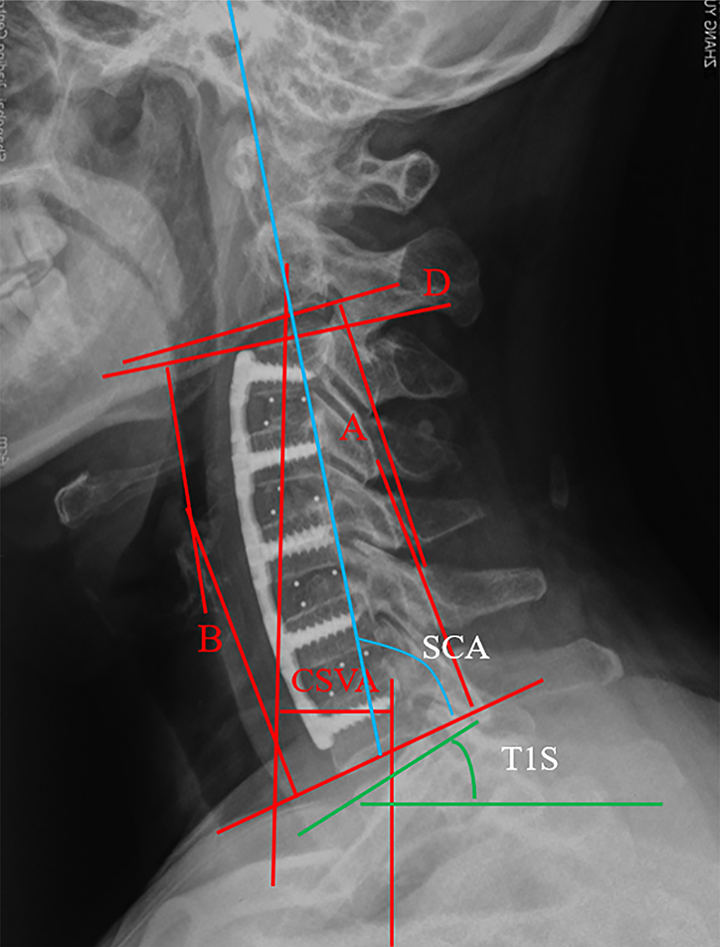
Lateral radiograph of the cervical spine showing measurements of the C2-7 Cobb angle (Angle A), Cobb angle of the fused segments (Angle B), proximal junctional sagittal Cobb angle (Angle D) and the CSVA, SCA and T1S. CSVA, cervical (C2-7) sagittal vertical axis; SCA, spinocranial angle; T1S, T1 slope.
Statistical Analysis
All statistical analyses were performed using the IBM SPSS Statistics for Windows software, version 24.0 (Armonk, NY IBM Corp [Released 2016]). We used the chi-square, analysis of variance, and rank sum tests based on the types of data analyzed. Continuous variables are presented as mean ± standard deviation, and categorical data as frequencies or percentages. A P value < .05 was considered statistically significant.
Results
This study included 84 patients (40 men, 44 women, mean age 65.47 ± 12.45 years) who were categorized into 3 groups based on the degree of cervical lordosis correction as follows: mild (0-10°), moderate (10-20°), and complete correction (>20°). The mild-, moderate-, and complete-correction groups included 28, 24, and 32 patients, respectively. We observed no statistically significant intergroup differences in age, sex, BMI, length of hospital stay, and duration of follow-up (Table 1).
Baseline Characteristics of Study Population.
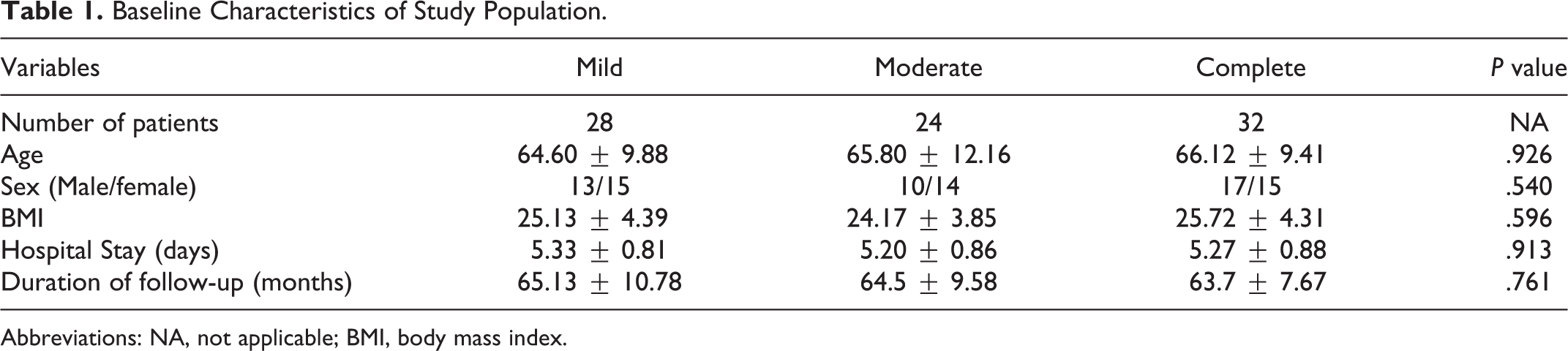
Abbreviations: NA, not applicable; BMI, body mass index.
Intergroup Comparison of Radiographic Parameters
The preoperative angle A (C2-7 Cobb angle) was −5.90 ± 3.10, −5.41 ± 3.88, and −5.75 ± 4.68 in the mild-, moderate-, and complete-correction groups, respectively (P = .233, Table 2). No significant intergroup difference was observed in the preoperative angle B (the angle of the fused segment) (P = .442). However, we observed significant intergroup differences in the postoperative angle B (P < .001). The mean Angle C (degree of cervical lordosis correction) was 8.30 ± 1.22, 16.07 ± 2.42, and 22.04 ± 2.04 in the mild-, moderate-, and complete-correction groups, respectively (P < .001). No significant intergroup difference was observed in the pre-CSVA and CSVA measured 3 days postoperatively. However, the CSVA correction loss at the final follow-up was lesser in the mild- and moderate groups than in the complete-correction group (P < .05). Moreover, the SCA and T1 S were significantly higher in the moderate- and complete-correction groups than in the mild-correction group, 3 days postoperatively. The prevalence of CPJK was 4 (16.67%) and 21 patients (65.63%) in the moderate- and complete-correction groups, respectively, whereas CPJK was not observed in the mild-correction group (Figures 2 and 3). Postoperative ASD occurred in 6 (21.43%), 9 (37.50%), and 19 (59.38%) patients in the mild-, moderate-, and complete-correction groups, respectively. Notably, the rate of ASD following CPJK was significantly higher in the complete-correction group than in the mild- and moderate-correction groups.
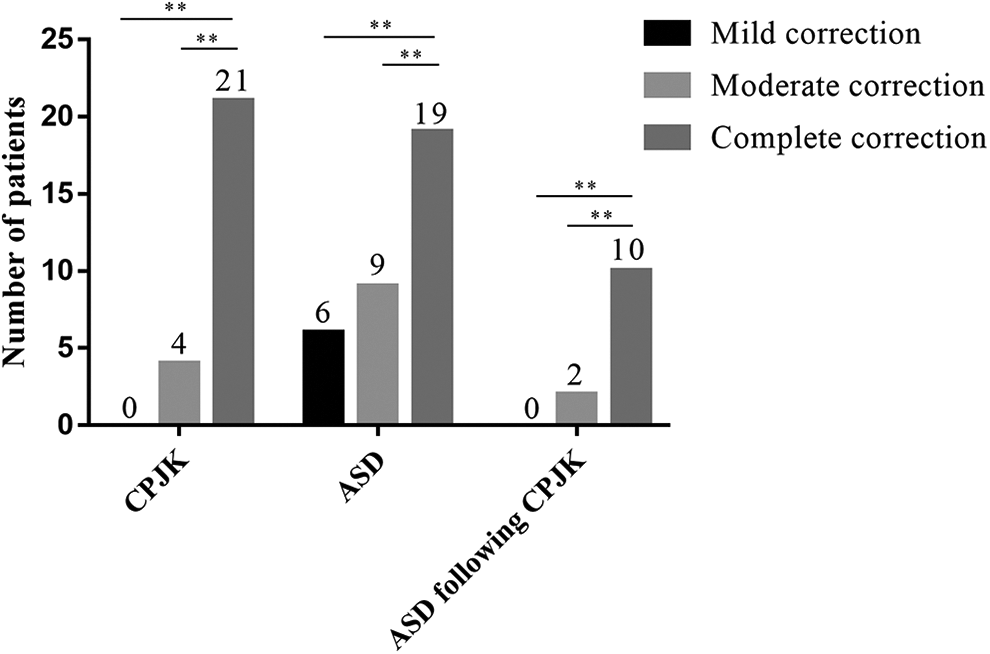
Image showing CPJK, ASD, and ASD following CPJK. ASD indicates adjacent segment degeneration; CPJK, cervical proximal junctional kyphosis.
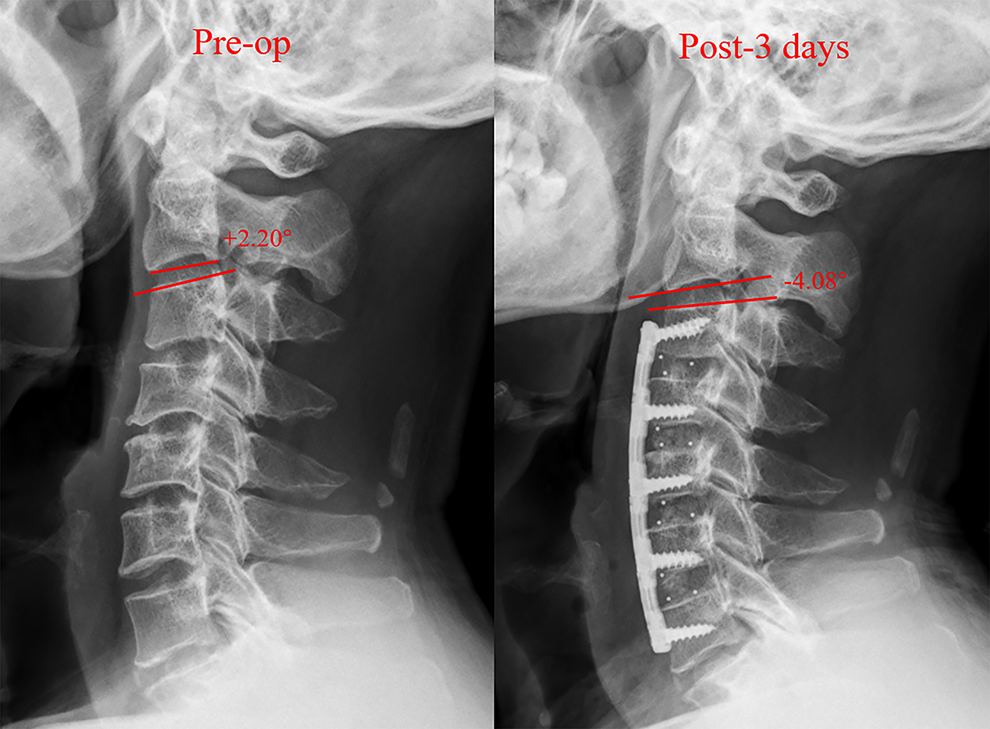
Image showing postoperative CPJK. CPJK indicates cervical proximal junctional kyphosis.
Comparison of Radiographic Parameters Between the 3 Groups.*
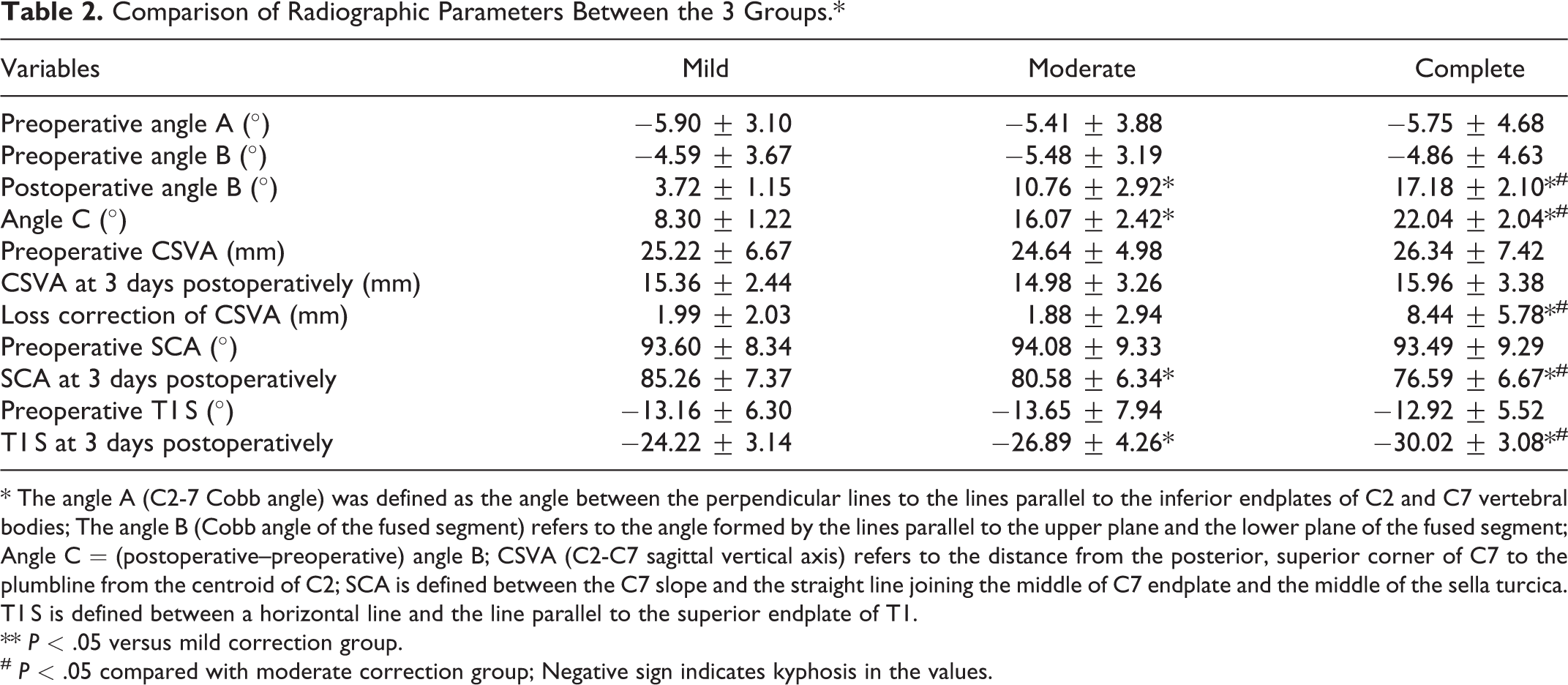
* The angle A (C2-7 Cobb angle) was defined as the angle between the perpendicular lines to the lines parallel to the inferior endplates of C2 and C7 vertebral bodies; The angle B (Cobb angle of the fused segment) refers to the angle formed by the lines parallel to the upper plane and the lower plane of the fused segment; Angle C = (postoperative–preoperative) angle B; CSVA (C2-C7 sagittal vertical axis) refers to the distance from the posterior, superior corner of C7 to the plumbline from the centroid of C2; SCA is defined between the C7 slope and the straight line joining the middle of C7 endplate and the middle of the sella turcica. T1 S is defined between a horizontal line and the line parallel to the superior endplate of T1.
** P < .05 versus mild correction group.
# P < .05 compared with moderate correction group; Negative sign indicates kyphosis in the values.
Postoperative Complications
In addition to ASD, the postoperative complication rates in the mild-, moderate-, and complete-correction groups were 14.29%, 20.83%, and 28.12%, respectively (P = .424, Table 3). Internal fixation failure occurred in 5 patients in the complete-correction group; no patient in the mild- and moderate-correction groups developed this complication (Figure 4).
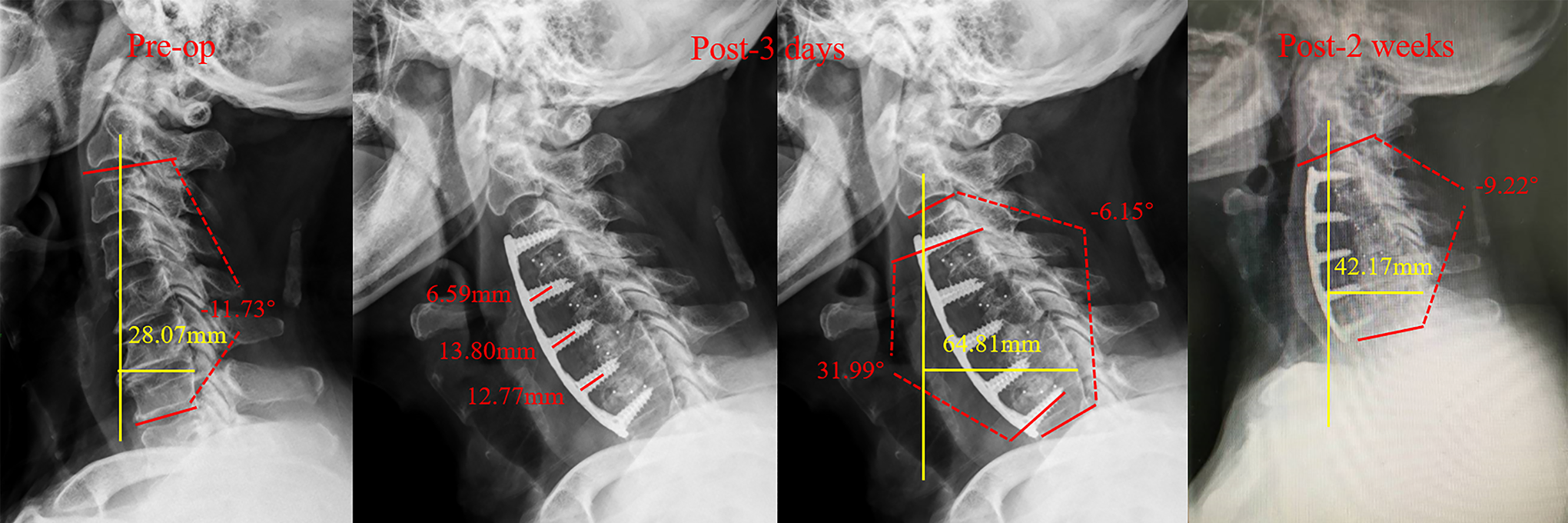
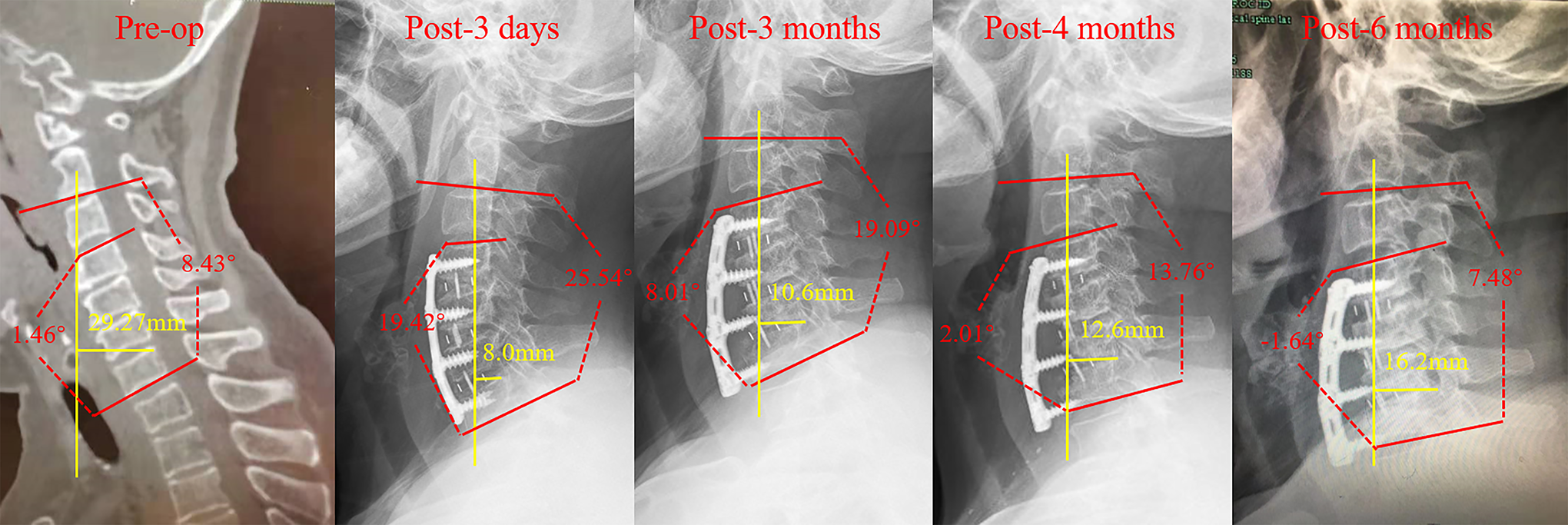
Image showing internal fixation failure secondary to complete correction of cervical lordosis in a representative case of a 65-year-old man without osteoporosis. Cervical lordosis correction is approximately 40°. Screw loosening gradually worsened over the first 2 weeks postoperatively, and the cervical spine curvature gradually returned from a lordotic to kyphotic pattern. Preoperative findings: Cobb angle −11.73°, CSVA 28.07 mm; 3 days postoperatively: Cobb angle −6.15°, CSVA 64.81 mm; 2 weeks postoperatively: Cobb angle −9.22°, CSVA 42.17 mm. CSVA indicates, cervical sagittal vertical axis.
Postoperative Complications and Reoperations.*
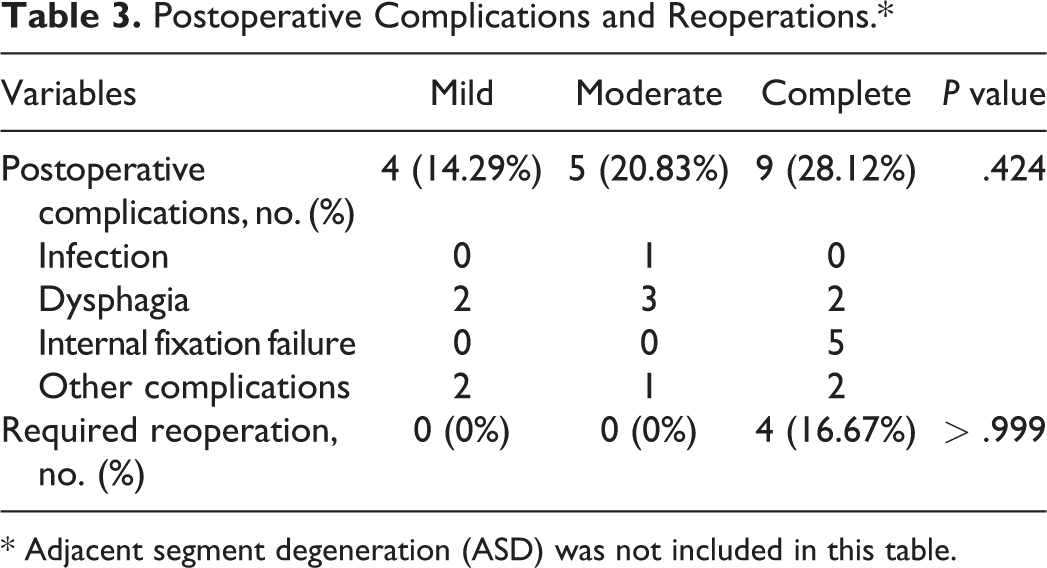
* Adjacent segment degeneration (ASD) was not included in this table.
Clinical Outcomes
All 3 groups showed significant improvements in postoperative JOA and NDI scores (Figure 5A). However, we observed no significant intergroup differences in the JOA and NDI scores at any time point (Figure 5B).
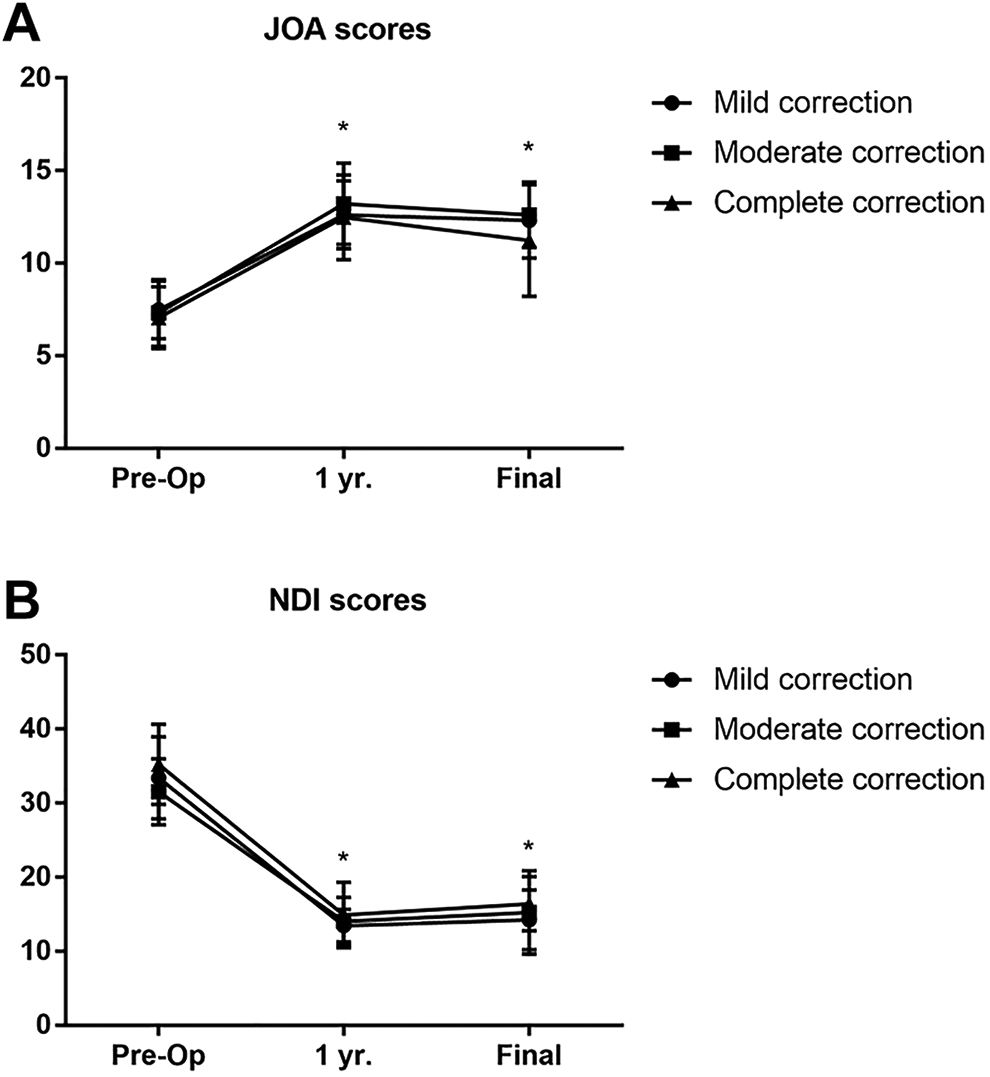
JOA and NDI scores in the 3 study groups. A. JOA indicates Japanese orthopedic association; B. NDI, neck disability index.
Discussion
Proximal junctional kyphosis (PJK), which shows multifactorial etiology is a common complication following adult spinal deformity surgery and may cause proximal junctional failure. 28 A greater magnitude of deformity correction is associated with a high rate of PJK, and the increased degree of postoperative lumbar lordosis also contributes to the high risk of PJK in such cases.28,29 In this study, PJK was described as CPJK, a postoperative complication of a 4-level ACDF. Usually, the cervical proximal junctional sagittal Cobb angle measures >0° owing to the physiological lordotic curvature of the cervical spine. Therefore, with reference to the definition of PJK, CPJK was defined as a proximal junctional sagittal Cobb angle measuring <0°. The results of this study showed that the CPJK rate was higher in the complete-correction group than in the mild- and moderate-correction groups, which indicates that complete correction of cervical lordosis serves as a risk factor for CPJK. Similar to the mechanism observed in PJK, this phenomenon may be attributed to increased axial stress that occurs after complete correction in patients with kyphosis. The increased axial stress forces the adjacent segment to form CPJK to partly buffer the axial stress. CSVA is a critical parameter in cervical deformity surgery. 19 In this study, we observed no significant intergroup difference in the preoperative CSVA; however, the CSVA correction loss at the final follow-up was significantly greater in the complete-correction group. This finding could be attributed to the fact that when the increased axial stress is greater than the buffering effect of CPJK, the CSVA correction loss will inevitably and gradually increase as a compensatory mechanism to maintain cervical sagittal balance, and this may contribute to internal fixation failure. Moreover, the SCA and T1 S were significantly higher in the moderate- and complete-correction groups than in the mild-correction group, 3 days postoperatively, which can be viewed as a compensatory mechanism for a higher degree of correction of cervical lordosis.
The prevalence of ASD after cervical fusion surgery was 40.47% in our study, which is similar to the findings reported by Kong et al. 7 Although several studies have investigated the mechanical and other risk factors of ASD,30-33 this subject remains unclear and controversial. In our study, ASD rates were higher in the complete-correction group than in the mild- and moderate-correction groups. More importantly, the post-CPJK ASD rates were significantly higher in the complete-correction group than in the mild-and moderate-correction groups, which suggests that CPJK may be an important risk factor associated with ASD. We hypothesized that CPJK may cause concentration of stress in adjacent segments, and increase the intradiscal pressure and consequently accelerate disc degeneration.
Our results showed no significant intergroup differences in the postoperative complication rates (excluding ASD). However, 5 patients in the complete-correction group showed internal fixation failure; 4 patients required reoperation and 1 patient received conservative treatment. Notably, this complication did not occur in the mild- and moderate-correction groups. Studies have shown that proximal junctional failure is a severe form of PJK that follows adult spinal deformity fusion surgery and that this complication is associated with the magnitude of deformity correction. 28 Similarly, the mean degree of cervical lordosis correction was significantly higher in the complete-correction than in the mild- and moderate-correction groups, which supports our results. The increased axial stress that results from complete correction may be another contributor to this phenomenon. We observed that cervical internal fixation failure occurred in 5 patients between 3 days and 3 months postoperatively; this time range indicates that it may be an early postoperative phenomenon. Interestingly, internal fixation failure usually presents as loosening of the middle screws, and the screws implanted at both ends remain normal. This finding may be attributed to the fact that axial stress on the middle screws is stronger than that applied at both ends, which consequently proves the hypothesis of increased axial stress. We also observed that patients with 3-level ACDF showed internal fixation failure secondary to complete correction (Figure 6). However, whether other factors, including the number of fusion levels, osteoporosis, and curvature pattern of the entire cervical spine were associated with internal fixation failure remains unclear and warrants further investigation. Although the complete-correction group had higher CPJK, ASD, and internal fixation failure rates, we observed no significant intergroup differences in the JOA and NDI scores at any time point.
Representative case of a patient who underwent 3-level ACDF with postoperative internal fixation failure secondary to complete correction of cervical lordosis. ACDF indicates anterior cervical discectomy and fusion.
In summary, complete correction of cervical lordosis may cause CPJK, promote ASD, aggravate CSVA correction loss, and may even cause cervical internal fixation failure. Based on our results, we conclude that mild-to-moderate correction (0-20°) of cervical lordosis may protect against CPJK and consequent complications. Specifically, a smaller bending angle of the steel plate used intraoperatively can prevent CPJK. Ji et al 34 reported that compared with fusion using cage and plate constructs, fusion using stand-alone cages may potentially reduce the incidence of ASD because it can theoretically buffer the increased axial stress (at least to some extent) associated with complete correction. Maintenance of overall spinal balance includes an interaction between several factors, which should be considered to comprehensively determine the optimal degree of cervical lordosis correction. We observed that the phenomenon of CPJK was more pronounced in radiographs obtained during cervical spine flexion than in lateral views obtained during standing, which implies that frequent postoperative cervical flexion may favor CPJK and that the dynamic nature of the cervical spine needs to be considered as well. We are of the view that this study may significantly contribute to the literature and that our findings could serve as guidelines to develop an optimal surgical strategy.
Followings are the limitations of the study: (a) The small sample size is a drawback, and large-scale studies are warranted to establish conclusive results. (b) The retrospective study design is a drawback, and a prospective randomized study is required to verify the findings of this study. (c) We considered this complex issue only with regard to postoperative complications; however future studies should investigate the role of other possible contributors, for example, the number of fusion levels.
Conclusions
Mild-to-moderate correction of cervical lordosis is superior to complete correction in 4-level ACDF surgery performed in patients with kyphosis, because this approach is associated with lesser axial stress, CPJK, ASD, and CSVA correction loss. Future research should determine the role of other possible factors that should be considered to comprehensively determine the optimal degree of cervical lordosis correction required in such cases.
Footnotes
Authors’ Note
Qing-Xin Song, Xin-Jin Su, and Kun Wang contributed equally to this work and should be considered as co-first authors. This study was approved by the Ethics Committee of Renji Hospital before data collection (IRB: RA-2020-040), and we obtained written informed consent from all patients.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Program of Shanghai Subject Chief Scientist (PYIV-17-002) and the Smart Medical Special Research Project of Shanghai Municipal Commission of Health and Family Planning (2018ZHYL0215).