
Abstract
Study Design:
Retrospective cohort study.
Objectives:
To conduct the first comprehensive national-level study examining specific risks, outcomes, and costs surrounding surgical treatment of lumar spinal stenosis (LSS) in patients with and without neurogenic claudication (NC).
Methods:
Data for patients with or without NC who underwent decompression with a lumbar interbody fusion approached anteriorly (ALIF), posteriorly (PLIF), or laterally (LLIF) for LSS was collected from the 2013-2014 National Inpatient Sample using International Classification of Disease codes.
Results:
A total of 121 025 LSS cases without NC and 20 095 cases with NC were included in this study. The most significant complications associated with NC status by organ system included renal (P = .0030) and hematological complications (P = .0003). Multivariate regression controlling for key demographic and comorbidity variables showed that patients with NC did not have significantly higher odds of complication, non-home discharge, or extended hospitalization compared to patients without NC regardless of fusion type. Interestingly, NC patients had comparatively lower total charges for their hospitalization following PLIFs (P = .0001) and LLIFs (P < .0001), but not ALIFs (P = .6121).
Conclusion:
NC does not appear to significantly increase odds of adverse outcomes following fusion in LSS. Given the large prevalence of LSS and coincidental NC, these findings may carry important implications in managing this challenging patient population and justifies future prospective investigation of this topic.
Introduction
Lumbar spinal stenosis (LSS) is one of the leading pathologies related to lower back pain and disability in the population and the leading indication for patients older than 65 years to undergo spine surgery. 1 -4 Patients can have numerous clinical presentations including localized back pain, radiculopathy, neurogenic claudication (NC), or even asymptomatic. NC, however, is one of the most common presentations. 5 -7 The treatment of patients with LSS who present with NC is somewhat controversial. There is evidence in the literature for nonoperative management including calcitonin treatment, pain management, and patient surveillance. One systematic review assessed the effectiveness of nonoperative management in 21 clinical trials and concluded that little evidence exists to support nonoperative management of LSS with NC. 8
Previous studies have assessed surgical versus non-operative management for the treatment of LSS with NC. 9 -13 Surgical decompression, which may be accompanied by fusion, for LSS has been found to improve symptoms immediately postoperatively, and more recently in the Spine Patient Outcomes Research Trial (SPORT), for up to 4 years postoperatively compared with conservative treatment. 14 Despite these previous findings, however, there is a deficit in the literature comparing patient outcomes following surgical management of LSS with and without co-presenting NC. It is evident in the literature that patients suffering from NC are a well-studied and interesting population, yet few studies assess the impact of NC secondary to LSS on clinical and economic outcomes. This study seeks to ameliorate this deficit by comprehensively characterizing the effect that NC has on clinical and resource utilization outcomes following decompression and various lumbar interbody fusion procedures for LSS using national-level data.
Materials and Methods
The National Inpatient Sample (NIS) of the Healthcare Cost and Utilization Project (HCUP), Agency for Healthcare Research and Quality (AHRQ, Rockville, Maryland) was sampled to obtain data from 2013-2014. The NIS is structured as a stratified sample of 20% of nonfederal US hospitals with over 7 million hospitalizations annually, making it the largest all-payer national database. 15 An encoded weighting variable was applied to patient data to obtain regional and national estimates by accounting for the stratified clustering design of the database, as specified by HCUP (https://www.hcup-us.ahrq.gov/nisoverview.jsp). Our institutional review board has exempted studies involving the NIS from individual review.
Patients were included if they had an International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) diagnosis code of spinal stenosis in the lumbar region without neurogenic claudication (ICD-9-CM code 724.02) or spinal stenosis in the lumbar region with neurogenic claudication (ICD-9-CM code 724.03). In some analyses, cohorts were further categorized according to the fusion type used alongside decompression to treat lumbar stenosis. To do this, we used procedure codes for primary or repeat lumbar interbody fusion anteriorly (ALIF; 81.06, 81.36), posteriorly (PLIF; 81.07, 81.37), or laterally (LLIF; 81.08, 81.38). We identified 121 025 lumbar stenosis cases without NC and 20 095 cases with NC that underwent an ALIF, PLIF, or LLIF procedure for surgical treatment.
Demographic data was collected for both cohorts, including age, race, sex, primary insurance payer, income quartile by ZIP code, admission type, discharge disposition, hospital geographic region, comorbidities, and All Patients Refined Diagnosis Related Groups (APRDRG) scores for mortality risk and severity of illness. Procedure type was also considered as a covariate when assessing overall complication rates across groups.
The primary outcomes examined included in-hospital mortality rate, overall complication rate, complication rate by organ system, and other more specific perioperative complications faced by spine surgery patients. Secondary outcome and resource utilization metrics included length of hospital stay, discharge disposition, and total charges for the hospital visit. For purposes of data analysis, any discharge that was not to home was considered a nonhome discharge. In addition, an extended hospitalization was defined as a length of hospital stay that was greater than the 75th percentile of hospitalization lengths for the entire study population.
Organ system complications were determined for neurological (seizures 345.xx, stroke 433.x or 434.x, transient cerebral ischemia 435.x, and neurological complications after procedure 997.01 or 997.09), pulmonary (514, 518.xx, or 512.xx), cardiac (410.xx or 785.xx), peripheral vascular (venous thromboembolic 453.xx or 415.xx), renal (584.x), gastrointestinal (578.x, 560.1, or 00845), infectious (041.xx, 38.xx, 320.xx, 324.1, 481-486, 507.0, 595.0, 790.7, 995.9x, 996.64, 997.31, 998.59, 999.31), and hematological (285.xx or 998.1x, or red blood cell transfusion 99.04) systems. Sodium disturbance complications (253.5, 253.6, 276.0, or 276.1) were also tracked, along with cases required a tracheostomy (31.1, 31.2, 31.21, or 31.29) or gastrojejunostomy (43.1, 43.11, 43.19, or 46.32).
Statistical analysis was implemented with SAS 9.4 (SAS Institute, Cary, NC, 2013). Categorical variables were assessed using chi-square tests, while Fisher’s exact test evaluated contingency tables with expected counts less than one under the null hypothesis of independence. The means of continuous variables between the two cohorts were compared using two-sided, two-sample T tests. Univariate regression models were constructed to assess primary and secondary outcomes following surgery for LSS based on whether the patients also had NC.
Multivariable regression models were constructed to assess primary and secondary outcomes, including odds of complication, nonhome discharge, extended hospitalization, and total charges, while controlling for important differences in demographic and comorbidity characteristics between the cohorts. To do this, models incorporated predictor variables previously identified as differing significantly between the groups or were established factors known to impact surgical outcomes. Notably, these included age, along with sex, race, hospital geographic region, primary insurance payer, income quartile by ZIP code, chronic blood loss anemia, depression, diabetes mellitus with complications, hypertension, obesity, perivascular disease, and renal failure. These models were further stratified by the fusion type (ALIF, PLIF, and LLIF) performed along with decompression to account for procedure-level differences in outcomes. P < .05 was used to determine statistical significance. The variance inflation factor (VIF) was examined to assess model multicollinearity. Figures were produced using Prism 7 (Graphpad, La Jolla, CA, 2017).
Results
Demographics
We identified a weighted total of 121 025 LSS cases without NC and 20 095 cases with NC that underwent an ALIF, PLIF, or LLIF procedure along with decompression for treatment. Table 1 summarizes baseline demographic characteristics of LSS cases grouped by presence of NC. Comparison of demographic characteristics revealed differences in the distributions of age (P < .0001), sex (P = .0091), primary insurance payer (P < .0001), and discharge disposition (P < .0001) in the 2 cohorts (Table 1). LSS patients with NC were more likely to be older, male, insured by Medicare, and experience nonroutine discharge.
Demographics of the Study Population by Neurogenic Claudication Status.
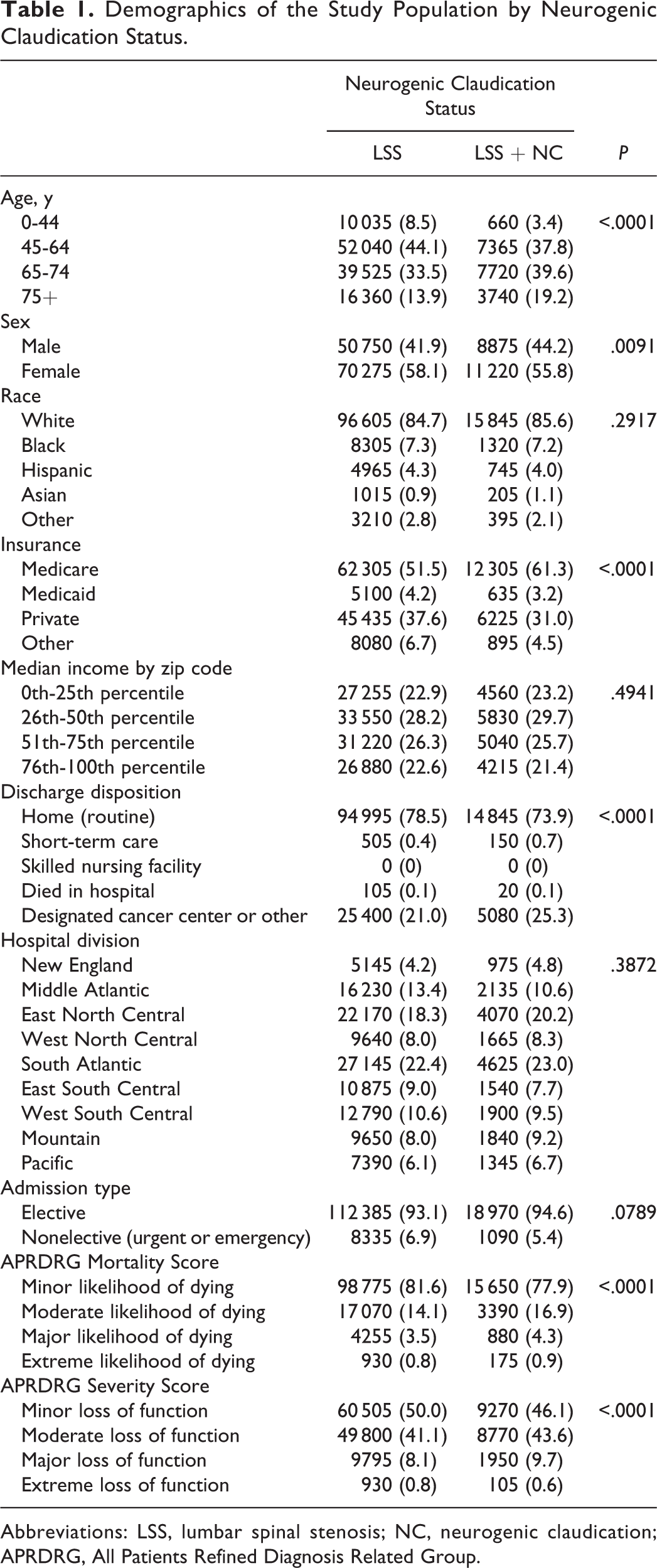
Abbreviations: LSS, lumbar spinal stenosis; NC, neurogenic claudication; APRDRG, All Patients Refined Diagnosis Related Group.
A higher proportion of LSS patients with NC also tended to have certain comorbid conditions compared to LSS patients without NC, including anemia from chronic blood loss (P = .0136), depression (P = .0174), diabetes mellitus with complications (P = .0011), hypertension (P < .0001), obesity (P = .0237), peripheral vascular disease (P = .0042), and renal failure (P = .0002) (Figure 1).
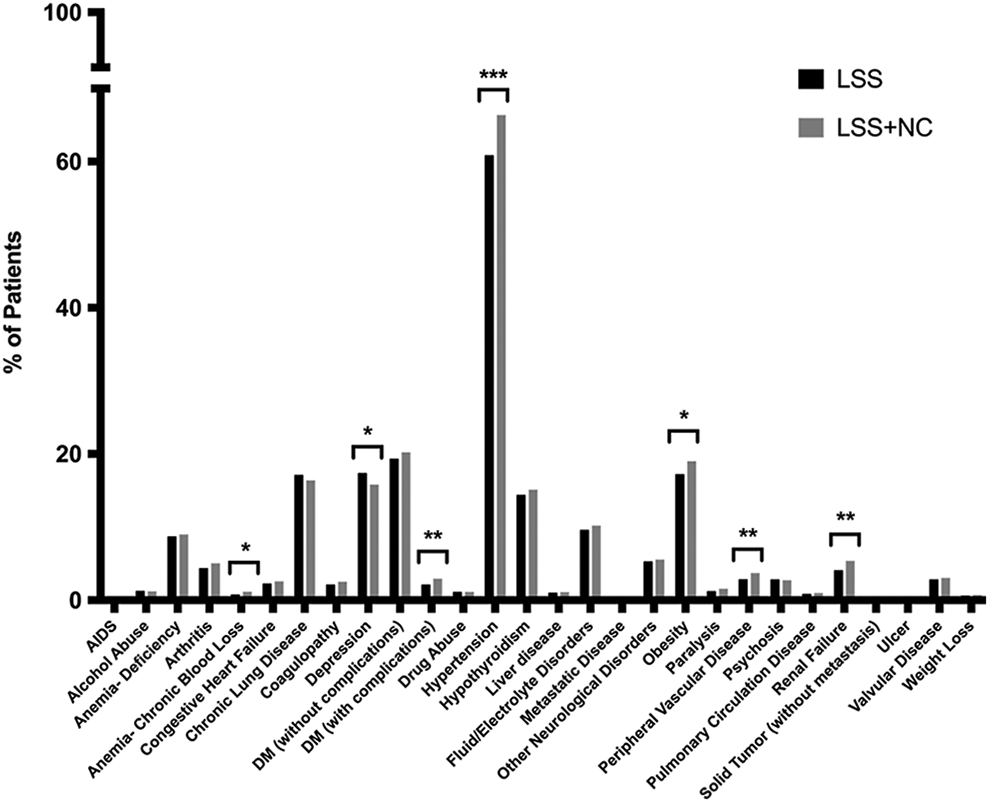
Comorbidity landscape of LSS patients with and without NC undergoing decompression and lumbar interbody fusion procedures. P < .05 was set as the threshold for statistical significance. *Indicates P < .05. **Indicates P < .01. ***Indicates P < .0001. LSS, lumbar spinal stenosis; NC, neurogenic claudication.
Further examination of baseline characteristics in the LSS patient cohorts revealed that patients with NC also had higher mean APRDRG Risk Mortality (P < .0001) and Disease Severity scores (P = .0003), as well as a greater number of diagnoses (P < .0001) and chronic conditions (P < .0001) on record (Table 2).
Differences in the Baseline Characteristics of the Study Population by Neurogenic Claudication Status.
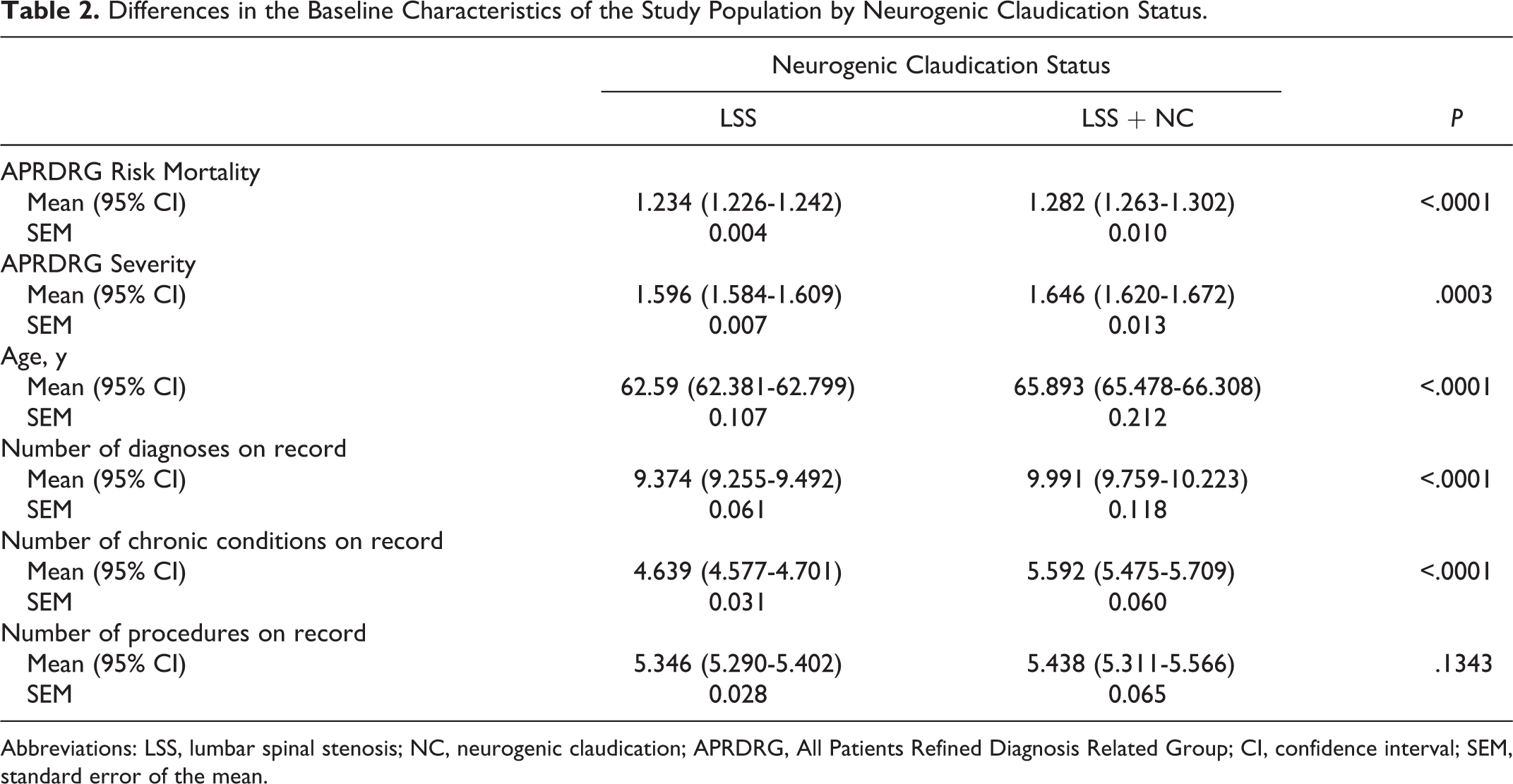
Abbreviations: LSS, lumbar spinal stenosis; NC, neurogenic claudication; APRDRG, All Patients Refined Diagnosis Related Group; CI, confidence interval; SEM, standard error of the mean.
Outcomes
Univariate regression models were built to examine how in-hospital mortality and complication rates varied according to NC status and procedure type (Table 3). In-hospital mortality rates did not differ between NC and non-NC patients, despite the NC group’s elevated APRDRG Risk Mortality scores. The NC group did, however, have a higher overall rate of complication (37.02%) compared with the non-NC group (33.94%) across all procedures (odds ratio [OR] 1.144; 95% CI 1.049-1.248; P < .0023). Repeating this analysis on specific procedural subsets revealed procedure-level differences in complication rates across LSS patients depending on NC status. For example, LSS patients with NC experienced higher odds of complication following an LLIF procedure (OR 1.145; 95% CI 1.031-1.273; P = .0118) but not ALIF (P = .2489) or PLIF (P = .0863) procedures.
Univariate Regression Models Evaluating the Impact of Neurogenic Claudiation Status on In-hospital Mortality and Complications by Procedure Type.
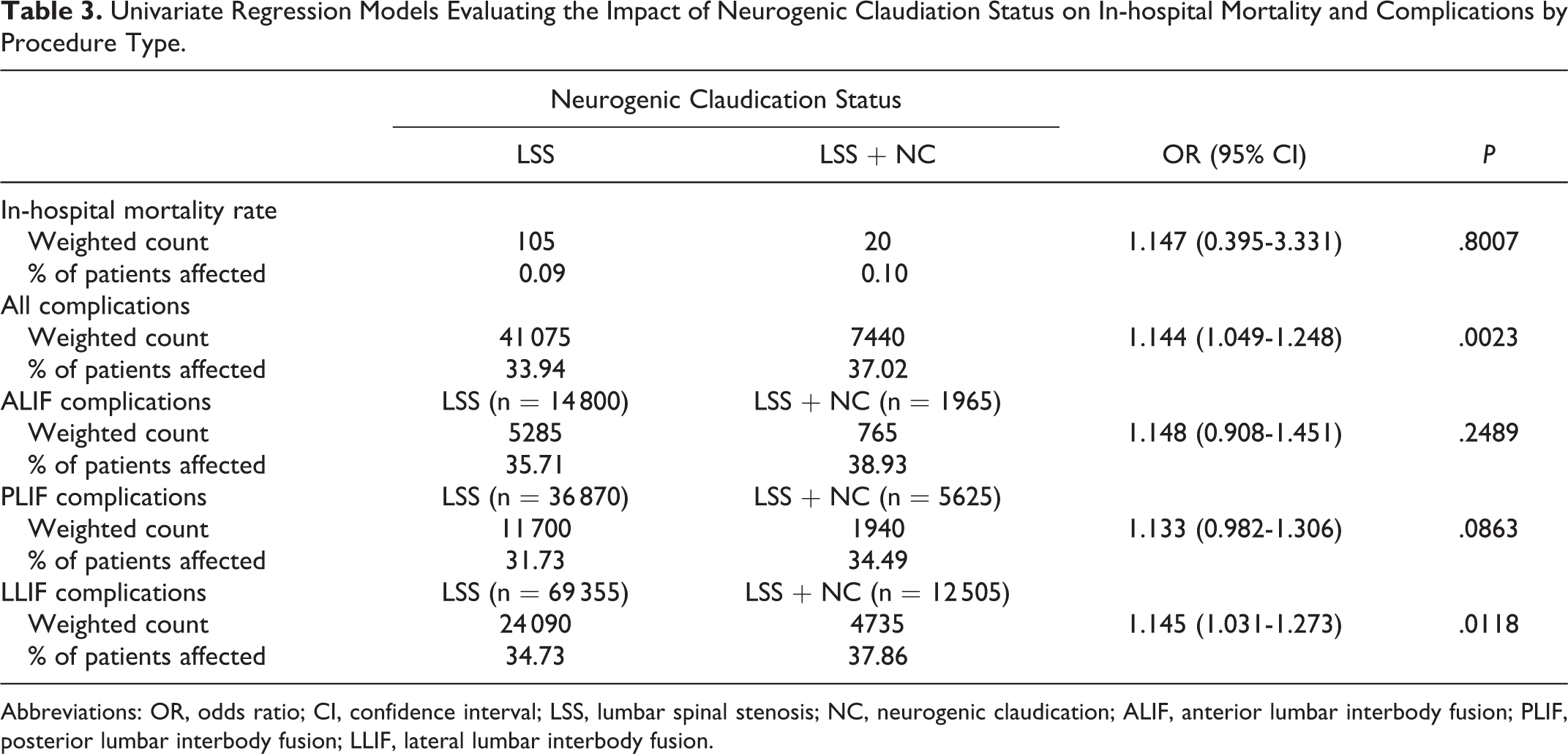
Abbreviations: OR, odds ratio; CI, confidence interval; LSS, lumbar spinal stenosis; NC, neurogenic claudication; ALIF, anterior lumbar interbody fusion; PLIF, posterior lumbar interbody fusion; LLIF, lateral lumbar interbody fusion.
Univariate regression analyses also examined the impact of NC status on certain complication risks by organ system using a selected set of common surgical complications categorized by organ system (Figure 2). This analysis revealed LSS patients with NC carried significantly higher odds of complication in certain organ systems, including renal (OR 1.347, 95% CI 1.106-1.640; P = .0030) and hematological complications (OR 1.193; 95% CI 1.085-1.313; P = .0003). Interestingly, patients with NC did not have significantly higher odds of neurological complications (P = .3664).
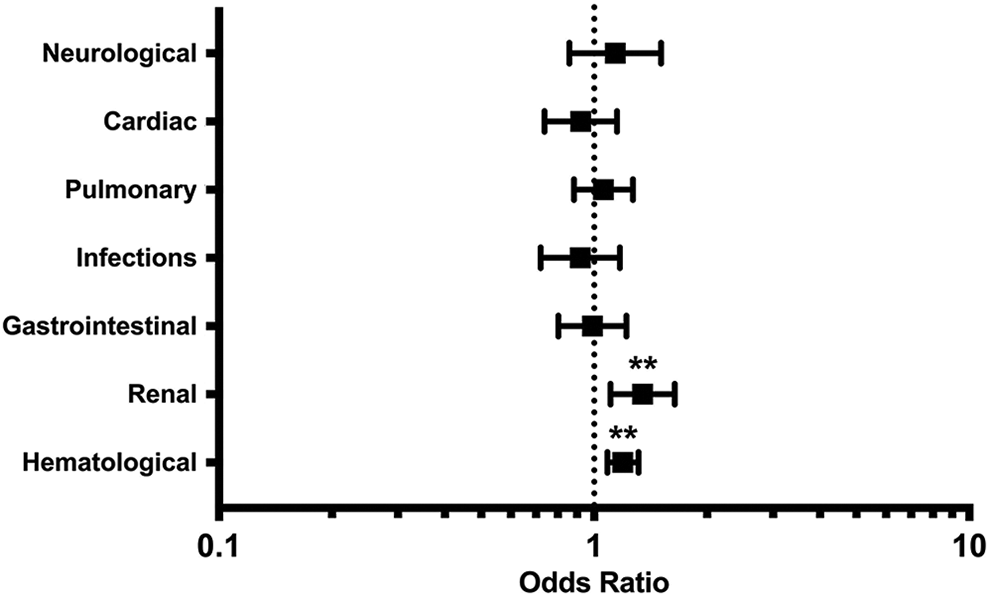
Odds ratios of complications by organ system following decompression and surgical fusion for LSS in patients with NC compared to those without NC. Odds ratios obtained through univariate logistic regressions. *Indicates P < .05. **Indicates P < .01. ***Indicates P < .0001. LSS, lumbar spinal stenosis; NC, neurogenic claudication.
A more detailed assessment of the complication profiles of these cohorts was obtained by building univariate regression models for specific perioperative complications that may result following surgery on the spine (Table 4). Among the 20 specific complications examined, patients with NC only had significantly higher odds of experiencing renal failure (OR 1.353; 95% CI 1.112-1.647; P = .0025) and postoperative anemia (OR 1.245; 95% CI 1.106-1.403; P = .0003) compared with patients without NC.
Univariate Regression Models Evaluating the Impact of Neurogenic Claudication Status on Certain Surgical Complications Across Organ Systems.
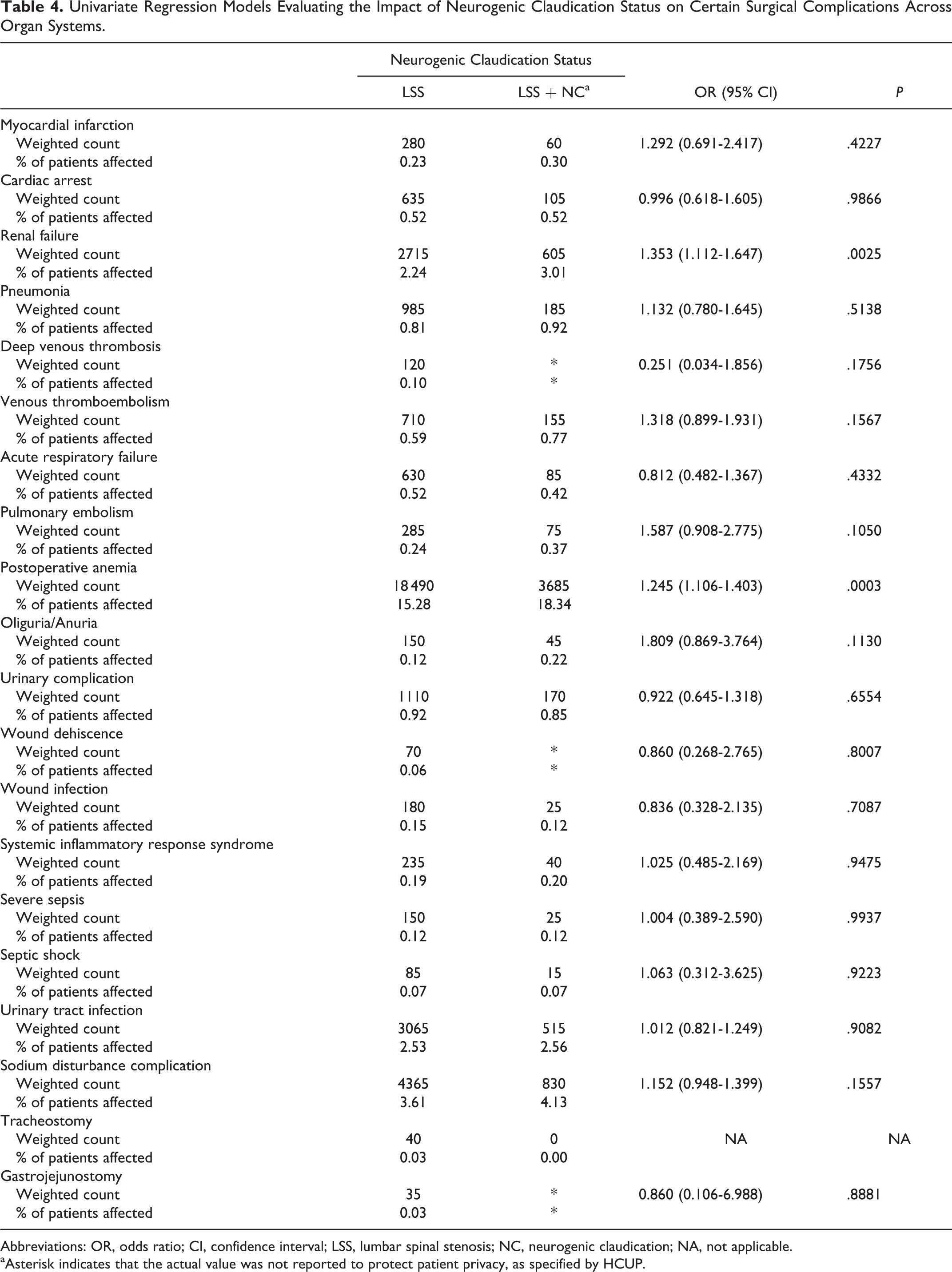
Abbreviations: OR, odds ratio; CI, confidence interval; LSS, lumbar spinal stenosis; NC, neurogenic claudication; NA, not applicable.
aAsterisk indicates that the actual value was not reported to protect patient privacy, as specified by HCUP.
Secondary outcomes and resource utilization metrics were also examined through univariate regression analysis to provide a more complete picture of how the outcomes between patients with and without NC group might differ following various lumbar interbody fusion procedures for LSS (Table 5). Patients with NC faced significantly higher odds of a nonhome discharge (OR 1.290; 95% CI 1.181-1.409; P < .0001). In addition, patients with NC did have higher odds of an extended hospitalization (OR 1.124; 95% CI 1.017-1.241; P = .0219), defined as a hospital stay greater than the 75th percentile of hospitalization lengths for the entire study population. Despite these findings, a total charges analysis revealed that there was not a significant difference between the average total charges for a hospital visit between patients with NC (mean $104 997; 95% CI $100 675-$109 318) and without NC (mean $109 226; 95% CI $106 507-$111 946) at the univariate level (P = .0512).
Univariate Regression Models Evaluating the Impact of Neurogenic Claudication Status on Resource Utilization and Secondary Clinical Outcomes.
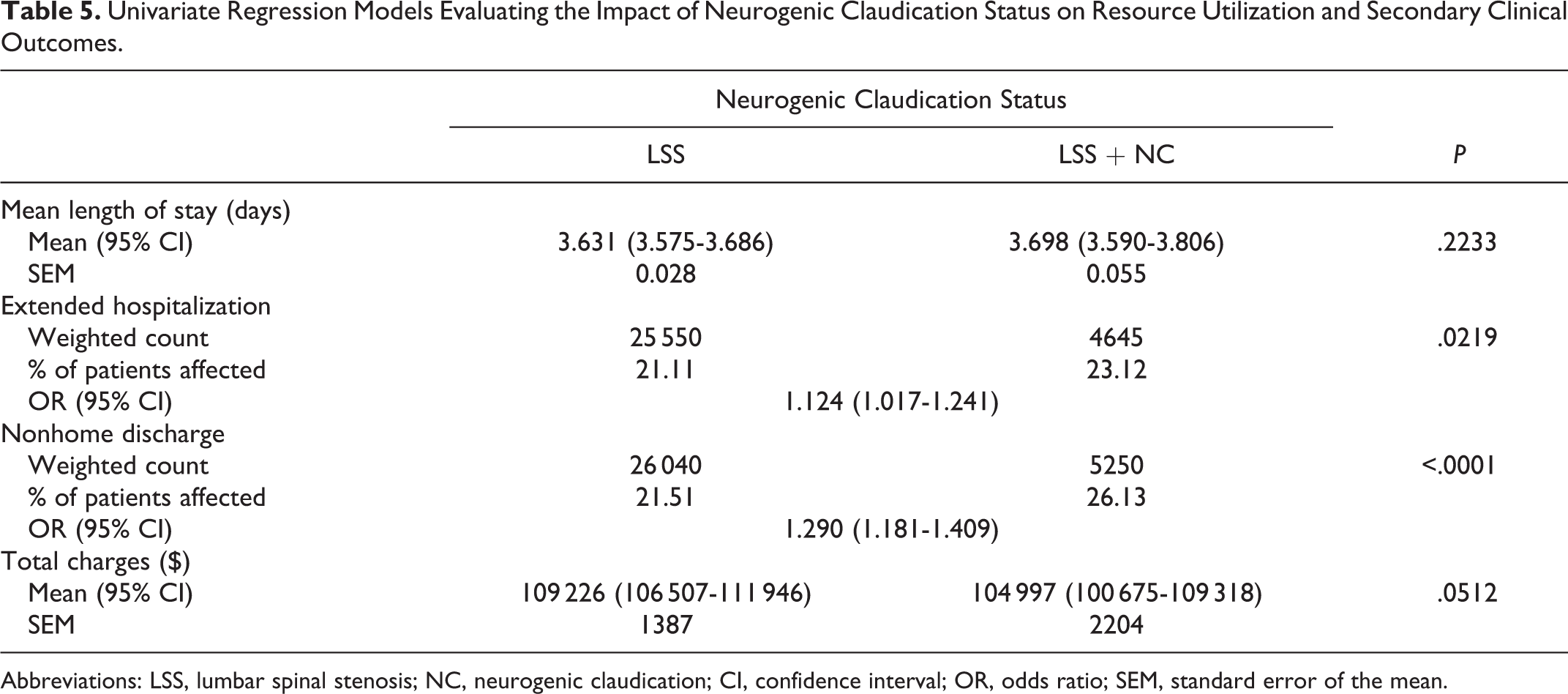
Abbreviations: LSS, lumbar spinal stenosis; NC, neurogenic claudication; CI, confidence interval; OR, odds ratio; SEM, standard error of the mean.
A series of multivariate regression models were constructed for each procedural technique to better evaluate how NC status impacted primary and secondary outcomes after controlling for key demographic and comorbidity variables. Interestingly, this analysis revealed that NC status did not significantly affect the odds of complication, nonhome discharge, or extended hospitalization across any of the procedure types after controlling for age, sex, race, primary payer status, hospital geographic division, and income quartile, as well as comorbidities, including chronic blood loss anemia, depression, diabetes mellitus with complications, hypertension, lymphoma, obesity, perivascular disease, and renal failure (Table 6). In addition, we noted a small but significant difference in total charges depending on the procedure type. Patients with NC actually experienced lower total charges than patients without NC following PLIFs (estimate = −$4893; standard error [SE] = $1275; P = .0001) and LLIFs (estimate = −$3,489; SE = $478; P < .0001), but not ALIFs (estimate = −$575; SE = $1034; P = .6121).
Multivariate Regression Models Evaluating the Impact of Neurogenic Claudication Status on Relevant Primary and Secondary Outcome Measures.a
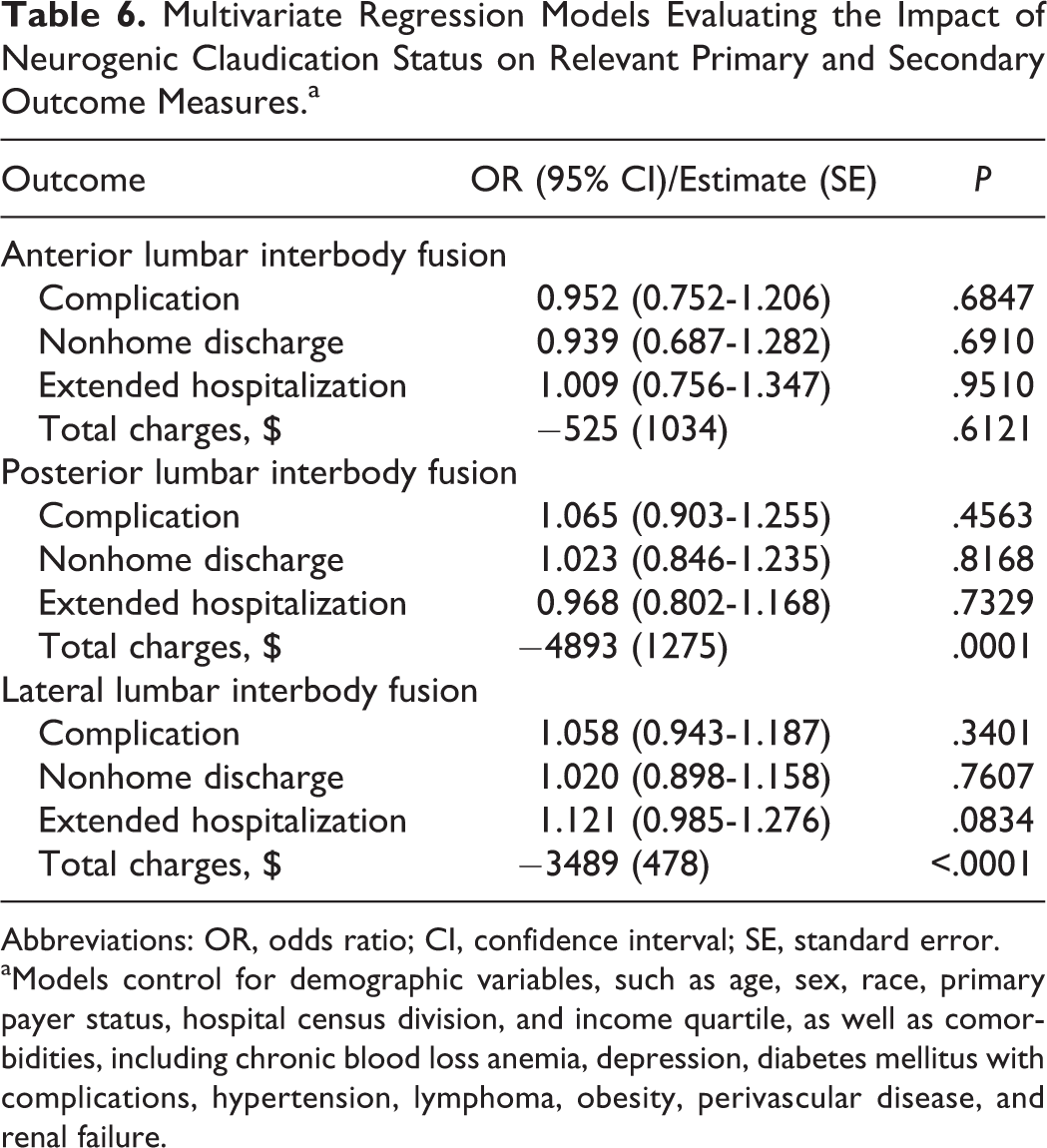
Abbreviations: OR, odds ratio; CI, confidence interval; SE, standard error.
aModels control for demographic variables, such as age, sex, race, primary payer status, hospital census division, and income quartile, as well as comorbidities, including chronic blood loss anemia, depression, diabetes mellitus with complications, hypertension, lymphoma, obesity, perivascular disease, and renal failure.
Discussion
Demographics and Comorbidities
Comparison of the demographic and comorbidity landscapes of LSS patients with and without NC revealed several important differences that would be of interest to neurosurgeons, neurologists, and other clinicians that often interact with these groups of patients. First, these groups showed statistically significant differences in the distributions of their ages, sex, primary insurance payer, and discharge disposition. In particular, LSS patients who also had NC tended to be older, male, insured by Medicare rather than a private payer, and nonroutinely discharged. Some of these population-level differences may suggest a less favorable clinical picture that is often associated with worse outcomes in previous studies of spine surgeries. In particular, previous studies have shown that older patients were more likely to experience more complications, in-hospital mortalities, and longer hospitalizations compared with the general adult population following various fusion and decompression surgeries. 16 A separate study focusing on elective lumbar spinal surgeries found that patients with private insurance have slightly greater improvement in their postoperative quality of life compared to patients with public insurance, though both groups experienced significant functional improvement overall postoperatively. 17
Similarly, we noted a significant difference in the prevalence of certain surgically relevant comorbidities between patients with and without NC. In particular, patients with NC were more likely to also have chronic blood loss anemia, depression, diabetes mellitus with complications, hypertension, obesity, peripheral vascular disease, and renal failure. Nearly all these comorbidities have been linked to worse clinical outcomes following spinal surgeries. 18 -22
Taken together, our analysis of the national populations of LSS patients suggest that those with NC carry important differences in their demographic and comorbidity profiles that could significantly affect their perioperative clinical outcomes and resource utilization following spinal surgery. While these findings alone present important considerations for surgeons and clinicians caring for these patients in the perioperative period, these variables must be carefully controlled for in statistical analysis between these 2 cohorts. Therefore, we constructed multivariate logistic regression models that account for these differences to better characterize how NC impacts clinical outcomes across various interbody fusion approaches for treating LSS.
Primary Outcomes: Complications and Mortality
Patients with symptomatic NC secondary to LSS represent an interesting cohort that has been studied within several medical and surgical contexts. However, no study to date has elucidated how the outcomes of this population compare to those of non-NC LSS patients following decompression and lumbar fusion procedures who likely presented with other symptomatology. Our study findings indicate that both groups showed low in-hospital mortality (<0.1% in each cohort), while the total complication rate across all 3 procedures was higher in patients with NC (P < .0023). However, when evaluating complication rate by independent procedure type, only LLIF remained significantly different. This observation could be due to the extent of stenosis where LLIF may be less suitable for severe stenosis, leading to more challenging procedures and greater rates of complications. 23 Extensive psoas muscle dissection and lumbar plexus neuropathies may also contribute to a higher complication rate.
Overall, systemic complication rates between these groups were relatively low and did not differ significantly. The fact that the presence of symptomatic NC does not affect outcomes may be due to the varying range of clinical presentation for similarly presenting radiographic disease. Correlation between radiographic findings, extent of disease, and clinical symptoms are often nonspecific and inconsistently demonstrated in the literature. 24,25 For example, one study prospectively assessed the relationship of symptomatic gait impairment in patients with LSS and found no correlation between severity of symptoms and extent of disease on magnetic resonance imaging. 26 As such, patients with more severe stenosis and worse clinical outcomes may be likely found in both the NC and non-NC cohorts, potentially offering a partial explanation as to why we observed similar clinical outcome profiles between the cohorts in this study.
Our analyses of clinical outcomes are also informative of the complexity of this patient population. Intuitively, a worse clinical presentation would lead to a more complicated and morbid postoperative course, however in this population, that is not the case. It is likely that the clinical presentation of NC in the population is inconsistent with the extent of LSS as well as other degenerative deformities, such as bony lateral recess stenosis and spondylolisthesis.
Secondary Outcomes: Resource Utilization
Comparison of the 2 LSS cohorts in this study through carefully controlled multivariate regression modeling found that the only significant difference in resource utilization was total charges. Interestingly, patients with NC had significantly lower total charges for their hospital visits than non-NC patients following PLIF and LLIF fusion approaches. One of the potential drivers of this effect might be related to NC patients experiencing more profound symptom relief after their operation, which in turn, could lead to decreased time to ambulation, decreased physical therapy utilization, and fewer assistive devices. These lower total charges may also, in part, be due to the potentially increased utilization of nonoperative therapies by symptomatic NC patients prior to their hospitalization for surgery. Patients who are symptomatic with NC secondary to LSS most likely seek nonoperative therapies prior to undergoing lumbar decompression and fusion. As such, the utilization of nonoperative management preoperatively may influence resource utilization and cost measures during the intrahospital and postoperative periods.
Though no studies have examined the direct effect that nonoperative care prior to hospitalization may have on intra- and postoperative costs and resource utilization, a retrospective study did review the costs for NC patients receiving nonoperative care prior to lumbar decompression and fusion and found a large preoperative cost burden with minimal clinical benefit. 27 Many of the patients in that study were using services such as chiropractors, physical therapists, and pain specialist prior to their procedure. Having these resources in place preoperatively may favorably influence patient length of stay and disposition from the hospital, thus reducing cost and improving resource utilization at the time of fusion.
It is important to note that while the results from this study and others provide some initial thoughts regarding the cost burden and efficiency of healthcare utilization in the perioperative period for these patient populations, further investigation is warranted to advance discussions of this topic in realms of policy, health care delivery, and research as LSS and NC are likely to become increasingly important issues in surgical spine practices.
Limitations
A primary limitation of this study was its retrospective design. Retrospective studies are unable to discern temporal relationships and may include selection bias in the data. A second limitation pertains to the inherent design of the NIS. The NIS does not track events that occur outside the hospital. Therefore, mortality and complications with delayed onsets may not be completely represented. A third limitation is that NIS data is accessed through ICD-9 codes, meaning that certain data not ICD-9-encoded could not be considered. These might include extent of spinal stenosis, severity of NC, anesthesia metrics, number of levels involved, intraoperative blood loss, surgery duration, or postoperative mobilization time. Finally, it is important to acknowledge that a certain degree of heterogeneity may underlie national-level data, as surgical cases occur under a variety of circumstances with surgeon- and team-level differences inherent to the practice. On the other hand, this intrinsic diversity may also enhance the generalizability of these findings.
Conclusions
NC is one of the most common symptomatic presentations for patients with LSS. Despite the high prevalence of LSS presenting with NC, no studies have investigated how LSS patients with NC fare in lumbar spinal surgery compared with LSS patients who do not have co-presenting NC. This is one of the first studies comprehensively characterize the effect that NC has on the clinical and economic outcomes following decompression with various lumbar interbody fusion procedures for LSS. Our results indicate that there are not obvious distinctions between outcomes in the 2 cohorts and support the need for prospective clinical studies to further assess outcomes by NC, as this knowledge could influence management of this challenging patient population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JMC reports receiving consulting fees from Zimmer Biomet.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.