
Abstract
Study Design:
Retrospective large database study.
Objective:
To determine the impact of cirrhosis on perioperative outcomes and resource utilization in elective spinal fusion surgery.
Methods:
Elective spinal fusion hospitalizations in patients with and without cirrhosis were identified using ICD-9-CM codes between the years of 2009 and 2011 using the Nationwide Inpatient Sample database. Main outcome measures were in-hospital neurologic, respiratory, cardiac, gastrointestinal, renal and urinary, pulmonary embolism, wound-related complications, and mortality. Length of stay and inpatient costs were also collected. Multivariable logistic regressions were conducted to compare the in-hospital outcomes of patients with and without cirrhosis undergoing spinal fusion.
Results:
A total of 1 214 694 patients underwent elective spinal fusions from 2009 to 2011. Oh these, 6739 were cirrhotic. Cirrhosis was a significant independent predictor for respiratory (odds ratio [OR] = 1.43, confidence interval [CI] 1.29-1.58; P < .001), gastrointestinal (OR = 1.72, CI 1.48-2.00; P < .001), urinary and renal (OR = 1.90, CI 1.70-2.12; P < 0.001), wound (OR = 1.36, CI 1.17-1.58; P < 0.001), and overall inpatient postoperative complications (OR = 1.43, CI 1.33-1.53; P < .001). Cirrhosis was also independently associated with significantly greater inpatient mortality (OR = 2.32, CI 1.72-3.14; P < .001). Cirrhotic patients also had significantly longer lengths of stay (5.35 vs 3.35 days; P < .001) and inpatient costs ($36 738 vs $29 068; P < .001).
Conclusions:
Cirrhosis is associated with increased risk of perioperative complications, mortality and greater resource utilization. Cirrhotic patients undergoing spinal fusion surgeries should be counseled on these increased risks. Current strategies for perioperative management of cirrhotic patients undergoing spinal fusion surgery need improvement.
Key Points
In spinal fusion surgery, cirrhosis was a significant independent predictor for respiratory, gastrointestinal, urinary and renal, wound, and overall complications.
Cirrhosis was a significant independent predictor of inpatient mortality (more than 2-fold) in spinal fusion surgeries.
Cirrhosis was also associated with increased length of stay and inpatient costs.
Cirrhotic patients undergoing spinal fusion surgery should be counseled on the increased risk of perioperative morbidity and mortality. Moreover, current perioperative management strategies for cirrhotic patients undergoing spinal fusion surgery need to be improved.
Introduction
Cirrhosis is a chronic condition that is characterized by irreversible liver fibrosis and can occur secondary to autoimmune conditions, hepatotoxic medications, alcoholism, viral hepatitis, or nonalcoholic fatty liver disease. 1,2 This chronic disease can lead to coagulopathy, malnutrition, ascites, encephalopathy, and impaired immunity, which can adversely affect postoperative outcomes. 1 -4 Cirrhosis has been identified as a significant risk factor for surgical wound complications, hematomas, and surgical site infections following total joint arthroplasty, aortic valve replacement, cardiac, and general surgery. 5 -10 Because of improvements in the medical care of cirrhosis, the prevalence of cirrhosis has increased over the past decade and thus the number of cirrhotic patients who undergo spine surgery is likely to increase as well. 11 Currently, there are no large-scale studies that have evaluated the prevalence of cirrhosis or assessed the impact of cirrhosis on inpatient mortality, complications, and costs in the elective spine surgery population on a national level.
The purpose of this study was to evaluate the inpatient postoperative outcomes and health care resource utilization of cirrhotic patients who underwent elective spinal fusion surgery using the Nationwide Inpatient Sample (NIS) database. We hypothesized that cirrhotic patients undergoing spinal fusion surgery had a significantly greater risk of inpatient complications and mortality, longer length of stay, and greater inpatient costs when compared to those without cirrhosis.
Materials and Methods
Database
This was a retrospective study of a large administrative dataset. The NIS database is maintained by the Healthcare Cost and Utilization Project (HCUP) and is the largest inpatient database in the United States, consisting of a 20% stratified sample of all hospital discharges. 12,13 For identification of procedures, diagnoses, and comorbidities, the database utilizes the International Classification of Disease Ninth Revision, Clinical Modification (ICD-9-CM). Given the de-identified, publicly available nature of this dataset, this study qualified for institutional review board exempt status under section 4 of 45 CFR46.101(b).
Sample Selection
The NIS database from years 2009 to 2011 was queried for all patients undergoing spinal fusion as defined by the Clinical Classification Software (CCS) code 158. The CCS is a categorization scheme developed by the HCUP to group ICD-9-CM codes into more clinically meaningful groups. 14 Any patients younger than 18 years were excluded. To further select for patients undergoing elective procedures, only those with degenerative pathologies were included, as defined by the ICD-9-CM codes of: 721.0-721.3, 721.4x, 722.0, 722.1x, 722.4, 722.5x, 722.7x-722.9x, 723.x, 724.00-724.03. 15 -19 ICD-9-CM codes (571.0, 571.2-571.4, 571.40 571.42 571.49 571.5, 571.6, 571.8, 571.9) were used to identify cirrhosis and separate the patients into 2 groups: those with cirrhosis and those without cirrhosis.
Outcomes
For each patient, the following data was collected: age, gender, race, hospital size, hospital teaching status, hospital region, and primary payer. Comorbidities were defined using the well-validated Elixhauser Comorbidity Index. 20,21 Charges, costs, and length of stay were also extracted from the database. Complications were assessed using the following ICD-9-CM codes: neurologic complications (997.00-997.09); respiratory complications (518.4, 518.5, 518.81-518.84 997.3); cardiac complications (410 997.1); gastrointestinal complications (535.0 570 575.0, 577.0, 997.4); renal and urinary complications (584 997.5); pulmonary embolism (415.1); and wound-related complications (998.1, 998.3, 998.5, 998.83 999.3). 22
Data Analysis
The data set was weighted using the supplied discharge weights to produce national estimates.
T tests were used to compare continuous variables and chi-square tests were used to compare categorical variables. To determine the impact of cirrhosis on inpatient complications and inpatient mortality, multivariable logistic regressions were performed while controlling for age, sex, race, Elixhauser Comorbidity Index, hospital size, hospital teaching status, hospital region, and primary payer type. Statistical analysis was conducted in SPSS Version 21 (IBM Corp, Armonk, NY). Statistical significance was set at P < .05.
Results
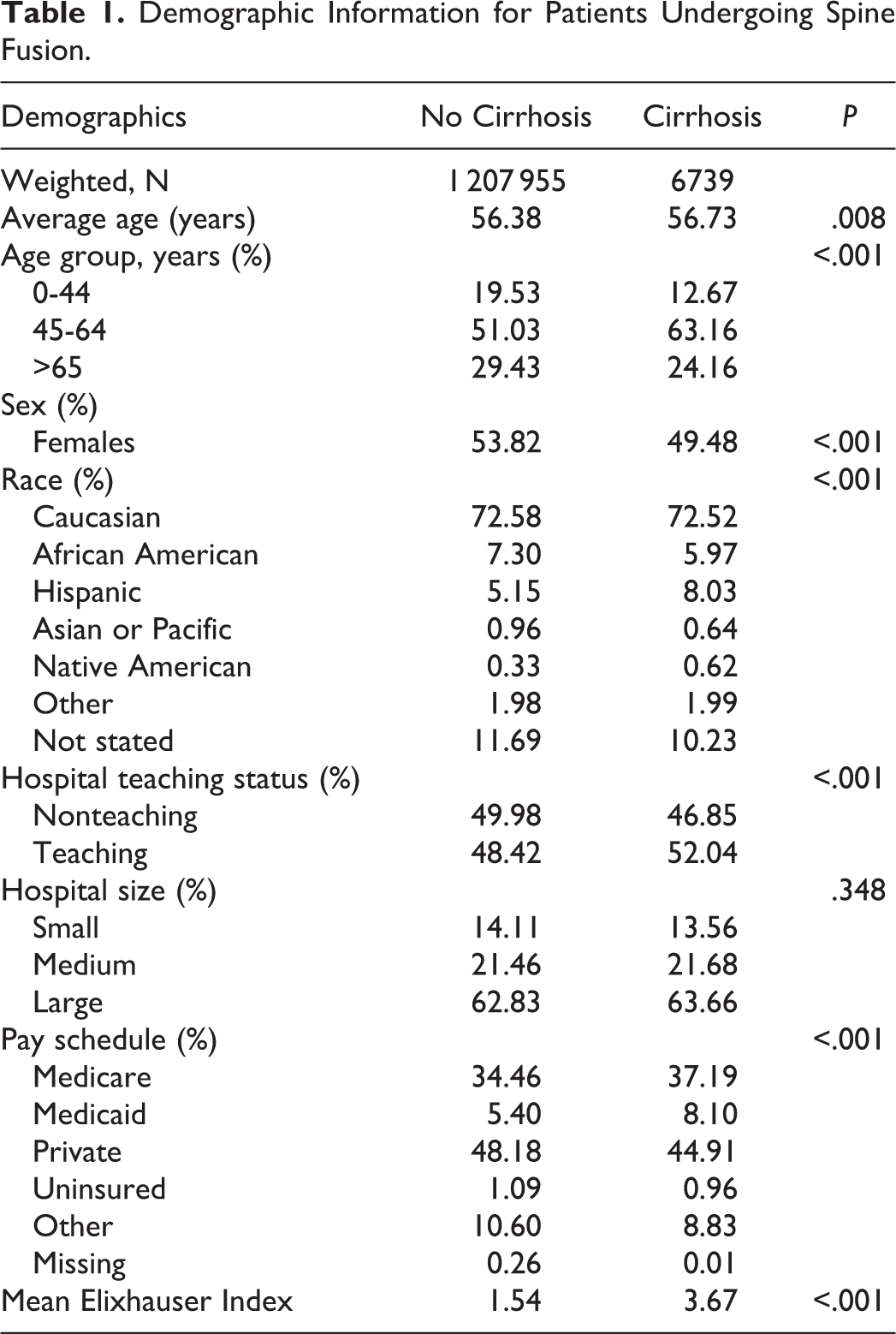
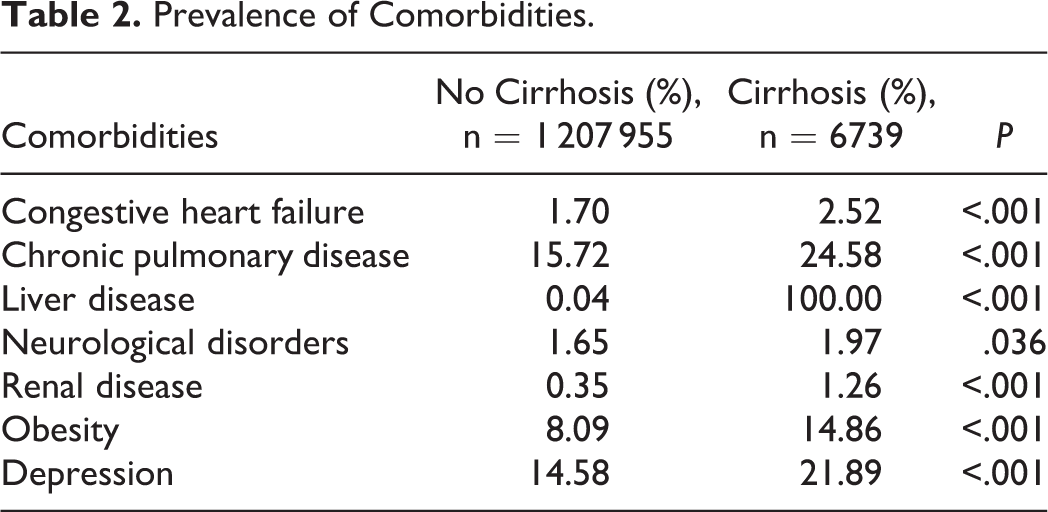
A total of 1 214 694 patients who underwent spinal fusions were identified. From this population, 6739 (0.55%) had a diagnosis of cirrhosis. Compared with noncirrhotic patients, cirrhotic patients were of similar age (56.7 vs 56.3 years) and slightly more likely to be male (50.5% vs 46.2%; P < .001; Table 1). In the cirrhosis population, there was a significantly greater prevalence of congestive heart failure, chronic pulmonary disease, neurological disorders, renal disease, obesity, and depression (Table 2). The overall comorbidity burden as measured by the mean Elixhauser Comorbidity Index was significantly greater in cirrhotic patients (3.67 vs 1.54; P < .001).
Demographic Information for Patients Undergoing Spine Fusion.
Prevalence of Comorbidities.
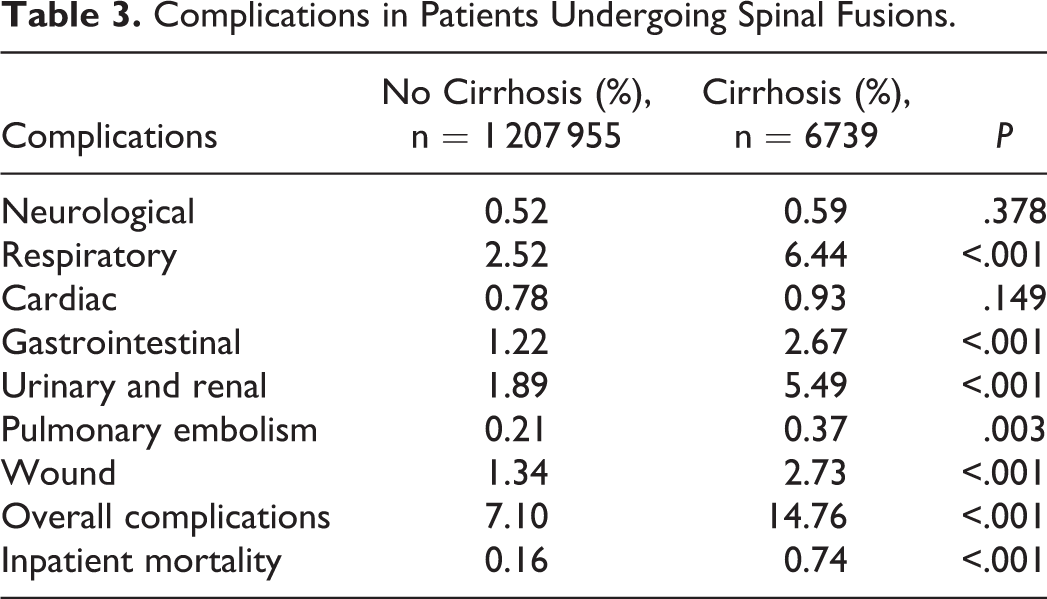
Rates of cardiac (0.93% vs 0.78%; P = .149) and neurological complications (0.59% vs 0.52%; P = .378) were not significantly different between cirrhotic and noncirrhotic patients. However, the rates of respiratory, gastrointestinal, urinary and renal, pulmonary embolism, surgical wound, and overall complications were significantly greater in patients with cirrhosis compared to those without cirrhosis. Importantly, the rate of inpatient mortality was significantly greater in patients with cirrhosis compared to those without cirrhosis (0.74% vs 0.16%; P < .001; Table 3).
Complications in Patients Undergoing Spinal Fusions.
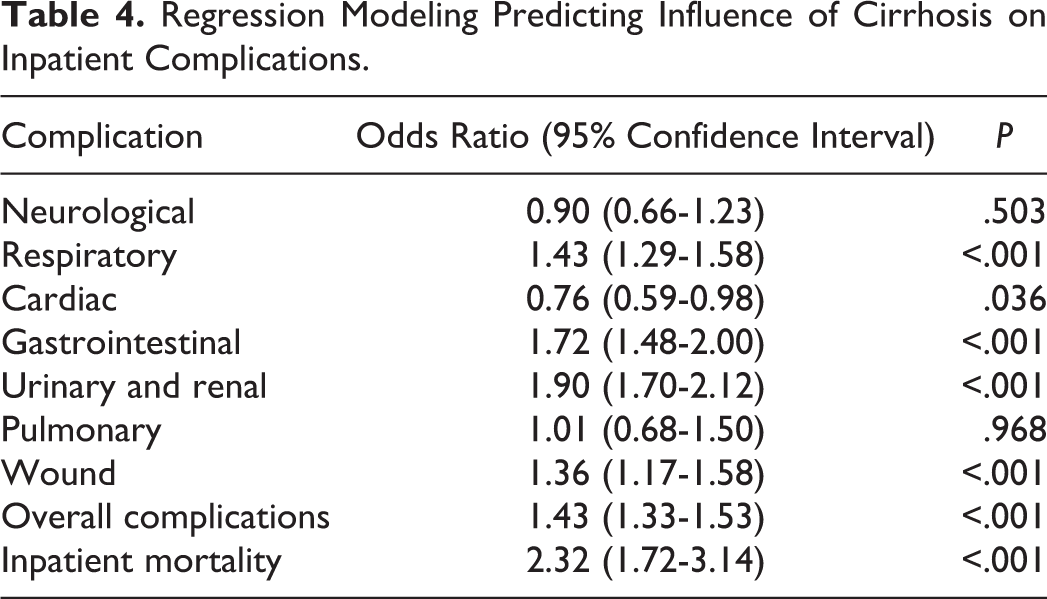
After controlling for patient and hospital baseline characteristics, multivariate regression analysis demonstrated that cirrhosis was a significant independent predictor of greater overall inpatient complications (odds ratio [OR] = 1.43, confidence interval [CI] 1.33-1.53; P < .001). Specifically, cirrhosis was found to be a significant independent predictor of gastrointestinal (OR = 1.72, CI 1.48-2.00; P < .001), urinary and renal complications (OR = 1.90, CI 1.70-2.12; P < .001), wound complications (OR = 1.36, CI 1.17-1.58; P < .001), and respiratory complications (OR = 1.43, CI 1.29-1.58; P < .001). Cirrhosis was found to be associated with significantly reduced cardiac complications (OR = 0.76, CI 0.59-0.99; P < .036). The odds ratios for pulmonary embolism (OR = 1.01, CI 0.68-1.50; P = .968), and neurological complications (OR = 0.90, CI 0.66-1.23; P = .503) did not reach statistical significance. Importantly, cirrhosis was found to be a significant independent predictor of inpatient mortality (OR = 2.32, CI 1.72-3.14; P < .001; Table 4).
Regression Modeling Predicting Influence of Cirrhosis on Inpatient Complications.
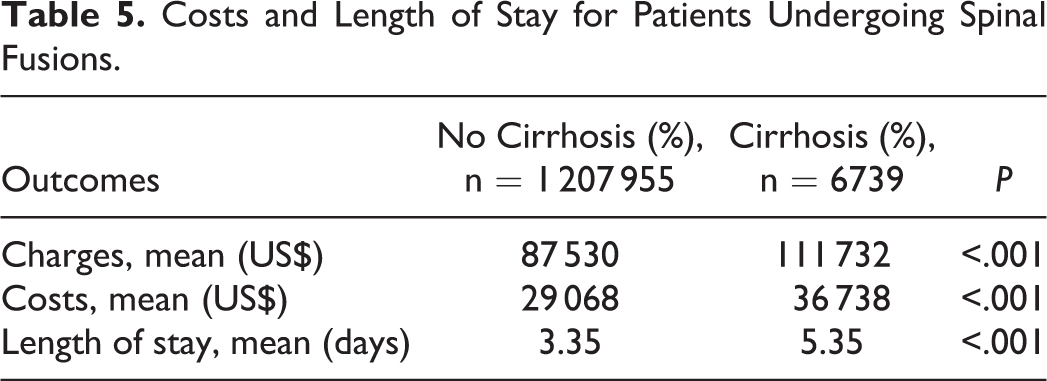
For resource utilization, patients with cirrhosis demonstrated significantly greater inpatient costs ($36 738 vs $29 068, P < .001) and significantly longer length of stay (5.35 vs 3.35 days; P < .001; Table 5).
Costs and Length of Stay for Patients Undergoing Spinal Fusions.
Discussion
The identification and understanding of surgical risk factors are critical components in surgical decision making and perioperative medical management in spine surgery. Cirrhosis represents an important surgical risk factor as portal hypertension, encephalopathy, infection, sepsis, ascites, and coagulopathy are medical problems that can occur in the postoperative period, leading to increased rates of complications, longer length of stay, greater health care resource utilization, and higher perioperative mortality rates. 1,2,5,6,8-10,23,24 However, the impact of cirrhosis on elective spinal fusion surgeries on a national level was unknown.
From 2009 to 2011, the incidence of cirrhosis in elective spinal fusion surgery was 0.55%, which was greater than the national prevalence of cirrhosis of 0.27%, highlighting the importance of understanding this risk factor in spine surgery. 11 Multivariable analysis that adjusted for patient demographics, hospital characteristics, and medical comorbidities demonstrated that cirrhosis was a significant independent predictor of inpatient mortality (with odds ratio greater than 2-fold) as well as respiratory, gastrointestinal, urinary and renal, wound, and overall inpatient complications following elective spinal fusion surgeries. Patients with cirrhosis also had significantly longer hospital lengths of stay and inpatient costs.
These results are consistent with a recent study that evaluated the impact of cirrhosis in the cervical spine trauma patient population. 25 Bessey et al 25 conducted a retrospective study using the Massachusetts statewide inpatient database that evaluated 10 841 patients who sustained cervical spine trauma. From this population, 117 patients were identified as having chronic liver disease. 25 Similar to our analysis, the study found that cirrhosis was independently associated with greater rates of inpatient mortality, failure to rescue, and overall inpatient complications. 25 However, in this study population, only 24 cirrhotic patients underwent surgery and thus this small sample size limited the interpretation of these findings regarding the impact of cirrhosis on spine surgical outcomes. 25 Furthermore, this analysis evaluated cervical spine trauma population rather than an elective spinal surgery population. 25
A retrospective study by Liao et al 26 evaluated cirrhosis in lumbar spine surgery using a cohort of 58 patients (29 cirrhotic and 29 noncirrhotic patients). There was a significantly higher complication rate in the cirrhotic group compared with the noncirrhotic group and the incidence of complications was significantly greater in patients with more severe cirrhosis. 26 However, due to limited sample size, the study was unable to assess the impact of cirrhosis on inpatient mortality, as there was only 1 inpatient death in the entire study population. 26 Other studies that evaluated the outcomes of pyogenic spine infections or surgical treatments for epidural abscesses also found that cirrhosis was associated with greater rates of complications. 27,28 In turn, our findings were consistent with prior studies that were conducted with smaller cirrhotic patient populations.
Our study has several limitations that are inherent to large database analyses. We were unable to determine the severity of cirrhosis from the NIS database and thus were unable to evaluate the relationship between the severity of cirrhosis and outcomes following spine surgery. The NIS database also does not contain information on preoperative medical management of cirrhosis or long-term postdischarge outcomes including postdischarge mortality or readmission rates. Moreover, the NIS database relies on clinical coding and diagnosis entry and therefore there may be inaccuracy, bias or lapses in coding for cirrhosis. Additionally, because of the limitations of our analysis, we were unable subgroup patients at different spinal fusion levels, which would be of interest to identify differences based on level of fusion. Our study also only includes NIS data from 2009 to 2011 and thus lacks more recent datapoints. Given advances in medical management of cirrhosis, a future study is needed to evaluate the current impact of cirrhosis on inpatient outcomes following spinal fusion. Despite these limitations, our study is the first large-scale analysis that demonstrated that cirrhosis is an important risk factor in spinal fusion surgeries that requires careful preoperative medical evaluation and optimization and postoperative care.
Although further research is needed to determine the utility of cirrhosis screening in spine surgery, the use of liver function tests in at-risk patients (history of intravenous drug abuse or alcoholism) may help identify those with previously unrecognized cirrhosis who may be at a higher risk of developing postoperative complications. In cases of diagnosed cirrhosis, preoperative medical management should include correction of any nutritional deficiencies, assessment of liver disease severity, and optimization of hepatic function. 1,4,29,30 Specifically, Child-Turcotte-Pugh and Model for End-Stage Liver Disease scores should be calculated preoperatively to determine the severity of liver disease and hepatic function.
Intraoperatively, collaboration with anesthesiologists with experience managing cirrhosis may be helpful as inappropriate fluid management can result in peripheral edema and worsening ascites. 1,31 During the postoperative period, cirrhotic patients need to be carefully monitored and treated for signs of ascites, infection, surgical site bleeding, and encephalopathy. 1,4 In addition, analgesics should also be carefully administered as hepatic metabolism and clearance of various medications may be impaired. 1,32 In turn, consultation with a hepatologist should be considered to help with evaluation and characterization of surgical risk, preoperative medical optimization, and postoperative management of cirrhosis.
In conclusion, on a national level cirrhosis is a significant independent predictor of inpatient complications and mortality and is associated with significantly higher healthcare resource utilization in spinal fusion surgeries. These findings may be useful for surgical decision making, patient counseling, and perioperative medical management. Moreover, further research is needed to determine strategies and protocols to improve the current medical management of cirrhotic patients undergoing spinal fusion surgery. Collaboration with associated medical specialists is critical in the perioperative management of such patients and may have an impact in minimizing complications.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.