
Abstract
Study Design:
Retrospective case series.
Objectives:
An increasing focus has been placed on removing implicit (unconscious) bias from the surgical selection process. In spine surgery, there is the potential for implicit bias to affect the decision to either operate on a patient or not, given lack of definitive surgical indications for many elective procedures. The objective of this study was to analyze the surgical decision making of a single spine surgeon in an effort to understand surgical decision-making trends based on certain demographic factors.
Methods:
This was a retrospective study of 484 patients who had undergone a corrective procedure for cervical myelopathy by an orthopedic spine surgeon at our institution. The preoperative modified Japanese Orthopaedic Association score served as the metric of severity of disease for cervical myelopathy. The factors that have been associated with implicit bias that were evaluated were smoking status, narcotic use status, gender, body mass index, and age.
Results:
Multivariate linear regression analysis showed that even after controlling for comorbidities and confounders, the only variable which predicted likelihood to operate on a patient of a milder symptomology was age (odds ratio [OR] = −0.138; (confidence interval [CI] = −0.034 to −0.006). The other factors (smoking status, narcotic use status, gender, and body mass index) were not associated with surgical decision making.
Conclusions:
Our study demonstrates absence of association between commonly studied areas of implicit bias and the decision to operate on a patient with milder symptomology at initial presentation of cervical spondylotic myelopathy.
Introduction
A growing awareness of the impact of implicit associations (unconscious biases) on human behavior has led to much research aimed at characterizing these patterns and documenting their potential to lead to unequal treatment across patient groups. 1 Implicit bias (IB) involves a conflict between what a person explicitly believes and has been taught and what a person may unconsciously associate with a group or demographic cohort. 2 With the introduction of the Implicit Association Test (IAT), researchers have been able to characterize a wide variety of potential implicit associations. 3 Literature demonstrates evidence of anti-black IB in health care workers. 2 Other factors such as sexual orientation, gender, and ethnicity are other sources of IB. 4 Additionally, emerging evidence demonstrates IB in relation to other factors such as against those with a past history of drug or narcotic abuse or in favor of those who appear younger. 5 Age bias, as this latter phenomenon is known, has been well described and affects the likelihood of an individual being hired for a job, especially those which require face-to-face customer service. 6 Additional documented IBs include antismoking bias, antiobesity bias, and gender bias. 7 -11
Cervical myelopathy is a common pathology of the cervical spine causing significant morbidity across the country. Generally, cervical spondylotic myelopathy (CSM) results from spinal canal stenosis following degenerative osteoarthritis of the vertebra. Outcomes after corrective procedures for cervical myelopathy are variable, and overall efficacy has been associated with being lower in various demographic cohorts. 12 -16 Given variable patient performance after operative management of CSM, there is potential for surgeon bias in the decision-making process. It is worthwhile to determine which factors spine surgeons may be using in the surgical decision-making process. By so doing, eventual awareness of IB may surface. Additionally, explicit biases that may or may not be acceptable given current literature regarding increased surgical risk seen in certain demographics can be evaluated.
The purpose of this study was to uncover certain biases (whether intentional or unintentional) in the selection process for patients undergoing procedures of the cervical spine. We hypothesized that patient with nonsmoker status, female gender, non–narcotic user status, younger age, and decreased body mass index (BMI) would be more likely to be offered a spine procedure regardless of disease severity.
Methods
Data Collection
This study was a single-center retrospective study of 484 patients who had undergone a corrective procedure for cervical myelopathy (cervical laminectomy, discectomy, or fusion) by an orthopedic spine surgeon at our institution from May 24, 2014 to August 16, 2018. We chose to include patients from only 1 surgeon intentionally to eliminate potential surgeon-specific confounding factors as discussed in the article by MacDermid et al. 17 The institutional review board of Emory University School of Medicine approved the creation of the database utilized for this study. A priori power analysis was performed and a target sample size of 400 patients was obtained. Smoking status, narcotic use status, gender, and body mass index (BMI) were recorded at time of initial preoperative visit. Additionally, relevant comorbidity data such as hypotension, diabetes mellitus, or less common medical issues such as rheumatoid arthritis or history of malignancy were recorded. A trained physician with experience in assessing patients with cervical myelopathy read through each initial preoperative patient visit chart and assigned an independent preoperative modified Japanese Orthopaedic Association (mJOA) score to each patient based on presence or absence of symptoms in the history of present illness. The preoperative mJOA score served as the metric of severity of disease for cervical myelopathy, as has been done in previous studies evaluating outcomes after corrective procedures for cervical myelopathy. 18
Disease Severity Groupings
After retrospective chart review, patients were grouped into having mild, moderate, or severe disease based on mJOA at time of initial preoperative patient visit: mild (mJOA of 15-17), moderate (mJOA of 12-14), and severe (mJOA < 12). These classifications were chosen based on literature which classifies degree of severity based on these criteria of mJOA. 19 The control group was defined to be the severe mJOA group (mJOA < 12)—the patients who would almost certainly be recommended surgery regardless of demographic grouping due to the crippling burden of their CSM. The test groups were the mild and moderate groups—patients whose demographic characteristics may be biasing a surgeon toward operating upon them or not, given more minor symptomology of CSM.
Statistical Analysis
SPSS was used to record descriptive stats for each of the variables and a multivariate logistic regression was run to control for confounders and assess for differences in mJOA in sex, smoking status, BMI groupings (20-25, 25-30, >30 kg/m2), age (0-60, 61-70, 71-80, >81 years), and narcotic use cohorts. Preoperative medical comorbidities (diabetes mellitus, hypertension, and other less common comorbidities such as rheumatoid arthritis) were included in the regression analysis to control for such factors that are strong potential confounders affecting the decision to proceed with surgical correction of CSM. A P value <.5 was considered statistically significant for all tests.
Results
After completing chart review and excluding patients who did not meet study criteria, a sample size of 446 patients who had received corrective procedures for cervical myelopathy from a single surgeon at our institution was obtained. Thorough chart review was completed on each of these patients. Of these patients, 248 were male and 198 were female (Table 1). After grouping patients by severity of disease, 138 patients were found to have mild disease while 245 and 63 patients were found to have moderate and severe disease, respectively. Seventy-seven of the patients were smokers and 249 patients were narcotic users. A total of 184 patients had a relevant comorbidity such as hypotension, diabetes mellitus, or less common medical issues such as rheumatoid arthritis or history of malignancy. Overall, 262 patients did not have a relevant medical comorbidity. The majority of the patients included in the analysis were not smokers (369), while 77 patients reported a history of smoking.
Patient Demographic Characteristics.
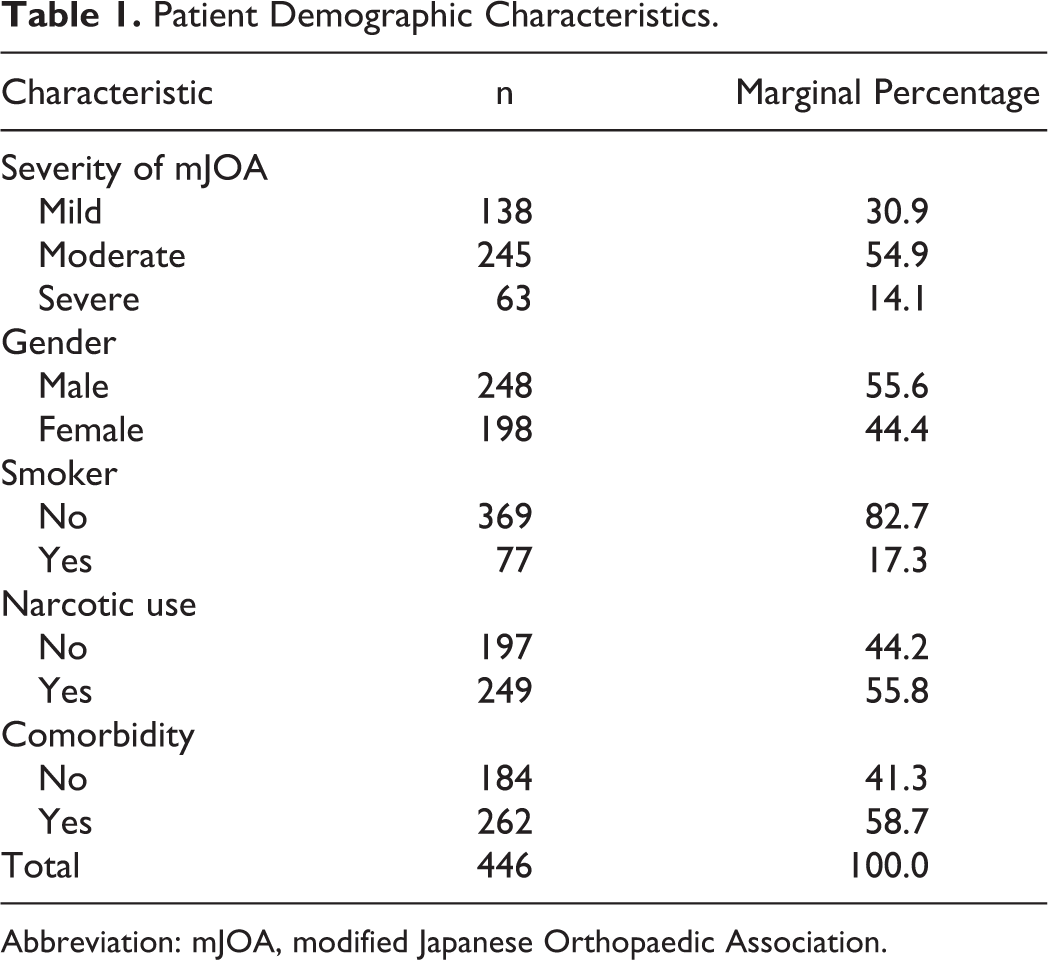
Abbreviation: mJOA, modified Japanese Orthopaedic Association.
Multivariate linear regression analysis showed that even after controlling for comorbidities and confounders, the only variable that predicted likelihood to operate on a patient of a milder symptomology was age (odds ratio [OR] = −0.138; confidence interval [CI], −0.034 to −0.006). As age increased, there was a negative likelihood of operating on patients with disease in the mild severity grouping.
Multivariate linear regression analysis demonstrated that the other variables of interest were not associated with the decision to operate (Table 2). While all of the odds ratios of the variables of interest were negative (indicating a negative likelihood of operating on patients with disease in the mild severity grouping if the patients were in the category of interest), none of these associations was statistically significant. Gender was not associated with the decision to operate (OR = −0.076; CI = −0.611 to −0.065). Additionally, BMI (OR = −0.022; CI = −0.034 to 0.021) and presence of comorbidity (OR = −0.040; CI = −0.491 to 0.200) were not associated with the operative decision. Last, status as a narcotic user (OR = −.051; CI = −0.524 to 0.152) or smoker (OR = −0.074; CI = −0.807 to 0.105) was not associated with the decision to operate.
Beta Coefficients and Significance of Potential Sources of Implicit Bias on Degree of Severity of Myelopathy.a
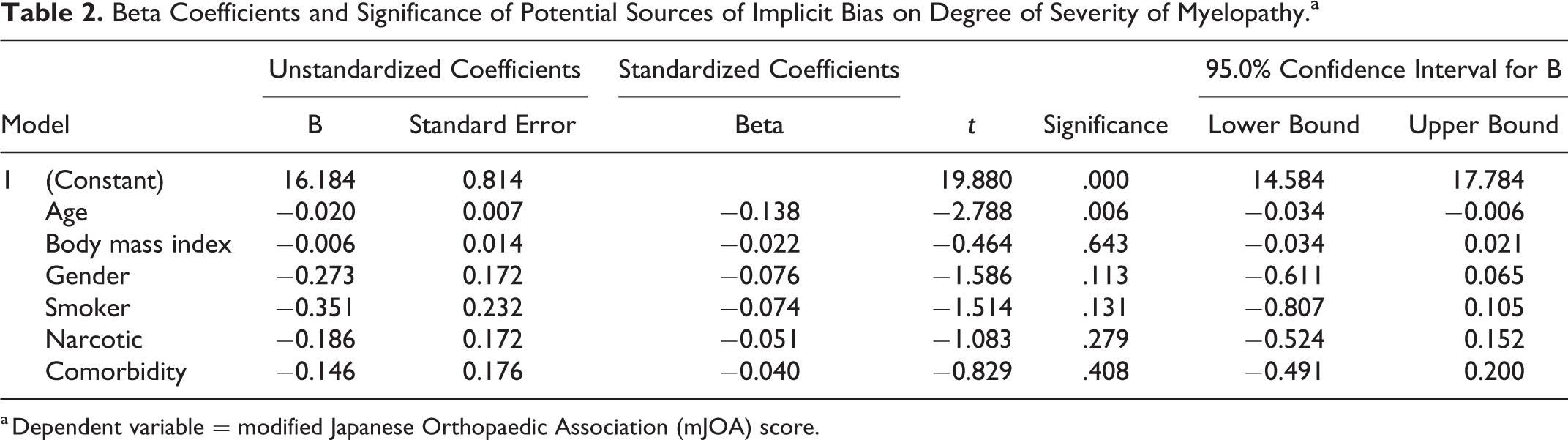
a Dependent variable = modified Japanese Orthopaedic Association (mJOA) score.
Discussion
This study aimed to assess orthopedic spine surgeon bias against smoking status, female gender, increased BMI, older age, and narcotic-use status. A sample of 446 patients undergoing corrective procedures for CSM was analyzed. The primary outcome was severity of CSM at the time of surgery with the goal of determining if any of these potential areas for IB affects the severity of disease which will meet the threshold to consider operative intervention. Of all the areas of potential for IB, only age was correlated with choosing to operate on patients of milder symptoms of CSM.
Age Bias Versus Appropriate Clinical Decision Making and Natural Disease Progression
Advancing age was associated with higher severity of symptomology of CSM at the time of operation. This finding indicates that surgeons are hesitant to operate on older patients unless they have very severe disease. It is difficult to assess if this hesitancy is due to a form of age bias, or if such clinical decision making is based on evidence-based practice. Advanced age is a well-known factor associated with higher mortality rate and rates of adverse outcomes, and a recent report by Massarweh et al 20 demonstrates that the rate may be even higher than previously thought. Indeed, given the increased mortality seen in older patients, choosing to operate on a patient with mild symptoms who is less likely to benefit as significantly as a patient with more severe symptoms may be a poor decision. However, the possibility of the existence of an age bias must be entertained, as it is possible that some individuals of advanced age may not be receiving an appropriately indicated surgery purely based on age and without the completion of a through risk-benefit assessment.
Other Areas of Implicit Bias
Our study also evaluated for the presence of IB against smoking status, narcotic use status, gender, and obesity. We did not find that any of these factors were associated with operating on individuals with more severe symptomology when compared to normal cohorts. This data conflicts with much existing literature demonstrating the presence of IB against individuals within these demographic cohorts in the health care setting. 2,4
Tobacco use disorder constitutes an area of well-documented IB. Smoking rates are dropping across the country and tobacco use is becoming more confined to lower-income brackets. 7 The literature demonstrates that practitioners have begun viewing smokers as having less concern for personal health and being less deserving of expensive medical therapies. 7 With regard to surgical decision making, smoking and use of other nicotine containing products is an important factor for consideration, given vasoconstrictive properties of nicotine, which have been shown to affect healing and postoperative outcomes. 21 Still, IB against smokers must be separated from legitimate concerns about outcome balance with risk of surgery. Likewise, narcotic use has been associated with practitioner mistrust of a patient. 5 Additionally, this relationship appears to be inversely true as well, with patients who suffer from opioid dependence having been shown to be warry of provider mal-intention. 5 However, preoperative narcotic use is an independent risk factor for higher rates of postoperative pain, rendering surgical intervention less beneficial in certain cases. 22 Again, a provider’s IB against such cohorts must be considered in light of higher operative risk in smokers and narcotic users.
Body composition constitutes another factor against which IB is common, as individuals who have elevated BMIs are seen as “unproductive” and “unconcerned about their health.” 10 Like smoking status, obesity is an independent risk factor associated with complication rates and poor postoperative functionality. 23 In orthopedics, the total joint literature demonstrates consistent poor functional scores and higher adverse outcomes in morbidly obese populations, leading to several authors suggesting a hard BMI cutoff of 40 kg/m2 for individuals being evaluated for total hip and knee arthroplasty. 23 These findings are consistent in other surgical fields. BMI has been linked to adverse effects in major gastroenterological surgeries. 24 While the risks of surgery associated with morbid obesity are numerous, antiobesity bias plays a significant role in clinical decision making. A 2015 review article on the subject concludes, “Many healthcare providers hold strong negative attitudes and stereotypes about people with obesity. There is considerable evidence that such attitudes influence person-perceptions, judgment, interpersonal behavior and decision-making.” 10 Our finding that obesity does not predict unwillingness to operate on individuals with a lower severity score indicates that antiobesity bias may not be a strong factor in the surgical decision making process at our institution.
Last, gender bias is one of the most broadly researched forms of bias. 25,26 In choosing the next generation of surgeons, much literature has described biases in the residency selection process. Gender bias has been demonstrated across multiple surgical subspecialty training programs. 8,9 These biases with regard to residency selection may ultimately affect levels of IB in practicing surgeons, which may affect patient care. Moreover, demographic information of surgeons themselves has been shown to be linked to the decision of whether or not to operate, with factors such age and self-confidence levels biasing surgical decision making in similar patient scenarios. 17 All of these potential areas of IB must be considered carefully in order to avoid their involvement in the surgical decision-making process.
Strengths and Limitations
In attempting to characterize IB in demographic areas which have traditionally been less analyzed in the literature, our study has several strengths. First, the large sample size of this single-surgeon cohort lends credence to the trends observed therein. Additionally, to our knowledge, this specific constellation of factors which have been previously shown to be areas associated with IB have never been studied in the spine literature. Furthermore, a large sample size from a single surgeon allows for removal of surgeon-specific confounders, as discussed by Macdermid et al 17 Other series attempting to analyze IB in spine surgery may have to rely on data from multiple surgeons to obtain an adequate sample size. We believe or methodology to be reproducible for other surgeons who wish to self-analyze their own potential IB, not as any form of punitive measure, but as a chance to improve patient care and become aware of areas of bias in their own practice.
This study does have multiple limitations. First, the retrospective nature of this work lends inherent limitations to the study. Additionally, while our database includes a variety of factors which have been demonstrated to be associated with IB, there are several additional factors which have also been associated with IB. Race, workers compensation status, and insurance status are all variables that may factor into the surgical decision-making process. While our decision to analyze only the patients from a single surgeon over a several year periods was based in prior literature of surgeon-specific confounders, another potential limitation is the reproducibility of our results for other spine surgeons at other institutions. To remedy this, we hope that additional analyses will be undertaken in multiple settings, at multiple institutions. This constellation of data would help to explain patterns of IB seen across the country, as there may be regional influences effecting surgical decision making.
Additional Research
Additional research in the area of focus of this study could assess for bias in other variables such as race and insurance payer status. Race and ethnicity have been shown to affect whether or not a surgeon decides to pursue operative management for a patient. 1 A 2018 article published in JAMA demonstrated improved access to surgical care in states that had elected to pursue Medicaid expansion. 27 This study indicates that insurance payer status strongly influences surgical decision making as well as access to care.
Conclusion
In conclusion, our study demonstrates absence of association between commonly studied areas of IB and the decision to operate on a patient with milder symptomology at initial presentation of CSM. These results indicate that the surgical decision making of the spine surgeon whose patients were analyzed in this study is not heavily affected by the factors evaluated for in this work. Instead, the degree of severity of disease appears to be the strongest factor determining whether or not surgical intervention is undertaken. To our knowledge, this study represents the first single-surgeon analysis of IB related to the specific factors that had been undertaken in the spine literature. We hope surgeons will apply our methodology to their own retrospective data, in an effort to better understand the influences that may be affecting their own surgical decision making.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.