
Abstract
Study Design:
Longitudinal cohort study.
Objectives:
To investigate whether a cutoff point in leg pain intensity measured preoperatively or at early follow-up could identify patients at risk of poor outcomes in terms of disability at 1-year and 2-year follow-up after first-time lumbar discectomy, and to identify the characteristics associated with early postoperative leg pain intensity.
Methods:
From 2010 to 2013, 556 patients underwent lumbar discectomy. Leg pain intensity was measured preoperatively and at early postoperative follow-up and dichotomized according to an established cutoff point on a 0 to 100 visual analogue scale (mild <30, moderate/severe ≥30). The outcome measurement was Oswestry Disability Index (ODI). Generalized estimating equations modelling established the association between leg pain intensity and ODI. Characteristics associated with early postoperative leg pain intensity were identified using common hypothesis tests.
Results:
Moderate/severe leg pain intensity at early follow-up showed a statistically significant association with higher ODI at 1-year and 2-year follow-up compared to mild leg pain intensity (median [interquartile range]: 24 [26] and 26 [26] versus 12 [18] and 10 [20], respectively). Patients reporting moderate/severe leg pain intensity were more often smokers, were more prone to receive social benefits, and were more prone to have chronic back pain. The preoperative measurement of leg pain intensity showed inferior associations.
Conclusion:
The proposed cutoff point in leg pain intensity at early follow-up can identify patients at risk of disability at both 1-year and 2-year follow-up after first-time discectomy. Future research should be undertaken to investigate whether patients with moderate/severe leg pain intensity at early postoperative follow-up could benefit from additional or more intensive postoperative interventions.
Keywords
Introduction
In a clinical low back pain population, the prevalence of sciatica is 11% to −12% 1,2 and reaches a peak during working age. 2,3 Lumbar disc herniation (LDH) is the causing pathology in an estimated 90% of cases. 4 Although nonsurgical treatment for LDH can relieve pain and improve physical function, 5 approximately 14% to 30% of patients with LDH undergo discectomy due to severe or persistent symptoms. 6,7 Of these, 8% to 21% will experience poor outcomes in terms of continued pain and disability within 1 to 5 years after discectomy. 5,8
Early identification of patients at risk of poor outcomes after discectomy is vital as prolonged symptoms can result in severe consequences for the individual and substantial costs for the society. 9,10 In spine surgery, these costs are particularly associated with postoperative treatment and productivity loss due to sick leave or functional limitations. 11
Being able to identify patients at risk of poor outcomes in terms of disability could help improve the accuracy of informed prognosis and facilitate the planning of postoperative interventions such as medical and/or vocational rehabilitation.
Studies have shown that higher leg pain intensity both preoperatively and within 2 months after lumbar discectomy is associated with disability and the ability to work at later follow-ups. 8,12,13 Although this information is vital to the clinician, it can be hard to implement in daily practice. The identification of cutoff points at which patients are at risk would give the surgeon a manageable tool. Within the area of anesthesiology, such cutoff points in pain intensity have been established and have proven to be useful in guiding individual subacute postoperative pain treatment. 14,15 To our knowledge, however, no study has examined whether a cutoff point in leg pain intensity measured preoperatively and at an early follow-up could identify patients at risk of poor outcomes after lumbar discectomy.
The objectives of this study were the following:
To investigate whether a previously established cutoff point in leg pain intensity preoperatively or at early follow-up could identify patients at risk of poor outcomes in terms of disability at 1-year and 2-year follow-up after lumbar discectomy.
To identify the preoperative and perioperative characteristics associated with early postoperative leg pain intensity.
Methods
Design
A longitudinal cohort single-center study was conducted based on prospectively collected registry data from DaneSpine, 16 Statistics Denmark, 17 and clinical data from the patients’ electronic medical records. The study adheres to STROBE guidelines.
Setting and Participants
The study population comprised a consecutive series of patients who underwent single-level open discectomy or micro-endoscopic discectomy and were enrolled in the database DaneSpine. All patients were referred to the surgical department of a public hospital from primary or secondary care after unsuccessful nonsurgical treatment or the presence of a clear indication for surgery. All patients had persistent or severe symptoms compatible with LDH and received a magnetic resonance imaging scan, or alternatively a computed tomography scan, verifying the diagnosis. Patients were 18 years or older and had an American Society of Anesthesiologists (ASA) classification score <3. 18 Twelve different surgeons conducted the discectomies during the inclusion period between September 1, 2010, and December 31, 2013.
Excluded from the study were patients who had (1) previous spine surgery at any level, (2) other serious spinal pathology at the time of surgery, (3) a missing functional disability score preoperatively or at 2-year follow-up, or (4) a missing preoperative leg pain intensity score. All settings related to the study remained unchanged throughout the study period.
Variables and Data Sources
On the day of admission, patients completed a baseline questionnaire that included questions on age, gender, self-reported leg and back pain intensity measured on a visual analogue scale (VAS-LP and VAS-BP, respectively), 19 functional disability measured by Oswestry Disability Index (ODI), 20,21 and health-related quality of life measured by both EuroQoL (EQ-5D) 22 and the Short Form Health Survey version 1 (SF-36). 23 ODI and VAS-LP scores were also collected at 1-year and 2-year follow-up via questionnaires. In addition, VAS-LP score was collected at “early follow-up,” which was between 4 and 6 weeks postoperatively (median 34 days). Assigned personnel entered the data into the DaneSpine database using a standardized codebook. Data on deaths, emigrations, and socioeconomic classification within the study period was retrieved from Statistics Denmark. 17,24
The DaneSpine database is maintained by the Danish Society of Spine Surgeons to monitor, evaluate, and potentially improve aspects of the surgical treatment beneficial to patient outcomes through prospective data collection. The hospital department in this study enrolled 98% to 99% of the patients who were first-time operated for lumbar radiculopathy. (Source: Calculations based on data from the Danish Society of Spine Surgeons and the National Patient Register. 25 )
Statistics Denmark is the central authority for collecting, compiling, and publishing statistics on the Danish society. All persons living in Denmark are registered in the Danish Civil Registration System and are assigned an individual personal identification number at birth or on immigration, making possible a unique and accurate linkage between all national registers and datasets. 26
Ethics and Data Control
This study was approved by the Danish Health Safety Authority (#3-3013-1174/1) and the Danish Data Protection Agency (#14/26 345). According to Danish law, ethical approval from the Regional Scientific Ethics Committee for Southern Denmark was not required for this type of study. 27 On completing the DaneSpine questionnaires, patients gave written consent for the use of their data in research. All patient data is strictly confidential and is stored according to the Danish Open Administration Act, the Danish Act on Processing of Personal Data, and the Health Act. Institutional review board approval was not required.
Data Management and Statistics
Leg pain intensity at both time points (VAS range 0-100) was categorized according to Collins et al 28 : mild (VAS < 30), moderate (VAS ≥30 and <70), and severe (VAS ≥ 70), and then reduced to mild versus moderate/severe to enhance clinical usefulness. The associations between both preoperative and early postoperative dichotomized leg pain intensity and the ODI were examined using crude and adjusted generalized estimating equations modelling. Comparing the preoperative and perioperative characteristics of the study population and the patients excluded due to missing ODI score at 2-year follow-up (nonresponders) identified the covariates for which the models were adjusted. The appropriateness of the models was assessed using QQ-plots and the internal validity tested using bootstrapping.
Stratified by the dichotomized leg pain intensity as assessed preoperatively and at early postoperatively follow-up, differences in medians of ODI at 1-year and at 2-year follow-up were evaluated using Mann-Whitney test. Preoperative and perioperative characteristics associated with moderate/severe leg pain intensity at early follow-up was identified using Student’s t test, χ2 test, and Mann-Whitney test. Prevalence proportion ratios (PR) were calculated for variables found significantly associated with moderate/severe leg pain to ease the clinical interpretation.
Analyses were performed using Stata 15.1 (StataCorp, College Station, TX) with an α level of 0.05.
Results
Participants and Descriptive Data
In total, 835 patients were eligible for the study according to DaneSpine (Figure 1). However, 252 patients were excluded due to missing ODI at 2-year follow-up, and 27 were excluded due to other reasons, leaving 556 patients in the final study population. Baseline characteristics of the final study population and the nonresponders are shown in Table 1. Compared with the study population, a significant portion of the nonresponders were younger, were smokers, were more prone to receive social benefits, and to a lesser degree, they were employed and had a longer duration of leg pain and back pain at baseline. In addition, nonresponders had a statistically significant but not clinically relevant higher level of back pain intensity and a lower health-related quality of life measured by EQ-5D and SF-36. Moderate or severe leg pain intensity was reported by 88% of the patients at baseline and 28% at early follow-up.
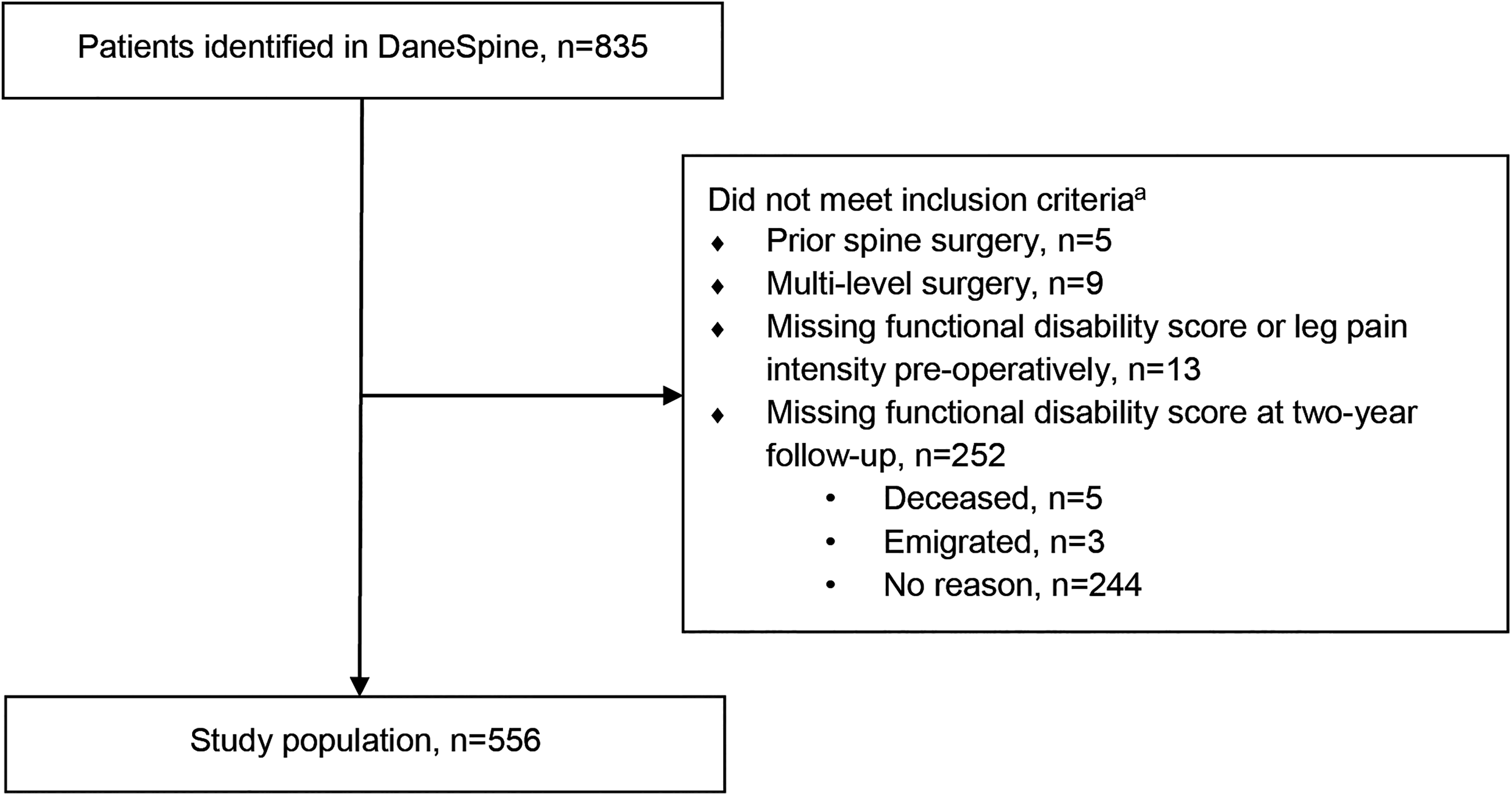
Flowchart of the study population selection process.
Baseline Characteristics of the Study Population and Non-Responders at 2-Year Follow-Up After First-Time, Single-Level, Lumbar Discectomy.a
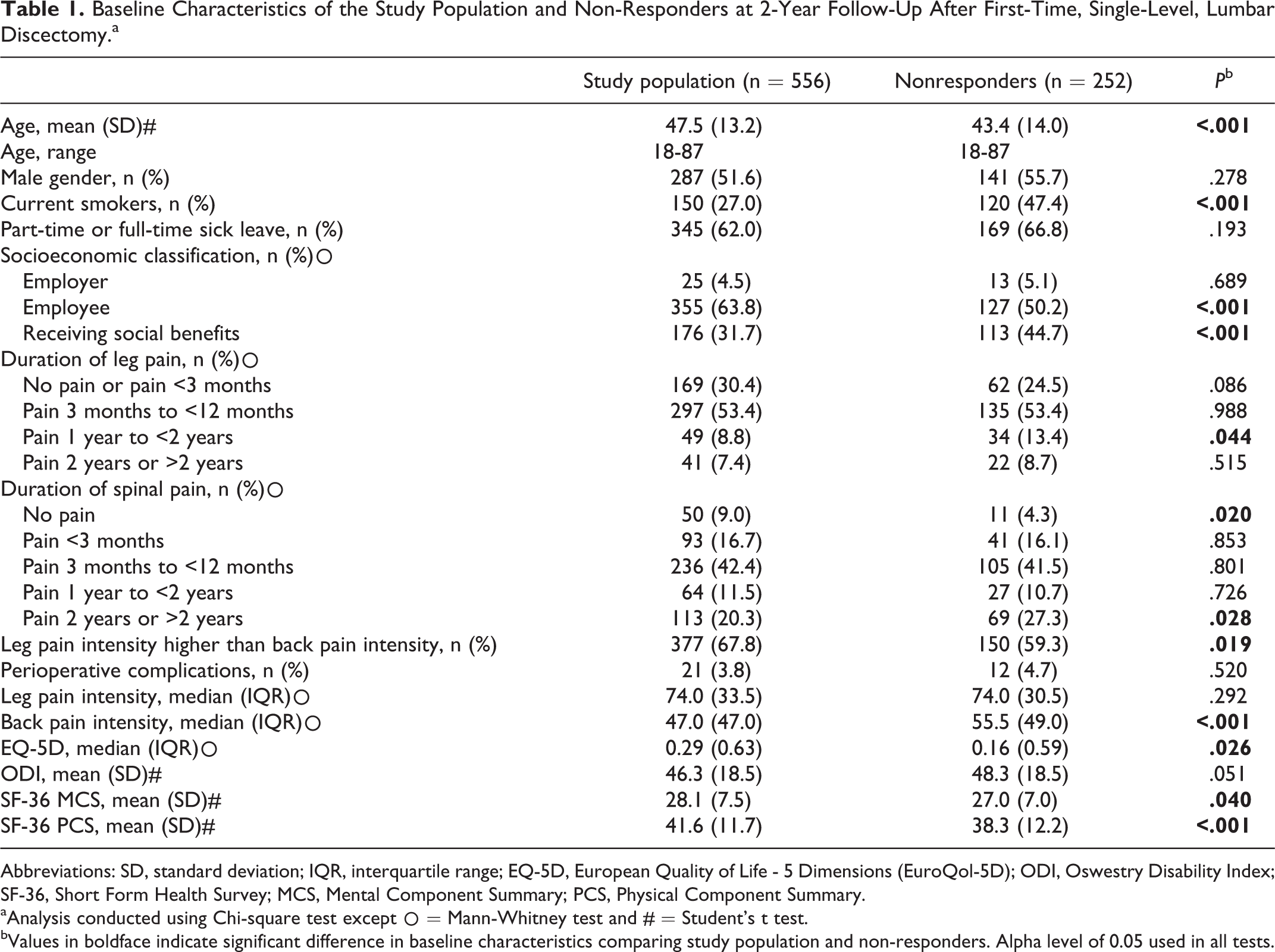
Abbreviations: SD, standard deviation; IQR, interquartile range; EQ-5D, European Quality of Life - 5 Dimensions (EuroQol-5D); ODI, Oswestry Disability Index; SF-36, Short Form Health Survey; MCS, Mental Component Summary; PCS, Physical Component Summary.
aAnalysis conducted using Chi-square test except ○ = Mann-Whitney test and # = Student’s t test.
bValues in boldface indicate significant difference in baseline characteristics comparing study population and non-responders. Alpha level of 0.05 used in all tests.
Outcome Data
Data completeness of the ODI was between 92% and 100% preoperatively and at follow-ups. The completeness of the variable leg pain intensity was 100% preoperatively and 86% at early follow-up.
Main Results
The Association Between Dichotomized Leg Pain Intensity and Disability at 1-Year and 2-Year Follow-up
In a crude analysis, the presence of moderate/severe leg pain intensity was associated with increased disability at 1-year and 2-year follow-up regardless of time of measurement (Table 2). Only the association between preoperative leg pain intensity and ODI at 2-year follow-up failed to reach statistical significance. The coefficients for early follow-up leg pain intensity were higher than for the preoperative leg pain intensity, and the QQ-plots were correspondingly in favor of the models based on the leg pain intensity measured at early follow-up (data not shown). In the adjusted analyses, only early follow-up leg pain intensity showed a statistically significant association with the ODI score at follow-ups. Patients who reported moderate/severe leg pain intensity at early follow-up had statistically significant higher and clinically relevant ODI scores at 1-year and 2-year follow-up compared with those who reported mild leg pain intensity (Table 3). When nonresponders were included in the analyses, preoperative dichotomized leg pain intensity showed a statistically significant association with postoperative disability at 1-year and 2-year follow-up although it was much weaker compared with the dichotomized leg pain intensity measured at early follow-up (data not shown).
Association Between Dichotomized Preoperative and Early Postoperative Leg Pain Intensity and Disability at 1-Year and 2-Year Follow-Up After First-Time, Single-Level, Lumbar Discectomy.a
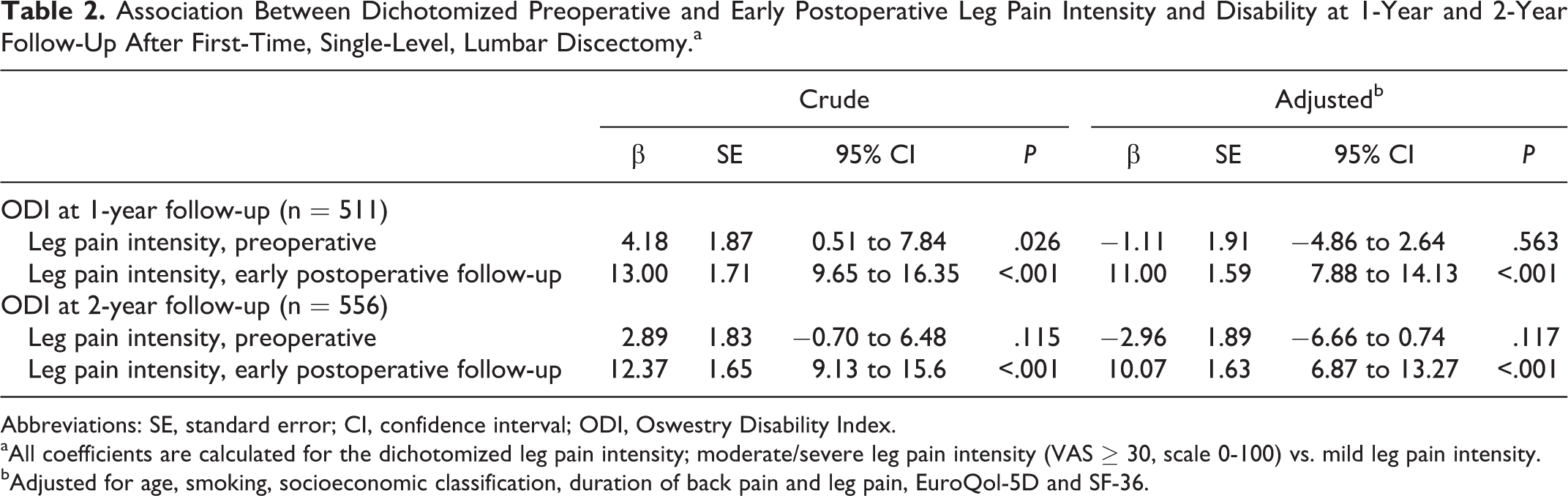
Abbreviations: SE, standard error; CI, confidence interval; ODI, Oswestry Disability Index.
aAll coefficients are calculated for the dichotomized leg pain intensity; moderate/severe leg pain intensity (VAS ≥ 30, scale 0-100) vs. mild leg pain intensity.
bAdjusted for age, smoking, socioeconomic classification, duration of back pain and leg pain, EuroQol-5D and SF-36.
Disability (ODI) at all Time-Points, Stratified by Leg Pain Intensity as Measured Preoperatively or at Early Follow-Up.
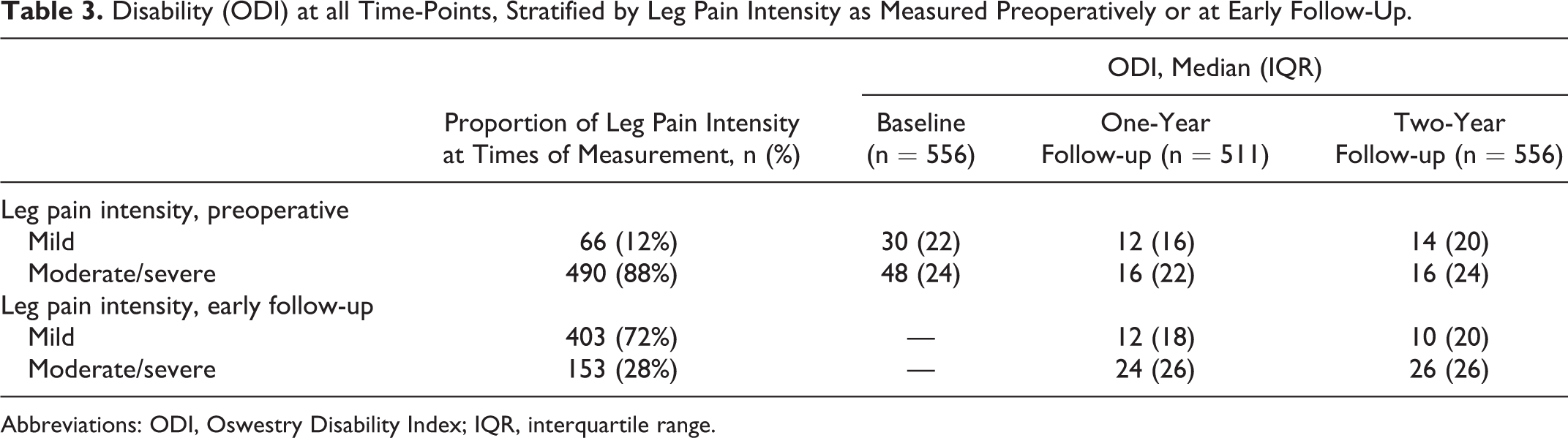
Abbreviations: ODI, Oswestry Disability Index; IQR, interquartile range.
The Association Between Leg Pain Intensity at Early Follow-up and Preoperative and Perioperative Characteristics
Patients reporting moderate/severe leg pain intensity at early follow-up were more often smokers (PR 1.48; 95% confidence interval [CI] 1.12-1.94). That is, the prevalence of reporting moderate/severe leg pain intensity at early follow-up among smokers was 1.48 times higher relative to the group of nonsmokers. Also, patients reporting moderate/severe leg pain intensity at early follow-up were more prone to receive social benefits (PR 1.82; 95% CI 1.40-2.37) and more prone to long-term duration of back pain compared to patients with mild leg pain intensity (PR 1.48; 95% CI 1.11-1.98; Table 4). Furthermore, they had higher baseline leg pain intensity and lower SF-36 PCS than patients with mild leg pain intensity. However, as the differences were only 2 (0-100 scale) and 3.9 (0-100 scale), respectively, the clinical relevance was questionable.
Baseline Characteristics Associated with Leg Pain Intensity at Early Follow-Up (4-6 Weeks) After First-Time, Single-Level, Lumbar Discectomy.a
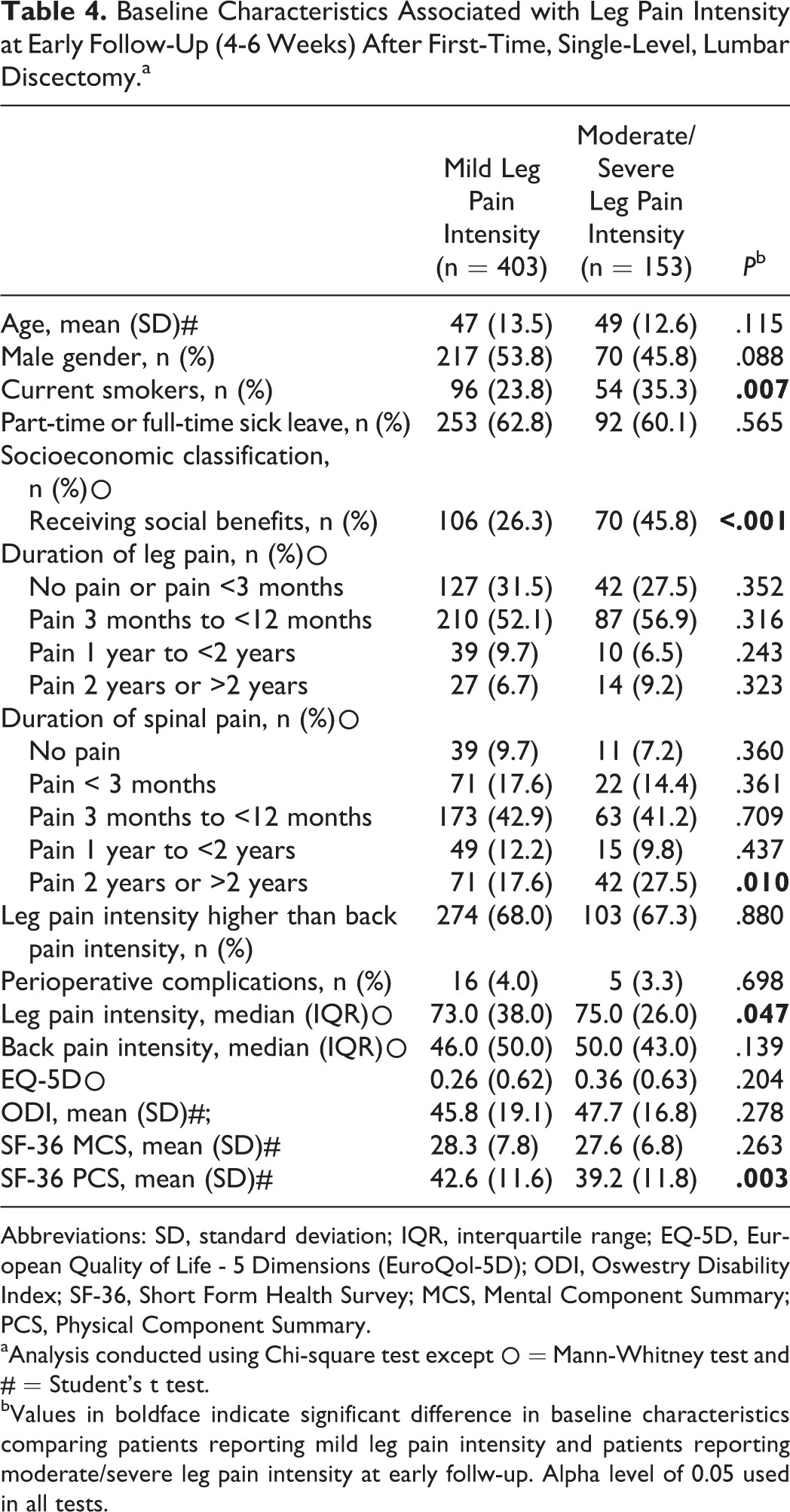
Abbreviations: SD, standard deviation; IQR, interquartile range; EQ-5D, European Quality of Life - 5 Dimensions (EuroQol-5D); ODI, Oswestry Disability Index; SF-36, Short Form Health Survey; MCS, Mental Component Summary; PCS, Physical Component Summary.
aAnalysis conducted using Chi-square test except ○ = Mann-Whitney test and # = Student’s t test.
bValues in boldface indicate significant difference in baseline characteristics comparing patients reporting mild leg pain intensity and patients reporting moderate/severe leg pain intensity at early follw-up. Alpha level of 0.05 used in all tests.
Discussion
Key Results
The Association Between Leg Pain Intensity and Disability at 1-Year and 2-Year Follow-up
The dichotomized leg pain intensity (mild and moderate/severe) measured at early follow-up showed a statistically significant association with disability in both the crude and adjusted analyses at 1-year and 2-year follow-up after first-time, single-level lumbar discectomy. The lack of statistical significance found between the preoperative leg pain intensity and disability might be explained by the limited number of patients with mild leg pain intensity preoperatively (n = 66), leading to overfitting in the adjusted analysis. Moreover, as nearly all patients had moderate/severe leg pain intensity (88%) preoperatively, the proposed cutoff point was not clinically useful at that time point. A categorization of the preoperative leg pain intensity as suggested in the definition (mild 0-29, moderate 30-69, severe 70-100) 28 would likely enhance the associations between preoperative leg pain intensity and disability at follow-ups. However, in clinical decision making, the distinction between moderate and severe leg pain intensity would not likely affect the treatment options offered, nor would it be gainful to the clinic. The finding of early postoperative leg pain intensity being more strongly associated with the outcome compared to the preoperative leg pain intensity is in line with previous studies using continuous leg pain intensity scores. 8,12 In this study, early follow-up was defined as 4 to 6 weeks after surgery, but it is possible that patients at risk of a poor outcomes could be identified even earlier. In a study by den Boer et al, 29 high levels of pain intensity measured only 3 days postoperatively were predictive of reduced return to work at 6-month follow-up.
Leg pain intensity is not the only variable associated with postoperative functional limitation. Other studies have found that psychological factors including cognitive-behavioral factors, 13,30 sociodemographic factors, and work-related factors 31,32 are associated with postoperative functional limitation. However, compared to these factors, leg pain intensity, especially when dichotomized, is easily assessable and more manageable for the surgeon or personnel within the health care system.
Characteristics Associated With Early Follow-up Leg Pain Intensity
Dichotomization of the leg pain intensity at early follow-up provides a clinically useful guide to customizing postoperative management as patients with moderate/severe leg pain intensity at early follow-up are at risk of increased disability compared to patients with lower leg pain intensity. This accounted for 28% of the population and is therefore a fairly large proportion of patients receiving surgery in this study. The median ODI at 1-year and 2-year follow-up identified by the cutoff point was above 20, which is moderate by definition. 21 A Japanese study found that an ODI ≥22.07 identified individuals with disability due to low back pain in the general population aged 20 to 69 years (n = 1200). 33 Identified by the proposed cutoff point, we found that 31% of the study population had median ODI scores of 24 at 1-year follow-up and 36% had median ODI scores of 26 at 2-year follow-up. The clinical implications following an ODI > 20 as mentioned above justifies the use of the proposed cutoff point.
This study identified some modifiable sociodemographic characteristics that were associated with early follow-up leg pain intensity (Table 4). The findings could inform future studies investigating the impact of characteristics on the outcome in large-scale, multifactorial studies.
Strengths and Limitations
A strength of this study is the use of secondary data from a suitable database, which minimizes the potential bias associated with retrospective studies as all data is prospectively collected. Moreover, the model adjustment using covariates identified in the nonresponder analysis limits the risk of selection bias when using complete cases only.
The nonresponders were more prone to receive social benefits and to a lesser degree were employed and younger, and they were more often smokers at baseline compared to the responders. This pattern is previously demonstrated although with slight variations of characteristics. 34,35 Receiving social benefits and being a smoker were also associated with the risk of moderate/severe leg pain intensity at early follow-up and, consequently, the associations were likely underestimated. Among the nonresponders were also a higher proportion of patients with dominating and chronic back pain, which has previously been shown to be associated with increased ODI after surgery. 36 This likely influences the associations found in this study.
Generalizability and Perspectives
Given that this was a single-center study, generalizability is limited and the findings need to be replicated in future studies of similar and extended populations. The hospital department from which the data were collected only operates patients with an ASA classification score <3, which influences the generalizability of the results. Patients with an ASA classification score ≥3 would likely demonstrate different outcomes, making adjustment for comorbidity necessary.
As 28% of the population reached the cutoff point, we suggest that further research investigate whether patients with moderate or severe leg pain intensity at early postoperative follow-up would benefit from additional or more intensive postoperative interventions. Future research should investigate the impact of preoperative interventions targeting modifiable characteristics as some of these are associated with pain intensity at early follow-up.
Conclusion
A cutoff point in leg pain intensity (>29 on a 0-100 scale) measured at early postoperative follow-up (4-6 weeks) can identify patients at risk of clinically significant disability at 1-year and 2-year follow-up after first-time, single-level lumbar discectomy.
In contrast, the preoperative cutoff point failed to identify patients at risk due to primarily methodological reasons and is therefore not useful to preoperative decision making.
Key Points
A cutoff point in leg pain intensity (mild 0-29, or moderate/severe 30-100), measured at early follow-up after first-time, single-level, lumbar discectomy was associated with level of disability at 1-year and 2-year follow-up.
Out of 556 patients, 28% reported moderate/severe leg pain intensity at early follow-up after first-time, single-level, lumbar discectomy.
Patients with moderate/severe leg pain intensity at early follow-up were statistically significant more often smokers (PR 1.48; 95% CI 1.12-1.94), receiving social benefits (PR 1.82; 95% CI 1.40-2.37), and prone to long-term duration of back pain (PR 1.48; 95% CI 1.11-1.98).
Supplemental Material
Supplemental Material, STROBE_udfyldt - The Association Between Early Postoperative Leg Pain Intensity and Disability at 1-Year and 2-Year Follow-Up After First-Time Lumbar Discectomy
Supplemental Material, STROBE_udfyldt for The Association Between Early Postoperative Leg Pain Intensity and Disability at 1-Year and 2-Year Follow-Up After First-Time Lumbar Discectomy by Dorthe Schoeler Ziegler, Rikke Krüger Jensen, Lisbeth Storm, Leah Carreon and Mikkel Oesterheden Andersen in Global Spine Journal
Footnotes
Acknowledgments
The authors are grateful to Karen Hoejmark Hansen, Spine Surgery and Research, Spine Center of Southern Denmark—part of Lillebaelt Hospital, for her help with data extraction from DaneSpine.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the IMK Foundation (2015/DSZ); the Danish Foundation for Chiropractic Research and Postgraduate Education (14/3074), and the Region of Southern Denmark PhD Fund (16/13 504).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.