
Abstract
Study Design:
Retrospective review.
Objectives:
(1) Identify the 90-day rate of readmission following revision lumbar fusion, (2) identify independent risk factors associated with increased rates of readmission within 90 days, (3) and identify the hospital costs associated with revision lumbar fusion and subsequent readmission within 90 days.
Methods:
Utilizing 2014 data from the Nationwide Readmissions Database, patients undergoing elective revision lumbar fusion were identified. With this sample, multivariate logistic regression was utilized to identify independent predictors of readmission within 90 days. An analysis of total hospital costs was also conducted.
Results:
In 2014, an estimated 14 378 patients underwent elective revision lumbar fusion. The readmission rate at 90 days was 3.1% (n = 446). Diabetes with chronic complications was the only comorbidity found to carry significantly increased odds of readmission. Surgical complications such as deep venous thrombosis, surgical wound disruption, hematoma, and pneumonia (experienced during the index admission) were also independent predictors of readmission. Anterior approaches were associated with increased odds of readmission. The most common related diagnoses on readmission were hardware issues, postoperative infection, and disc herniation. Readmissions were associated with an average of $96 152 in increased hospital costs per patient compared with those not readmitted.
Conclusion:
Relevant patient comorbidities and surgical complications were associated with increased readmission within 90 days. Readmission within 90 days was associated with significant increases in hospital costs.
Keywords
Introduction
Lumbar spinal fusion is a common spinal procedure that may require subsequent revision in a number of cases. In the United States, the volume of elective lumbar fusions performed increased 62.3% from 2004 to 2015, according to a review of National Inpatient Sample data. Similarly, the rate of lumbar surgery per 100 000 US adults increased 32.1% within the same timeframe (60.4 per 100 000 to 79.8 per 100 000). The greatest increase in volume (138.7%) and rates (73.2%) of lumbar fusions were in patients age 65 and older. 1 Given recent estimates that the Medicare population is expected to swell from 39.7 million to 67.0 million individuals from 2010 to 2030, it stands to reason that the amount of lumbar fusions performed in the United States will only continue to increase. 2 With this precipitous increase in the amount of lumbar fusions, it should be expected that there will also be an increase in the amount of lumbar fusion revisions performed. Previous studies have found reported rates of revision lumbar fusion from 9.2% to 12.8%, and total reoperation rates of 20.1%. 3 -5
Compared with primary lumbar fusion surgery, revision lumbar fusion has been associated with increased complications and morbidity. 6 This can lead to increased health care visits, inferior outcomes, and increased total healthcare costs. A review of National Inpatient Sample (NIS) data from 1998 to 2006 found an increase in surgical-related complications in revision surgery compared with primary surgery. 6,7 Additional studies have also borne out that revision lumbar surgery carries increased risk of surgical-related complications such as surgical site infections in comparison to primary procedures. 8,9 The increased risks of revision surgery come at a high cost to patients and health systems alike. A 2012 study looking at a cohort of 150 patients who underwent revision lumbar fusion found that the average direct patient cost associated with the procedure was $32 915 in the first 2 years after surgery. 10
The cost of health care in the United States grew at an inflation-adjusted 4.0% per year from 1995 to 2005, a rate that outpaced the growth of the total US economy over the same timeframe (2.4% per year). 11 In order to combat these increases in health care spending, the Centers for Medicare and Medicaid Services began testing alternatives to the traditional fee-for-service models. One such alternative is the Bundled Payments for Care Improvement (BPCI) initiative, which seeks to align stakeholders, improve health care outcomes, and decrease health care expenditures. 12 Similar to the BPCI model 2, the Comprehensive Care for Joint Replacement (CJR) model has seen rapid integration into many orthopedic procedures including total joint arthroplasty, covering reimbursement for the initial procedure, and any subsequent costs associated within the first 90 days following the initial procedure. 13 Outcomes after implementation of the BPCI and CJR have been favorable—noting decreased health care costs and rates of readmission. 14 -16 Given the success of BPCI in common orthopedic procedures, it is likely that BPCI models will become more common in the reimbursement for other procedures such as revision lumbar fusion. It is therefore important for physicians to understand the risk factors and costs associated with 90-day readmissions in patients undergoing revision lumbar fusion.
There is a paucity of literature that examines the rates, factors, and costs associated with 90-day readmissions following elective revision lumbar fusion. To our knowledge this study is the first to examine 90-day readmissions characteristics in this population on a national level. In doing this, we hope to enable physicians to recognize patients who are at increased risk of readmission so that perioperative risk-reduction strategies may be implemented to increase positive outcomes and minimize any associated health care costs in the future. The objectives of this study are to (1) determine the total incidence and rate of readmission within 90 days after elective revision of lumbar fusion; (2) identify risk factors associated with readmission; and (3) evaluate the cost associated with these readmissions within a 90-day window of care.
Materials and Methods
Study Population Selection
A retrospective cohort study was conducted using 2014 data from the Nationwide Readmissions Database (NRD). This database is an aggregate of inpatient databases from 27 states and is estimated to represent 56.8% of all hospitalizations in the United States. The data presented in this study is based upon Healthcare Utilization Project (HCUP) sample weights, which represent the approximately 36 million annual hospital discharges in the United States. 17 Institutional review board exemption was obtained for this study.
Inclusion and Exclusion Criteria
All patients within the NRD undergoing revision lumbar fusion were identified using International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) procedure codes. Patients who were identified as younger than 18 years old, death during initial admission, or nonelective admission were excluded from this study. The NRD allows the tracking of patients and their subsequent readmissions within the same year and the same state as their index admission. Therefore, patients who were readmitted in a different state or different year than their index admission would not be recorded as a readmission. To reduce any confounding that this may cause, patients whose index admission was during the final quarter of 2014 were excluded from the study to allow for follow-up of 90 days from the index procedure. The remaining included population was then divided into 2 cohorts based on whether or not they were readmitted to the hospital within 90 days of their index admission.
Patient and Hospital Characteristics
Patient demographic characteristics, payer status, and diagnoses were retrieved from the NRD. The teaching status and size of each hospital where the patient was admitted were also gathered from the NRD. Patient comorbidities were obtained using the HCUP Comorbidity software, which uses ICD-9 and DRG coding to classify patients. This software also calculates an Elixhauser Comorbidity Index for each patient.
Patient Outcomes and Readmissions Analysis
The NRD uses clinical classification software (CCS) to group together similar diagnoses and ICD-9 codes so that patient outcomes can be efficiently analyzed. The most common CCS codes were obtained to identify diagnoses on readmission. Metrics gathered included incidence and rate of 90-day readmission, procedures carried out during the readmission, and the primary diagnosis associated with the readmission.
Length of Stay and Hospital Costs
The length of stay and total cost to the hospital were also obtained. The NRD lists the total amount of money that the hospital charged for the hospital stay. This total was adjusted using a specific cost-to-charge ratio provided by the HCUP, and then the adjusted cost was corrected for inflation using data from the Consumer Price Index. 18,19 The cost of each individual readmission, the aggregate cost of the index admission, and any associated readmission were also calculated.
Statistical Analysis
All statistical analyses were performed using SPSS v24 (IBM Inc, Chicago, IL). The patient characteristics for both groups were analyzed with a Student’s t test and χ2 test. Continuous variables were analyzed with an independent Student’s t test, while categorical variables were analyzed with a χ2 test. Multivariate logistic regression analysis was then used to examine associations between demographic characteristics and comorbidities with 90-day readmissions. Only covariates that were found to be statistically significant in the initial univariate analysis were included in the multivariate analysis along with hospital characteristics. The associations were reported as adjusted odds ratios (ORs) with 95% confidence intervals (CIs). A P value <.05 was set as standard statistical significance.
Results
General Patient Data
An estimated 14 378 patients underwent elective revision lumbar fusion in 2014. There was no significant difference in the Elixhauser Comorbidity Index between patients who were readmitted and those who were not. A complete list of patient characteristics is available in Table 1.
General Sample Characteristics.
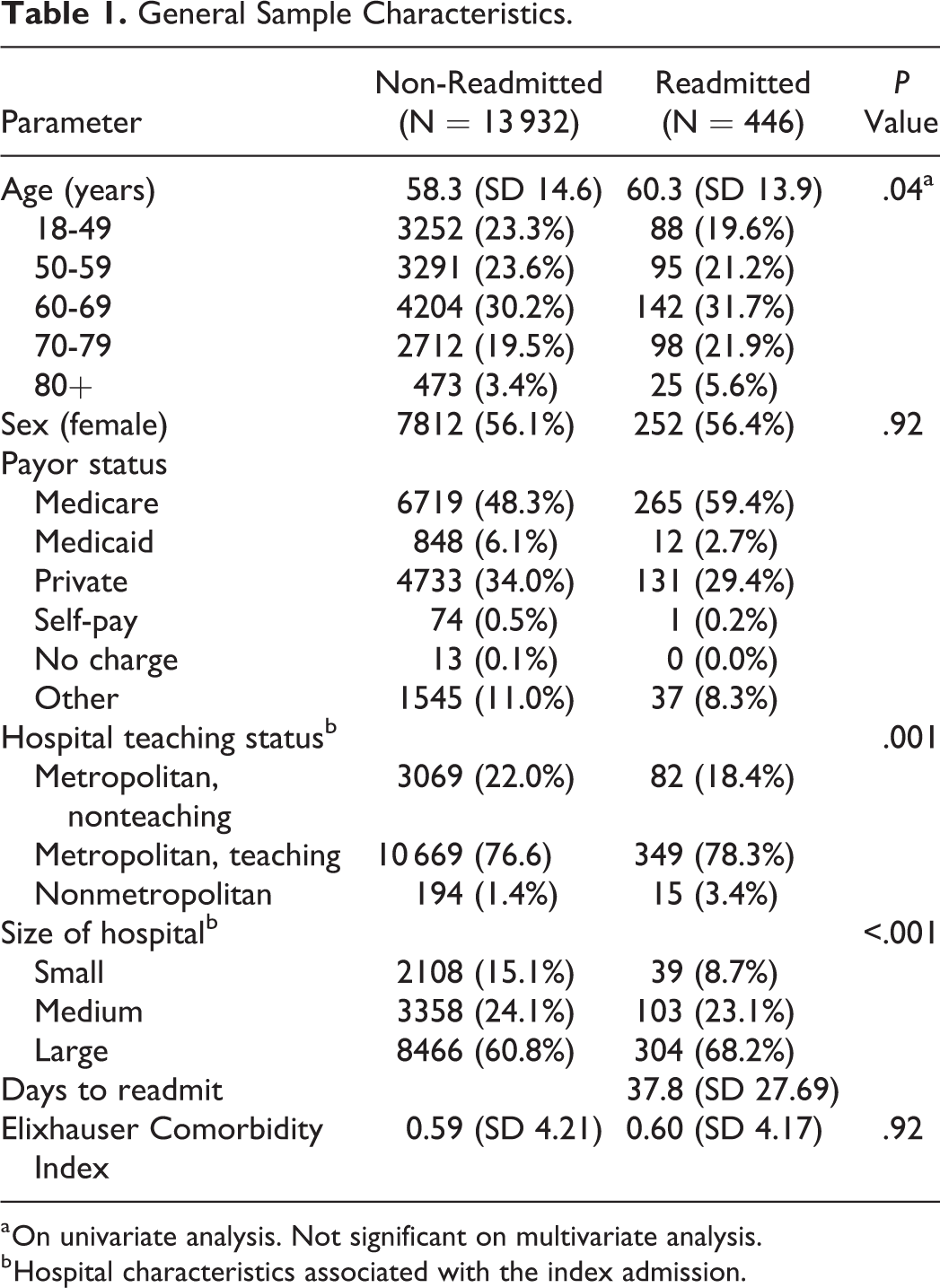
a On univariate analysis. Not significant on multivariate analysis.
b Hospital characteristics associated with the index admission.
Rates and Predictors of Readmission
The rate of readmission within 90 days of elective revision lumbar fusion was 3.1% (n = 446), with an average of 37.8 days to readmission. Of the 29 comorbidities that were assessed, only diabetes with chronic complications was found to be a significant predictor of readmission in both univariate and multivariate analyses (OR 1.57, CI 1.31-1.89; P < .001). Complications associated with increased odds of readmission included deep vein thrombosis (OR 1.78, CI 1.23-2.57; P = .002), disruption of surgical wound (OR 2.39, CI 1.08-5.30; P = .032), hematoma/seroma (OR 2.24, CI 1.20-4.18; P = .011), and pneumonia (OR 3.84, CI 2.21-6.67; P < .001). The complete univariate comorbidity analysis is available in Table 2.
HCUP NRD-Defined Comorbidities.
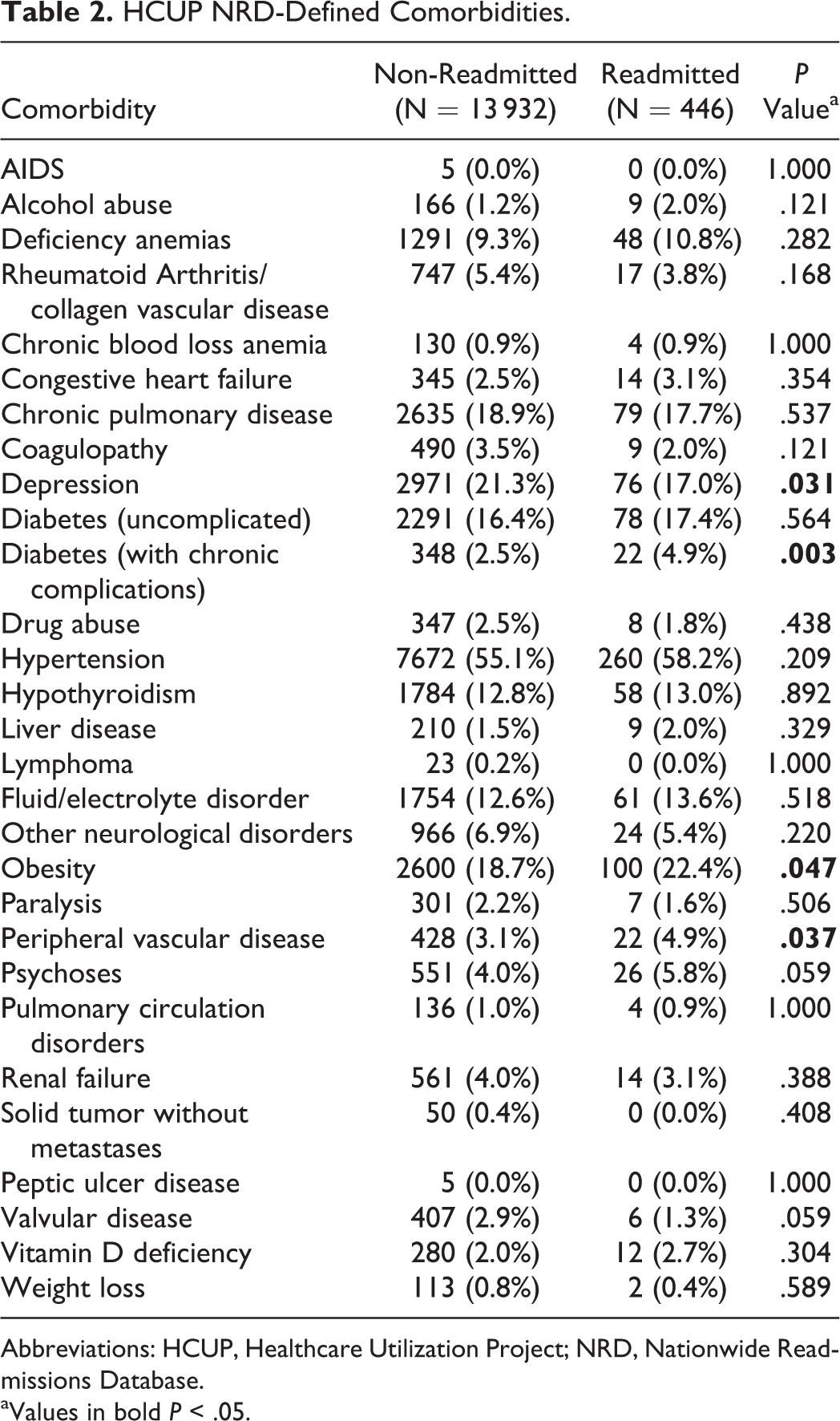
Abbreviations: HCUP, Healthcare Utilization Project; NRD, Nationwide Readmissions Database. aValues in bold P < .05.
When assessing strictly anterior and posterior surgical approaches, an anterior approach was associated with increased odds of readmission (OR 1.40, CI 1.12-1.75; P = .003). When assessing payer status as a risk factor for 90-day readmission, Medicare was used as the reference value. None of the other payer groups were associated with a significantly increased risk of readmission. Neither age nor patient disposition following index admission was associated with significantly increased odds of readmission within the 90-day window. The complete multivariate analysis is available in Table 3. The surgical approaches and procedure codes assessed are available in Table 4.
Ninety-Day Multivariate Analysis.
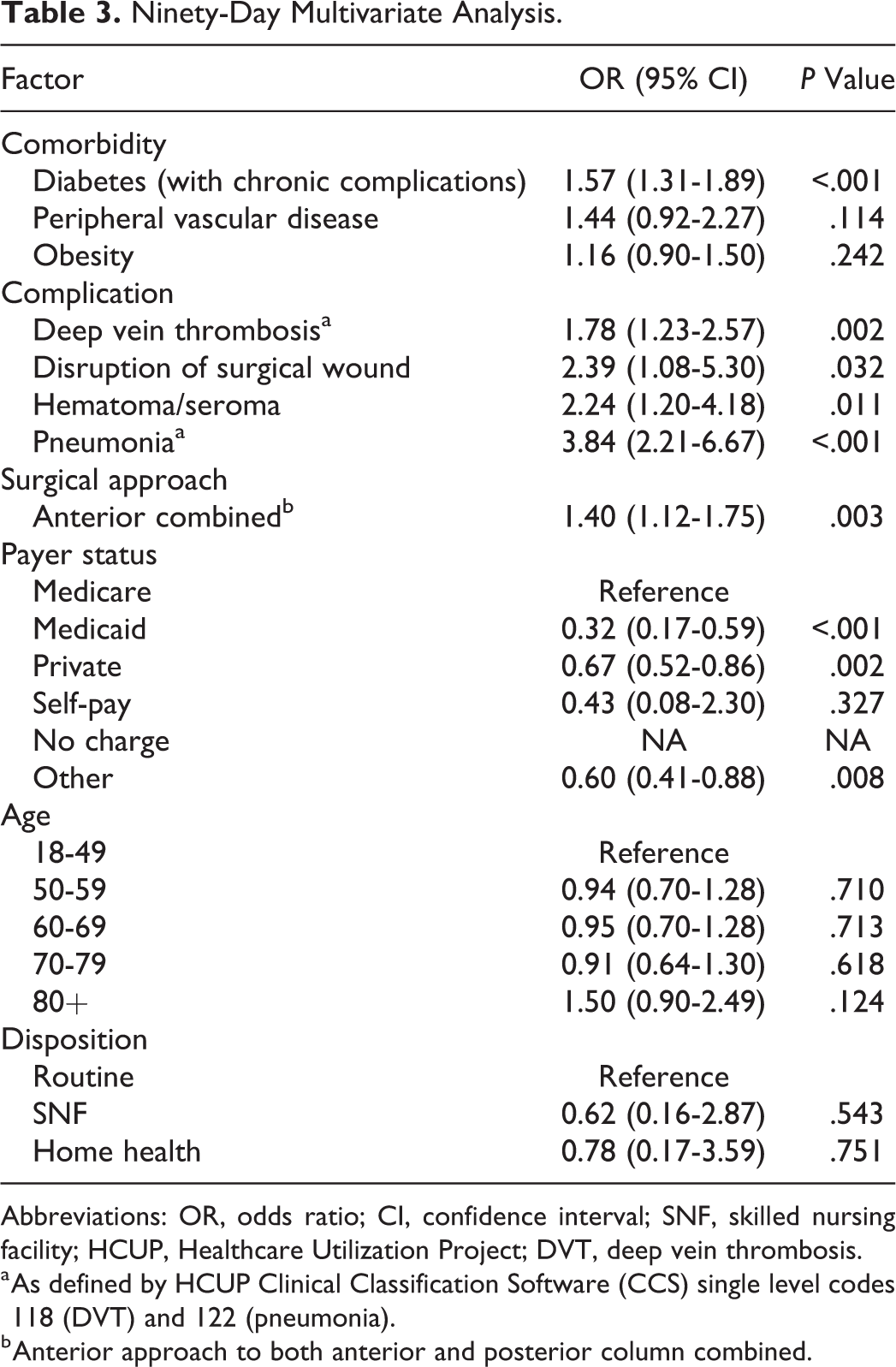
Abbreviations: OR, odds ratio; CI, confidence interval; SNF, skilled nursing facility; HCUP, Healthcare Utilization Project; DVT, deep vein thrombosis.
a As defined by HCUP Clinical Classification Software (CCS) single level codes 118 (DVT) and 122 (pneumonia).
b Anterior approach to both anterior and posterior column combined.
Surgical Approach/Procedure Codes.
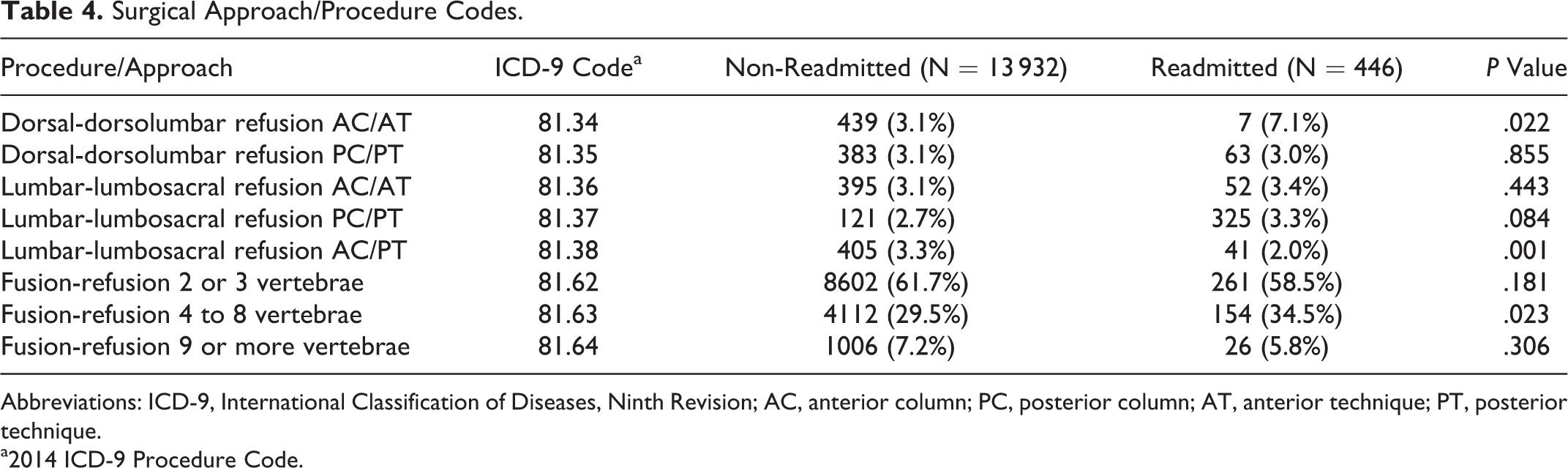
Abbreviations: ICD-9, International Classification of Diseases, Ninth Revision; AC, anterior column; PC, posterior column; AT, anterior technique; PT, posterior technique.
a2014 ICD-9 Procedure Code.
The diagnoses on readmission were assessed by identifying the ICD-9 diagnosis codes associated with each readmission. The 20 most common ICD-9 codes assigned on readmission can be found in Table 5. These diagnoses codes were further analyzed to determine diagnosis codes that were directly related to the index condition. The 3 most common of these diagnoses on readmission were (1) implant-related complications (n = 67, 15.0%), postoperative infection (n = 39, 8.74%), and disc herniation (n = 36, 8.07%).
Top 20 Overall Diagnoses on Readmission.
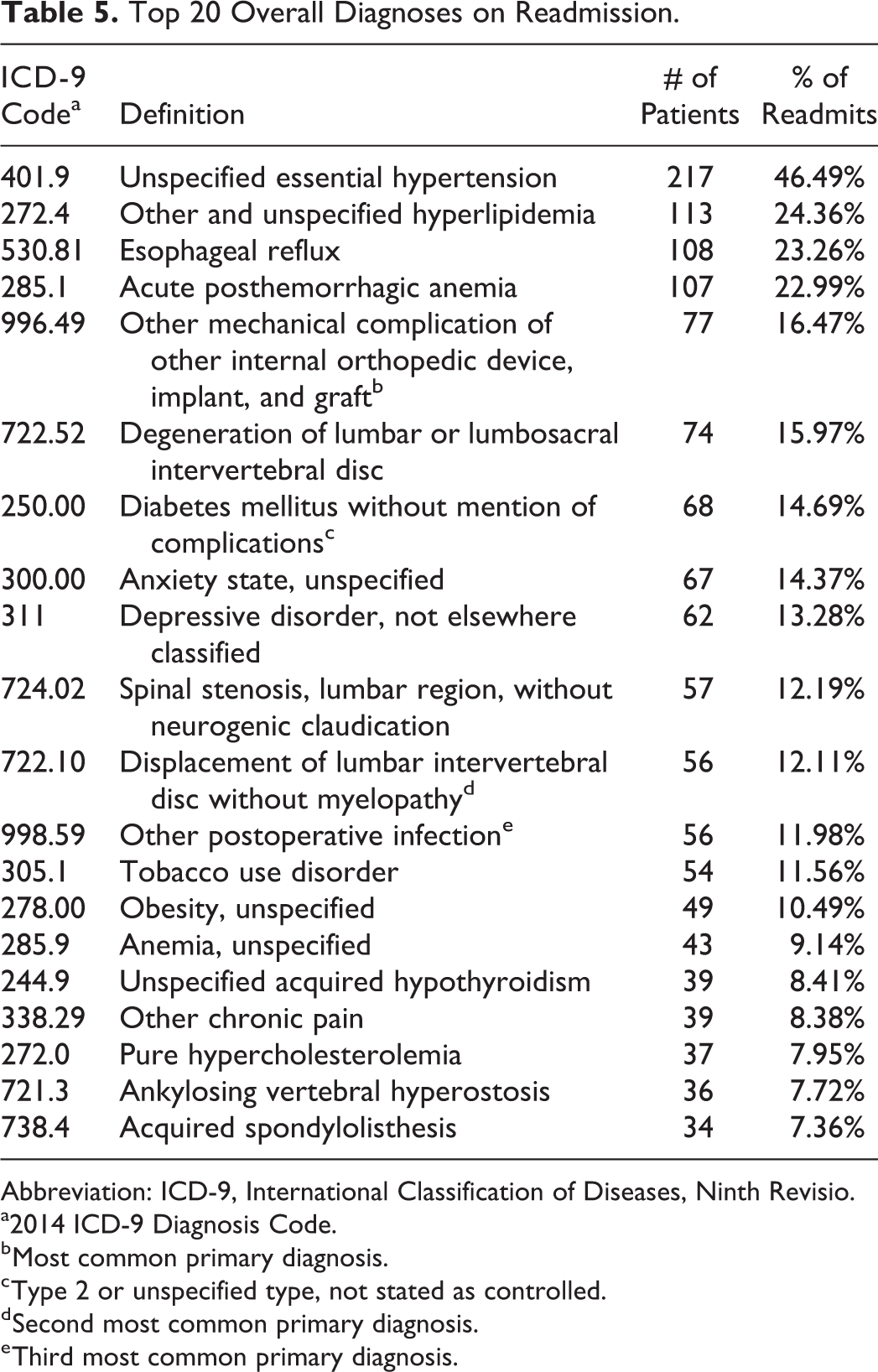
Abbreviation: ICD-9, International Classification of Diseases, Ninth Revisio.
a2014 ICD-9 Diagnosis Code.
b Most common primary diagnosis.
c Type 2 or unspecified type, not stated as controlled.
d Second most common primary diagnosis.
e Third most common primary diagnosis.
Total Hospital Cost
The average total hospital cost for patients who were readmitted (ie, cost of index hospitalization in addition to cost of readmission) within 90 days was estimated to be $136 087 compared with $39 935 for patients who were not readmitted (ie, incurred expenses for index hospitalization only); P < .001. Consequently, readmission within 90 days was associated with an average of $96 152 in additional hospital costs.
Discussion
To our knowledge, this is the first study to look at 90-day rates of readmission following elective revision lumbar spinal fusion in the inpatient setting. Prior to the onset of the BPCI and CJR programs, much of the readmission data regarding orthopedic procedures was focused on the 30-day window. An analysis of ACS-NSQIP (American College of Surgeons National Surgical Quality Improvement Program) data from 2005 to 2013 found a 30-day readmission rate of 5.8% following lumbar fusion revision surgery. 20 Another previous review of ACS-NSQIP data found that PLIF/TLIF (posterior lumbar interbody fusion/transforaminal lumbar interbody fusion) and ALIF/LLIF (anterior lumbar interbody fusion/lateral lumbar interbody fusion) revision lumbar surgery were associated with a 53% increased odds of morbidity, including bleeding events requiring transfusion. The study, however, found no significant difference between readmission rates in revision versus primary lumbar procedures. 21 There have been numerous studies to report 90-rates readmission rates following lumbar surgery, though the surgical approach and study designs certainly differ. Baaj et al conducted an analysis of 86 869 patients who received lumber spinal fusion surgery between 2005 and 2014 using the New York Statewide Planning and Research Cooperative System (SPARCS) and reported an overall 90-day readmission rate of 24.8%. 22 However, the authors noted that the state of New York had one of the highest rates of readmission in the nation. Cui et al examined 26 727 posterior lumbar fusion cases performed in 2013 in the NRD and reported an overall 90-day readmission rate of 9.74%. 23 These 90-day readmission rates appear higher than the 3.2% readmission rate from our data. Differences in our readmission rate from those reported in the literature likely reflect our exclusion of nonelective cases and serial readmissions (ie, if a patient was readmitted more than once). However, these latter differences are likely small and difficult to measure. 24 Further studies would be warranted to identify the specific causes for disparity between rates of readmission.
Of the 29 comorbidities analyzed by our study, only diabetes with chronic complications was found to be associated with increased odds of readmission. Our findings correlate with previous studies examining risk factors for readmission following lumbar surgery. 20,25,26 This makes sense clinically, given diabetes’ association with impaired wound healing, neuropathy, and increased risk of infection. 27 Since there are an increasing number of Americans living with diabetes, 28 it is important for surgeons to identify and medically optimize glycemic levels in patients undergoing elective revision lumbar surgery.
There is a lack of previous literature examining surgical approach in revision lumbar fusion and associated risk of readmission. There are previous studies that investigate how surgical approach affects readmissions following primary lumbar fusion, and this may provide insight into how surgical approach affects readmissions after revision lumbar fusion. A review of 343 068 Medicare patients undergoing elective spinal surgery from 2003 to 2007 found that both a combined anterior and posterior approach and a posterior approach were associated with decreased rates of readmission in comparison to anterior approach (OR 0.81 and 0.67, respectively) after undergoing elective lumbar surgery. 29 The findings of our study suggested that any of the lumbar fusion revisions that involved anterior approach carried increased odds of readmission at 90 days (OR 1.40). This discordance is best explained by our study’s broader payer mix, utilization of a 90-day window of inquiry versus a 30-day window, and focus on revision lumbar fusion versus all elective lumbar spine surgery.
Interestingly, according to our data, when compared with the Medicare population, it appears that private payors and patients receiving their health benefits through Medicaid may be less likely to be readmitted. Consequently, it is possible that Medicare payer status is associated with increased odds of readmission, which is consistent findings in previously published literature. 30
Our data found no significant difference in the odds of readmissions between different age groups in reference to the 18- to 49-year-old age group. This is in contrast to previous studies that have indicated increasing age as a risk factor for readmission following elective lumbar surgery. 29 This finding is important for physicians to consider when assessing the risk of readmission before revising a lumbar fusion in older patients. Our findings suggest that older patients are not at an increased risk relative to the 18- to 49-year-old age group based on their age alone.
There has been previous literature looking at hospital charges associated with revision lumbar fusion, but to our knowledge this is the first study to analyze costs associated with 90-day readmissions. 6 We found that the average added hospital cost for patients readmitted within 90 days of elective lumbar fusion revision was $96 152. As the prevalence of primary lumbar fusion and revision procedures increases in the future, implementing strategies to reduce subsequent readmissions will become increasingly relevant. This is important for physicians and hospital administrators to note and potentially control as delivering high-quality health care becomes increasingly important, both on the level of the individual provider as well as at the level of the overall health care system.
There are limitations associated with large database analyses such as this study. Collection of all data is performed retrospectively; therefore, risk of selection bias and coding bias is present. Also, due to the nature of the Nationwide Readmissions Database, only readmissions within the same state and in the same year as the index admission can be tracked. Furthermore, revision lumbar surgery is a heterogeneous cohort, encompassing a wide range of complexity. However, these limitations were acceptable given the large number and geographical distribution of the study population.
Conclusion
There are relevant patient comorbidities and perioperative complications that have an independent, significant association with increased odds of readmission within the 90-day window following elective revision lumbar fusion. Readmissions within the 90-day window have been shown to incur immense total cost to the hospital in comparison to those patients who were not readmitted. Implementation of strategies to mitigate the impact of these comorbidities and complications will help improve outcomes and reduce hospital costs within this population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.