
Abstract
Study Design
Retrospective Cohort Study.
Objectives
Patients with sickle cell disease (SCD) experience distinct physiological challenges that may alter surgical outcomes. There has been no research establishing 10-year lumbar fusion (LF) implant survivorship rates among individuals with SCD. This study aims to determine the 10-year cumulative incidence and indications for revision LF between patients with and without SCD.
Methods
A national database was queried to identify patients with and without SCD who underwent primary LF. SCD patients undergoing LF were propensity-score matched in a 1:4 ratio by age, gender, and Charlson Comorbidity Index (CCI) to a matched LF control. In total, 246 SCD patients were included along with 981 and 100,000 individuals in the matched and unmatched control cohorts, respectively. Kaplan-Meier survival analysis was utilized to determine the 10-year cumulative incidence rates of revision LF. Furthermore, multivariable analysis using Cox proportional hazard modeling was performed to compare indications for revisions and surgical complications between cohorts including hardware removal, drainage and evacuation, pseudoarthrosis, and mechanical failure.
Results
No significant differences were found in the cumulative incidence of 10-year all-cause revision LF between patients in the SCD cohort and either of the control cohorts (P > .05 for each). Additionally, there were no significant differences between the SCD cohort and either of the control cohorts in regards to the indications for revision or surgical complications in LF (P > .05 for each).
Conclusions
This study indicates that SCD patients do not have increased risk for revision LF, nor any of its indications.
Introduction
Sickle cell disease (SCD) is a well-recognized hematologic disorder affecting approximately 100,000 Americans. 1 Individuals affected by SCD, whether homozygous or heterozygous for the genotype, are predisposed to complications which lead to a higher likelihood of needing revision surgery, particularly in total joint arthroplasty.2-4 These complications encompass a cascade of end-organ failure, avascular necrosis as a result of vascular occlusion, chronic anemia, and repeated infections due to impaired immunity.5,6 In the current literature, the effect of SCD on joint arthroplasty is limited to total knee arthroplasty (TKA)2,3 and total hip arthroplasty (THA). 4 Interestingly, research in these areas has shown that SCD is linked to unfavorable outcomes in patients undergoing TKA, whereas a study investigating the influence of SCD on THA outcomes did not find a significant difference when compared to non-SCD patients.
Whereas prior studies indicate decreased survivorship and increased risk of revision in TKA, 3 literature suggests limited impact on survivorship in the setting of THA. 7 However, conspicuously absent from the existing body of literature is an exploration of the effects of SCD on lumbar fusion surgeries. With a growing trend in volume of lumbar fusion surgeries within the United States 8 and with recent advancements elongating the lifespan of SCD patients, there is an urgent need to characterize the impact of SCD on lumbar fusion outcomes. Moreover, to the best of our knowledge, there are currently no studies investigating the impact of SCD on revision rates in lumbar fusion.
Thus, the main objectives of this study are twofold: (1) to assess the influence of SCD on 10-year lumbar fusion implant survival and (2) to identify etiologies for lumbar fusion revision and surgical complications in SCD patients compared to both a matched non-SCD cohort and an unmatched general population cohort. Based on the results of prior literature as well as the increased likelihood of infection inherent in the SCD population, we hypothesize that SCD patients will exhibit significantly higher rates of 10-year all-cause revisions and an increased prevalence of infections following lumbar fusion when compared to either a matched control cohort or the general population. By addressing these hypotheses, this research aims to provide evidence-based recommendations and insights that can inform the decision-making process when considering lumbar fusion as a treatment option for individuals living with sickle cell disease.
Methods
Database
A database study was conducted utilizing the PearlDiver Patient Records Database (https://www.pearldiverinc.com/). The database contains information of more than 157 million patients from 2010-2021 with minimal loss to follow-up. As the database utilizes completely de-identified patient data, this study is considered exempt from obtaining informed consent. Additionally, this study was reviewed by the institutional IRB and has been deemed exempt from IRB review (IRB# NCR213330).
Patient Population
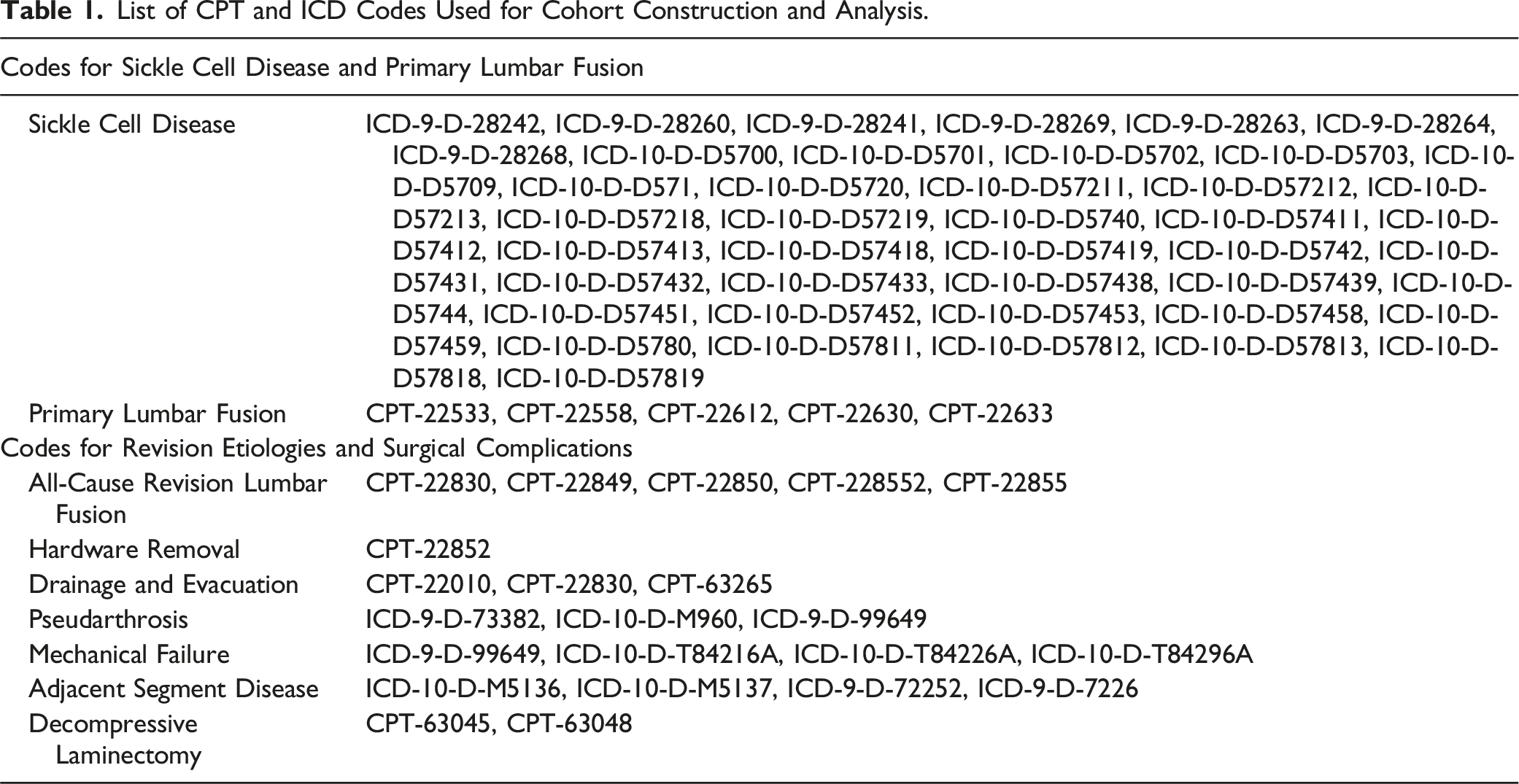
List of CPT and ICD Codes Used for Cohort Construction and Analysis.
Demographic, Comorbidities, and Outcome Variables
Demographic characteristics included age, gender, and Charlson Comorbidity Index (CCI). The primary outcome was the 10-year cumulative incidence for all-cause revision. Secondary outcomes included the indications for revisions and surgical complications in patients with SCD when compared to those without. Observed indications for revision included pseudarthrosis, mechanical failure, and adjacent segment disease. Observed surgical complications included hardware removal, drainage and evacuation, and decompressive laminectomy.
Propensity Score Matching
Demographic and comorbidity characteristics of Sickle Cell, Matched Control, and Unmatched Control cohorts.
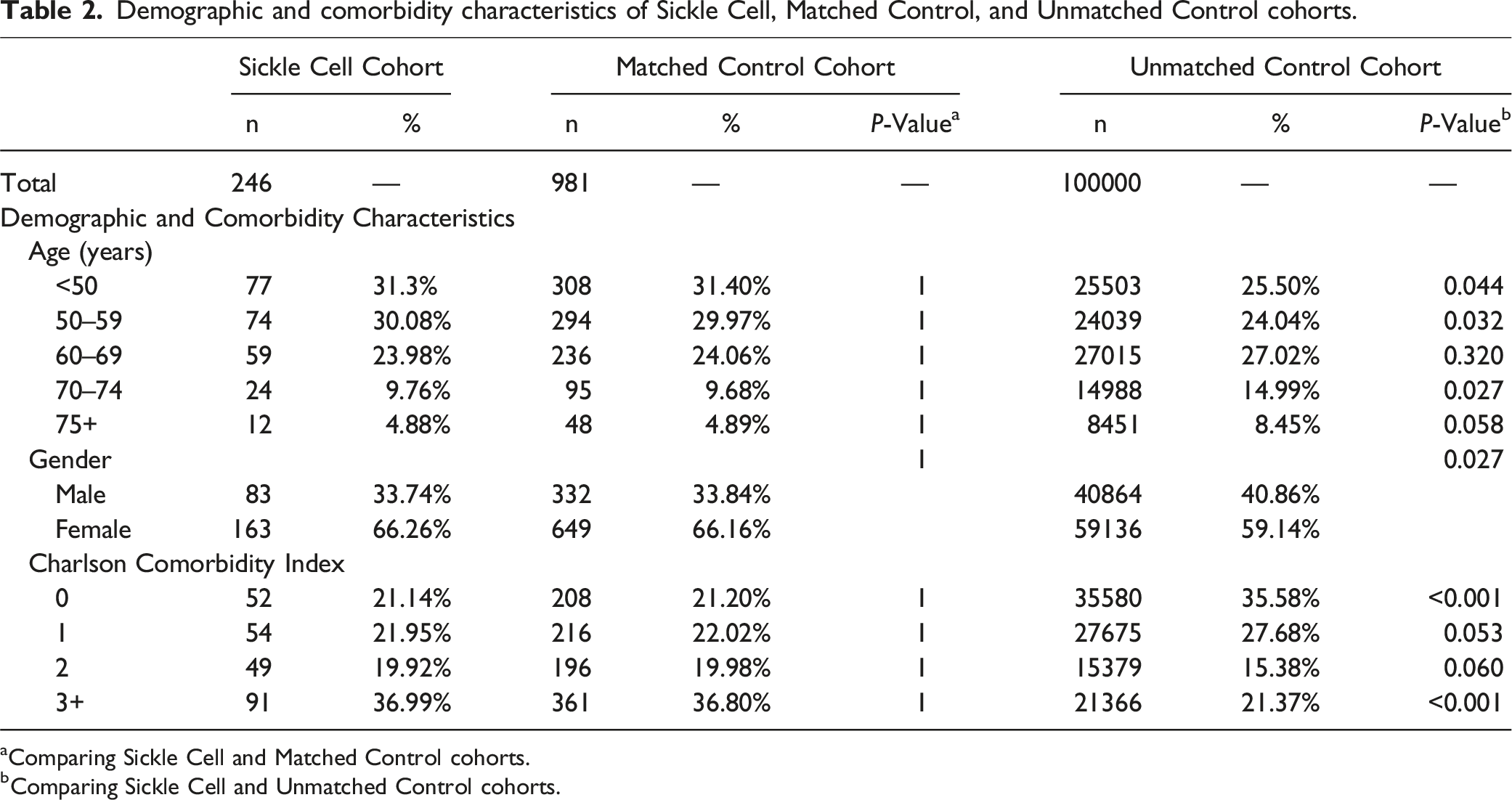
aComparing Sickle Cell and Matched Control cohorts.
bComparing Sickle Cell and Unmatched Control cohorts.
Statistical Analysis
Demographics and indications were compared in univariate analysis utilizing student t-tests and chi-square. Results were recorded as the incidence/prevalence rate (%) and the P-value. Kaplan-Meier survivorship analysis was utilized to generate the 10-year cumulative incidence of all-cause revision between the study cohorts, and cox proportional hazard model was conducted to quantify these differences in the cumulative incidence rates with the output recorded as the hazard ratios (HR), 95% confidence intervals (95% CI), and the P-value. A P-value less than .05 was used for the alpha level of statistical significance. All analyses were conducted using R software (Vienna, Austria) inherent in the PearlDiver database.
Results
Cumulative Incidence for Revision
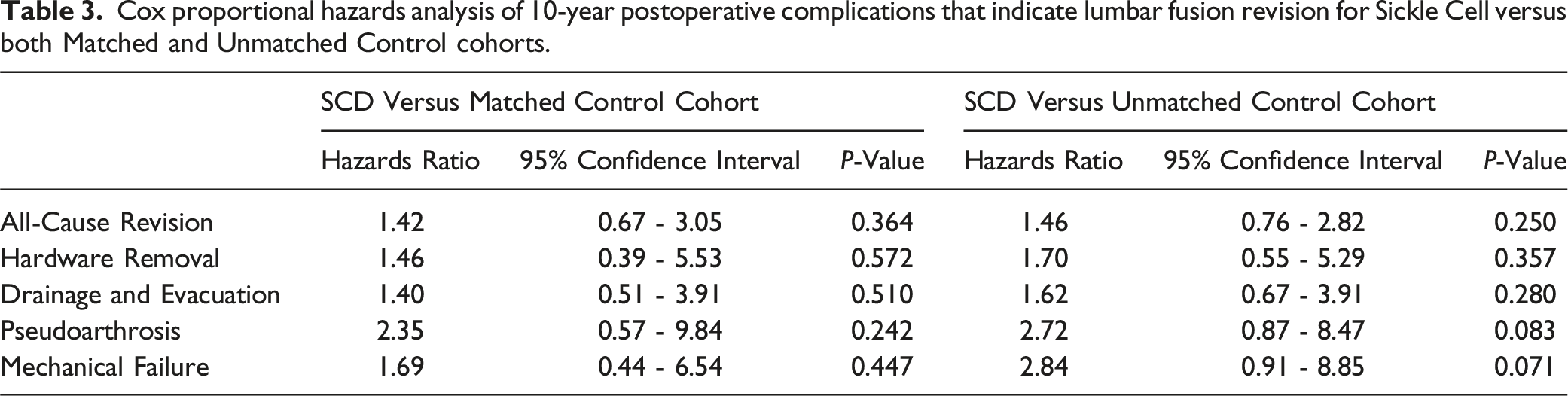
The cumulative incidence of revision for the SCD cohort was 1.2%, 2.4%, 3.3%, and 4.2% at 90-day, 2-year, 5-year, and 10-year, respectively (Figure 1). In the unmatched control, the cumulative incidence for revision for those without SCD was .6%, 1.4%, 2.3%, and 3.0% at 90-day, 2-year, 5-year, and 10-year, respectively (Figure 1). In the matched control, the incidence for revision was .7%, 1.3%, 2.7%, and 3.0% at 90-day, 2-year, 5-year, and 10-year, respectively (Figure 1). Compared to SCD patients, the 10-year cumulative incidence rate was not significantly higher for either the matched control (HR: 1.42; 95% CI: .67-3.05; P = .364) or unmatched control (HR: 1.46; 95% CI: .76-2.82; P = .250) cohorts (Table 3). Cumulative incidence of 10-year all-cause revision for the Sickle Cell, Matched Control, and Unmatched Control cohorts. A solid black line indicates the cumulative incidence of 10-year all-cause revision for the Sickle Cell cohort while the dashed and dotted lines indicate the cumulative incidence of 10-year all-cause revision for the Matched Control and Unmatched Control cohorts respectively. Cox proportional hazards analysis of 10-year postoperative complications that indicate lumbar fusion revision for Sickle Cell versus both Matched and Unmatched Control cohorts.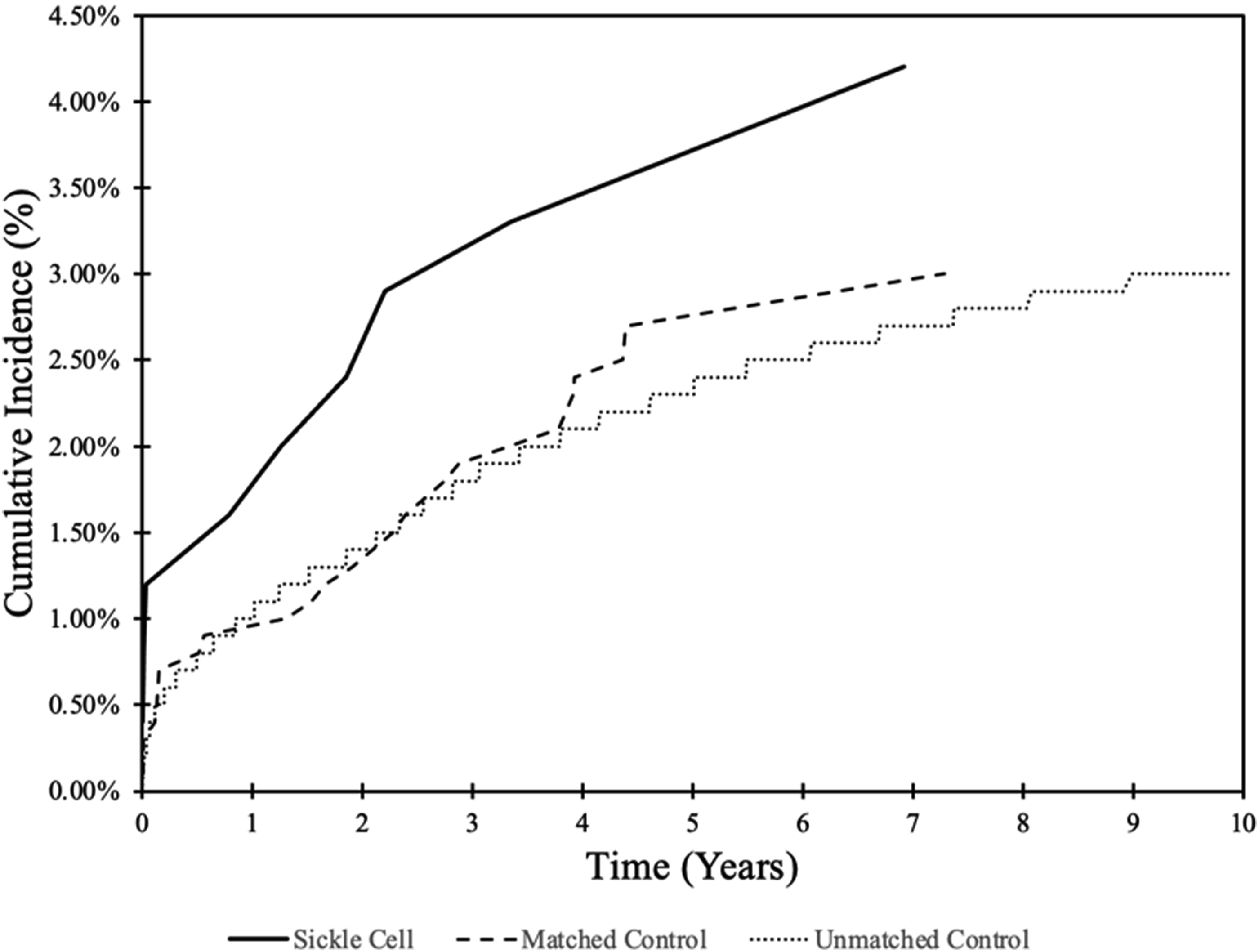
Indications for Revision and Surgical Complications
When compared to the matched control, SCD patients were not more likely to undergo revision for instrumentation removal (HR: 1.46; 95% CI: .39-5.53; P = .572), drainage and evacuation (HR: 1.40; 95% CI: .51-3.91; P = .510), pseudarthrosis (HR: 2.35; 95% CI: .57-9.84; P = .242), or mechanical failure (HR: 1.69; 95% CI: .44-6.54; P = .447) within 10 years of LF (Table 3).
When compared to the unmatched control, SCD patients were not more likely to undergo revision for instrumentation removal (HR: 1.70; 95% CI: .55-5.29; P = .357), drainage and evacuation (HR: 1.62; 95% CI: .67-3.91; P = .280), pseudarthrosis (HR: 2.72; 95% CI: .87-8.47; P = .083), or mechanical failure (HR: 2.84; 95% CI: .91-8.85; P = .071) within 10 years of LF (Table 3).
Discussion
This study demonstrates that SCD patients experience similar rates of revision for LF when compared to patients without SCD over a 10 year period. Additionally, we did not find significant differences in any of the observed indications for revision LF in the SCD cohort. To the best of our knowledge, this is the first study to establish 10-year LF survivorship rates among individuals with SCD. Our findings indicate that a diagnosis of SCD should not impact surgical decision-making from a survivorship perspective.
Albeit the first study to investigate the impact of SCD on LF outcomes, the results of this study can still be contextualized against the backdrop of analogous orthopedic procedures. Parel et al recently found that SCD patients are more likely to undergo revisions compared to patients who do not have SCD within 10 years of total knee arthroplasty (TKA), 2 and Viswanathan et al. further demonstrated that SCD patients are at significantly higher risk for systemic complications following TKA such as deep vein thrombosis and acute chest syndrome. 3 Similarly, in total hip arthroplasty (THA), Fassihi et al. found that SCD patients are at increased risk of medical and surgical complications. 4 In contrast, however, the literature in total shoulder arthroplasty (TSA) has been largely contrary. In a retrospective review of 17 primary TSAs in patients with SCD, Marigi et al demonstrated no significant difference in complication or reoperation rate when compared to patients without SCD. 9 These findings suggest that SCD may confer differential peri-operative and post-operative risks depending on the type of surgery performed. Thus, given the silence of current literature on the impact of SCD in lumbar spine surgery, there is an urgent need to establish the effect of SCD on survivorship and indications for all-cause revision following LF.
Several factors may contribute to our observation that, as in TSA, SCD does not significantly impact survivorship following LF. SCD is a multi-faceted disease with diverse clinical manifestations, and its effects may vary depending on the specific surgery performed. In the case of TKA and hip surgery, studies have highlighted increased risks and complications associated with SCD, possibly due to the systemic nature of these procedures and the potential for increased blood loss, thrombotic events, and peri-operative challenges.2,3,10 In contrast, LF is a procedure primarily focused on the lumbar spine, which involves different physiological considerations. LF typically involves stabilization and fusion of vertebrae, which may not entail the same level of systemic stress or blood flow alterations as procedures involving the extremities or hip joints.11-13 Consequently, the risk profile for LF may differ from that of other orthopedic surgeries in SCD patients. Furthermore, the spinal anatomy and its relative isolation from systemic circulation could potentially explain why SCD may not exert the same level of impact on LF outcomes. 14
There are several clinical implications to consider from this study. Our findings indicate that the physiological challenges associated with SCD do not have a substantial impact on the long-term stability of lumbar fusions. Moreover, our findings suggest that despite the unique vascular and hematological aspects of SCD, the indications for revision LF are not significantly different in SCD patients. This finding may alleviate concerns that SCD-related complications might lead to distinct patterns of revision surgery in these patients. This suggests that surgical management of LF in SCD patients can follow similar protocols as for patients without SCD, which may streamline surgical decision-making and postoperative care.
It is important to consider the potential limitations when interpreting the results. This study relied on retrospective patient data, which is contingent upon the accuracy of the data that is coded in the database and may be susceptible to errors. However, this limitation should affect all study cohorts to similar extents. Furthermore, our analyses were constrained by the available variables within the PearlDiver database. Thus, while we could observe trends in implant survivorship and etiologies for revision, we were unable to delve into more detailed information such as surgical approach or perioperative variables, which have potential influences on revision rates. As this finding is limited to revision LF and its indications, further research is needed to determine whether SCD alters postoperative outcomes in other orthopedic surgery procedures.
Conclusion
Over a 10-year period, patients who have SCD experienced similar all-cause revision when compared to patients who did not have SCD. Spine surgeons should consider these findings and need not delay care in SCD patients solely on the basis of concerns for survivorship.
Footnotes
Author Contributions
Conceptualization: BTS, AR, PMP, TQ, AM, TCP; Data Curation: BTS, AR, PMP, TQ, AM, TCP; Formal Analysis: BTS, PMP; Funding Acquisition: AM, TCP; Investigation: BTS, AR, PMP, TQ, AM, TCP; Methodology: BTS, AR, PMP, TQ, AM, TCP; Project Administration: BTS, AR, PMP, TQ, RAR, AM, TCP; Resources: AM, TCP; Software: BTS, PMP; Supervision: AM, TCP; Validation: BTS, AR, PMP, TQ, AM, TCP; Visualization: BTS, AR, PMP, TQ, RAR, AM, TCP; Writing – Original Draft: BTS, AR, PMP, TQ, AM, TCP; Writing – Review and Editing: BTS, AR, PMP, TQ, RAR, AM, TCP.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.