
Abstract
Study Design:
Prospective cohort study.
Objective:
To evaluate the long-term effectiveness of a posterior dynamic spine stabilization (PDS) System called PercuDyn system as a treatment for low back pain (LBP) in patients with degenerative disc disease who have failed conservative treatment.
Methods:
Thirty-five patients (21 males, 14 females, mean age 36 years) with chronic LBP due to degenerative disc disease underwent percutaneous facet augmentation with the PercuDyn system. Indications for implanting the PercuDyn device were chronic LBP without sciatica, significant disc degeneration, and who failed conservative treatment. Follow-up after surgery ranged from 4 to 8 years. Patients were clinically evaluated using visual analogue scale (VAS), Oswestry Disability Index (ODI) questionnaire, and the EQ-5D3L.
Results:
The VAS scale and ODI scores improved at 6 months, 1 year, 2 years, and 4 to 8 years in comparison with the baseline values (P < .001 and P < .01, respectively). Equally, data from the EQ-5D-3L questionnaire suggested improvements in all domains, including pain and discomfort, over the follow-up period. However, during follow-up, 16 patients (46%) have had unsatisfactory outcome including failure of implant to resolve symptoms (n = 8), developed symptomatic disc protrusion (n = 4), and loosening of the screws (n = 4).
Conclusion:
Our clinical experience highlights the rather high overall failure rate of this system. Although, some patients show significant improvement in their symptoms, we believe that patients with LBP related to degenerative disc disease are a poor indication for this PDS device.However, large scale studies, with optimised selection criteria are needed to demonstrate the exact role of this device in spinal patients.
Keywords
Introduction
Low back pain (LBP) is one of the widest spread public health problems in industrialized countries, with an estimated 60% to 70% of the adult population experiencing a back problem at some point in their lives. 1,2 Recently, LBP became one of the most common health disabilities in the world, as more than75% of patients with LBP suffer from short time disability and around 5% become permanently disabled. 3,4 The cause of LBP can be difficult to identify, but some reports suggest that disc degeneration are a source of LBP. Schwarzer et al 5 reported that 39% of cases of chronic LBP are discogenic. Other causes of LBP are facet joints degeneration, cauda equina syndrome, infection, tumor, osteoporosis, arthritis, and fractures. Chronic LBP treatment varies from nonoperative management, including physiotherapy to interventional treatment, which might include spinal injections or radiofrequency ablation for pain relief. 6 If conservative methods fail, operative options such as spinal fusion, anterior disc replacement and posterior dynamic stabilization (pedicle/spinal process-based devices) can be considered. Because of uncertain outcome, many young and active patients do not want to proceed with major surgeries such as fusion or disc replacement as this cannot be reversed, if the patient fails to improve. In addition to that, there is a risk of biomechanical changes after fusion surgery, which may lead to accelerated degeneration of the adjacent segments and persistent back pain.
In recent years, minimal invasive, motion-preserving techniques that restore intersegmental stability have been developed as an alternative method for open surgery in the treatment of LBP. Minimal invasive techniques have a better immediate postoperative recovery due to lesser soft tissue injuries, blood loss and injury to other anatomical structures compared with open procedures. 7 In addition, these devices might decrease the risk of adjacent segment degenerative changes by minimizing the biomechanical changes of the spine through preserving mobility of the targeted level and disperse the load from the facet joints/intervertebral discs. 8
In this study, we present results of an 8-year prospective trial on the effectiveness of a posterior dynamic spine stabilization (PDS) system called PercuDyn system as a treatment for LBP in patients with degenerative disc disease (DDD) who have failed conservative treatment. This cohort study is to present the long-term follow-up results of patient receiving the PDS-PercuDyn device. We hypothesized that PercuDyn system (Interventional Spine Inc) is an effective and long lasting minimally invasive treatment of patients presenting with persistent LBP related to DDD. Several case series have described the immediate and short-term results. However, no experiences are published on the long-term results of this implant. Authors publishing their experiences with the PercuDyn device have reported follow-up periods up to 24 months. 9 -12 However, given the nature of the treated condition and the type of the implant, it is important to describe the long-term effect, risks and benefits. Although we did not achieve the recruitment target of 50 patients over the period from 2009 to 2014 as set out in our trial protocol, the study was not extended, and recruitment was stopped at 35 patients due to high rate of treatment failure. In that light, it is perhaps especially appropriate to report the long-term effects of this system.
Methodology
This is a prospective single site cohort study with an ethical approval by the original ethical review board. From September 2009 to November 2013, 35 consecutive patients were enrolled and treated with PercuDyn implant at a single center. All patients included in this study underwent at least 1 year of comprehensive conservative treatment. Inclusion criteria: Patients with LBP aged 18 years and older, chronic LBP without radiation to the lower limbs, not undergoing any other concurrent treatments for pain other than routine analgesia, patients with lumbar disc degeneration grade 2, 3, or 4 according to Pfirrmann’s classification of lumbar intervertebral disc degeneration, and patients who failed nonoperative treatment such as nonsteroidal anti-inflammatory drugs (NSAIDs), muscle relaxant, local injective therapies, and structured physiotherapy. Exclusion criteria included previous lumbar spinal surgery, normal intervertebral disc (grade 1) or loss of the intervertebral disc height of more than 50% (grade 5) on magnetic resonance imaging scan according to Pfirrmann’s classification, significant leg pain from neural compression (slipped disc, sciatica), trauma, infection, malignancy, inflammatory joint disease, unstable neurological signs/symptoms, pregnancy, and inability to complete questionnaires. The primary outcome measure was visual analogue scale (VAS). The secondary outcome measures included the Oswestry Disability Index (ODI) and EuroQol 5-D (EQ5-D).
Recruitment Process
Patients with LBP referred by their general practitioners to the spinal outpatient clinic of our institution were screened for eligibility for the study. Potential participants were selected in a spinal outpatient clinic and then contacted by the researcher receiving both verbal and written information relating to participation in this study, and written informed consent was obtained before enrollment.
Assessment and Follow-up
A preoperative lumbar spine magnetic resonance imaging, and flexion/extension radiographs were acquired. In addition, patients completed booklet questionnaires of 3 outcome measures (ODI, EQ-5D-3L, and VAS). Patients were admitted for surgery as a day case or for 24-hour stay. Outpatient review took place at 6 weeks, 6 months, 1 year, 2 years, and long-term varying between 4 and 8 years postoperatively in form of a clinical review, flexion/extension radiographs, and evaluation with questionnaires. Adverse events were assessed continuously throughout the follow-up according to the trial protocol.
Operative Techniques
PDS PercuDyn system is a percutaneous facet augmentation device which aims to treat chronic LBP due to DDD. The device limits excessive extension and pressure on the disc and facet joints, acting as a mechanical shock absorber between the articulating facets. 13 The advantage of PercuDyn system is that it is minimally invasive (percutaneous), has a minimal anatomical impact and is reversible. It limits both extension and lateral bending at the level targeted, suitable for all levels of the lumbar spine (including L5/S1) and comes in one size screw. It can be done under local or general anesthesia. The device can be removed percutaneously, if there has not been any improvement which leaves the patient still with other surgical options.
The PercuDyn system is inserted through 2 small skin incisions (15 mm, bilateral, minimally invasive access ports).
The patient is positioned prone and slightly flexed. Intraoperative fluoroscopy (anteroposterior and lateral views) is used to mark the entry point and infiltrate with local anesthetic. A bone marrow needle (Jamshidi biopsy needle) is inserted targeting the pedicle at the medial inferior articular facet joint, followed by the insertion of a K-wire. The biopsy needle is removed, and an incision of 15 mm length of the skin and the fascia is made to accommodate the insertion of the Teleport (tubular retractor). The final step is the insertion of a tap, countersink and implant (Figure 1). At the end of the procedure, all patients have radiography to check the final position of the implants (Figure 2A and B).
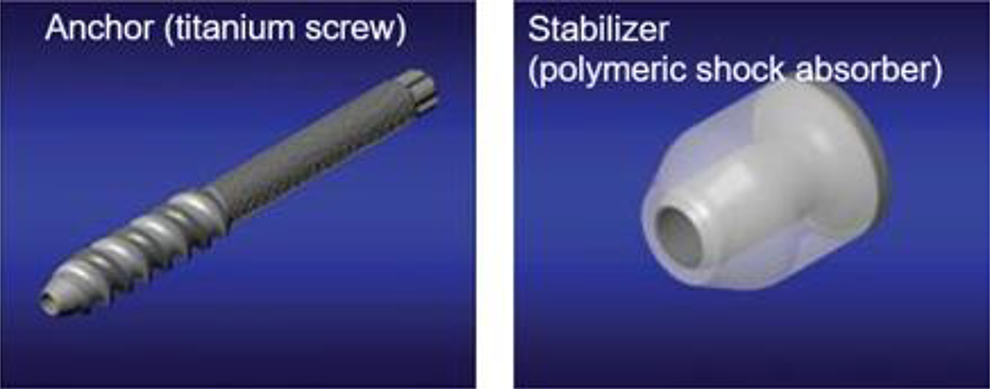
PercuDyn implants.
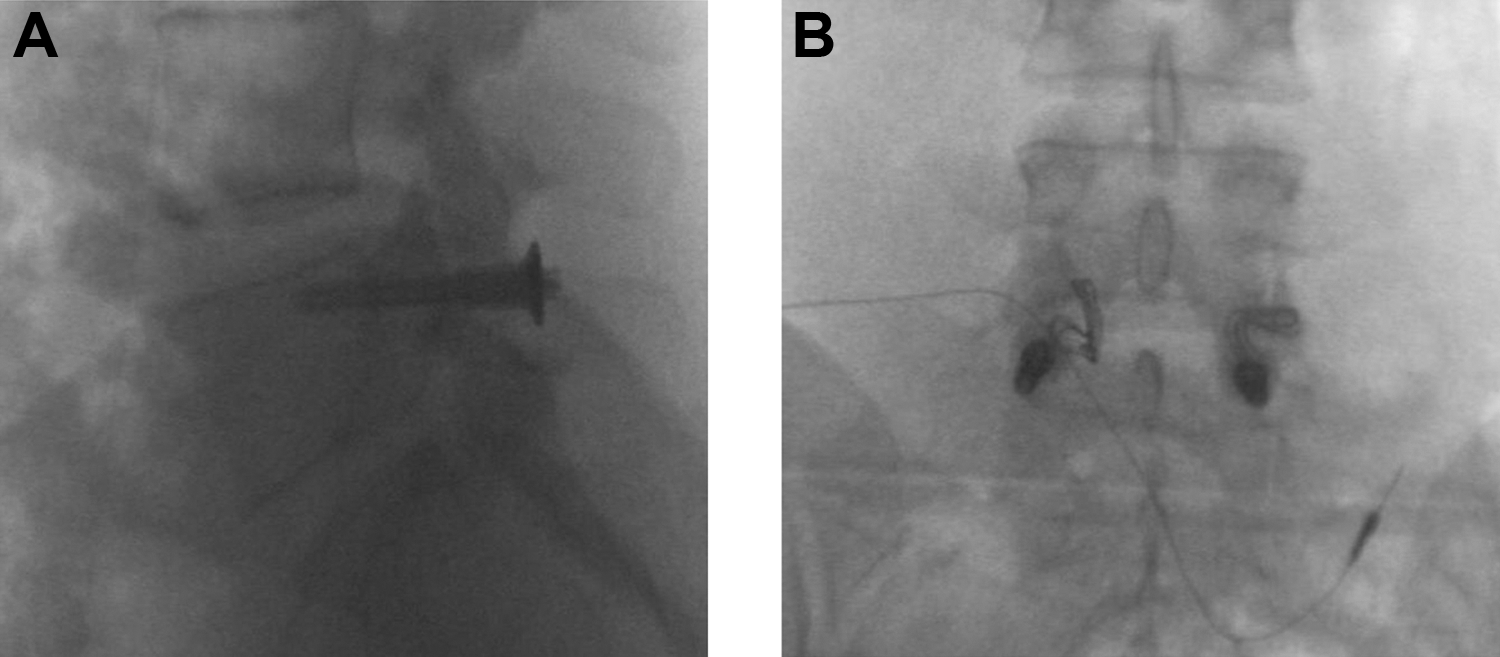
(A) Postoperative radiograph, lateral view. (B) Anteroposterior view, showing the implant’s position.
Statistical Analysis
Ideally statistical methods such as multivariate regression models are needed that allow an isolation of (treatment) effect. It should be noted that because of the low sample size the power of regression analyses is limited. Therefore, descriptive analysis was primarily used. Categorical variables are reported as frequency (%) and compared between groups by the chi-square or Fisher exact test. Continuous variables are summarized as either mean ± SD or mean (range) and compared across groups using a Student t test or Mann-Whitney U test as appropriate. Statistical significance was set at P < .05.
Results
Over a 4-year period, a total of 35 successive patients, 21 (60%) were male and 14 (40%) were females, referred to the spinal clinic at our institution fulfilled the inclusion criteria and consented to participate in the study. Patients age ranged from 23 to 58 years (mean [SD] age 35 [8.7] years). Most of the patients, 21(60%) have no associated comorbidities (Table 1). Out of 35 patients, 19 presented with 1 level degenerative disc, 12 presented with 2 levels degenerative disc, and 4 with 3 levels degenerative disc. Fifty-five spinal levels were treated (26 levels L5/S1, 23 levels L4/5, 5 levels L3/4, 1 L2/3). The mean (range) operative time was 66 (25-146) minutes according to the number of levels were treated. For 1-, 2-, and 3-level procedures, the mean operative time was 55 minutes (range 25-146), 73 minutes (range 42-145), and 90 minutes (range 50-130), respectively.
Characteristics of Enrolled Subjects.
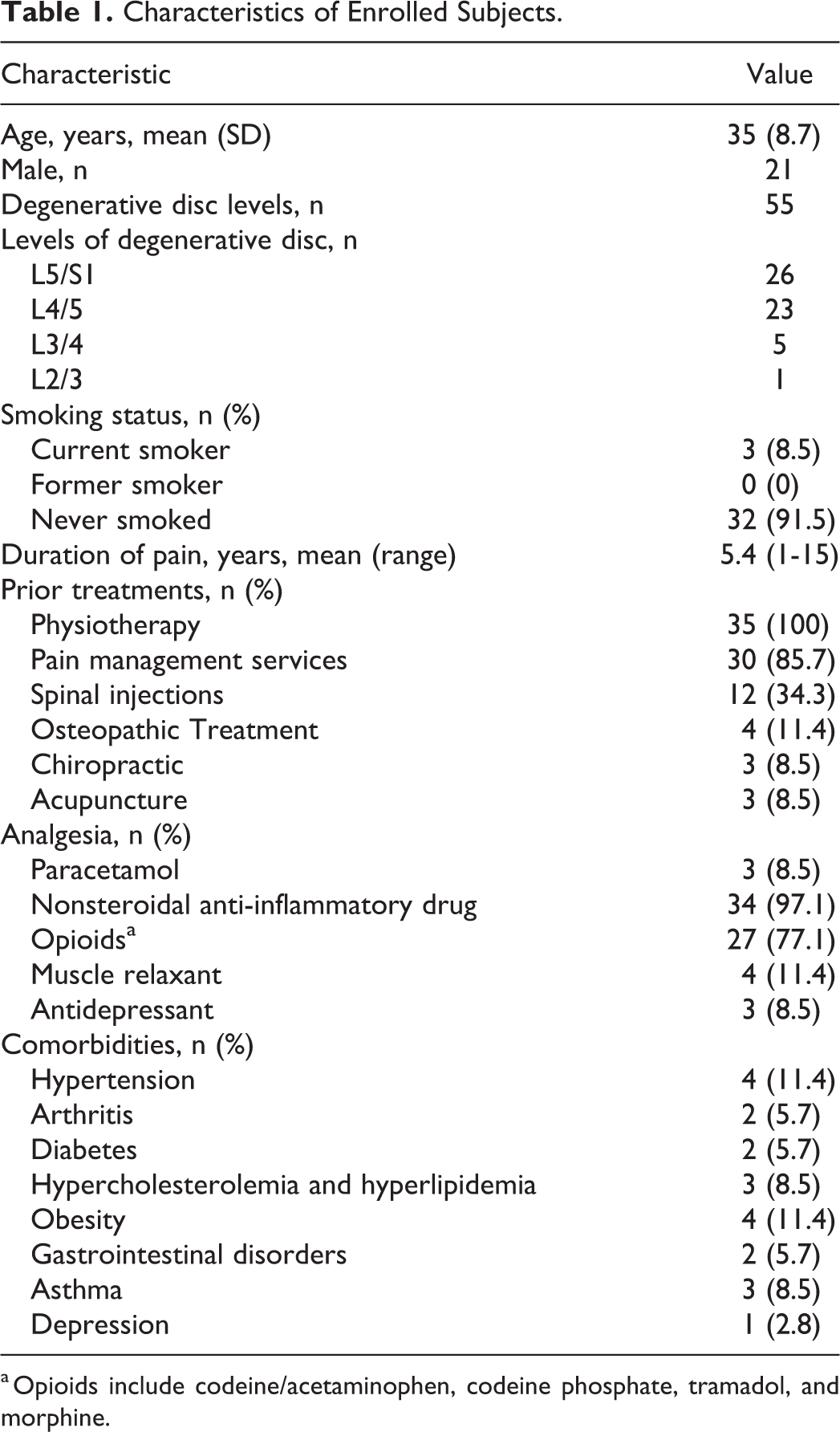
a Opioids include codeine/acetaminophen, codeine phosphate, tramadol, and morphine.
The VAS scale showed a statistically significant difference at 6 months, 1 year, 2 years, and 4 to 8 years with regard to the baseline (preoperative) value (P < .001). There was more than 20% reduction in the VAS score between the baseline score (preoperative) and other scores obtained during follow-up (Table 2 and Figure 3A). For chronic back pain, a change of about 20% in VAS score is regarded to be clinically significant. 14 Descriptive statistics on the VAS score suggested that the PercuDyn system might improve the patients back pain and disability respectively (Table 3).
Changes in Visual Analogue Scale (VAS) Pain and Oswestry Disability Index (ODI) Over the Follow-up Period.

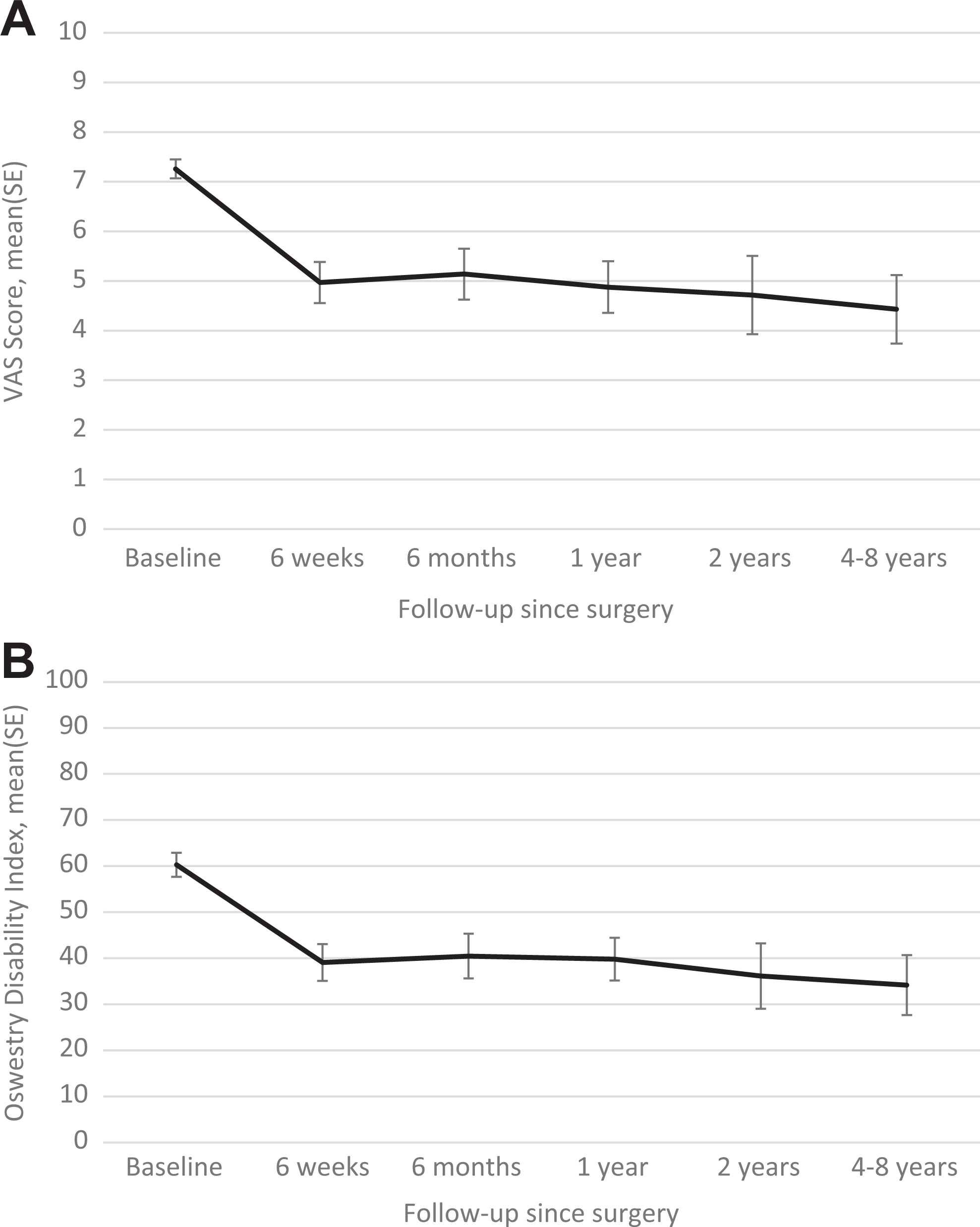
VAS score changes during follow-up (A) and Oswestry Disability Index changes during follow-up (B). SE, standard error; VAS, visual analogue scale.
Back Pain Reporting (%) Following Treatment With the PercuDyn Device in Patients Stratified by Visual Analogue Scale (VAS) Scores Group Over the Follow-up Time-Points.

The ODI demonstrated a significant difference (P < .01) at 6 months, 1 year, 2 years, and 4 to 8 years follow-up with regard to the baseline (preoperative) value. Also, there was more than 20% difference ODI score between baseline score (preoperative) and other scores obtained during follow-up appointments (Table 2 and Figure 3B). A difference of 10% of ODI is considered to be clinically significant in back pain. 15
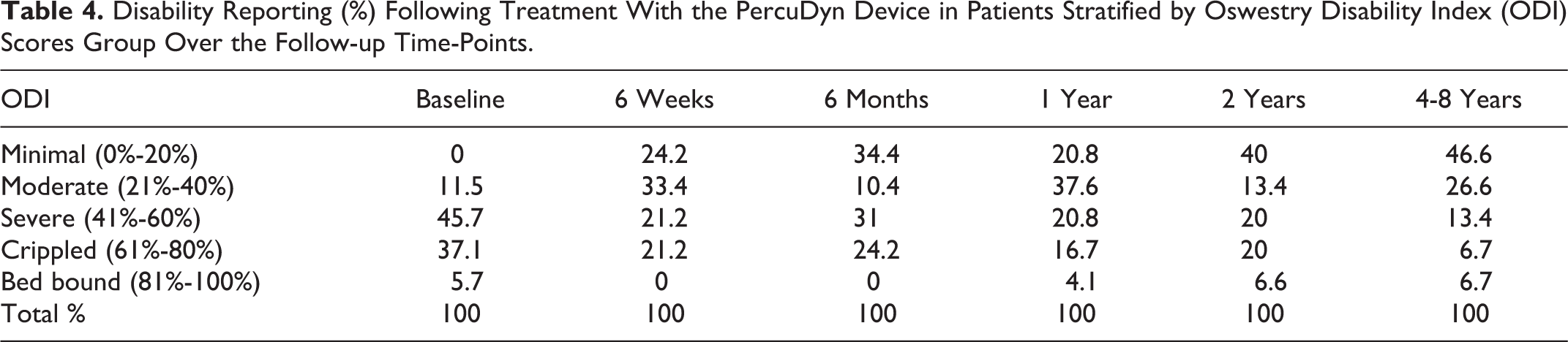
Descriptive statistics on the ODI score, there was a significant difference in the disability index in patients 6 weeks postoperative follow-up. More than 88% of the patients reported severe, crippling or bed-ridden disability in the preoperative assessment, this figure decreased to 42% with no patients in the bedridden category (Table 4).
Disability Reporting (%) Following Treatment With the PercuDyn Device in Patients Stratified by Oswestry Disability Index (ODI) Scores Group Over the Follow-up Time-Points.
Data from the EQ-5D-3L health status questionnaire demonstrated changes on each domain of the EQ-5D at the different time-points of follow-up compared with the baseline. The changes suggest improvements in patients’ mobility, self-care, anxiety, and depression in addition to the improvement in pain/discomfort, and usual activity. Using the Pareto Classification of Health Change (PCHC) to evaluate overall improvements in EQ-5D profiles, 16 it suggests that the overall health has improved (Table 5 and Figure 4).
EQ-5D-3L Health Status Outcome Stratified by Domains and EQ-VAS Scores in Patients Treated With the PercuDyn Device at Various Time-Points of Follow-up Compared With Baseline.
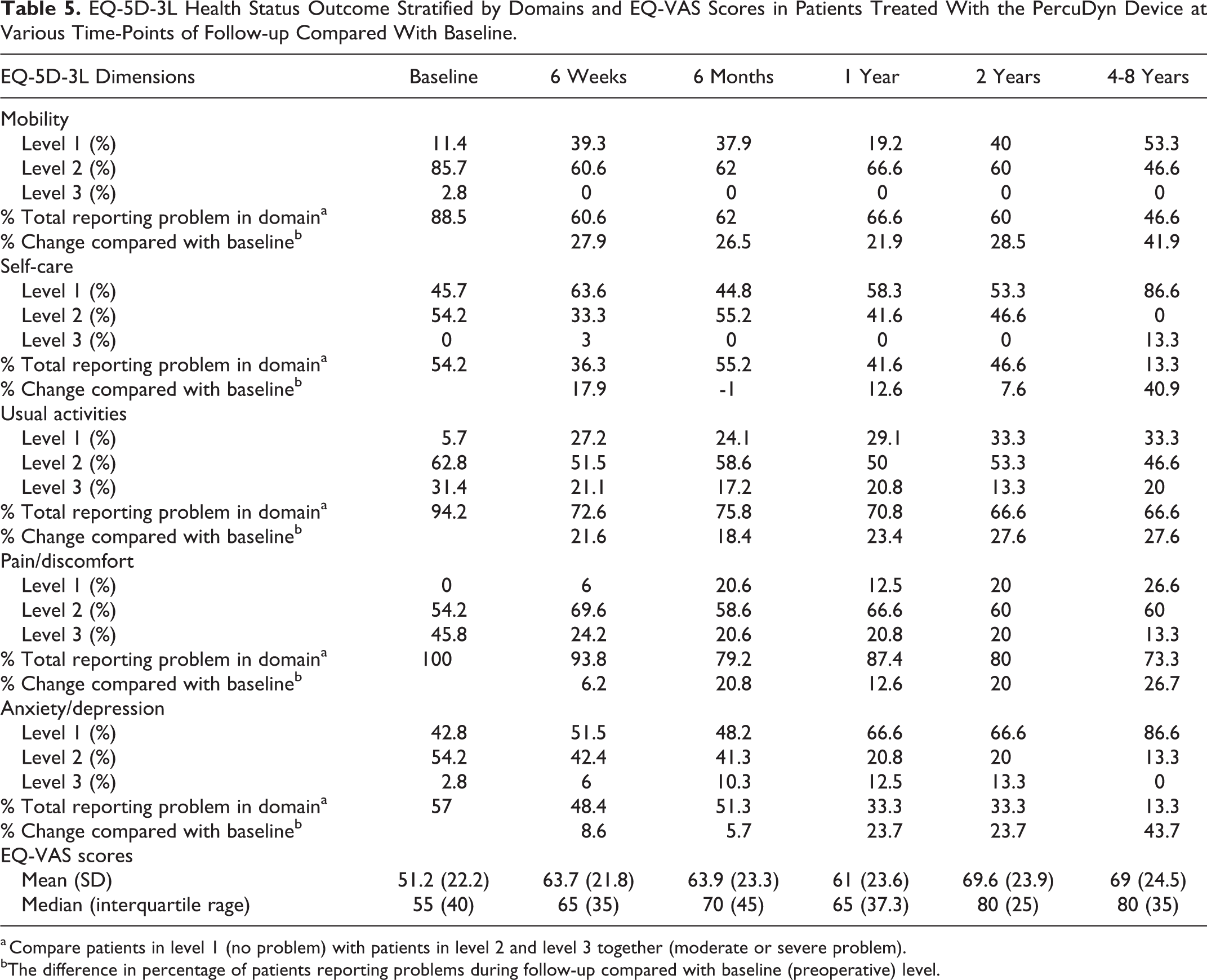
a Compare patients in level 1 (no problem) with patients in level 2 and level 3 together (moderate or severe problem).
bThe difference in percentage of patients reporting problems during follow-up compared with baseline (preoperative) level.
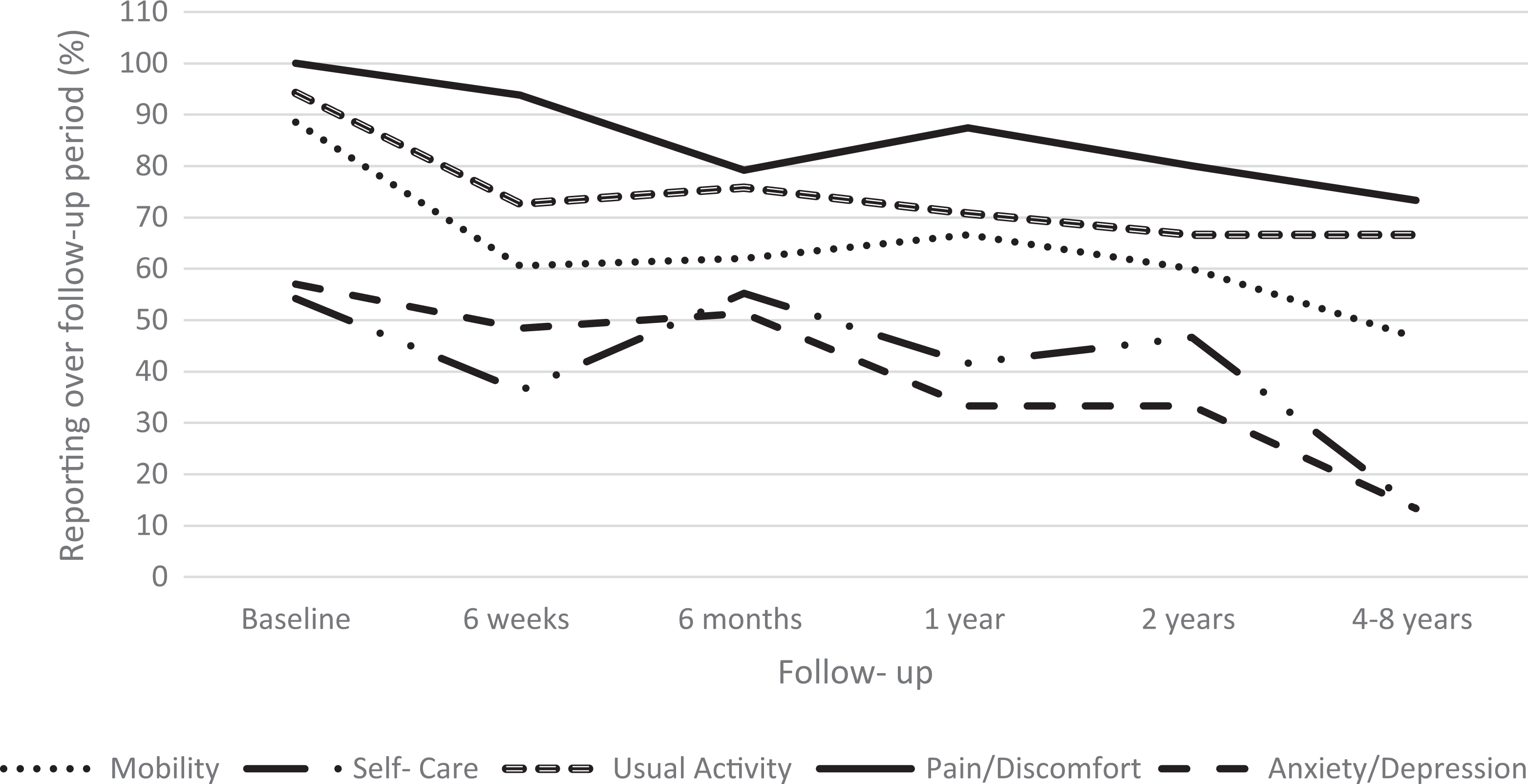
EuroQol 5-D (EQ5D) reporting over follow-up period.
The EQ-VAS shows patients overall health on a 0-to-100 scale, we observed a 12.5% improvement in the mean overall health status within 6 weeks postoperative compared with the preoperative score; this modestly increased to 17.8% within 4 to 8 years follow-up (Table 5). The EQ-VAS shows a statistically significant difference at 6 weeks, 6 months, 1 year, 2 years, and 4 to 8 years when compared with the preoperative value (P < .05) (Table 6).
Table Summarizing Case Series Reporting Outcomes on the PercuDyn Device.
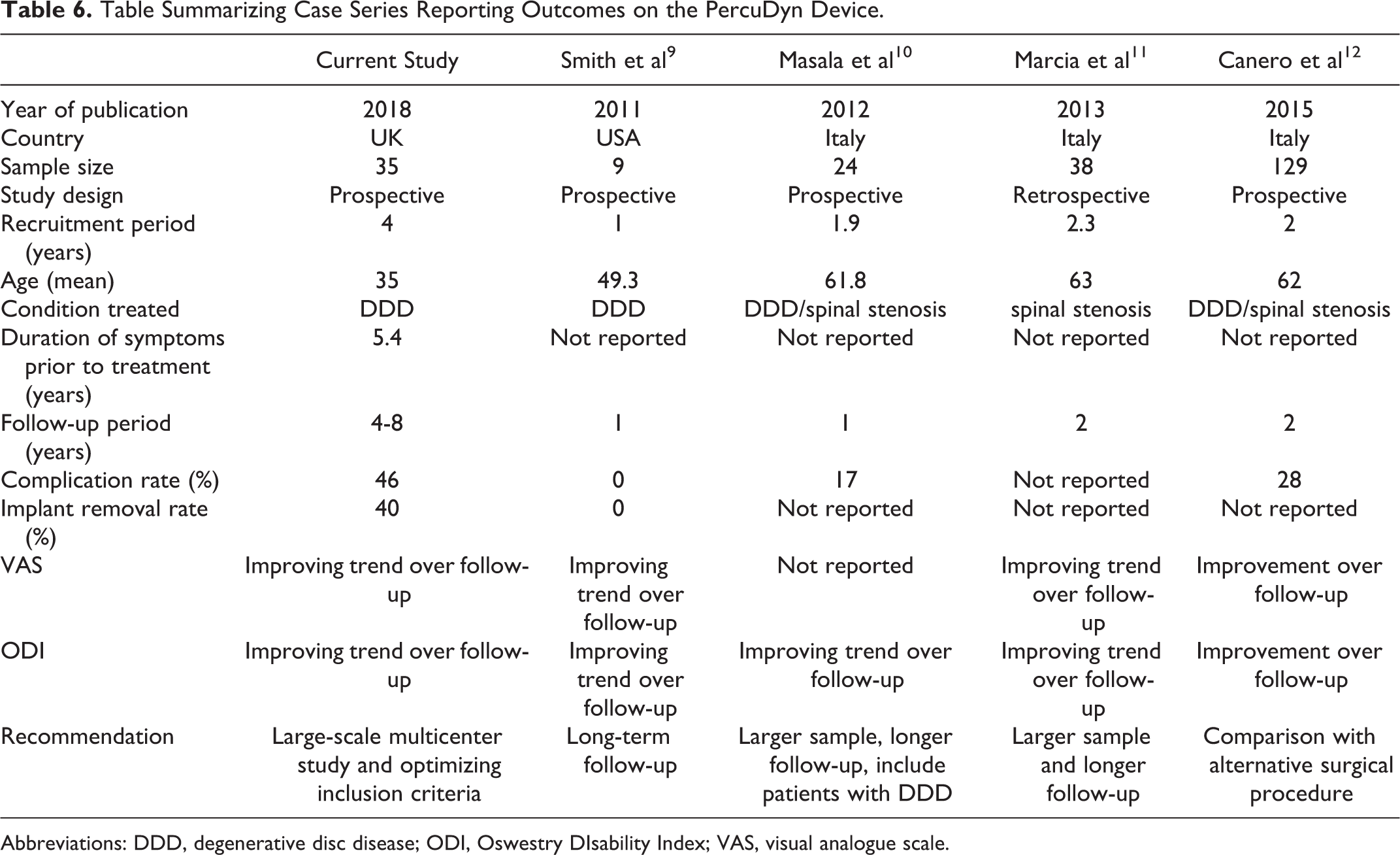
Abbreviations: DDD, degenerative disc disease; ODI, Oswestry DIsability Index; VAS, visual analogue scale.
During postoperative follow-up, 16 patients (46%) developed implant-related issues in form of failure to improve symptoms (n = 8), symptomatic disc protrusion (n = 4), and loosening of the screws (n = 4) (Table 7). Out of the 16 patients, 14 patients underwent implants removal, 5 of them had spinal fusion and 2 underwent microdiscectomy at the same time. The remaining 2 patients (out of 16) developed radicular symptoms related to spinal level other than the level of the implant, underwent microdiscectomy without implant removal. Implant complications were defined in our study protocol as secondary outcomes, and these patients were followed up clinically and radiologically. Thirteen patients were still suffering severe pain with average VAS score 77.9%, including the 5 patients with the spinal fusion, while only 3 patients left with mild pain with a mean VAS of 37%. All the patients with severe pain were actively followed up and treated in the pain management clinic. No complications related to operative techniques such as nerve root injury, inaccurate placement of the implant, infection or cerebrospinal fluid leak were reported. The characteristics of 19 (54%) patients who still have the implants are summarized in Table 8.
Adverse Events in 35 Consecutive Patients Treated With the PercuDyn Device.

Characteristic of the Patients With Implants.
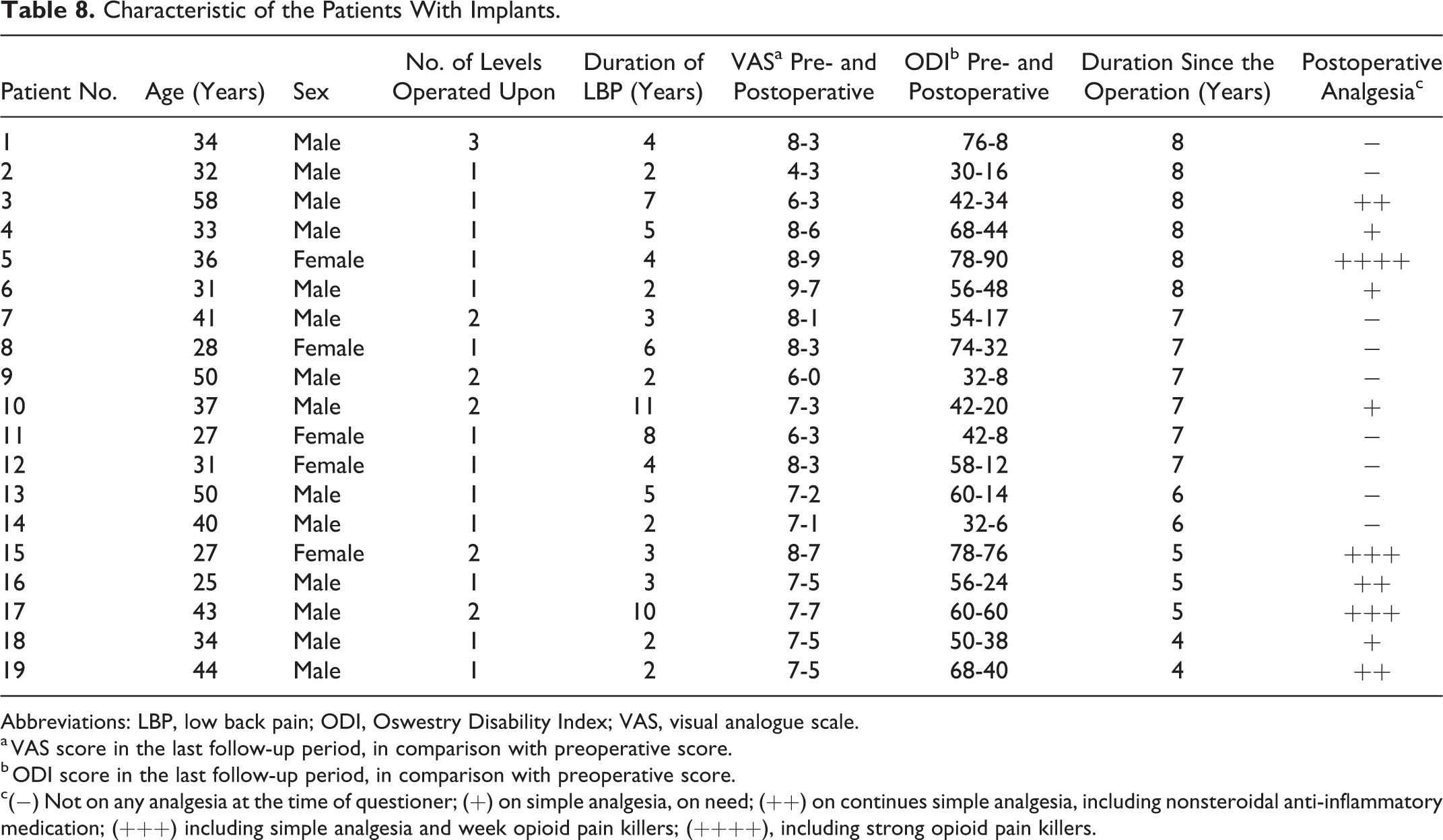
Abbreviations: LBP, low back pain; ODI, Oswestry Disability Index; VAS, visual analogue scale.
a VAS score in the last follow-up period, in comparison with preoperative score.
b ODI score in the last follow-up period, in comparison with preoperative score.
c(−) Not on any analgesia at the time of questioner; (+) on simple analgesia, on need; (++) on continues simple analgesia, including nonsteroidal anti-inflammatory medication; (+++) including simple analgesia and week opioid pain killers; (++++), including strong opioid pain killers.
Discussion
PDS procedures are used to treat chronic back pain related to degenerative discs or spinal stenosis. Preventing spine hyperextension movement and improve the diameter of the intervertebral foramina and spinal canal by lifting the medial facet joint and prevent buckling of the ligamentum flavum during hyperextension movement. The implants can reduce pain by stabilizing the affected levels or levels restricting excessive motion while allowing a degree of mobility without affecting the adjacent levels. It reduces the load on facet joints and intervertebral discs, which can be pain generators in many of patients with chronic LBP. 17 Dynamic stabilization systems are often seen as a gold standard and an alternative to the spinal fusion procedures for treatment of LBP that have failed conservative treatment. 18
A matched cohort study based on the Spine Tango Registry by Bieri et al 8 reported longer term findings of DSS dynamic stabilization system versus posterior lumbar interbody fusion (PLIF). They reported comparable improvement in primary and secondary clinical outcomes at an average 3.3 years. The DSS group had only 3 repeat surgeries at an average 4.5 years. There is a big difference in revision surgery rate between their study and current study. The other difference was that they used DDS after open decompression for patients with back and leg pain. The current study used percutaneously applied implants without open decompression for patients with pure DDD. 8 In a prospective study on 387 patients with degenerative lumbar spinal disease treated with DSS dynamic stabilization system, Greiner-Perth et al 19 found a good and stable clinical outcome after 4 years follow-up and concluded that this treatment is an effective alternative to spinal fusion surgery. However, there is a paucity of evidence comparing PDS versus spinal fusion as treatment of back pain, and whether dynamic stabilization is more beneficial than spinal fusion remains debatable. 20 -22
The PercuDyn system is a facet augmentation where screws need to be positioned under the medial part of the facet joints in to the pedicles in order to alleviate the load on the facet joints directly, and the intervertebral disc of this level indirectly. 17 Furthermore, PercuDyn PDS system is transferring the load from the articular facet joint to the pedicle, which is a very strong bone. This is usually achieved by slight flexion of the facet joints during insertion of the implants. In comparison with other PDS devices that use the spinal process as a pivot to decrease the load. Masala et al 10 reported no device-related complications in their 24 consecutive patients at 1-year follow-up. However, they reported technical difficulties in insertion of PercuDyn implants. 10 This was not our experience. However, it is of great advantage to have experience in other percutaneous techniques to be familiar with landmarks and trajectories on fluoroscopy. In one case of a high-level athlete (rower), we experienced difficulties in insertion of the device due to heavily calcified pedicles.
In comparison with other PDS devices like X-Stop and Isobar, the PercuDyn device has more theoretical advantages in treatment of DDD and chronic LBP. It can be easily used at L5/S1 as well as other lumbar spine levels, while other devices are limited benefits at L5/S1 level, given an often small or poorly developed S1 spinous process. 9 Evidence based on cadaveric study comparing 3 posterior lumbar motion preservation devices, PercuDyn system was the most effective in preventing hyperextension and decreasing extension movement with a follower load by a mean of 52% compared with injured conditions, while the effect of X-Stop and Isobar was 27% and 22%, respectively. 23
This PercuDyn study is a prospective cohort study with highly selective inclusion criteria. We recruited patients with LBP related to DDD without associated spinal canal stenosis or radicular features in the lower limbs related to neural tissue entrapment. Only patients with DDD grade 2, 3, or 4 according to Pfirrmann’s classification of lumbar intervertebral disc degeneration were recruited in the study. 24 We followed up patients for an extended period of 4 to 8 years. After the 2-year follow-up, 65% of all patients who did not have the implants removed reported satisfactory outcome of the procedure, with a statistically significant improvement in the outcome measures scores (ODI, EQ-5D-3L, and VAS). Our findings are comparable to those from Canero et al, 12 although they included patients with spinal stenosis and radiculopathy in addition to DDD. They also found a significant improvement in the VAS score and ODI score, with 70% of patients being satisfied with the procedure after 2 years of follow-up. However, they report revision surgery of 14.3% at 5 years due to loosening of the screws. Furthermore, Marcia et al 11 found good improvement of clinical scores (VAS and ODI) in their retrospective evolution of effectiveness of the PercuDyn implant for treatment of degenerative LBP combined with facet joint hypertrophy and canal stenosis, and statistically significant widening of the neural foramina, they reported only one incorrect screw positioning without any further complication at 2 years 11 (Table 6).
In our experience, the most common cause of the implant removal was failure to improve symptoms in 8 patients (22.8%) which appears as early as 6 months follow-up. Radicular symptoms related to prolapsed discs, were reported in 4 patients (11.4%) who were diagnosed after 1-year follow-up and required surgical intervention. Two of the patients with disc prolapsed where in different level of the implants, which did not require implant removal. Loosening of implants was also a common complication after 2 years of follow-up in 4 patients (11.4%), this will total to an overall failure rate of 46%. Short-term follow-up evaluation studies of PDS system have reported that screw loosening in PDS systems is not uncommon, it has been reported that about 5% risk of screws loosening within 2 years follow-up period. However, the degree of clinical impact was not correlate well with this complication and the author recommended a longer period of follow-up evaluation. 25 In our study, all cases with loosening screws or failure to improve back pain underwent revision surgery to remove the implants with or without posterior lumbar fusion, however this is not the case in other literatures. 10 -12
Although the PercuDyn system is purely designed to treat LBP related to DDD and facet joint degeneration, several studies reported benefits from treatment of the spinal canal stenosis and radiculopathy based on the facts that PercuDyn system restricts the extension movement of the spine and potential increase in the diameter of the spinal canal and the intervertebral foramina. 10,11
This study offers insights into an otherwise unexplored area, the long-term outcome of patients with the PercuDyn implant. In our case series, the modest improvement of clinical scores (VAS, ODI and EQ-D5-3L), noted 6 weeks postoperatively, reaches a plateau in the first 6 months and remained stable throughout the follow-up period. This suggests that patients who do not improve in the first few months would be unlikely to improve later. We hypothesize that this is mostly related to the patient’s selection rather than failure of the implants. We believe that missing psychosocial assessment in this study is a significant limitation as pathogenesis of pain in DDD is highly correlated to psychosocial factors. Some of the patients underwent spinal fusion after removal of PercuDyn implant, which also failed to improve their back pain. Although this research provides insights into the effect of this implant during long-term follow-up, there are a few limitations that should be addressed. First, the sample size does not allow for firm conclusions or strong generalizations. This article mainly aims at examining the long-term outcomes of the patients enrolled in this study. Larger studies, including different inclusion criteria and possibly comparison with different PDS products, should be conducted to be able to generalize the results. Also, highly selective inclusion criteria and the single-center design of the study, further limited the overall number of patients and the generalizability of the results. The study was not further extended for recruitments to achieve the prespecified sample of 50 participants due to the early high rate of implant-related adverse effects, which led to implant removal.
Conclusion
Although the theoretical benefit of PDS procedures to decrease the load on facet joints and inter-vertebral discs has led to development of implants such as PercuDyn system, our clinical experience highlights the rather high overall failure rate of this PDS system. Although, some patients show significant improvement in their symptoms, we think that patients with LBP related to DDD are a poor indication for this PDS device. We feel that it is important to present our negative results with the use of PercuDyn, juxtaposed to the promise held for this system cited in the aforementioned literature.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Initially, the author(s) received an unrestricted research grant to perform the study from Interventional Spine Inc; however, this company is no longer operational.