
Abstract
Study Design:
Biomechanics study.
Objectives:
To evaluate the biomechanical advantage of interfacet allograft spacers in an unstable single-level and 2-level anterior cervical discectomy and fusion (ACDF) pseudoarthrosis model.
Methods:
Nine single-level and 8 two-level ACDF constructs were tested. Range of motion in flexion-extension (FE), lateral bending (LB), and axial rotation (AR) at 1.5 N m were collected in 4 testing configurations: (1) intact spine, (2) ACDF with interbody graft and plate/screw, (3) ACDF with interbody graft and plate/loosened screws (loose condition), and (4) ACDF with interbody graft and plate/loosened screws supplemented with interfacet allograft spacers (rescue condition).
Results:
All fixation configurations resulted in statistically significant decreases in range of motion in all bending planes compared with the intact spine (P < .05). One Level. Performing ACDF with interbody graft and plate on the intact spine reduced FE, LB, and AR 60.0%, 64.9%, and 72.9%, respectively. Loosening the ACDF screws decreased these reductions to 40.9%, 44.6%, and 52.1%. The addition of interfacet allograft spacers to the loose condition increased these reductions to 74.0%, 84.1%, and 82.1%. Two Level. Performing ACDF with interbody graft and plate on the intact spine reduced FE, LB, and AR 72.0%, 71.1%, and 71.2%, respectively. Loosening the ACDF screws decreased these reductions to 55.4%, 55.3%, and 51.3%. The addition of interfacet allograft spacers to the loose condition significantly increased these reductions to 82.6%, 91.2%, and 89.3% (P < .05).
Conclusions:
Supplementation of a loose ACDF construct (pseudarthrosis model) with interfacet allograft spacers significantly increases stability and has potential applications in treating cervical pseudarthrosis.
Keywords
Introduction
Anterior cervical discectomy and fusion (ACDF) is the most common surgical procedure for the treatment of cervical radiculopathy and myelopathy. 1 Fusion requires placement of an interbody graft or spacer and ultimately bony union. Unfortunately, nonunion occurs in up to 20% of single level and even higher rates in multilevel fusions. 2 -8 Despite anterior instrumentation, pseudarthrosis results in intersegmental motion and, in many cases, loosening of screws or hardware. Treatment of symptomatic nonunion can be either revision anterior surgery or posterior fusion with or without decompression. A recent meta-analysis showed that both anterior and posterior revision surgery result in similar clinical outcomes but the posterior approach had significantly greater fusion rates. 9 Posterior lateral mass fixation is the most commonly utilized technique although other fixation methods such as interfacet screws and interfacet allograft spacers may provide sufficient stability to allow healing of the motion segment. 10,11
The facet joints align the spinal column and aid in control of motions in all axes. The facet orientation changes from coronal in the cervical and thoracic spines to more sagittal in the lumbar spine, which correspondingly changes direction of movements at those levels. Controlling segmental motion of the facet joints by blocking with bone graft or interfacet allograft spacers may stabilize the spine and result in spine fusion and indirect foraminal decompression. 10,12 -17 Machined interfacet allograft spacers are placed directly into the facet joint and they have a relatively large surface area that stiffens the spinal segment, and potentially increases foraminal height and area to indirectly decompress the neuroforamina. 11,17,18 Interfacet allograft spacers are machined cortical allografts sized 2 to 4 mm in height and contain ridges that provide stability to resist retropulsion. In a cadaveric kinematic study, Tan et al reported the interfacet spacer grafts increased foraminal height by 1.4 mm and cross-sectional area by 18%. 18 Clinical studies have similarly demonstrated increased foraminal height and area after placement of interfacet spacers. 13,19 Recent studies have described the application of these interfacet allograft spacers to treat disc herniation, and spondylotic radiculopathy and myelopathy. 13,20,21
We have observed that, in addition to foraminal decompression, the interfacet spacers significantly stabilize the spine and may be used for the treatment of pseudarthrosis after ACDF. In this biomechanical study, we hypothesize that the interfacet machined allograft spacers would significantly increase segmental stability after failed anterior interbody fusion. The study aims are to evaluate the biomechanical properties of machined bone allograft interfacet spacers in a pseudarthrosis model and to determine the biomechanical advantage gained from placement of allograft spacers into an unstable single-level and 2-level ACDF construct.
Methods
Seventeen C3-C7 fresh-frozen human cadaveric spines (10 male and 7 female; mean age 51 years) were used. Orthogonal radiographs were taken to ensure the absence of significant degeneration, congenital fusion, deformity, or fractures. Extraneous soft tissue was dissected with preservation of the ligaments and intervertebral discs. The superior aspect of C3 and inferior aspect of C7 were mounted into a resin pot (Bondo; 3M, Maplewood, MN) with screws drilled into the endplates to increase purchase.
The caudal end of the cervical segment was attached to the floating table of the test frame (Bionix 6DOF; MTS, Eden Prairie, MN) and displaced to align the potted cephalad section of the cervical segment with the MTS actuator. The actuator containing the 6 degrees of freedom load cell with a 5 kN/110-N m load capacity (MC3A-6; AMTI, Berkshire, United Kingdom) was locked to the cephalad side. Four infrared emitting diode markers (Optotrak Certus; NDI, Ontario, Canada) were attached to each vertebral body and a reference marker was attached to the immobile section of the MTS actuator. Spinal motion was tracked using the NDI Optotrak Certus with First Principles motion capture software (Northern Digital Inc, Ontario, CA).
Range of motion was assessed using a pure-moment flexibility testing protocol. Tests were conducted in flexion-extension (FE), lateral bending (LB), and axial rotation (AR) to a maximum of ±1.5 N m by applying unconstrained moments to the cephalad vertebral body using the 6 degrees of freedom load cell of the MTS. Moments were applied in the test direction of interest while moments in the remaining directions were maintained close to 0 N m and shear forces minimized using the floating table. The loading waveform consisted of 3 sinusoidal loading cycles with moments applied at a rate of 0.025 Hz. Data from the reflective markers were collected during all cycles of the loading modes. Data from the last cycle was utilized to calculate the range of motion for each test configuration. Euler angle calculations were performed using a custom Matlab code (Matlab r2014a, Mathworks, Natick, MA) to quantify intersegmental range of motion.
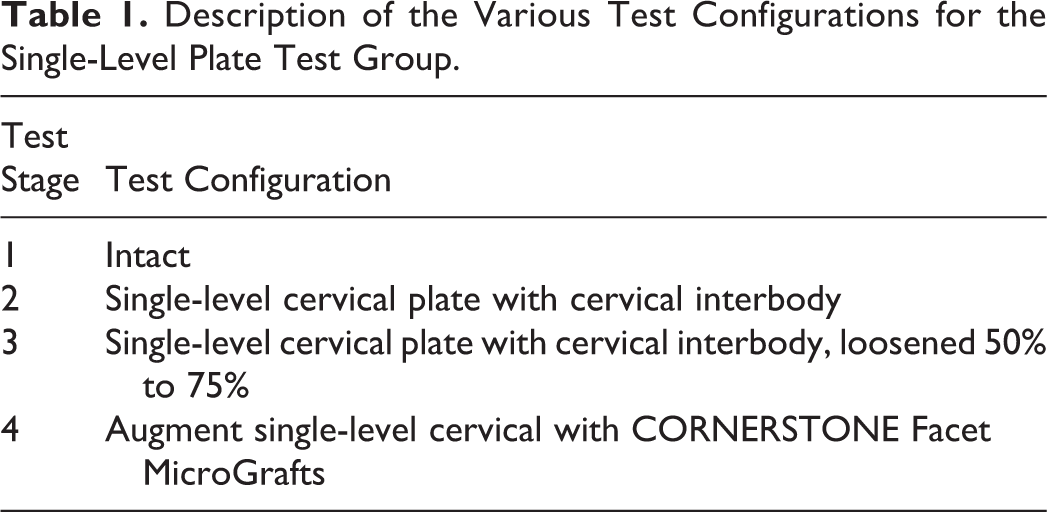
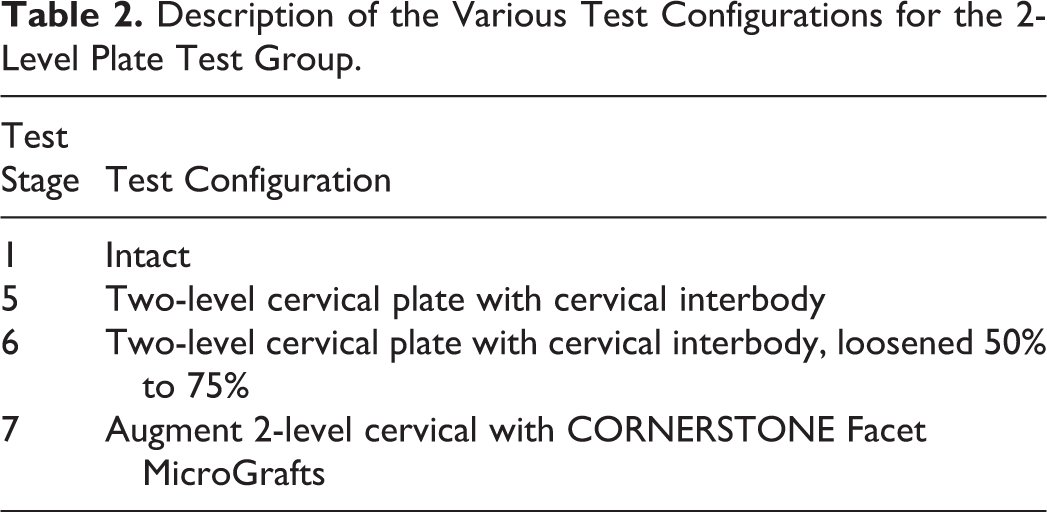
Fellowship-trained spine surgeons experienced in the utilized techniques performed all surgical procedures. We examined the following 7 conditions (Tables 1 and 2, Figure 1):
Description of the Various Test Configurations for the Single-Level Plate Test Group.
Description of the Various Test Configurations for the 2-Level Plate Test Group.
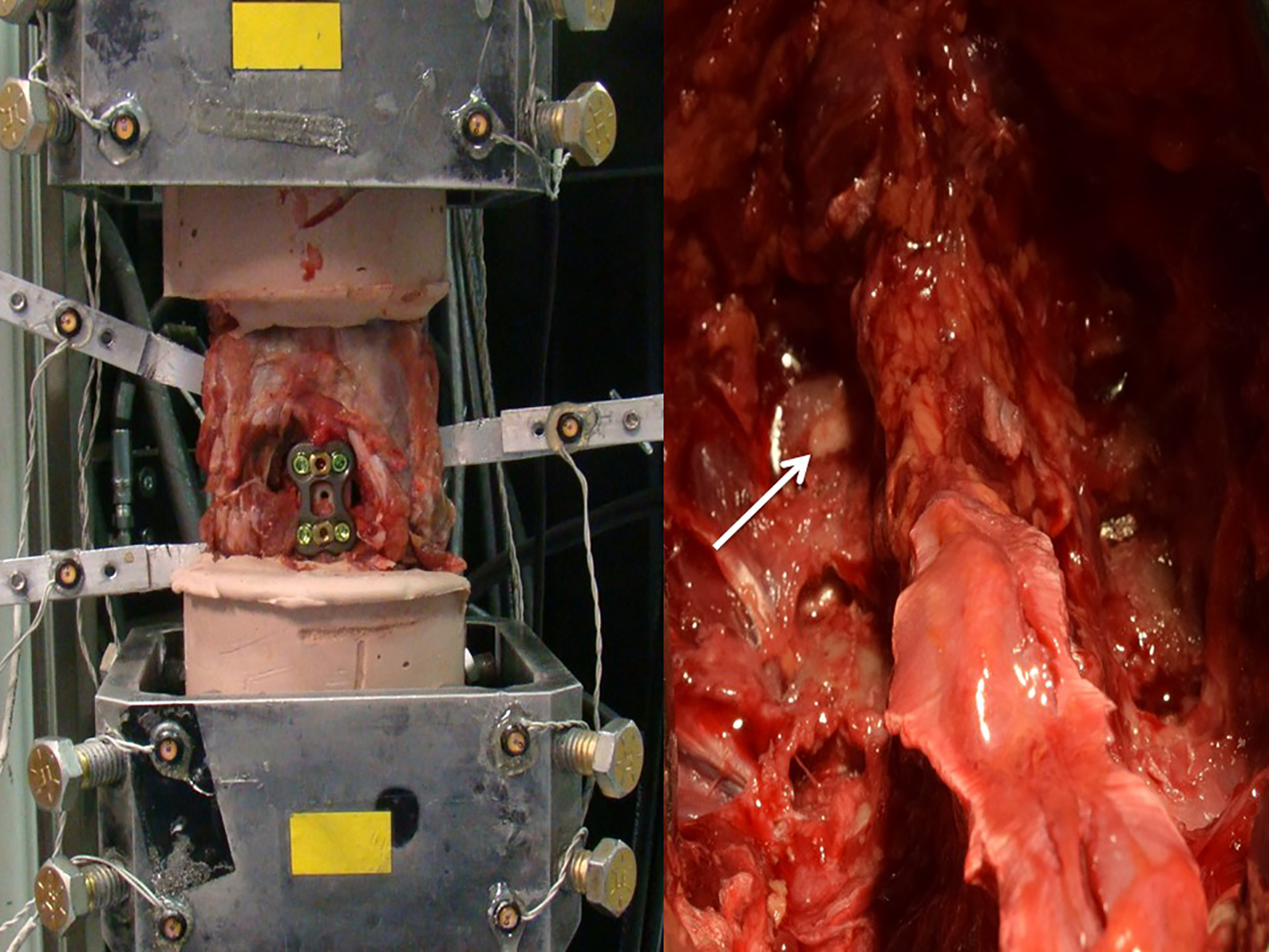
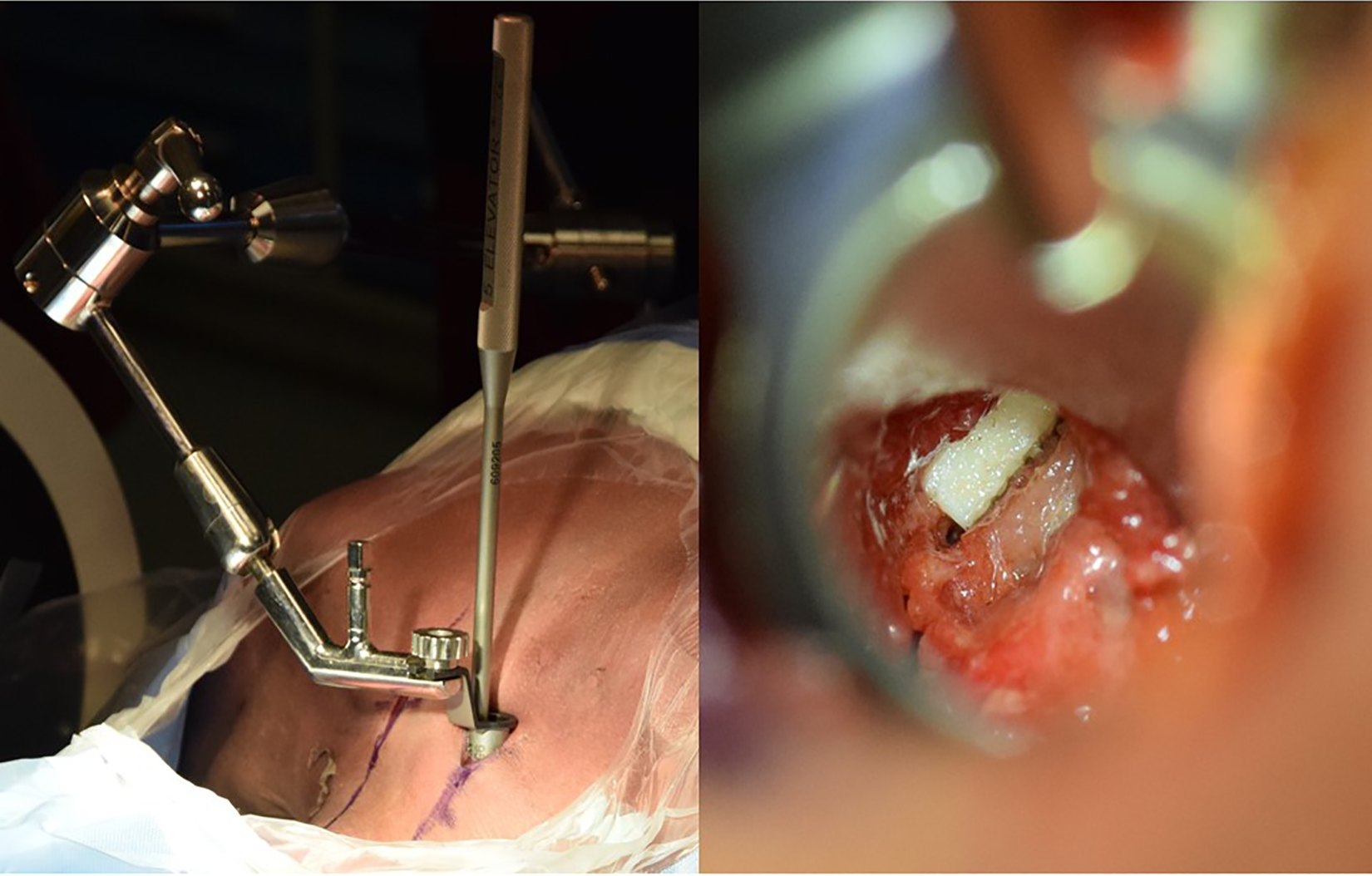
(Left) Single-level ACDF test setup on MTS machine. (Right) Posterior view with allograft spacers. White arrow points to spacer within facet joint.
Intact. The spines were tested intact for normative data.
Single-level ACDF. Nine cadavers (6 male and 3 female; average age 54) were used for the single-level test condition. All ACDFs were performed at C5-6. The anterior longitudinal ligament and anterior annulus were incised and a complete discectomy was performed. Caspar pins and an intervertebral distracter were used to distract the disc space. A high-speed burr was used to square the endplates. Appropriately sized polyetheretherketone (PEEK) spacers (Anatomic PEEK; Medtronic, Minneapolis, MN) were implanted. An anterior cervical plate (Medtronic RTG Spinal and Biologics; Medtronic, Minneapolis, MN) was secured across C5-6 using variable-angle screws (3.5 mm diameter, 14 mm length).
Single-level ACDF pseudarthrosis model. After condition 2 was tested, all 4 screws were loosened a quarter turn to simulate a nonunion condition.
Single-level ACDF pseudarthrosis model + posterior interfacet allograft spacers. After condition 3 was tested, the C5-6 lateral masses were exposed. The cartilage from each facet joint was removed using customized elevators and rasps (Medtronic, Minneapolis, MN). Machined 3 mm interfacet allograft spacers (Cornerstone Facet Micrografts; Medtronic, Minneapolis, MN) were tamped into the facet joints.
Two-level ACDF. Eight cadavers (4 male and 4 female; average age 47.5) were used for the 2-level test condition. The surgical technique for ACDF was repeated at both C4-5 and C5-6. Appropriately sized PEEK spacers (Anatomic PEEK; Medtronic, Minneapolis, MN) were implanted. An anterior cervical plate (Medtronic RTG Spinal and Biologics; Medtronic, Minneapolis, MN) was secured from C4-6 using variable-angle screws (3.5 mm diameter, 14 mm length).
Two-level ACDF pseudarthrosis model. After condition 5 was tested, all 6 screws were loosened a quarter turn to simulate a nonunion condition.
Two-level ACDF pseudarthrosis model + posterior interfacet allograft spacers. After condition 6 was tested, the C4-5 and C5-6 lateral masses were exposed. The surgical technique for the interfacet allograft spacer was repeated at both levels.
Data was assessed for normality and a repeated-measures analysis of variance (ANOVA) was used to evaluate differences in range of motion data and stiffness between the different test configurations (Minitab v16; Minitab Inc, State College, PA). A P value ≤.05 was considered significant.
Results
Single-Level Results
Compared to the intact condition, all fixation configurations resulted in statistically significant reductions (P ≤ .05) in C5-6 intersegmental range of motion in all 3 bending planes except for flexion-extension in the loose configuration (Figure 2). When normalized to the intact spine, the addition of interfacet allograft spacers (rescue condition) resulted in the greatest percent reduction, followed by the ACDF condition, followed by the loose condition. Performing ACDF with interbody graft and plate on the intact spine reduced FE, LB, and AR 60.0%, 64.9%, and 72.9%, respectively. Loosening the ACDF screws decreased these reductions to 40.9%, 44.6, and 52.1% in FE, LB and AR, respectively, compared with the intact spine. The addition of interfacet allograft spacers to the loose condition increased these reductions to 74.0%, 84.1%, and 82.1% in FE, LB and AR, respectively, compared with the intact spine. These differences were not statistically significant, although the lateral bending in the rescue condition compared with the loose condition approached significance (P = .08).
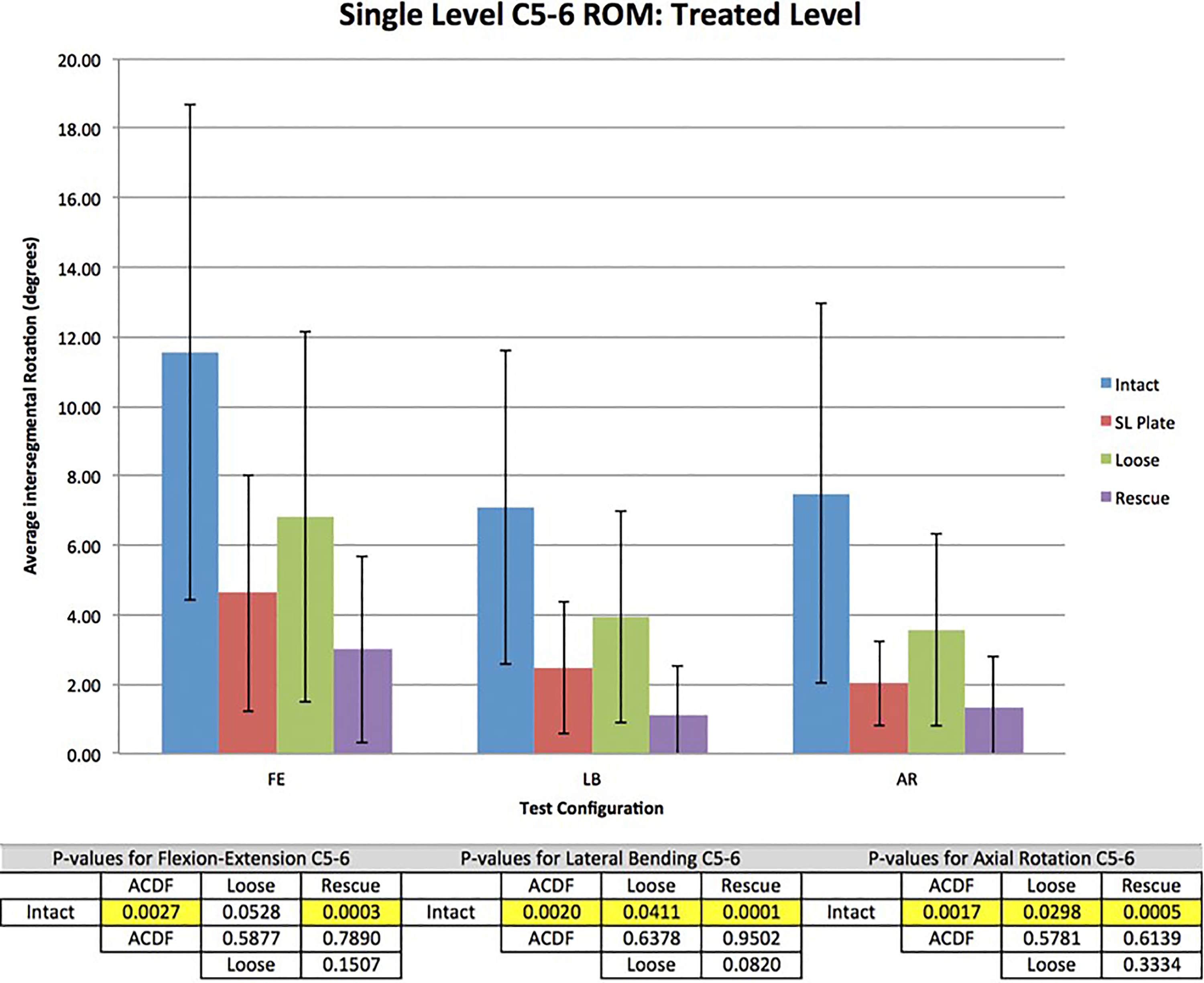
Total range of motion (ROM) in all test configurations at the treated level with associated P values. The order of range of motion from high to low was intact, loose, ACDF (anterior cervical discectomy and fusion), and rescue. Data are shown with 1 standard deviation error bars.
There were no significant differences in range of motion at C4-5 (adjacent unfused segment) between all testing configurations (Figure 3).
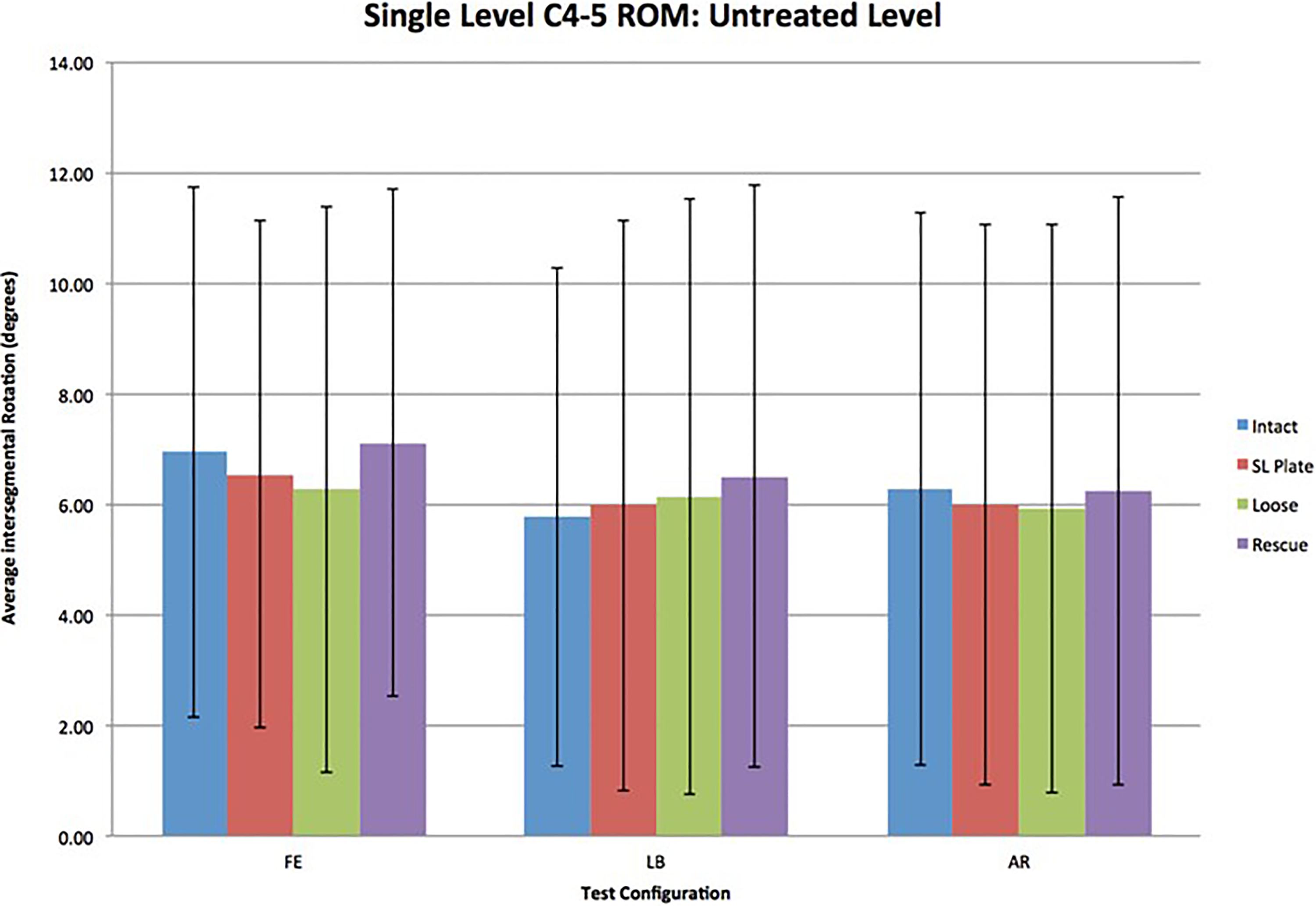
Total range of motion (ROM) in all test configurations at the untreated C4-5 level. Data are shown with 1 standard deviation error bars.
Two-Level Results
Combined C4-6 Range of Motion
Compared with the intact condition, all fixation configurations significantly reduced range of motion (P ≤ .05) in all 3 bending planes (Figure 4). When normalized to the intact spine, the addition of interfacet allograft spacers (rescue condition) resulted in the greatest percent reduction, followed by the ACDF condition, followed by the loose condition. Performing ACDF with interbody graft and plate on the intact spine reduced FE, LB, and AR 72.0%, 71.1%, and 71.2%, respectively. Loosening the ACDF screws decreased these reductions to 55.4%, 55.3%, and 51.3% in FE, LB, and AR, respectively, compared with the intact spine. The addition of interfacet allograft spacers to the loose condition increased these reductions to 82.6%, 91.2%, and 89.3%, in FE, LB, and AR, respectively, compared with the intact spine.
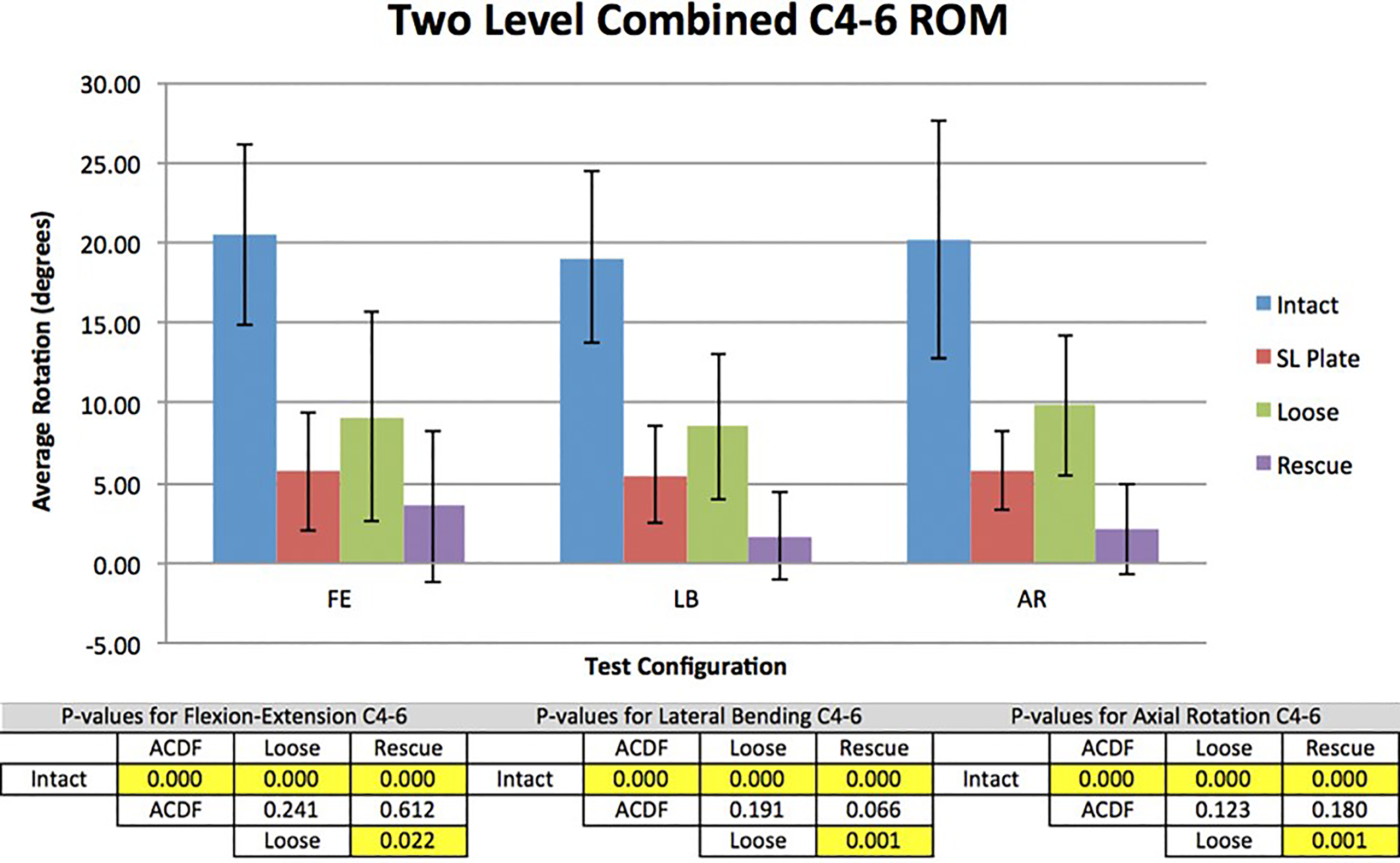
Total range of motion in all test configurations from C4-6 with associated P values. The order of range of motion (ROM) from high to low was intact, loose, ACDF (anterior cervical discectomy and fusion), and rescue. Data are shown with 1 standard deviation error bars.
The reduction in range of motion from the loose condition to the rescue condition was statistically significant (P ≤ .05). The differences between the ACDF and loose condition were not statistically significant. There were no statistically significant differences between the ACDF and rescue conditions although lateral bending approached significance (P = .07).
Intersegmental C4-5 Motion
Compared with the intact condition, all fixation configurations resulted in statistically significant reductions (P ≤ .05) in all 3 bending planes (Figure 5). The reduction in range of motion was again highest for the interfacet allograft spacers (rescue condition; 88.5%, 95.8%, and 95.2% in FE, LB, and AR, respectively), followed by the ACDF condition (83.3%, 75.1%, and 78.0% in FE, LB, and AR, respectively), followed by the loose condition (70.9%, 60.8%, and 60.5% in FE, LB, and AR, respectively). The reductions from the loose condition to the rescue condition were statistically significant (P ≤ .05).
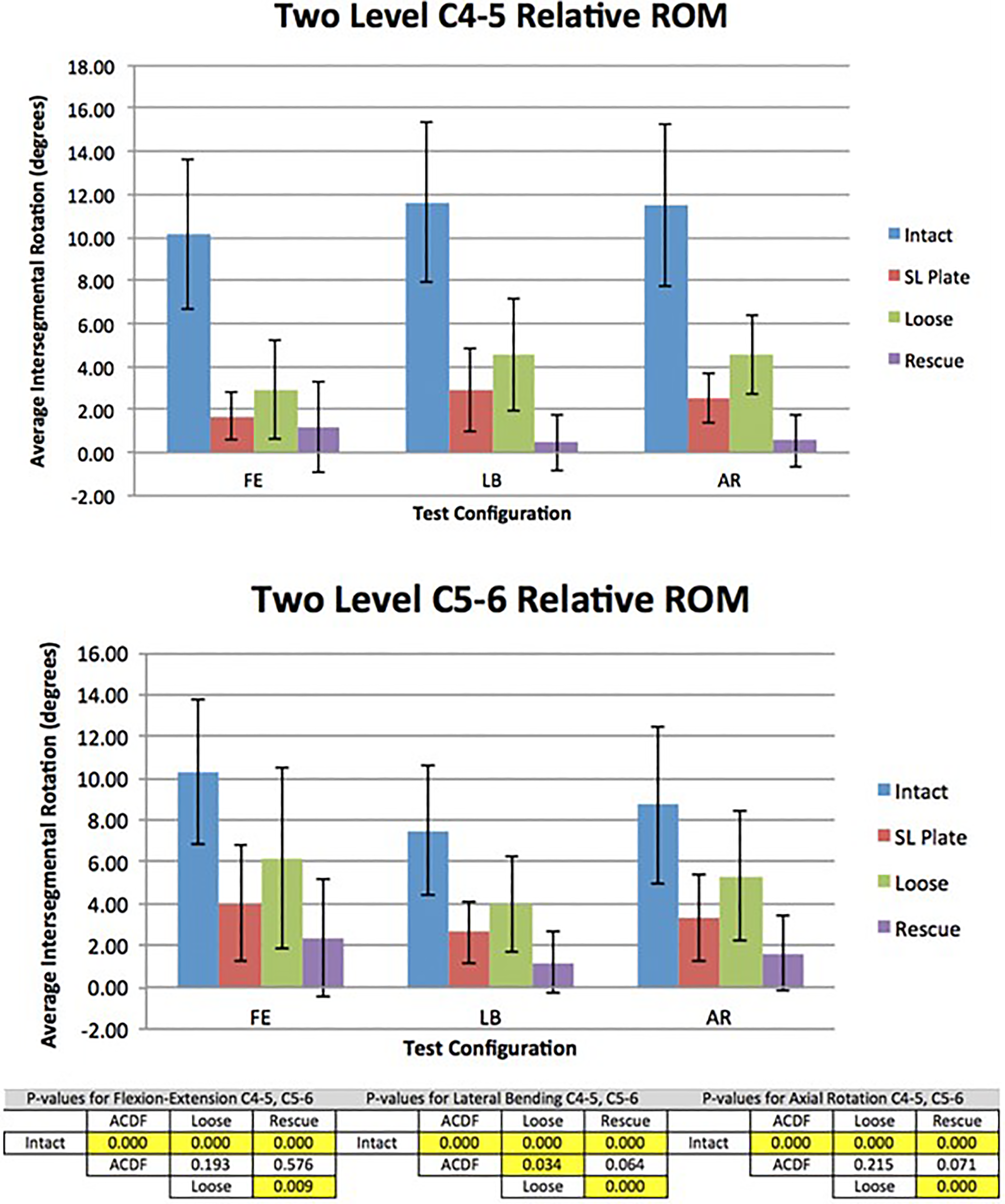
Intersegmental range of motion (ROM) in all test configurations at the treated C4-5 and C5-6 level with associated P values. The order of range of motion from high to low was intact, loose, ACDF (anterior cervical discectomy and fusion), and rescue. Data are shown with 1 standard deviation error bars.
Intersegmental C5-6 Motion
Compared with the intact condition, all fixation configurations resulted in statistically significant reductions (P ≤ .05) in all 3 bending planes (Figure 5). The reduction in range of motion was again highest for the interfacet allograft spacers (rescue condition; 76.8%, 84.0%, and 81.6% in FE, LB, and AR, respectively), followed by the ACDF condition (60.9%, 64.9%, and 62.3% in FE, LB, and AR, respectively), followed by the loose condition (40.0%, 46.7%, and 39.3% in FE, LB, and AR, respectively). The reductions from the loose condition to the rescue condition were statistically significant (P ≤ .05).
Discussion
Anterior cervical discectomy and fusion is a common procedure with a high clinical success rate. 2,22 -27 Pseudarthrosis remains an issue, particularly with multilevel fusions, 2 -8 and is a leading cause for postoperative pain and revision. 28 In the treatment of a symptomatic pseudarthrosis, the primary goal is to obtain additional stability and stiffness to increase the likelihood of achieving solid fusion. 29 Various supplemental fixation techniques have been developed with this reduction of motion in mind. Machined interfacet allograft spacers have previously demonstrated significant increases in foraminal height and construct stiffness when assessed in an intact cervical spine cadaveric specimen. 11 This study investigated whether the addition of interfacet allograft spacers could result in reduced intersegmental motion of the cervical spine in a 1-level and 2-level ACDF pseudarthrosis model.
Overall, our data show that 1-level and 2-level ACDF with interbody allograft and plate fixation significantly reduced motion compared with an intact cervical specimen. Systematic loosening of the ACDF screws was validated as a reasonable pseudarthrosis model, showing roughly 30% to 50% increased range of motion compared with the ACDF condition in all bending planes for both a 1-level and 2-level constructs. The addition of interfacet allograft spacers to the loose 1-level and 2-level ACDF conditions (pseudarthrosis model) resulted in significant gains in stability and ultimately resulted in a stiffer construct than the ACDF condition alone, although not statistically significant due to likely type II error. We did not test the range of motion of an intact ACDF construct with allograft spacers; however, for both 1-level and 2-level conditions, the ACDF pseudarthrosis model with interfacet allograft spacers (rescue condition) was the stiffest construct, demonstrating the effectiveness of this supplemental fixation method.
Kasliwal et al reviewed the clinical use of allograft facet spacers in addition to posterior fixation in the treatment of 19 patients with symptomatic pseudarthrosis. 17 Although lateral mass fixation was used in addition to the spacers, patients had significant improvement in clinical outcomes without significant change in alignment parameters. Our study gives biomechanical support to the possibility of standalone use of these spacers without additional posterior fixation in a pseudarthrosis case. As the minimally invasive placement of allograft spacers is feasible (Figure 6), this could translate to improved patient outcomes as the midline dissection necessary for lateral mass screw placement could be obviated.
(Left) Allograft spacer impactor through tubular retractor. (Right) View through 18 mm tubular retractor of facet with allograft spacer in place.
Other techniques of supplemental percutaneous fixation techniques have been studied. 30,31 The placement of facet screws have shown biomechanical and clinical promise, but placement above C5 may be limited due to occipital prominence. 10 Corollary issues may arise with placement of interfacet spacers at the lower cervical segments due to inadequate imaging and prominence of the shoulders. Further investigation is needed to determine the feasibility of minimal access placement at all cervical levels.
Previous studies have also addressed the hypothetical concern that these spacers may cause loss of lordosis or kyphosis. Goel and Shah reviewed 36 patients and did not demonstrate significant loss of lordosis. 13 Tan et al reviewed 64 patients whose treatment included interfacet allograft spacers and did not find a significant difference between preoperative and postoperative cervical lordotic angle. 32 While we did not investigate this in our study, this should certainly be an area of continued future research.
The limitations of this study are the same for any ex vivo analysis and can only represent the immediate postoperative condition. Additional limitations include the infeasibility of testing more than the 3 primary rotational planes. We did not assess the effect of compressive load or cyclic loading on the various constructs. Furthermore, we did not biomechanically compare the interfacet allograft spacers to standard posterior lateral mass or pedicle screws commonly used in the treatment of ACDF pseudarthrosis. Last, although our results demonstrated notable difference in range of motion among the various constructs, we were likely underpowered to demonstrate a significant difference between all construct comparisons during 1-level testing and comparison of the ACDF construct to the loose or rescue conditions in 2-level testing.
Potential clinical limitations of the interfacet allograft spacer include the induction of kyphosis as the spacers sit posterior to the sagittal axis of rotation in the cervical spine. Previous studies have excluded patients with kyphotic alignment when assessing the clinical results of similar devices. 31 Currently, the authors of this study would recommend utilization of the interfacet allograft spacers in patients undergoing anterior fusion at risk for pseudoarthrosis. Additional potential applications include in patients undergoing tumor resection as the spacers may enhance imaging characteristics due to less metal artifact. Last, the spacers could be used to augment traditional posterior cervical fusion in patients without robust screw purchase whereby the spacers may improve structural stability along with lateral mass or pedicle screws.
Our data demonstrated that supplementation of an ACDF pseudarthrosis model with interfacet allograft spacers significantly increases stability and has potential applications in treating cervical pseudarthrosis. Interfacet allograft spacers may also be used as adjunctive fixation in cases with high nonunion risk such as multilevel anterior interbody fusions, degenerative spondylolisthesis, and tumor resection, but further biomechanical and clinical studies are still needed to assess the application of this technique in these settings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by a research grant from Medtronic.