
Abstract
Study design:
Invited narrative review.
Objectives:
The aim of this review was to summarize current literature regarding risk factors that surgeons can optimize in the preoperative setting in the spinal surgery patient, in order to reduce complications and improve patient-reported outcomes.
Methods:
Review of the relevant literature by the authors.
Results:
Modifiable risk factors identified relative to the patient include obesity, malnutrition/nutrient deficiency, diabetes/hyperglycemia, preoperative anemia, vitamin D/DEXA (dual-energy radiograph absorptiometry), nicotine use/smoking, and opioid use/psychosocial factors.
Conclusion:
By maximizing a patient’s physiological and psychological status prior to elective spine surgery, we may move closer to achieving the goals of value-based care: improving patient-reported outcomes while decreasing the cost of care.
Keywords
Introduction
In recent years, the cost and utilization of spine care both nonoperatively as well as operatively has increased significantly without documented evidence of improvement in outcomes. 1,2 There has been a push recently to shift to a model of value-based care, with the goal of achieving the highest quality of care for the least cost rather than simply cutting cost or improving quality alone. This trend has led to a multidisciplinary approach in the management of spine patients undergoing elective surgery. Additionally, with the change in going from the fee-for-service compensation model to one of bundled payments for surgical intervention, there is greater pressure on physicians to lower overall treatment costs. Optimizing patients preoperatively may lead to improved outcomes and treatment cost reductions. 3,4
This section will examine the recent literature to provide insight into ways that spine surgeons can optimize surgical patients in the preoperative setting in an attempt to reduce complications and ideally improve patient-reported outcomes.
There has been a significant amount of research examining the use of local and systemic measures to reduce surgical site infections in spine surgery, including examining procedure-specific and patient-specific factors. 5 -8 The use of preoperative methicillin-resistant Staphylococcus aureus screening, bathing protocols, wound lavage, and intraoperative vancomycin powder will be discussed in a subsequent section. Modifiable risk factors relative to the patient, including obesity, malnutrition/nutrient deficiency, diabetes/hyperglycemia, preoperative anemia, vitamin D/DEXA (dual-energy radiograph absorptiometry), nicotine use/smoking, and opioid use/psychosocial factors will be discussed below.
Obesity
The obese represent a challenging patient population to spine surgeons. In addition to the myriad medical comorbidities associated with obesity, such as diabetes, coronary heart disease, and pulmonary disease, obesity in of itself has been shown to be an independent risk factor for complications associated with spine surgery. 9 -12 For example, in the Spine Patient Outcomes Research Trial (SPORT), 9 the 4-year follow-up data demonstrated a high complication profile for obese patients (infection and revision rates, as compared to nonobese patients) though similar improvements in patient-reported outcomes in the surgical group were reported. McGuire et al 12 in a subgroup analysis of the 4-year SPORT data for obese patients, particularly those with BMI >35 kg/m2 (Class II and Class III obesity), reported worse outcomes in complications, operative time, and baseline patient-reported outcomes particularly in the degenerative spondylolisthesis group. 12 However, Rihn et al 13 demonstrated in a subgroup analysis of obese (BMI >30 kg/m2) versus nonobese (BMI < 30 kg/m2) undergoing treatment of lumbar disc herniation that there was no significant differences in the surgical complication profile between the 2 groups.
When looking solely at patient-reported outcomes based on the McGuire et al 12 and Rihn et al 13 studies, there is evidence to suggest that obese patients do find benefit with surgical interventions despite overall increase in surgical complication profile between nonfusion and fusion operations. These studies as well as others highlight a complication profile that warrants appropriate screening and counseling. 14,15
Because obesity is a modifiable risk factor, enrolling patients in a nonsurgical weight loss plan could address this complex complication profile. Roffey et al 16 in a prospective cohort study with 46 obese individuals employed a 52-week medically supervised, multidisciplinary, nonsurgical weight loss program that demonstrated improvements and trends toward significance in pain scale scores as well as Oswestry Disability Index (ODI) scores for low back pain and disability. Although there was no control group, this study highlights that a nonsurgical weight loss program may have a role in improving functional outcomes for spine patients. There are a few studies that have examined the role of surgical weight loss and its effect on minimizing complications in patients undergoing spine surgery. 10,14,17 However, a recent retrospective cohort study by Jensen et al, 10 which looked at reported outcomes of cervical and lumbar surgery, demonstrated that patients who had undergone bariatric surgery had worse reported outcomes and satisfaction following lumbar surgery than their counterparts. We have a paucity of data to guide us regarding nonsurgical or surgical weight loss, and further studies are necessary to suggest one intervention over the other. The focus must be placed on minimizing the associated medical risk factors associated with obesity and focus on potential nonsurgical weight loss to improve outcomes in the perioperative setting.
Malnutrition/Nutrient Deficiency
In the orthopedic and neurosurgery literature, we have interchangeably used serological markers such as albumin, pre-albumin, transferrin, and total lymphocyte count to define malnutrition. Albumin levels <3.5 g/dL, serum total lymphocyte count <1500 cells per cubic millimeter, low pre-albumin levels, and/or transferrin levels <200 mg/dL have been shown to be signs of malnutrition and have been harbingers of increased complications such as wound healing and surgical site infections. 11,18 -22 Kudo et al 23 in a retrospective analysis of over 100 patients examined the effect of the rapid turnover proteins (pre-albumin and transferrin) and the ability to predict surgical site infections. In this study, pre-albumin, transferrin, and albumin levels alone did not demonstrate statistical significance in predicting surgical site infection using multivariate analysis. However, in their univariate analysis there was statistical significance reached for those variables suggesting a possible role in predicting surgical site infections.
The most widely used markers in the literature appear to be serum albumin and total lymphocyte count as markers of malnutrition, and subsequently, these markers have been utilized to screen patients who are at risk for perioperative complications. 24 -27
If patients undergoing elective spine surgery have laboratory or serum markers that fall below normal values or below the thresholds outlined above, then a nutritional consult is warranted. In the setting of elective spine surgery, nutritional deficiencies may be addressed preoperatively to reduce the overall complication profile and potentially minimize risk of surgical site infections. In trauma or oncologic cases, these markers can be utilized to predict which individuals may be at higher risk of surgical site infections.
Diabetes/Hyperglycemia
Similar to obesity, diabetes and hyperglycemia have been shown to be independent risk factors for increased surgical complications. 28 -30 It is believed that diabetes and/or hyperglycemia causes impaired oxygen delivery via the glycosylation of hemoglobin, which leads to the downstream effect of tissue ischemia. The disruption of glucose utilization has been shown to increase the risk of surgical site infections in orthopedic surgery. 31,32 As in obesity, individuals with diabetes are more likely to have additional medical comorbidities that affect surgical outcomes. 28,33 -35 In addition to increased complication profile for diabetic patients, studies have suggested increased cost associated with the perioperative management of diabetic patients. Underwood et al, 36 using National Surgical Quality Improvement Program (NSQIP) database as well as patient registry data determined that preoperative A1C above 8% demonstrated increased length of stays and complications. Walid et al 37 -39 have demonstrated in several papers the increased cost associated with diabetes and other comorbidities across patients undergoing spine surgery and has advocated for the use of glycated hemoglobin (A1C) as screening tool.
Perioperative hyperglycemia has been noted to have an additive effect on patients undergoing the stress of surgery. Modulation of the stress response, specifically the hypothalamic-pituitary-adrenal axis as well as sympathetic nervous system, are often disrupted in the setting of diabetes or hyperglycemia as shown in critically ill patients. 40 -42 In the orthopedic literature it has been established that diabetes increases the complication profile for those undergoing elective total joint arthroplasty. 43,44
Careful coordination and appropriate cardiovascular risk stratification in patients with diabetes is also warranted. The Clinical Guidelines Committee from the American College of Physicians has recommended an insulin infusion to maintain glucose levels <200 mg/dL with a maintenance goal in the range of 140 to 180 mg/dL for critically ill patients. 45 However, in the perioperative period, patients with relatively well-controlled blood sugars can be transitioned or managed with subcutaneous or supplemental insulin therapy (ie, insulin sliding scale) to maintain blood sugars in the 140 to 200 mg/dL range particularly if they are being transitioned to enteral nutrition and receiving appropriate intravenous fluids (often dextrose solution, 5%, with either normal or half normal saline). The utilization of an insulin sliding scale is a corrective method of treating hyperglycemia and can lead to continued variability in point of care blood sugars. The initiation of proactive measures such as placement on basal or bolus insulin may be more effective in the management of inpatient hyperglycemia. 46
Appropriate preoperative screening with A1C and maintaining tight hyperglycemic control in the perioperative setting can effectively minimize complications and ultimately costs for elective spine procedures.
Anemia
It has been well established that preoperative anemia, defined as hematocrit <38%, or hemoglobin less than 12 g/dL (<13 g/dL for men), has been associated with increased rates of transfusion and perioperative morbidity and mortality 47 -53 during various non-cardiac procedures. Seicean et al, 47 using the American College of Surgeons NSQIP database, demonstrated that those individuals with anemia, regardless of the severity, had increased lengths of stay during their hospitalization and were more likely to experience complications and 30-day mortality compared to propensity-matched patients without anemia.
Guinn et al 54 implemented an anemia screening and treatment pathway for patients undergoing elective joint arthroplasty. In their study, patients who were indicated for surgery and found to be anemic using a point-of-care hemoglobin analyzer were placed in a pathway to manage their anemia. This pathway included obtaining labs to identify sources of anemia and included a complete blood cell count, basic metabolic panel, iron studies (ferritin, iron, iron saturation, total iron binding capacity, and reticulocyte count), B12 level, and folate. Depending on the results of the labs, patients had planned surgeries delayed in order to obtain appropriate medical referrals and to initiate treatment of anemia prior to scheduled surgery. Interventions included either IV iron infusions or PO iron supplementation or use of erythropoietin. 54 The results of this study identified 25 at-risk patients for anemia of which only one patient required perioperative transfusion. Blood management goals for patients undergoing surgery should include minimizing blood loss intraoperatively, as well as screening for and treating anemia to increase red blood cell mass. The effective screening of and treatment of perioperative anemia can lead to decreased lengths of stay and potentially transfusion avoidance, which can lower morbidity and mortality in the long run.
Vitamin D/DEXA:
With the increasing prevalence of osteoporosis in our aging population, there remains concern for bone-implant failures in patients undergoing elective spinal fusion procedures. Vitamin D is a fat-soluble steroid that facilitates the absorption of dietary calcium and phosphate. Typically, vitamin D insufficiency or deficiency stems from lack of exposure to sunlight or abnormal intestinal absorption. Screening for and treating vitamin D deficiency entails obtaining serum 25-hydroxyvitamin D (25OHD) and supplementing as necessary. Typically, this involves 50 000 IU of vitamin D orally weekly for upwards of 8 weeks. 55 In a meta-analysis, Bischoff-Ferrari et al 56 demonstrated a reduction in pooled fracture risk with 800 IU of vitamin D daily. The addition of 1200 mg of calcium to the 800 IU of vitamin D was also shown to reduce fracture risk, particularly those over 50 years of age. 57
In a review of over 300 patients undergoing spinal fusion that were screened for vitamin D levels, 27% were found to be deficient. The vitamin D–deficient patients were more likely to be obese and report greater disability on their outcomes. 58 In another study, patients with vitamin D deficiency (serum 25 OH levels < 20 ng/mL) undergoing elective spine surgery were found on multivariate analysis to have a higher risk of nonunion (odds ratio 3.449). 59
When deciding on screening for osteoporosis, the DEXA scan is the standard used by the World Health Organization. Osteoporosis is defined by a T score of <−2.5, or greater than 2.5 standard deviations below, optimal bone mineral density. A DEXA scan, in addition to other patient-specific factors, can be used to estimate an individual’s 10-year probability risk of major fracture by using a computer-based algorithm (ie, FRAX score). 60 Osteoporosis of the spine can pose a challenge for the spine surgeon when considering instrumentation. Although animal studies have demonstrated that treatment of osteoporosis with anti-resorptive drugs (bisphosphonates) or with anabolic agents such as teriparatide have improved radiographic signs of fusion, clinical trials have not shown clinically significant reduction in complications or patient-reported outcomes. 61 Regardless, it remains important for the practicing spine surgeon to ensure that elective fusion/instrumentation patients have been screened appropriately to prevent possible failures due to poor bone-implant characteristics. 62 Bjerke et al 63 demonstrated, in a retrospective cohort of 140 patients undergoing thoracolumbar fusion, increased osteoporosis-related complications (ie, failure of instrumentation, proximal junctional kyphosis/failure, and pseudarthrosis) in individuals with osteopenia and osteoporosis compared to those with normal bone density. The authors inferred increased risk of failure or poor outcomes T scores <−1.0.
Patients with a T score of <−2.5 should be approached cautiously when instrumentation is being considered, especially in multilevel fusion constructs. We recommend supplementing with vitamin D and calcium as well as using an anabolic agent such as teriparatide for 3 months preoperatively and continuing for 1 to 2 years postoperatively to limit the potential for complications in this subgroup of patients.
Nicotine
The deleterious effects of smoking are well established by not only the World Health Organization but the American Cancer Society as well. Smoking negatively affects soft tissue perfusion, wound healing, spinal fusion, and the ability of our immune system to fight pathogens. 64 -69
Screening for smoking history is the first step in helping improve patient outcomes. Once a patient has been identified as an active smoker, implementing a successful cessation pathway can be challenging. Nicotine replacement therapy (either with transdermal patches or chewing gums), self-help, and counseling have been utilized to improve the success rate of individuals wishing to quit. 70 Frequent counseling by health care providers as part of a smoking cessation program has also been shown to be clinically effective and can provide an opportunity for the surgeon to intervene. 71 Unfortunately, these resources may be scarce in the underinsured or Medicaid populations. Nonetheless, it is imperative to have a frank discussion with patients regarding the risks of continued cigarette smoking and its associated complications pertaining to spine surgery. 72 -74 Studies have not only demonstrated the increased risk of perioperative complications of smoking and/or nicotine use, but even more significant is how smoking can effect functional outcomes and patient-reported outcomes. 68,75,76 For example, Pearson et al 76 utilizing a subgroup analysis of the SPORT data demonstrated that smokers undergoing decompressive intervention without fusion had no statistical clinical difference in outcomes compared to the nonoperative treatment cohorts. This implies that smoking cessation may lead to improved patient-reported outcomes.
As far as determining duration of cessation and effects on patient-reported outcomes, there are no prospective studies demonstrating the ideal time for cessation or duration of cessation during the perioperative period. Glassman et al, 68 in a retrospective study of 357 patients, demonstrated that there were no differences between postoperative satisfaction scores and the length of preoperative smoking cessation; however, in patients who were able to remain compliant with smoking cessation in the postoperative period there was a trend toward improved patient satisfaction despite no statistical significance.
Every attempt should be made by the spine surgeon to counsel their patients on the perioperative complications and provide the resources/referrals necessary to begin smoking cessation at least a month prior to elective surgery, knowing full well that continuing to provide support for smoking cessation postoperatively may need to extend well past 3 months postoperatively not only for surgery-related outcomes, perhaps just as important regarding patient-reported outcomes.
Opioids and Psychosocial Factors
Spine surgery is physically and psychologically stressful for patients. The ability of patients to cope with these demands varies. 77,78 Often, our patients have a history of depression and/or anxiety and are taking psychoactive medications. Moreover, these individuals often have a long history of opioid use. Such patients require a diligent review for factors affecting their perioperative risks. Hu et al 79 describes utilizing a clinical pharmacist for adult spinal deformity patients in the preoperative setting to ensure that the appropriate medications are held preoperatively, and that the appropriate IV morphine equivalents are utilized postoperatively, to minimize the risks of additive side effects from poly-pharmacy.
Patients undergoing elective spine surgery have been shown to be at increased risk of opioid dependence. 80 Despite the rise in consumption of opioids in the management of pain, their use has not been substantiated in improving patient-reported outcomes particularly after spine surgery. 81 Hills et al 81 reported 1-year outcome data on over 2100 patients undergoing spine surgery, of which 21% of their cohort were on chronic opioid therapy. This subset of patients had higher adjusted odds ratios of continued pain, 90-day complications, and continued postoperative opioid use. More troubling is that opioid abuse and dependence places our patients at increased risk for all-cause morbidity as well as inpatient mortality. 80
Understanding risk factors and the complication profile of opioid use in our patients is paramount to implementing a pathway to improve not only perioperative surgical outcomes but patient-reported outcomes as well. Studies have demonstrated that opioid use within 6 months of surgery persists in the postoperative period, and the utilization of resources adds continued cost to our medical system. 82,83 Higher opioid use, as measured using morphine equivalents, is associated with increased hospital length of stay as well as significantly worse patient-reported outcomes following spine surgery. 84,85 Patients taking larger doses of opioids, greater than 10 mg of morphine equivalents per day, should be cautiously approached when recommending surgery. Involving Pain Management practitioners to assist with patient-specific regimens and reducing morphine equivalents prior to surgery may have benefit.
Mental health plays a significant role in the perception of pain and functional outcomes; moreover, it has been shown that depression and/or anxiety are closely associated with preoperative opioid or chronic opioid use. 84 -89 It is imperative as a surgeon to ensure that patients understand the expectation of minimizing chronic opioid use in the perioperative period, which may be accomplished with the assistance of a pain management physician who can set expectations for postoperative opioid consumption. A significant number of patients presenting to spinal surgeons have psychological disorders that may affect their outcomes. Surgeons’ ability to detect mental health issues alone is variable. 90 -92 A routine psychological screening questionnaire may be helpful in detecting patients that may need counseling prior to surgical intervention. 93,94 Miller et al 95 utilized the Patient Health Questionnaire–9 (PHQ-9) in over 900 patients undergoing various lumbar procedures and determined that the higher the PHQ-9 score (increased likelihood of depressive disorder), the more likely the minimally clinically important difference for EuroQoL-5D (EQ-5D) would not be met (odds ratio of 0.93). Merrill et al 96 was able to utilize patient-reported outcome measures (PROMIS physical function, pain, physical function, and ODI) in a retrospective cohort for 55 patients undergoing decompression alone and noted the depressed cohort (PROMIS depression score >50) had worse postoperative PROMIS physical function, pain, and ODI scores. In other words, patients who were depressed did have significant improvement following surgical intervention, and although these individuals had a greater magnitude of improvement compared to the nondepressed cohort, they overall had worse physical function, pain, and ODI scores at 6 months than those who were not depressed.
Appropriate recognition and screening of our patients for opioids and depression can ultimately improve patient-reported outcomes. Working closely with our mental health and pain management colleagues can also help facilitate improved functional outcomes in this challenging patient population.
Conclusion
Optimizing patient outcomes in patients undergoing spinal surgery requires an awareness of the multitude of preoperative factors that have been shown to affect our patients’ health and their ability to heal and recover from spinal surgery (Table 1). Reducing predictable complications through appropriate patient screening preoperatively can improve surgical as well as patient-reported outcomes. Providing our patients with the best surgical and functional outcomes involves an integrated multidisciplinary practice. By maximizing a patient’s physiological and psychological status prior to elective spine surgery, we may move closer to achieving the goals of value-based care: improving patient-reported outcomes while decreasing the cost of care through perioperative risk reduction.
Patient-Specific Factors for Minimizing Complications in Spine Surgery.
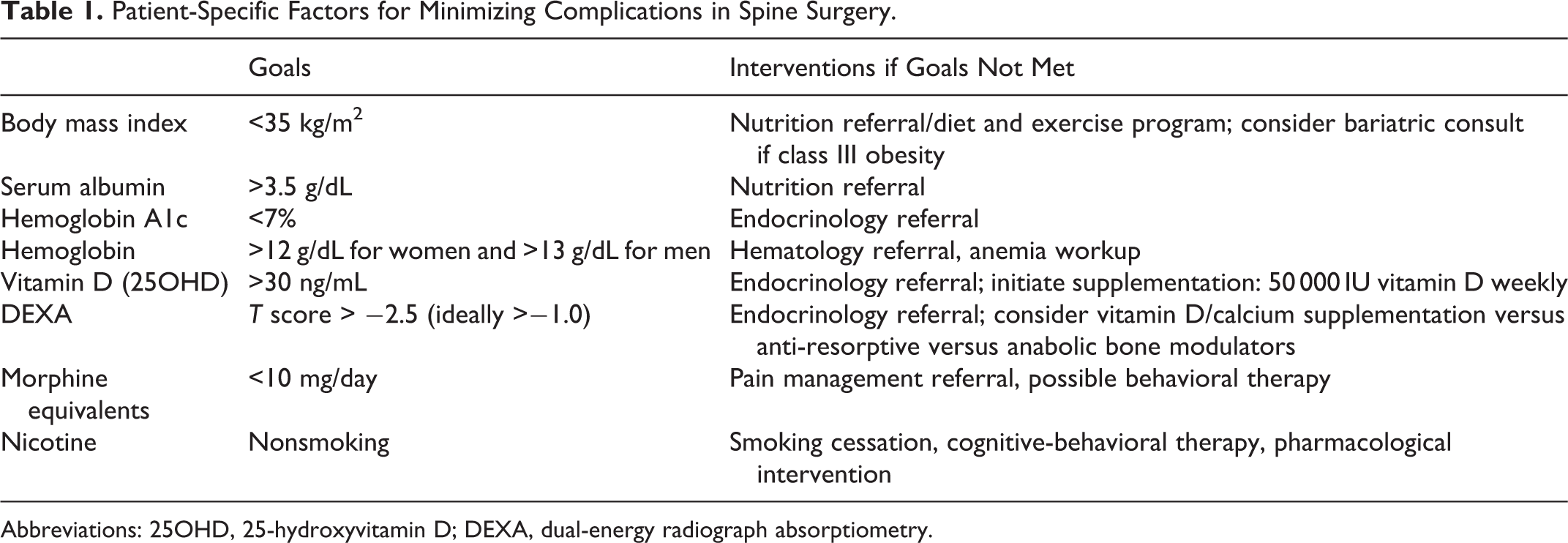
Abbreviations: 25OHD, 25-hydroxyvitamin D; DEXA, dual-energy radiograph absorptiometry.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This supplement was supported by funding from AO Spine North America.