
Abstract
Study Design:
Systemic review and meta-analysis.
Objectives:
Several studies have reported the impact of accidental dural tears (DT) on the outcome of spinal surgery, some with conflicting results. Therefore, the aim of this study was to carry out a systemic review and meta-analysis of the literature to establish the overall clinical outcome of spinal surgery following accidental DT.
Method:
A systemic literature search was carried out. Postoperative improvement in Oswestry Disability Index (ODI), Short-Form 36 survey (SF36), leg pain visual analogue scale (VAS), and back pain VAS were compared between patients with and without DT at different time intervals.
Results:
Eleven studies were included in this meta-analysis. There was a slightly better improvement in ODI and leg VAS score (standardized mean difference of −0.06, 95% confidence interval [CI] −0.12 to −0.01, and −0.06, 95% CI −0.09 to −0.02, respectively) in patients without DT at 12 months postsurgery, but this effect was not demonstrated at any other time intervals up to 4 years. There were no differences in the overall SF36 (function) score at any time interval or back pain VAS at 12 months.
Conclusion:
Based on this study, accidental DT did not have an overall significant adverse impact on the short-term clinical outcome of spinal surgery. More studies are needed to address the long-term impact and other outcome measures including other immediate complications of DT.
Keywords
Introduction
Accidental dural tears (DT) are a recognized complication of spinal surgery. They have been associated with other perioperative complications and with a relatively higher rate of neurological deficit. 1,2 The reported incidence has significantly varied in the literature, 3 and several risk factors have been associated with DT. 4 A variety of management protocols and repair techniques are described in the literature, 5,6 with more emphasis on achieving watertight repair whenever feasible.
Several studies have already addressed the short-term and long-term outcomes in patients who suffered DT but these have been marred with inconsistencies. 6,7 Saxler et al reported relatively worse outcome at a mean follow-up of 10 years following DT during lumbar discectomies. Patients had persistent leg pain and a high proportion of patients were not able to return to their previous occupations. 7 Wang et al, however, reported no adverse outcome in association with DT and reported similar results to a matched cohort of patients with no DT. 6 Since then, there have been several publications specifically addressing the clinical outcome of incidental DT using validated patient-reported clinical outcome scores. Many of these studies did not demonstrate any differences in the clinical outcome between patients with and without DT. 3,8 -10
We are not aware of any studies that systemically reviewed and analyzed the overall impact of accidental DT on the function and clinical outcome of patients following spinal surgery. Therefore, the aim of this study was to conduct a systematic review of the literature and carryout a meta-analysis of the outcome results to establish if there is an overall adverse effect of accidental DT on the overall outcome of spinal surgery. We focused on validated patient-reported outcome scores such as ODI (Oswestry Disability Index), SF36 (Short-Form 36 survey, function), and leg pain and back pain VAS (visual analogue scale scores).
Methods
A systemic literature search was conducted as part of a wider project looking at the treatment and outcome of accidental DT. Four databases (PubMed, Medline, Embase, and Cochrane) were initially searched from their inception until the end of January 2019. The following Mesh and text terms were used: dural tear, dural leak, dural injury, dural laceration, incidental durotomy, incidental dural tear, incidental dural leak, incidental dural injury, incidental dural laceration, accidental dural leak, accidental durotomy, accidental dural tear, accidental dural injury, accidental dural laceration, iatrogenic dural tear, iatrogenic dural leak, iatrogenic durotomy, iatrogenic dural Injury, iatrogenic dural laceration. The Boolean operators (“AND,” “OR”) were used to refine the search between the terms.
The search and articles selection was carried out according to PRISMA flowchart as outlined in Figure 1. Any article relating to DT in spinal surgery was initially selected for review for eligibility. The final selection and inclusion of the articles into the meta-analysis was conducted according to the following criteria:
Studies must be on accidental (incidental, iatrogenic or unintended) DT in elective spinal surgery. Studies on trauma or intended durotomies were excluded. Must compare at least one postoperative validated function outcome score to baseline (preoperative) score between patients with and without DT. Studies that do not report baseline (preoperative) scores were excluded. Any validated patient-reported outcome score was considered, such as ODI, SF36, and so on. Studies reporting nonvalidated patient outcome scores were not included. All study types were eligible for inclusion including case control, cohort, or randomized control trials. Case series with no comparative group (ie, no DT) were excluded.
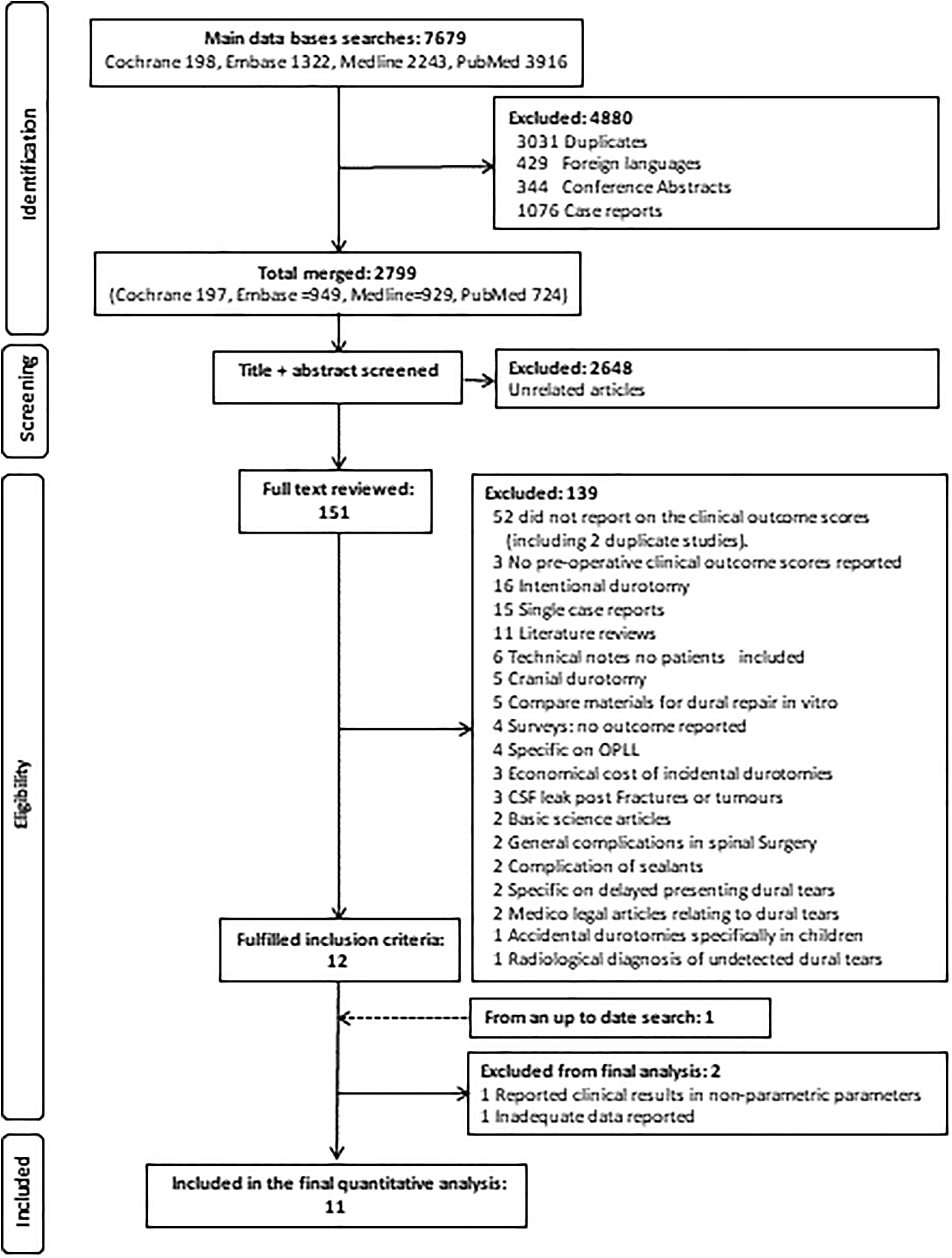
PRISMA flow chart demonstrating the selection process of the studies with clinical outcome scores.
A further up-to-date literature search covering the period from February to September 2019 revealed one recently published study that assessed clinical outcome at 12 months postsurgery. 11
Assessment of the Studies
There were no restrictions on the type of articles selected as long as they fulfilled the aforementioned eligibility criteria. The Newcastle-Ottawa Quality Assessment Scale (NOQAS) and the Methodological Index for Non-Randomized Studies (MINORS) 12 were both independently used by 2 authors to assess the quality of reporting. Differences in scores awarded by each author were discussed and a final score agreed.
Data Extraction
Functional scores were commonly assessed in the form of ODI, SF36, and JOA (Japanese Orthopaedic Association scale). Hence, parametric parameters (mean, standard deviation [SD], standard error [SE], and confidence interval [CI]) were extracted for patients with and without DT at baseline and at different postoperative time intervals. For each group, the improvement in score at different postoperative time intervals (relative to baseline) was calculated. This was then used in the meta-analysis calculations and comparisons as per Figure 2.
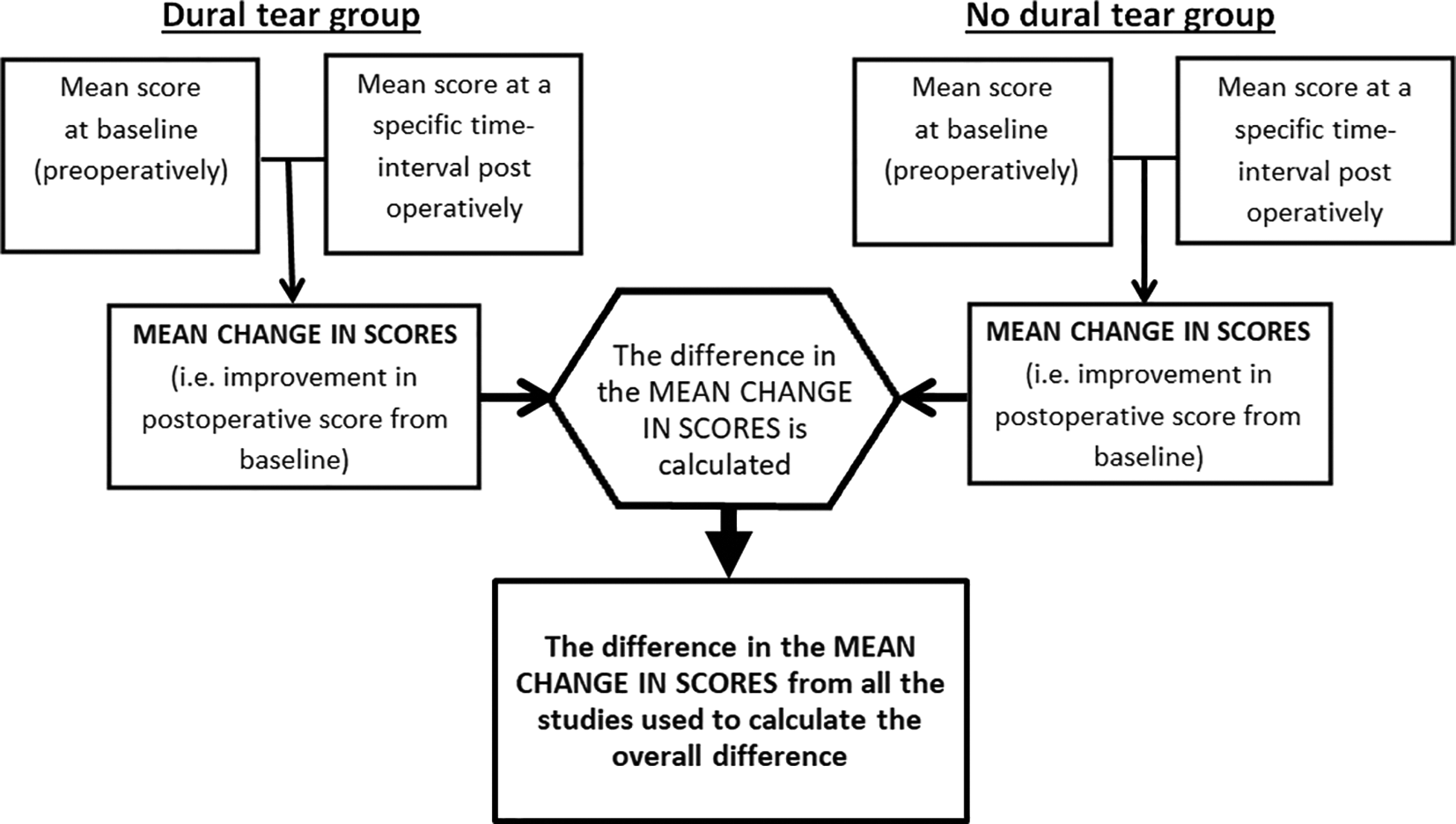
How the 2 groups’ outcome scores were compared in the meta-analysis for each time interval. For each study and for each time interval, the reported mean score at baseline and at the respective postoperative time interval were initially compared to yield the mean change in score for each group (dural tear and no dural tear groups). This mean change of score was then directly compared (between the dural group and nondural group) for that specific time interval for each study. Then this differences in the mean change in scores from all the studies (for that specific time interval) were entered into the meta-analysis to calculate the overall difference.
Data Synthesis
The mean change in the improvement of functional scores between the 2 groups (DT and no DT) was compared in the meta-analysis (Figure 2). The overall pooled, standardized mean difference (SMD) was calculated using the inverse variance and the fixed-effect model. The SMD was chosen because some studies used different functional scores and some presented their results in terms of percentage improvement rather than the actual absolute improvement in scores. Heterogeneity and publication bias were assessed using funnel plots. All the analyses were conducted using the Review Manager 5.3 software (Cochrane collaboration).
Results
Initially, 13 studies 3,8 -11,13 -20 fulfilled the inclusion criteria and all (except one) were case-control studies. Three studies were nested case-control studies from randomized control studies, 3,8,9 and these reported the outcome scores up to 4 years. None of the studies reported the long-term outcome (10 years or more). The studies’ description and their quality of reporting as assessed by NOQAS and MINORS are presented in Table 1.
Description of the Studies Included in the Final Quantitative Analysis With the Number of DT Cases at the First Respective Follow-up and the Total Duration of Follow-up for Each Studya.
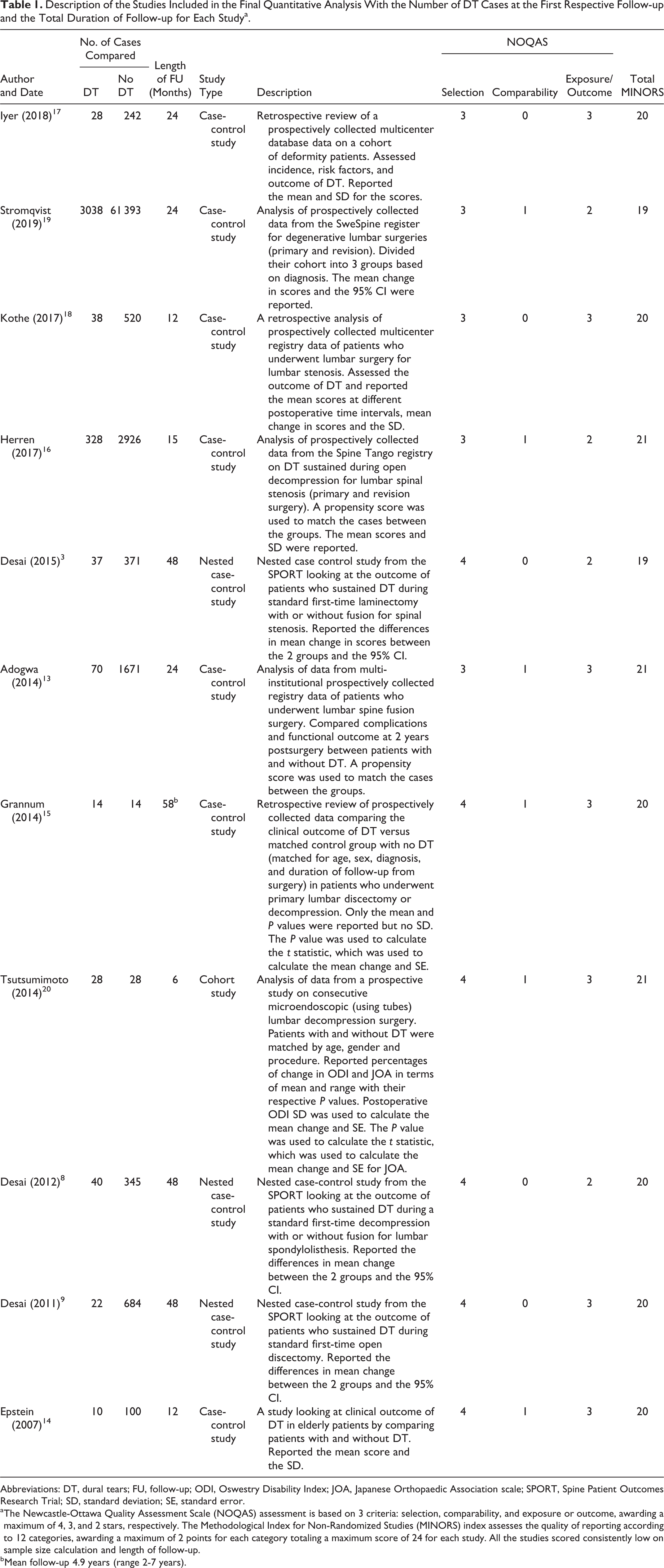
Abbreviations: DT, dural tears; FU, follow-up; ODI, Oswestry Disability Index; JOA, Japanese Orthopaedic Association scale; SPORT, Spine Patient Outcomes Research Trial; SD, standard deviation; SE, standard error.
a The Newcastle-Ottawa Quality Assessment Scale (NOQAS) assessment is based on 3 criteria: selection, comparability, and exposure or outcome, awarding a maximum of 4, 3, and 2 stars, respectively. The Methodological Index for Non-Randomized Studies (MINORS) index assesses the quality of reporting according to 12 categories, awarding a maximum of 2 points for each category totaling a maximum score of 24 for each study. All the studies scored consistently low on sample size calculation and length of follow-up.
b Mean follow-up 4.9 years (range 2-7 years).
Extraction of Data
Eleven of the studies 3,8,9,13 -20 reported the mean or the mean difference of the outcome scores at different intervals postoperatively. The 12th study 10 reported its results in the form of median and interquartile range (IQR). The corresponding author did not respond to our request to supply us with the parametric data format of the results, and hence their study was excluded from this meta-analysis. The 13th study’s data 11 was not sufficiently reported and the corresponding authors also did not respond to our request for further data. Therefore, their study could not be included in the analysis. This left a total of 11 studies 3,8,9,13 -20 for the meta-analysis.
The 3 studies by Desai et al 3,8,9 reported the differences between the mean change in scores with their 95% CI (between baseline and different time intervals for the 2 groups) and this was entered directly into our meta-analysis calculations. They also included graphic presentation of the mean changes in score (ie, improvement at different postoperative time intervals relative to baseline) for each group. This assisted in identifying the group with the most improved outcome score. The outcome score at 3 months from these studies were included in the 6 months interval analysis.
Tsutsumimoto et al 20 reported the SD for the postoperative ODI scores but not the SD for the preoperative score. We assumed that the SD was the same in preoperative and postoperative scores, which enabled us to calculate the mean change in scores and SE for the DT and non-DT groups. The SE for the JOA at 6 months was calculated using the t score, which was obtained by using the reported P value. Similarly, Grannum et al 15 did not report the SD or the SE in their results. The SE for the mean change in scores between the baseline and postoperative scores for each group was also calculated from the t score that was obtained using the reported P value. The rest of the studies either presented the mean change in scores and the respective 95% CI or the actual mean and the SD at each time interval for both groups.
Stromqvist et al 19 reported the largest cohort of patients categorized into 3 groups based on diagnosis: disc herniation, lumbar stenosis (LS) without spondylolisthesis, and LS with spondylolisthesis. The data was entered into the meta-analysis categorized according to the 3 groups. Sensitivity analysis by pooling the mean and the SD for all the groups was also carried out to assess if this had any impact on the overall results.
Grannum et al 15 reported their outcome at 6 months and also at final follow-up, which had a mean of 4.9 years (range 2-7 years). Therefore, the final follow-up data was included for the 48 months interval analysis.
Herren et al 16 reported the Core Outcome Measures Index (COMI) and leg pain and back pain VAS at an average of 15 months. The COMI score was included in the ODI meta-analysis at the 12-month interval. Leg pain and back pain VAS were also included in the meta-analysis at the 12-month interval.
The Effect of Sustaining DT on the Clinical Outcome
There were a total of 3653 DT cases (at the first respective follow-up) and these were compared with 68 294 cases with no DT. The pooled average follow-up was 13 months (pooled SD 5.5) with a range between 6 and 59 months. The range of follow-up for each study and the number of DT cases are reported in Table 1.
Most of the studies reported results for up to 1 year, and only 4 studies reported the ODI and SF36 score up to 4 years. The ODI score was slightly better in the non-DT group at 12 months (Figure 3) with an overall SMD difference of −0.06 (95% CI −0.12 to −0.01), P < .001. However, the ODI score did not show any difference at 6, 24, or even at 48 months: −0.03(95% CI −0.19 to 0.13), P = .73; −0.07(95% CI −0.08 to 0.21), P = .35; and 0.19 (95% CI −0.02 to 0.40), P = .07, respectively.
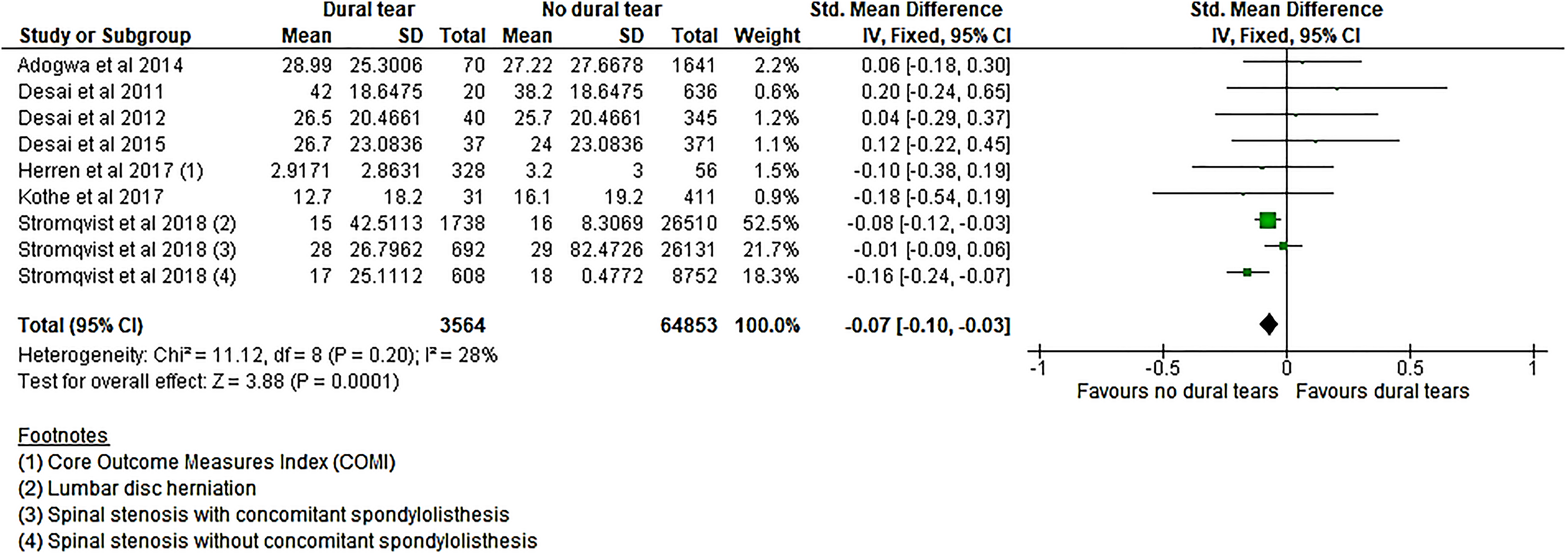
The standardized difference between the mean change in ODI scores between baseline and 12 months postsurgery. Herren et al reported the COMI score but included at this interval together with ODI scores from the other studies.
The SF36 functional score also revealed the same pattern with no differences in the scores between DT and non-DT groups at any time interval (Figure 4). SMD difference at 6, 12, 24, and 48 months were as follows: −0.07 (95% CI −0.10 to 0.24), P = .43; −0.01(95% CI −0.05 to 0.02), P = .51; 0.06 (95% CI −0.13 to 0.24), P = .54; and 0.12 (95% CI −0.10 to 0.34), P = .27, respectively.
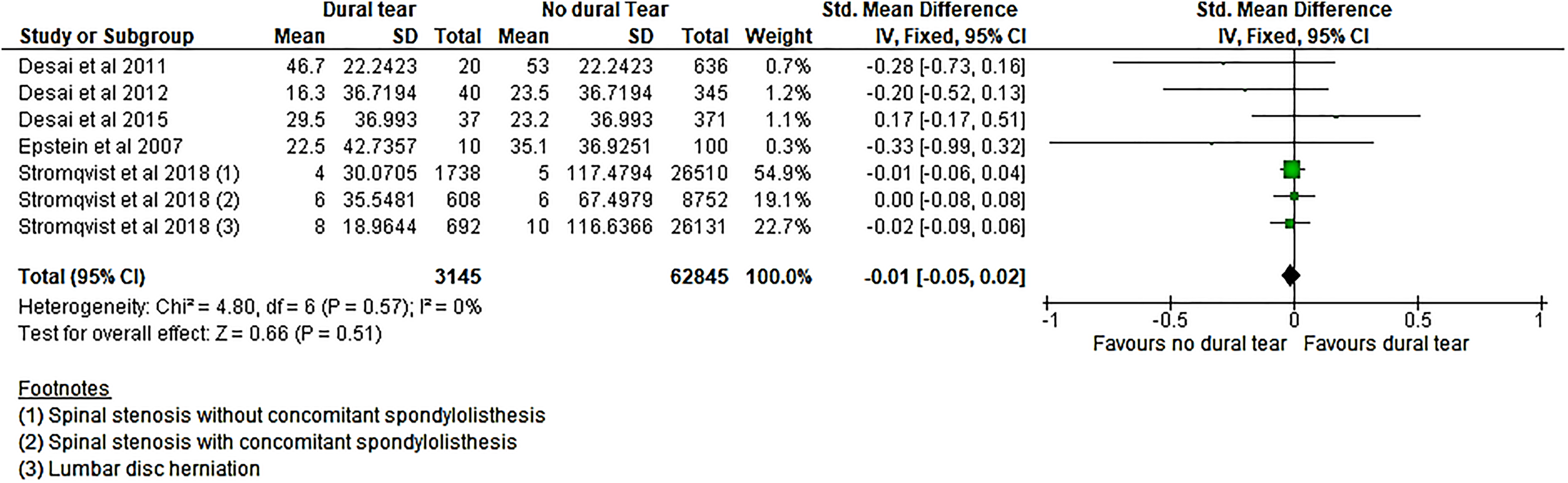
The standardized difference between the mean change in SF36 (function) scores between baseline and 12 months postsurgery.
Stromqvist et al 19 subdivided their cohort into 3 groups based on diagnosis, and initially the data was entered separately for each group in the meta-analysis. Further sensitivity analysis using the pooled mean and SD for the groups (for the whole cohort) did not change the above-mentioned outcome results.
Four studies 13,16,18,19 reported the leg pain and back pain VAS at 12 months. The overall improvement in the leg VAS was slightly better in the non-DT group with an overall SMD of −0.06 (−0.09 to −0.02), P = .001 (Figure 5); however, there was no difference in the back pain VAS between the 2 groups (Figure 6). Only 2 studies 15,18 reported the leg pain and back pain VAS for patients at 6 months and one 13 reported the leg pain and back pain VAS at 2 years and these did not show any difference between the 2 groups.
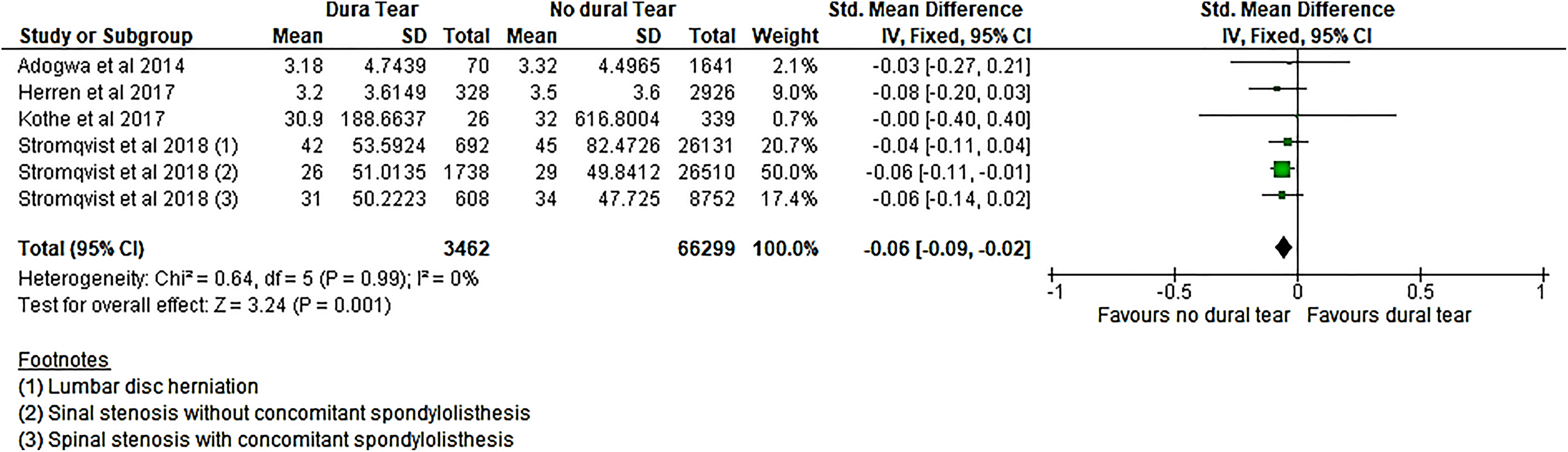
The standardized difference between the mean change in leg pain VAS between baseline and 12 months postsurgery.
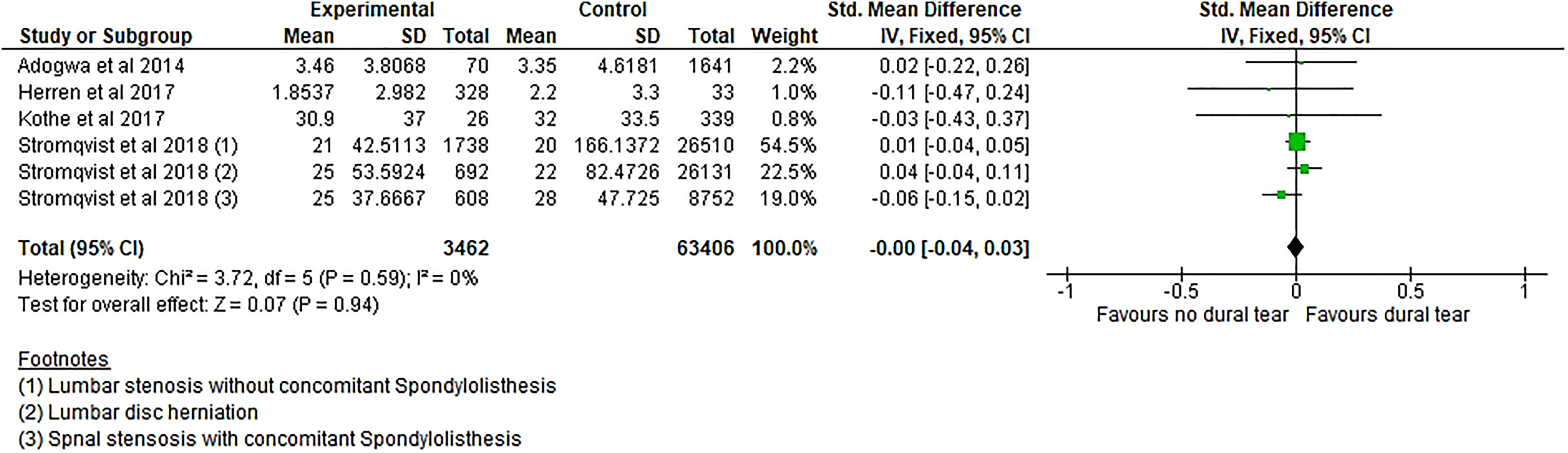
The standardized difference between the mean change in back pain VAS between baseline and 12 months postsurgery.
Subgroup analysis based on diagnosis is shown in Table 2. Lumbar spine stenosis was responsible for the significant results at 12 months in ODI and leg pain VAS. There was not enough description of the data in the studies to allow further subanalysis of the results according to the surgical approach or treatment.
Subanalysis Based on Diagnosis of Dural Tear Outcome at Different Time Intervals During the First 4 Years Postsurgery. Most of the Studies Reported the 12 Months’ Outcome.
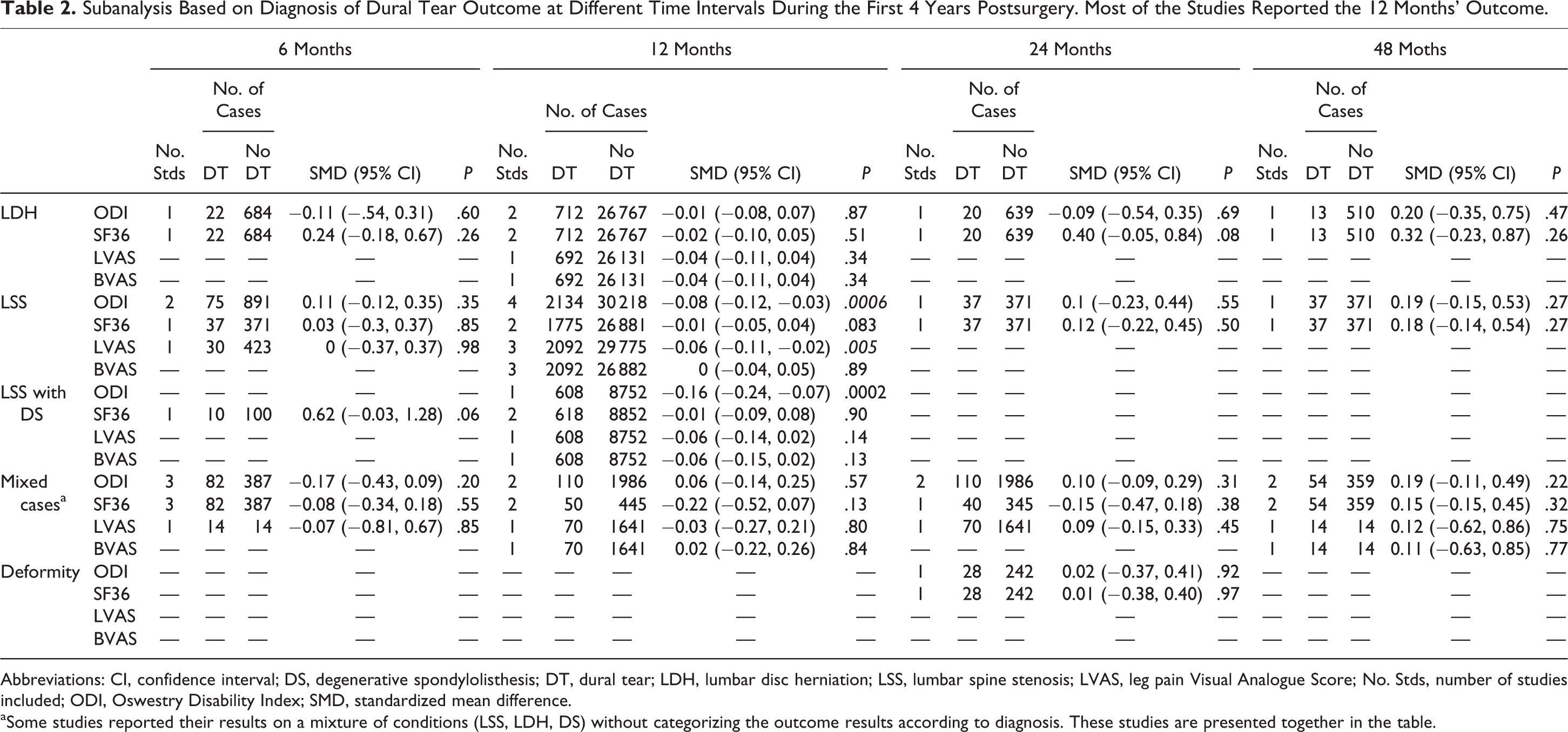
Abbreviations: CI, confidence interval; DS, degenerative spondylolisthesis; DT, dural tear; LDH, lumbar disc herniation; LSS, lumbar spine stenosis; LVAS, leg pain Visual Analogue Score; No. Stds, number of studies included; ODI, Oswestry Disability Index; SMD, standardized mean difference.
a Some studies reported their results on a mixture of conditions (LSS, LDH, DS) without categorizing the outcome results according to diagnosis. These studies are presented together in the table.
Discussion
This meta-analysis assessed patients’ reported outcome following accidental DT in elective spinal surgery up to 4 years postoperatively. We compared postoperative results to baseline (preoperative) data for both groups (DT and non-DT groups). Our meta-analysis revealed no difference in the SF36 functional outcome at any time interval postoperatively. There was, however, slightly better overall outcome in ODI in patients who did not sustained DT at 1 year following surgery, but this effect could not be demonstrated at 6 months and diminished at 2 and 4 years. The overall leg pain VAS score was also better in the non-DT group at 12 months, but the back pain VAS score was the same in both groups. There were not enough studies to conduct further comprehensive analysis at other time intervals for the leg pain and back pain VAS scores.
Jones et al 21 were the first to publish on the clinical outcome of 17 incidental DT cases that were repaired primarily during spinal surgery. These were matched (by age, sex, diagnosis, surgical procedure, surgeon, and follow-up) to a control group and followed-up for an average of 25.1 months. They found no statistically significant difference in the “long-term” outcome between the 2 groups with regard to the overall success of surgery, back pain and leg pain relief. Subsequently, Wang et al 6 reported a good outcome on a larger cohort of patients with accidental DT with a longer follow-up duration ranging between 2 and 8 years. Out of the 88 patients included, 76 (86%) reported good or excellent result, 9 (10%) reported satisfactory result, and only 3 (3%) reported poor outcome. Contrary to Wang et al, Saxler et al reported poorer results in a cohort of 41 patients who sustained DT during lumbar disc surgery over a longer period of follow-up with a mean of 10.2 years (range 4.2-18.5 years). Their cohort was also matched to a control group based on age, sex, spinal level, and duration of follow-up. Higher percentage of patients with DT reported no resolutions of symptoms and reported persistent leg pain and back pain.
None of the aforementioned studies objectively assessed the baselines (preoperative) functional status of patients and this could have affected their postoperative outcome. However, more recently, a number of studies prospectively assessed the preoperative and postoperative patient-reported outcome using validated outcome scores. This facilitated a more objective assessment of the outcome of patients following accidental DT and allowed direct comparison with control groups (no DT). Almost all the studies included did not demonstrate any statistical difference in ODI or SF36 or leg pain between the 2 groups. When the results of all the studies were combined in this meta-analysis, an overall significant difference in ODI and leg pain VAS score was significant only at 12 months interval but diminished subsequently. This is supported with the results of a recent study that did not demonstrate any differences in the outcome (ODI, JOA, SF36, and back pain and leg pain VAS) at 12 months between patients with and without DT following microendoscopic lumbar surgery. 11
We had expected that patients with DT would fare worse in their outcome, because DT are more likely to occur in complex procedures or revision surgeries. 2,17 Hence, these patients’ recovery is expected to be hampered by their underlying complex spinal conditions. However, most of the studies included in this meta-analysis reported on the outcome of primary lumbar surgeries and this might explain the similarities in the outcome between the 2 groups, as well as the reason for the low heterogeneity in our results. There were not enough studies to assess if DT had an impact on the overall outcome in more complex spinal conditions.
Stromqvist et al 19 had the largest cohort of patients of lumbar stenosis cases producing a larger weight on the meta-analysis, which influenced the overall results leading to a significant difference between the 2 groups in ODI and leg pain VAS at 12 months. This suggests that more studies are needed to improve the power to detect any true differences between the 2 groups at other time intervals.
Surgeons advocate direct repair of DT whenever feasible to minimize the risk of postoperative complications and to optimize recovery and outcome. 6,7,21 When direct repair is not feasible, indirect repair by patching with fat or muscle grafts or other synthetic agent is recommended. This minimizes the risk of persistent cerebrospinal fluid leak (and possibly revision surgery) and potentially ameliorate the impact of DT on the reported outcome.
It is well established that accidental DT are associated with longer operative time, longer hospital stay, and higher rate of neurological deficit and revision surgery. 1,16,22 This was outside the scope of this review, but all these outcome parameters can inevitably have a significant financial impact and affect the overall outcome of surgery. 22 Therefore, any study addressing the outcome of DT should also consider these perioperative complications and their overall financial impact.
Conclusion
Dural tears are well-known complications of spinal surgery but they do not appear to have a significant impact on the overall short-term patient-reported outcome. The number of studies is still limited, and we lack long-term studies on this topic.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.