
Abstract
Study Design:
Retrospective cohort study.
Objectives:
(1) To assess patient-reported outcomes—physical function, pain, and quality of life—in patients who underwent resection of a mobile spine chondrosarcoma. (2) To assess complications (90 days), readmissions, reoperations, oncological outcomes, and neurologic status.
Methods:
Thirty-three patients with spinal conventional chondrosarcoma resection between 1984 and 2014 at one hospital were included. The primary outcome measures were—minimally 6 months after surgery—the EuroQol 5 Dimensions (EQ5D), PROMIS–Physical Function, PROMIS–Pain Intensity, and Oswestry (ODI) Disability Index, or Neck (NDI) Disability established in 14 out of 20 alive (70.0%) patients. Complications, readmission, reoperations, oncological outcomes, and neurological status were reported for the complete cohort of 33 patients.
Results:
After spine chondrosarcoma resection, patients (n = 14) reported worse physical function (median 43, range 22-61, P = .026), worse quality of life (median EQ5D 0.70, range 0.04-1, P = .022), and comparable pain intensity (median 47, range 31-56, P = .362) when compared with US general population values. The median NDI/ODI was 25 (range 0-72) indicating mild to moderate disability. Patients undergoing reoperation had worse patient-reported outcomes than those who did not. Eighteen (55.5%) out of 33 patients suffered complications (90 days), 14 (42.4%) had unplanned readmission, and 13 (39.4%) underwent reoperation. Intralesional resection was associated with increased readmission, reoperation, and recurrence rate.
Conclusions:
Chondrosarcoma affects quality of life and physical function and its treatment frequently results in complications and reoperations. Our findings can be used to inform future patients about expected outcomes.
Introduction
Chondrosarcomas account for 20% to 27% of malignant bone tumors, 1,2 and 10% arise from the mobile spine. 3 –6 Spinal chondrosarcoma resection with negative margins has been shown to improve local control and survival 2 –4,7 –10 ; a complicating factor is the anatomy that often makes en bloc resection with negative margins technically difficult. Furthermore, these surgeries are associated with substantial morbidity. 11,12
The key aim of surgical resection is to achieve local tumor control and improve life expectancy. However, as long-term survival for these patients have improved due to better surgical and adjuvant treatment, 5,13 functional outcome and quality of life become important outcomes that the patient needs to be informed about. 14,15 Previous studies on spinal chondrosarcoma have reported on oncological outcomes; however, patient-reported outcome has not been studied. 3 –6,9,16 –18
Primarily, we assessed patient-reported outcomes—physical function, pain, and quality of life—in patients who underwent resection of a mobile spine chondrosarcoma and were available for follow-up. Secondarily, we assessed complications (90 days), readmissions, reoperations, oncological outcomes, and neurologic status in the complete cohort. We reported overall outcomes, and reported outcomes based on type of resection (en bloc vs intralesional) including margin status (negative vs positive).
Materials and Methods
Study Design and Participants
Our institutional review board approved this study and a waiver of consent was granted. We included patients aged 18 years or older, who underwent primary or secondary resection of a mobile spine chondrosarcoma at our Orthopaedic Spine Oncology Service between 1984 and 2014. Secondary resection includes resection of a recurrence or residual tumor after previous surgery at a different institution. Exclusion criteria were: nonconventional chondrosarcoma (dedifferentiated, secondary, mesenchymal, juxtacortical, and clear cell) and chondrosarcoma of a nonspinal origin metastasized to the spine. Thirty-three patients met these criteria and were identified by word-based queries searching operative and pathological reports in our orthopedic oncology database.
In February 2015 we sent an invitation letter to complete an online survey to 20 patients who were alive and had a minimum follow-up of 6 months (reminder at 2 and 8 months); 14 out of 20 patients (70.0%) completed all surveys. We were unable to contact 4 patients, and 2 refused participation. Survey data was collected using Assessment Center (Northwestern University Feinberg School of Medicine, Chicago, IL, USA, 2007). 19
Patient-reported outcomes were analyzed for those who completed the survey (n = 14), whereas all other outcomes (complications, readmissions, reoperations, oncological outcomes, and neurologic status) are described for the complete cohort (n = 33).
Treatment
Whenever achievable, we treat spinal chondrosarcomas by en bloc resection with negative margins, in conjunction with neoadjuvant or adjuvant photon/proton radiation and—when the tumor abuts the dura—intraoperative dural plaque radiation to address any dural tumor seeding. 13 The majority are treated by a 2-stage procedure; the first stage consists of posterior stabilization (with or without decompression of the spinal canal), and excision of the tumor is performed by an anterior approach in the second surgery. Relatively healthy patients with favorable neurologic and oncologic status, or those with tumor locations amenable to such, may be treated by a combined (anterior and posterior) approach in a single surgery.
Patients will undergo intralesional resection if the tumor location, size, or proximity to adjacent viscera or major vessels hinders resection with negative margins. Residual or recurrent tumors are often more challenging and are more likely to result in intralesional resection. 4,17,20
Outcomes and Explanatory Variables
Our primary outcome measures were the PROMIS (Patient-Reported Outcomes Measurement Information System) Physical Function (Cancer Bank), PROMIS Pain Intensity, EuroQol 5 Dimensions (EQ5D), and the Oswestry Disability Index (ODI; thoracolumbar lesions) or Neck Disability Index (NDI; cervical lesions) reflecting the health status of the patient at time of survey completion. 21 –25
The raw score of each PROMIS questionnaire is transformed into a t-score; a standardized score with a mean of 50 (US general population) and a standard deviation of 10. A higher PROMIS Physical Function t-score corresponds to better physical function. 22,23,26 A higher PROMIS Pain Intensity score corresponds to more pain.
The EQ5D questionnaire is a generic short form with 5 items, and assesses quality of life. 21,27 Higher scores indicate better quality of life. We compared scores with the US population average of 0.85. 28
ODI and NDI scores range from 0 to 100, with higher scores indicating more disability. 24,25,29
No questions regarding any of the secondary outcome measures were included in the questionnaires sent to patients to avoid bias.
Secondary outcome measures were complications (90 days), readmissions, reoperations, local recurrence rate, new metastases after surgery, disease-specific survival (from medical charts and from the Social Security Death Index), 30 and neurologic status at final follow-up. We categorized complications (90 days) into minor (ie, requiring pharmacological treatment, except for commonly used postoperative medications [eg, analgesics] and blood transfusion as all patients had blood transfusions) and major (ie, requiring surgical, endoscopic, or radiological intervention). 31
Baseline characteristics at time of surgery were age, Body mass index (BMI) in kg/m2, sex, smoking status, type of lesion, and symptoms at presentation. Oncologic preoperative variables were tumor location, World Health Organization (WHO) pathologic tumor grade, 8,32 Enneking tumor staging, 33 extent of the lesion (Weinstein-Boriani-Biagini [WBB] system), 34 tumor growth into local neurovascular structures, prior tumor embolization, and prior radiotherapy or chemotherapy. Surgical variables were: primary resection or (secondary) resection of a recurrence/residual tumor, year, approach, intraoperative radiotherapy, and resection margin status (positive defined as tumor tissue at the surface of the specimen).
Statistical Analysis
Categorical variables are presented with frequencies and percentages, and continuous variables with median, interquartile range (IQR), and range. We used the Mann-Whitney U test and the Fisher exact test to analyze differences between patients treated by en bloc resection with negative margins versus intralesional or en bloc resection with positive margins. We used the one sample signed rank test to assess whether scores differed from US population averages. We calculated differences in patient-reported outcomes for explanatory variables using the Mann-Whitney U test. We used the log-rank test to analyze differences for specific explanatory variables for oncologic outcomes. We performed all analyses with Stata 13.0 (StataCorp LP, College Station, TX, USA) and considered 2-tailed P values less than .05 as significant.
Results
Baseline Characteristics
The median age was 48 years (range 24-66 years), 20 (60.6%, 20/33) were men and the median BMI was 25 kg/m2 (IQR 24-29 kg/m2) (Table 1). Most patients presented with back pain (71.9%, 23/32), 35.5% (11/31) had neurologic deficits, and most tumors were located in the thoracic spine (72.7%, 24/33). Twenty-eight (85%, 28/33) were WHO grade I-II tumors, 3 (9.1%, 3/33) patients had a preoperative metastasis (2 locoregionally in the spine, 1 in the lung) (Table 2). Eighteen (54.5%, 18/33) patients had received local radiotherapy, 4 (12.5%, 4/32) underwent preoperative embolization, and 3 (9.1%, 3/33) had preoperative chemotherapy—all 3 with Adriamycin. Nineteen (57.6%, 19/33) patients underwent their first resection elsewhere (Figure 1).
Baseline Characteristics for Patients With Primary Chondrosarcoma in the Mobile Spine Treated by En Bloc Resection With Negative Margins or En Bloc Resection With Positive Margins/Intralesional Surgery.
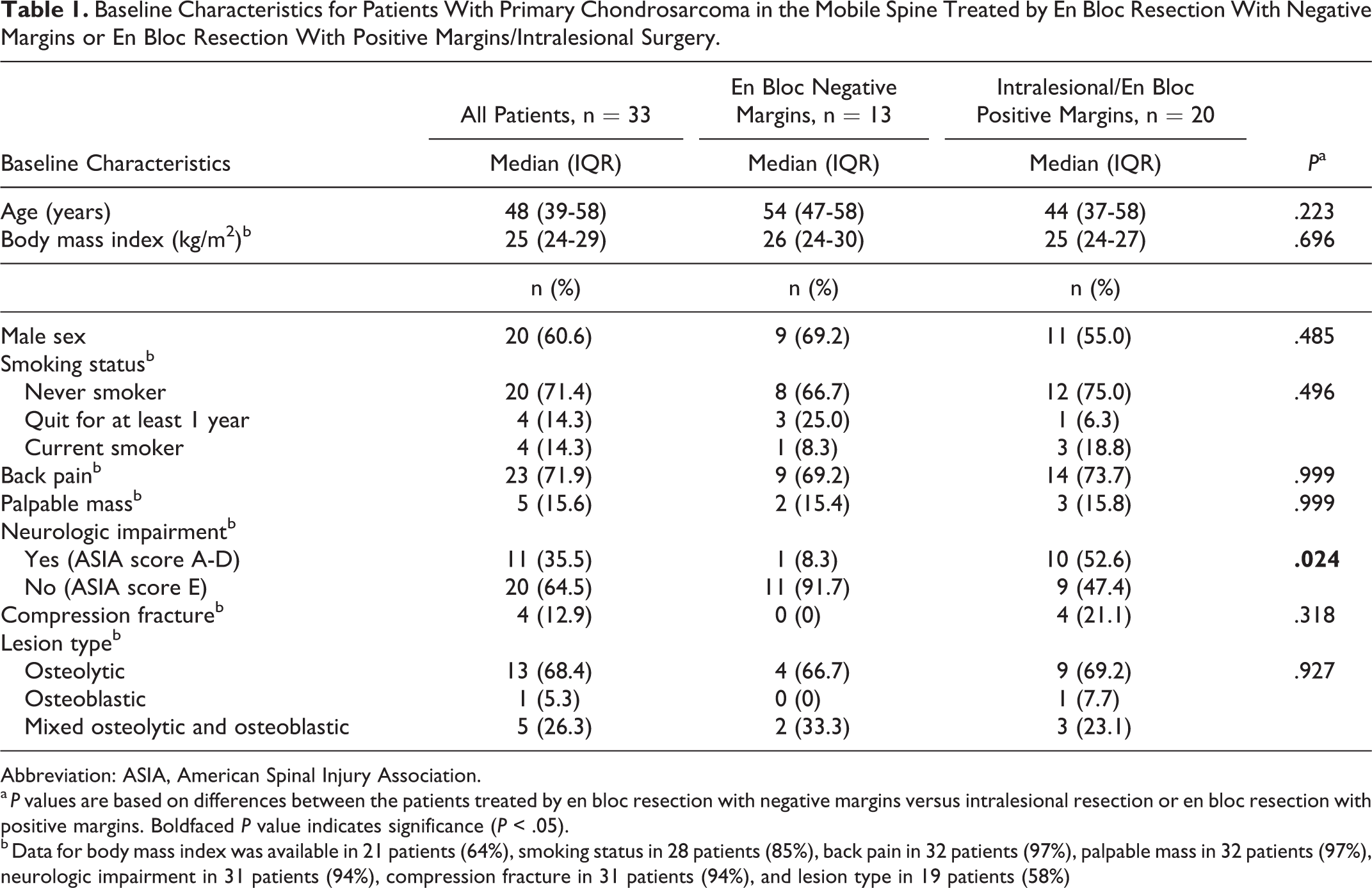
Abbreviation: ASIA, American Spinal Injury Association.
a P values are based on differences between the patients treated by en bloc resection with negative margins versus intralesional resection or en bloc resection with positive margins. Boldfaced P value indicates significance (P < .05).
b Data for body mass index was available in 21 patients (64%), smoking status in 28 patients (85%), back pain in 32 patients (97%), palpable mass in 32 patients (97%), neurologic impairment in 31 patients (94%), compression fracture in 31 patients (94%), and lesion type in 19 patients (58%)
Oncologic Status of Patients With Primary Chondrosarcoma in the Mobile Spine Treated by En Bloc Resection With Negative Margins or En Bloc Resection With Positive Margins/Intralesional Surgery.
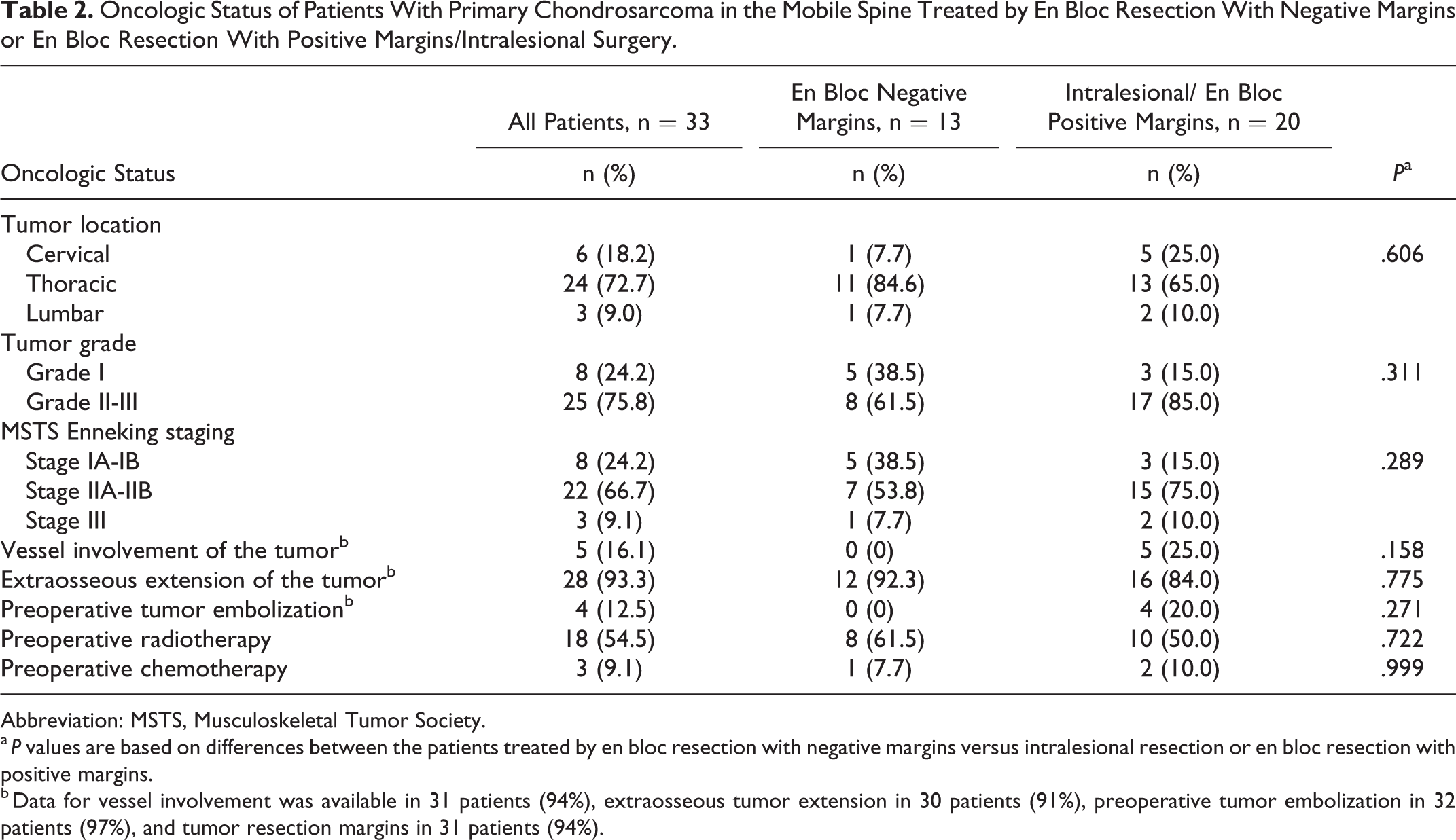
Abbreviation: MSTS, Musculoskeletal Tumor Society.
a P values are based on differences between the patients treated by en bloc resection with negative margins versus intralesional resection or en bloc resection with positive margins.
b Data for vessel involvement was available in 31 patients (94%), extraosseous tumor extension in 30 patients (91%), preoperative tumor embolization in 32 patients (97%), and tumor resection margins in 31 patients (94%).
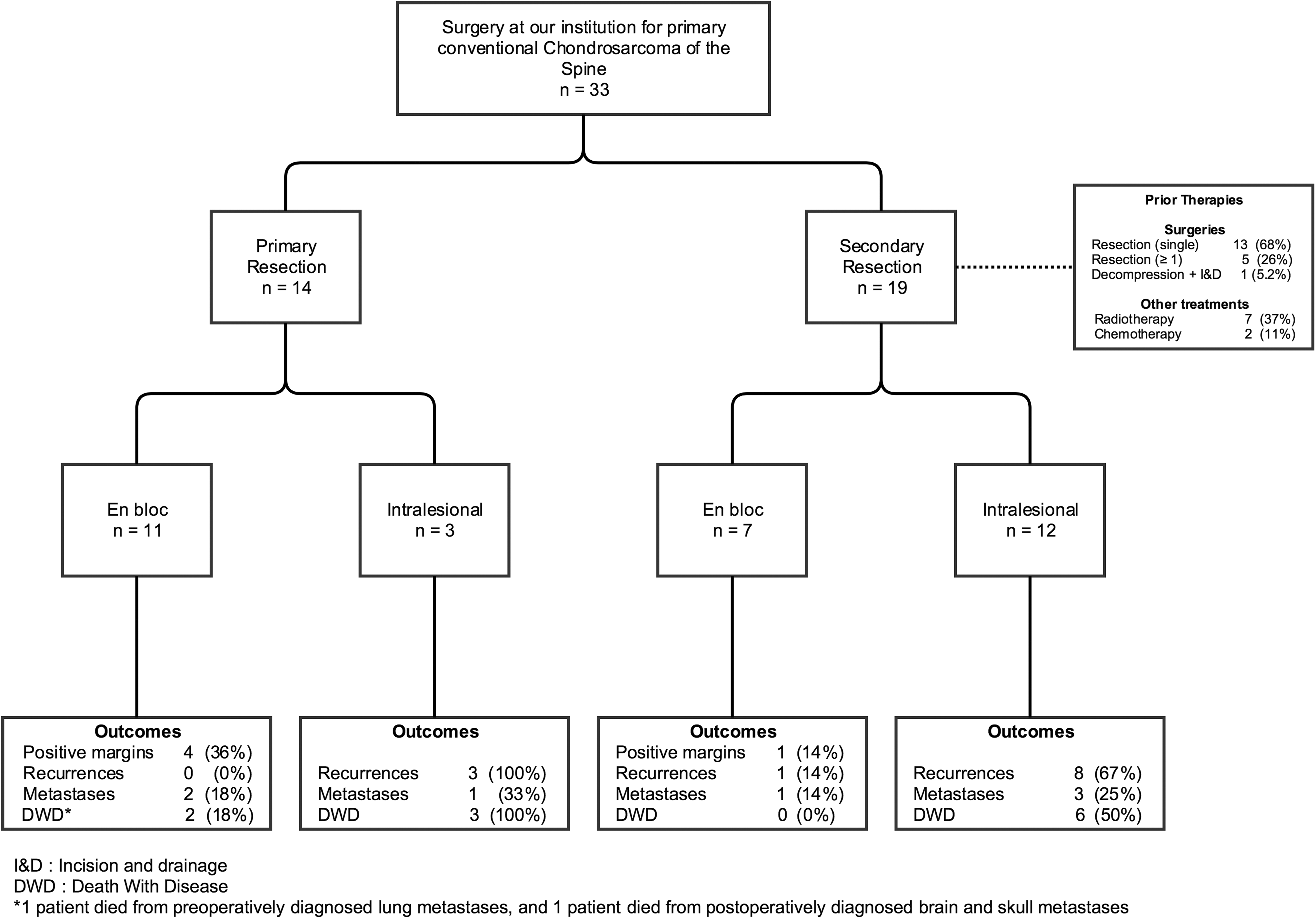
Flowchart displaying the treatment course for all 33 included patients.
We performed 18 (54.5%, 18/33) en bloc resections, and obtained negative resection margins in 13 (72.2%, 13/18) of these cases (Table 3); 8 wide resection margins (ie, continuous shell of healthy tissue around the tumor), and 5 marginal resection margins (ie, tumor mass covered mostly by only a “pseudocapsule”). 4 Twenty patients (60.6%, 20/33) had a combined—that is, posterior and anterior—approach, of which 15 patients (75%, 15/20) in a 2-staged fashion. Nine patients (27.3%) received intraoperative radiotherapy; 7 by intraoperative dural plaque brachytherapy, 2 by external beam therapy (20 kV peak applicator).
Surgical Characteristics for Patients With Primary Chondrosarcoma in the Mobile Spine Treated by En Bloc Resection With Negative Margins or En Bloc Resection With Positive Margins/Intralesional Surgery.
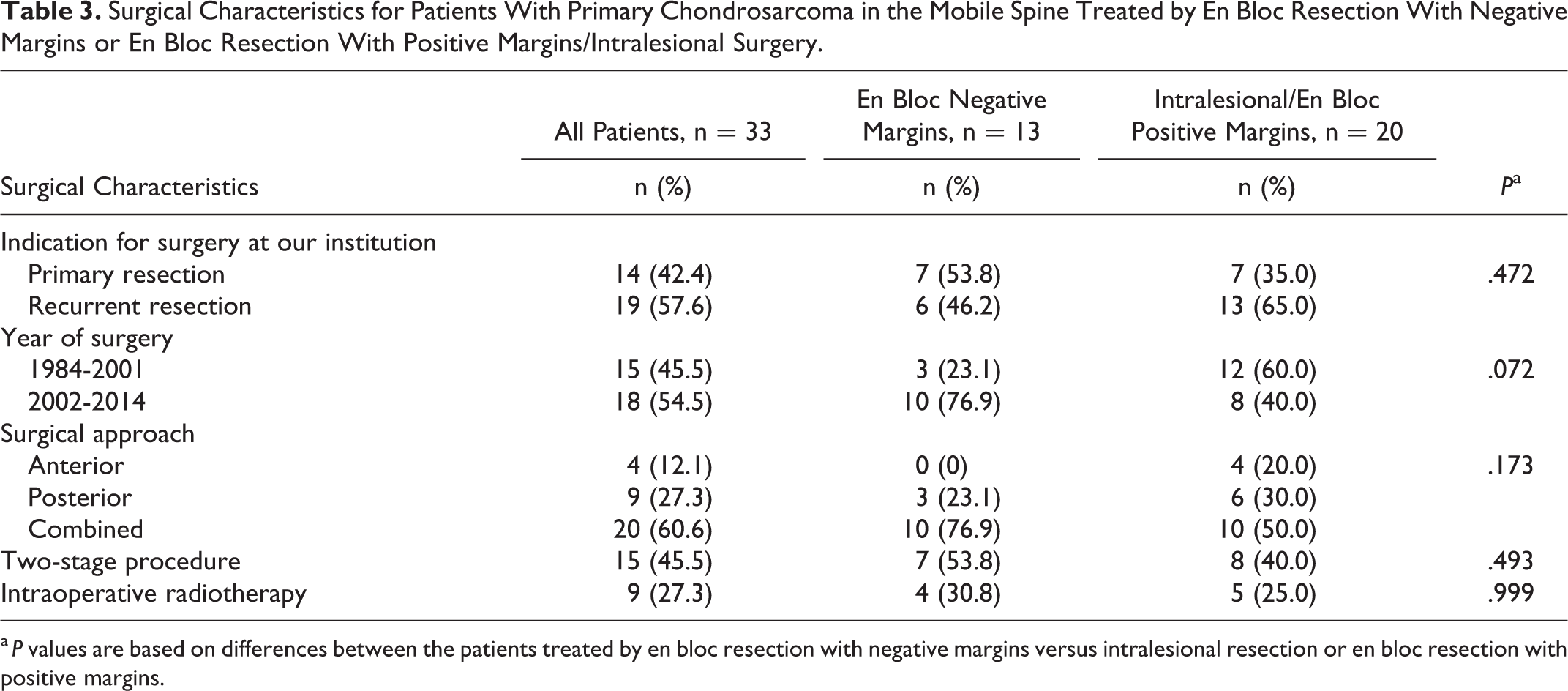
a P values are based on differences between the patients treated by en bloc resection with negative margins versus intralesional resection or en bloc resection with positive margins.
Patients who underwent en bloc resection with negative margins more often were neurologically intact as compared with patients who underwent intralesional resection or en bloc resection with positive margins (P = .024) (Table 1). There were no other differences in baseline, oncological, or surgical characteristics between these 2 groups (Tables 1–3).
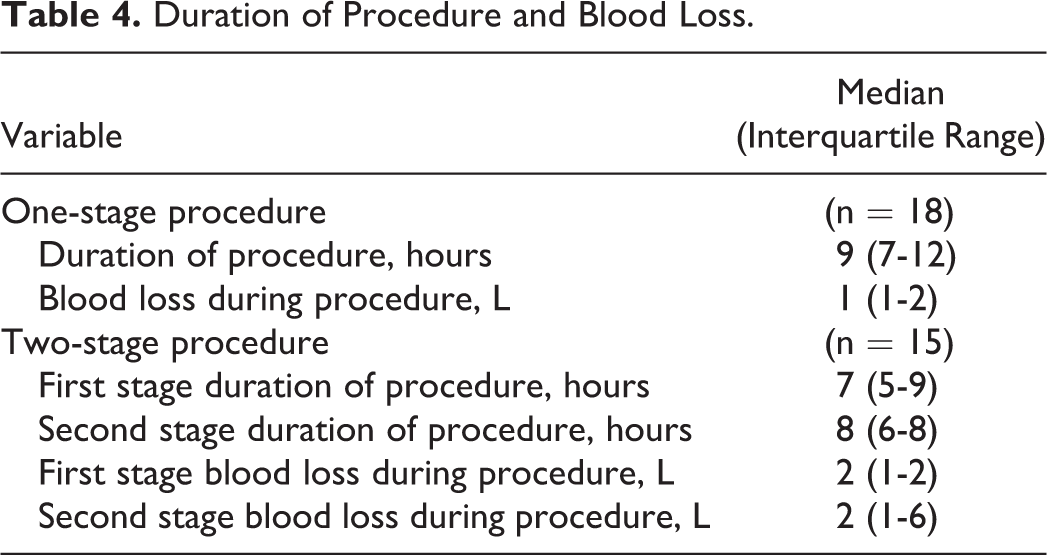
Eighteen (54.5%, 18/33) patients had a single-stage procedure lasting for a median of 9 hours (IQR 7-12 hours, available in 11 patients) with a median blood loss of 1 L (IQR 1-2 L, available in 13 patients) (Table 4). Fifteen (45.5%, 15/33) patients had a 2-stage procedure; first-stage surgeries lasted for a median of 7 hours (IQR 5-9 hours, available in 12 patients) with a median blood loss of 2 L (IQR 1-2 L, available in 13 patients); second-stage surgeries lasted for a median of 8 hours (IQR 6-8 hours, available in 10 patients) with a median of 2 L of blood loss (IQR 1-3 L, available in 8 patients). The median stay at the surgical intensive care unit was 1 day (IQR 1-6 days, range 0-38 days).
Duration of Procedure and Blood Loss.
The median clinical follow-up for all 33 patients was 24 months (IQR 9-96 months). Clinical follow-up was less than 6 months for 3 (9.1%) cases (7, 36, and 113 days). The median follow-up for the 14 patients answering questionnaires was 5 years (IQR 13-129 months, range 6 months to 18 years).
Patient-Reported Outcomes (n = 14)
Compared with the US general population values, patients with spinal chondrosarcoma had worse physical function (median t-score 43, range 22-61, P = .026), and worse quality of life (median EQ5D 0.70, range 0.04-1, P = .022). Pain intensity was comparable to the US population values (median t-score 47, range 31-56, P = .362). The median NDI/ODI was 25 (range 0-72) indicating mild to moderate disability (Tables 5 and 6). 24,25,29
Patient-Reported Outcome Measures (n = 14).
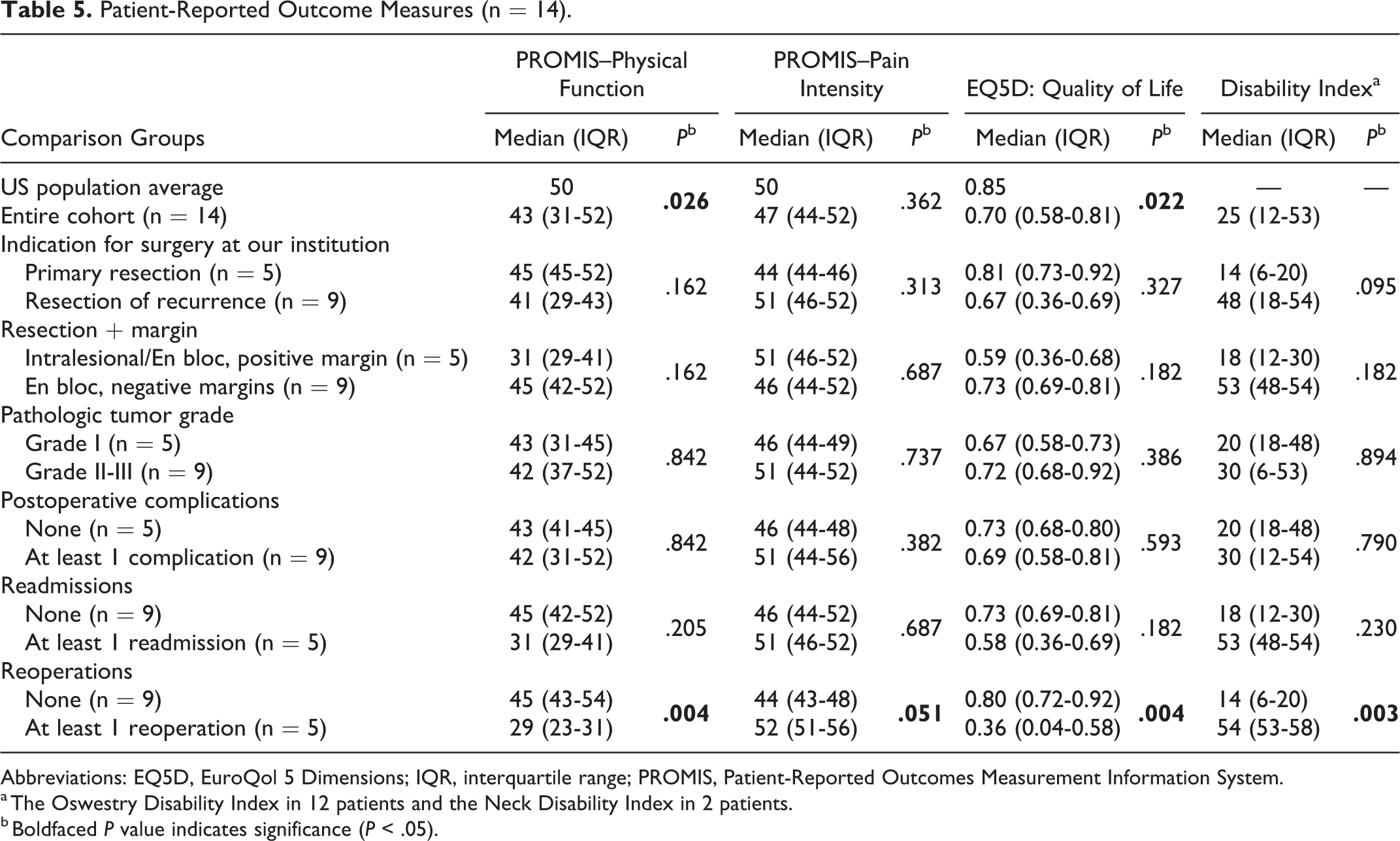
Abbreviations: EQ5D, EuroQol 5 Dimensions; IQR, interquartile range; PROMIS, Patient-Reported Outcomes Measurement Information System.
a The Oswestry Disability Index in 12 patients and the Neck Disability Index in 2 patients.
b Boldfaced P value indicates significance (P < .05).
Clinical Data and Patient-Reported Outcomes of the 14 Cases Surgically Treated for Chondrosarcoma at Our Institution and Who Filled Out the Questionnaire.
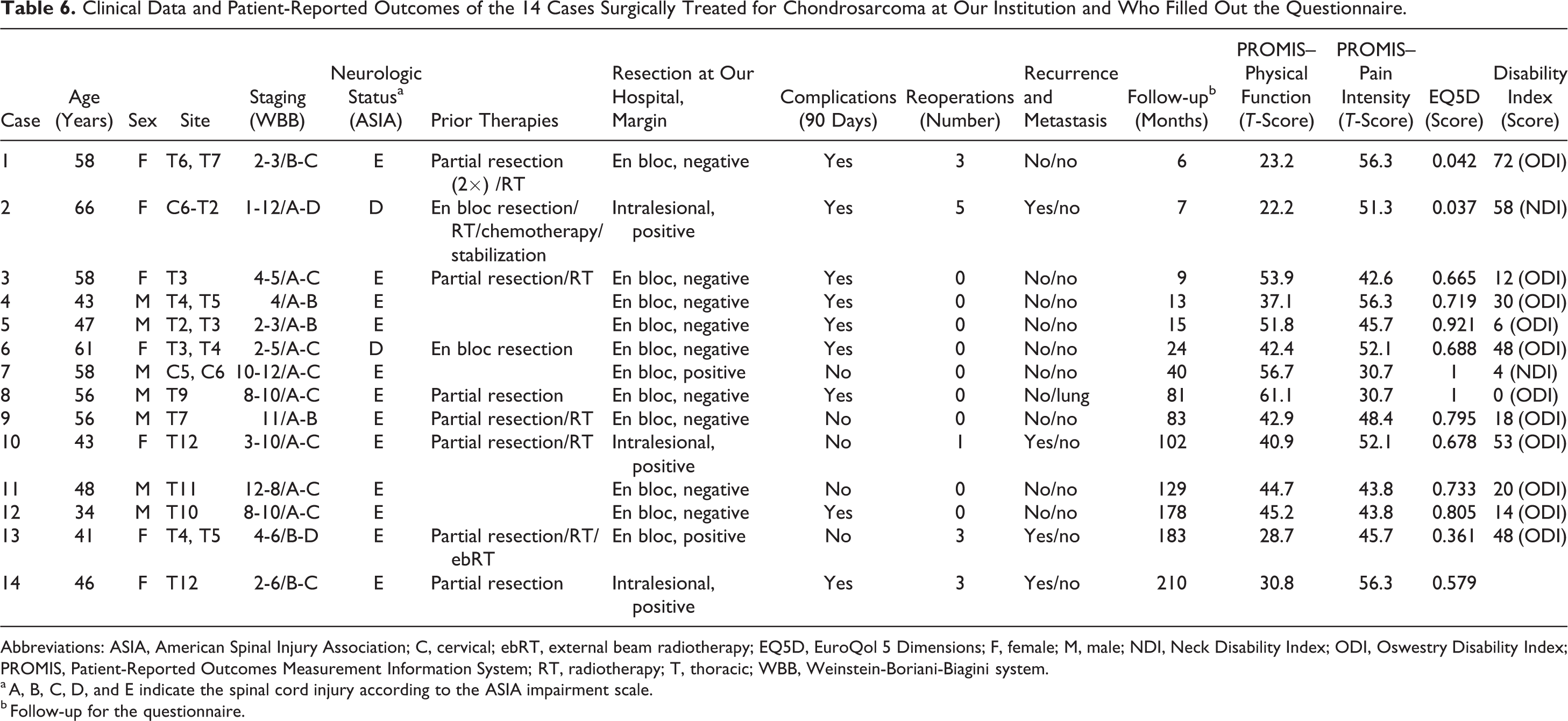
Abbreviations: ASIA, American Spinal Injury Association; C, cervical; ebRT, external beam radiotherapy; EQ5D, EuroQol 5 Dimensions; F, female; M, male; NDI, Neck Disability Index; ODI, Oswestry Disability Index; PROMIS, Patient-Reported Outcomes Measurement Information System; RT, radiotherapy; T, thoracic; WBB, Weinstein-Boriani-Biagini system.
a A, B, C, D, and E indicate the spinal cord injury according to the ASIA impairment scale.
b Follow-up for the questionnaire.
Patients who underwent reoperation after surgery at our institution (5/14) had worse physical function (P = .004), worse quality of life (P = .004), and were more severely disabled (P = .003) when compared with patients who did no undergo reoperation (9/14) (Table 5).
Complications (90 Days), Readmissions, and Reoperations (n = 33)
Thirty-two complications (90 days) occurred in 18 (54.5%, 18/33) patients; 14 (42.4%, 14/33) developed at least 1 major complication, and 10 (30.3%, 10/33) at least 1 minor complication (Table 7). Most common major complications were dural tear (n = 4), respiratory failure (n = 3), and deep wound infection (n = 2). Common minor complications were pulmonary embolism (n = 5), pleural effusion (n = 4), and urinary tract infection (n = 2). After en bloc resection with negative margins 9 out of 13 (69.2%) patients had at least 1 complication, and after intralesional resection or en bloc resection with positive margins 9 out of 20 (45.0%) patients had at least 1 complication (P = .284).
Complications (90 Days), Readmissions, and Reoperations After Resection for Patients With Chondrosarcoma of the Mobile Spine (n = 33).
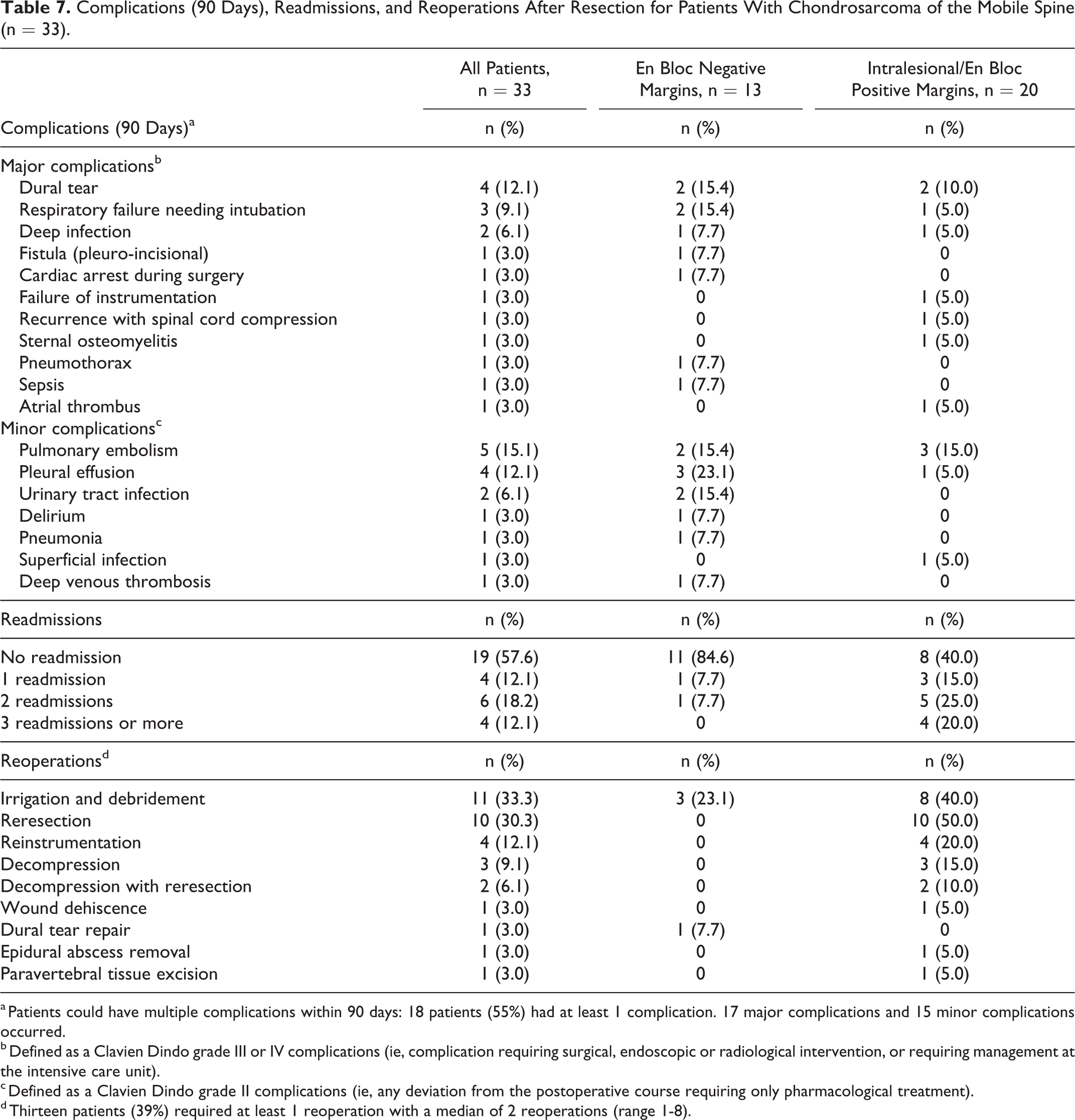
a Patients could have multiple complications within 90 days: 18 patients (55%) had at least 1 complication. 17 major complications and 15 minor complications occurred.
b Defined as a Clavien Dindo grade III or IV complications (ie, complication requiring surgical, endoscopic or radiological intervention, or requiring management at the intensive care unit).
c Defined as a Clavien Dindo grade II complications (ie, any deviation from the postoperative course requiring only pharmacological treatment).
d Thirteen patients (39%) required at least 1 reoperation with a median of 2 reoperations (range 1-8).
Fourteen (42.4%, 14/33) patients were readmitted after a median time of 13 months (range 1-197 months); 4 (12.1%, 4/33) patients had at least 3 readmissions (Table 7). After en bloc resection with negative margins, 2 out of 13 (15.4%) patients had at least 1 readmission, and after intralesional resection or en bloc resection with positive margins 12 out of 20 (60.0%) patients had at least 1 readmission (P = .015). Thirteen (39.4%, 13/33) patients required a reoperation, with a median of 2 reoperations (range 1-8 reoperations) (Table 7). Most common reoperations were irrigation and debridement in 11 (33.3%, 11/33) cases for infection (2 cases within 90 days), resection of a recurrence in 10 cases (30.3%, 10/33), and reinstrumentation in 4 cases (12.1%, 4/33). After en bloc resection with negative margins 2 out of 13 (15.4%) patients had at least 1 reoperation, and after intralesional resection or en bloc resection with positive margins, 11 out of 20 (55.0%) patients had at least 1 reoperation (P = .032).
Oncological Outcomes (n = 33)
All 12 local recurrences occurred in patients who underwent intralesional resection or en bloc resection with positive margins (60%, 12/20), while none recurred in the 13 patients who had en bloc resection with negative margins (P = .002) (Figure 2). Six (18.2%, 6/33) patients developed metastases to the lung (n = 4), distant bone (n = 2), brain (n = 1), soft tissue of the neck (n = 1), and periaortic region (n = 1) (Figure 3). Eleven (33.3%, 11/33) patients died of disease after a median of 7 years (IQR 1.2-12 years) (Figure 4); 10 (50.0%, 10/20) died of disease after intralesional resection or en bloc resection with positive margins, and 1 died of disease after en bloc resection with negative margins (P = .064)
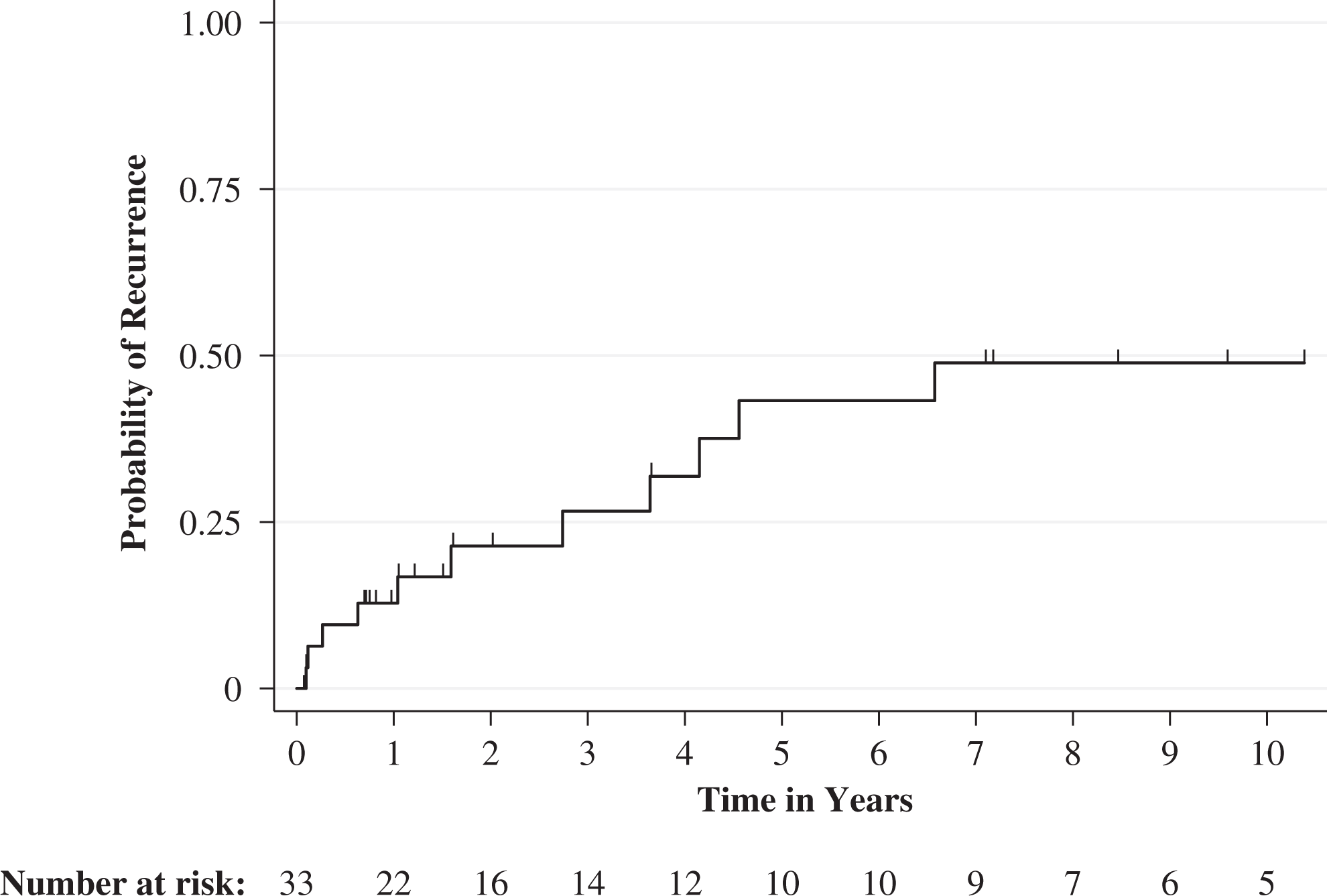
Kaplan-Meier curve displaying the time to local recurrence for 33 included patients. Hash marks on the curve represent censoring of a patient (moment of lost to follow-up).
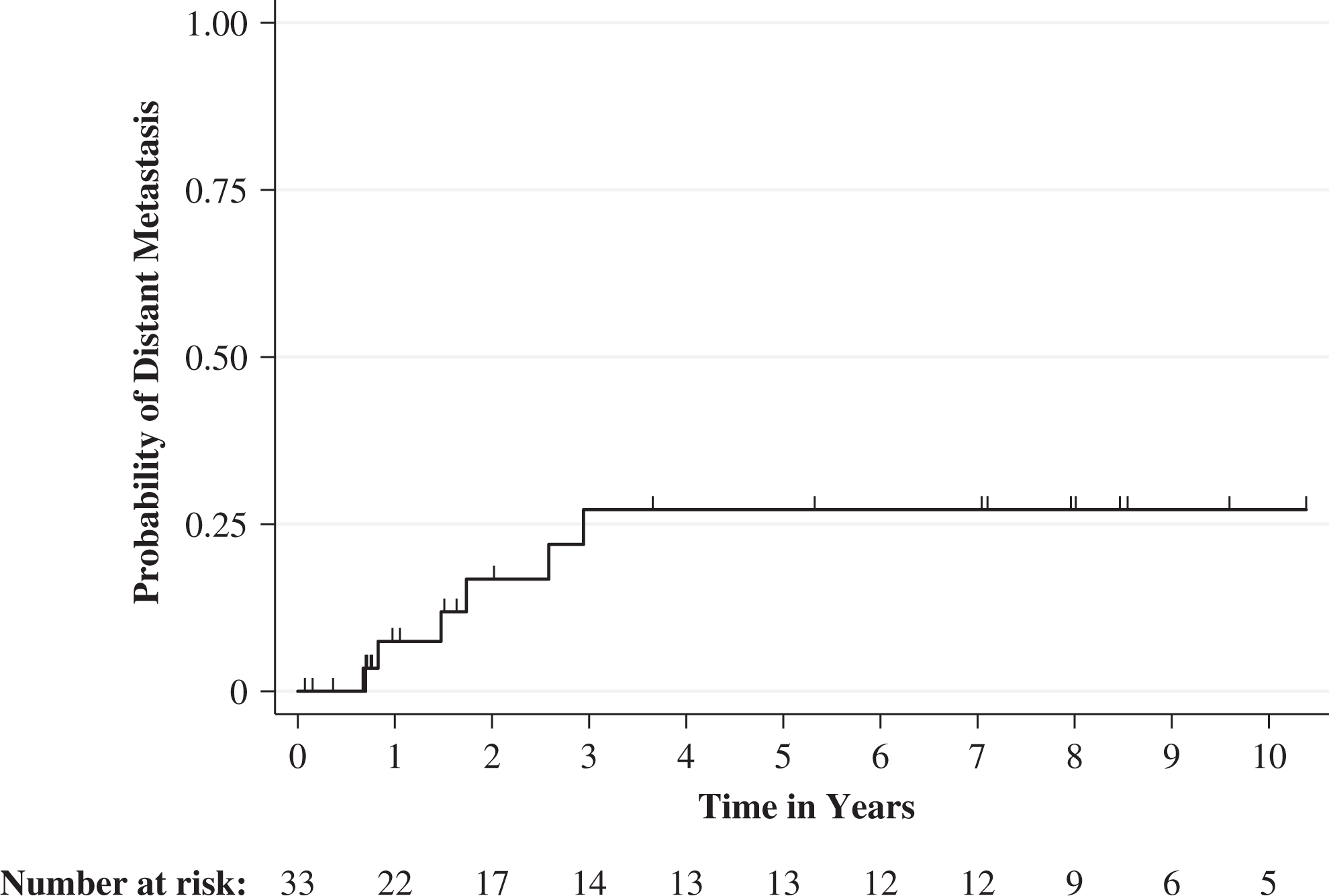
Kaplan-Meier curve displaying the time to distant metastasis for all 33 included patients. Hash marks on the curve represent censoring of a patient (moment of lost to follow-up).
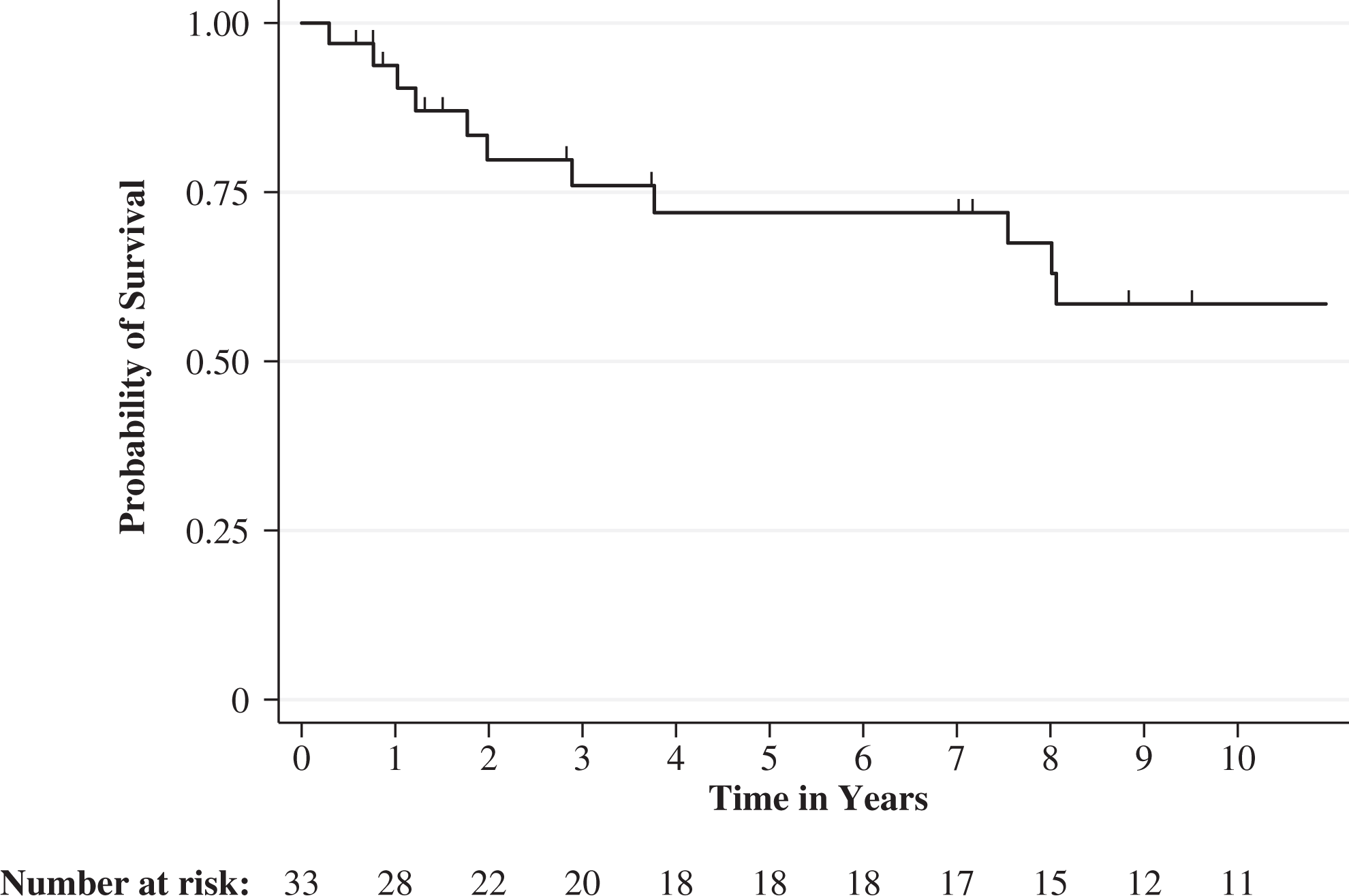
Kaplan-Meier curve displaying disease specific survival for all 33 included patients. Hash marks on the curve represent censoring of a patient (moment of lost to follow-up, or death without presence of disease).
Neurologic Status (n = 33)
Among 11 patients with preoperative neurologic deficits, 6 (66.7%, 6/9) improved, 2 (22.2%, 2/9) had neurologic decline, and 1 (11.1%, 1/9) had no change. Neurologic status at follow-up could not be established for 2 patients.
Discussion
We found that after a median follow-up of 5 years, patients who underwent surgery for spinal chondrosarcoma reported worse physical function and quality of life compared with the US population average. Reoperation was associated with worse physical function and quality of life. Complication rates, readmission rates, and reoperation rates were high. Readmission, reoperation, and local recurrence rates were higher after intralesional or en bloc resection with positive margins as compared with en bloc resection with negative margins. No other studies have reported on patient-reported outcomes after surgical resection of spinal chondrosarcoma. Srivastava et al 37 handed out a disease-specific questionnaire (ie, the EORTC QLQ-C30) to 17 spinal chordoma/chondrosarcoma patients before and at the end of proton beam therapy; quality-of-life scores were maintained in the majority of the patients during the course of proton beam therapy. Van der Geest et al 15 analyzed quality of life 7 years after treatment for—non-spinal—chondrosarcoma. Compared with healthy controls, patients with chondrosarcoma performed inferiorly in several quality-of-life domains (fatigue, physical function, and sleep). Melcher et al 38 report on 15 patients after total en bloc spondylectomy of primary malignant bone tumors or solitary metastases; quality of life was decreased for all individual scales when compared with (German) normal population values but exceeded values for chronic back pain patients. In another study, health-related quality of life (SF-36) was decreased for patients alive with disease, when compared to those with no evidence of disease after en bloc resection of primary malignant bone tumors or solitary metastases. 39 Mazel et al 40 report on 25 patients with primary bone tumors or single metastatic disease; quality of life was comparable to general (French) population values, and lower for those with a secondary tumor or those who had multiple levels resected. Colman et al 41 showed worse quality of life and physical function than average (US) population values for patients with mobile spine tumors (benign, malignant, and solitary metastasis). Kato et al 42 demonstrated that physical health was impaired in the early postoperative years after en bloc spondylectomy; this returned to normal approximately 3 years after surgery, indicating that these surgeries require long recovery periods. A comparison of quality of life (as measured by EQ5D) among patients in our study (0.70) with other common conditions shows that patients after resection of a chondrosarcoma of the spine do worse than patients with diabetes (0.76), asthma (0.82), and high blood pressure (0.79). However, their quality of life is comparable to that of patients with angina (0.71), myocardial infarction (0.73), and coronary artery disease (0.73) and slightly better than that of those who have suffered a stroke (0.69). All dimensions measured by the EQ5D among our patients were slight to moderately affected (ie, physical function, pain, and mental health). We believe that both the disease and the extensiveness of the surgery affects quality of life. However, both aspects most likely affect different dimensions of quality of life: For example, the disease probably has more impact on mental health (worrying about prognosis), whereas the surgery probably has more impact on pain and physical function. The quality of life and physical function among patients after resection of chondrosarcoma of the spine in our study (median EQ5D 0.70, ODI 25) is worse than a cohort of US patients from the Quality Outcomes Database who underwent surgery for degenerative spine conditions (including [recurrent-] disc herniation, spondylolisthesis, stenosis, adjacent segment disease, and disc collapse) at 12 months after surgery (median EQ5D 0.82, ODI 18, n = 5443). 44
Complication rates after spinal chondrosarcoma resection in 2 studies are 17% and 27%, although its definition and follow-up is unclear. 17,18 We focused on postoperative morbidity, and found a higher overall complication rate (55%). Our reoperation rate (42%) was comparable to a previous study (44%). 18 Oncological outcome following surgical resection of mobile spine chondrosarcoma is comparable to previous studies.
This study had limitations. First, we consider the short clinical follow-up as the most important limitation; 30% had a follow-up less than 1 year. A minimum follow-up period of 3 years is required before drawing conclusions on oncological outcomes. 4 Hence, our oncological outcomes should be interpreted with some caution. A previous study by our research group reports oncologic outcomes after a minimum follow-up of 2 years. 5 Second, we had patient-reported outcomes for 70% of eligible patients. The 19 patients for whom we did not have patient-reported outcomes did not differ in age (P = .228), sex (P = .427), type of resection (P = .723), tumor grade (P = .316), complications (P = .428), readmissions (P = .723), and reoperations (P = .999). Therefore, we believe that our results can be extrapolated to our complete cohort. Third, we set the minimum follow-up for patient-reported outcomes at 6 months, although patients might need a longer recovery time after these extensive surgeries. Patients whose questionnaires were obtained between 6 to 12 months after surgery (21.4%, 3/14) did not have more complications (P = .258), readmissions (P = .999), and reoperations (P = .505). In addition, we did not find a correlation between follow-up duration and any of the patient0-reported outcome measures in our study (PROMIS–Physical Function: ρ = 0.21, P = .49, PROMIS–Pain Interference: ρ = −0.36, P = .23, EQ5D Quality of Life: ρ = 0.35, P = .24, Disability Index: ρ = −0.21, P = .50; by Spearman correlation); however, it should again be noted that the number of patients with patient-reported outcome measures is limited. Fourth, we did not collect preoperative patient-reported outcomes; future studies should assess both preoperative and postoperative patient-reported outcomes to assess changes due to surgery and also assess the recovery of patient-reported outcome measures over time (months to years) after surgery. Fifth—as in other studies 35 —we combined the NDI and ODI into one score, although there is literature supporting that there might be differences. 36 Sixth, although radiation for chondrosarcoma is controversial; there is some evidence that high-dose (photon and proton combined) radiation has an effect. 13 A recent study on spine chordoma demonstrates that patients who underwent preoperative radiation do better than postoperative radiation. We extrapolated this and use preoperative high-dose radiation in chondrosarcoma. Preoperative radiation also allows a more focused field of radiation involving gross tumor with only a small margin. 13 Seventh, this is a retrospective study including patients over a long time span and with a limited sample size, which is a result of the rarity of mobile spine chondrosarcoma (incidence of chondrosarcoma in the United States is 1 in about 200 000 per year, of which 4-10% is in the mobile spine). 43
Conclusion
Chondrosarcoma affects quality of life and physical function and its treatment frequently results in complications and reoperations. Our findings can be used to inform future patients about expected outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.