
Abstract
Study Design
Retrospective analysis of a Medicare database (2005 to 2012).
Objective
To study postoperative complication rates following thoracolumbar fusion for traumatic thoracolumbar fracture in patients with ankylosing spondylitis (AS) compared with patients without AS.
Methods
The PearlDiver database (2005 to 2012) was queried to examine postoperative complication rates in patients with AS undergoing posterior thoracolumbar fusion for thoracolumbar fracture (n = 968). Complication rates were compared with proportion-matched controls without AS undergoing the same procedure (n = 1,979). We examined and compared the incidence of death, postoperative infection, transfusion, venous thromboembolism, respiratory failure, pneumonia, myocardial infarction, urinary tract infection, and acute renal failure in each cohort within 90 days postoperatively.
Results
Patients with AS had significantly higher rates of surgical site infection (odds ratio [OR] 1.6, 95% confidence interval [CI] 1.2 to 2.2, p = 0.002), day-of-surgery transfusion rates (OR 1.5, 95% CI 1.3 to 1.8, p < 0.0001), respiratory failure (OR 1.8, 95% CI 1.3 to 2.5, p = 0.0006), pneumonia (OR 1.8, 95% CI 1.3 to 2.5, p = 0.0002), acute renal failure (OR 1.6, 95% CI 1.2 to 2.3, p = 0.005), and total medical complications (OR 1.5, 95% CI 1.2 to 1.9, p < 0.0001). Ninety-day mortality was not different between the two cohorts (p = 0.18).
Conclusions
Thoracolumbar fusion for thoracolumbar fracture in patients with AS is associated with increased rates of surgical site infection, transfusion, respiratory failure, pneumonia, and acute renal failure postoperatively compared with patients without AS. The level of evidence in this study was III.
Introduction
Ankylosing spondylitis (AS) is a rheumatologic disorder with a prevalence of 0.1 to 1.4%, 1 and it is known to be more common in males. 2 The natural disease course consists of widespread enthesis inflammation and ossification of tendon and ligament insertions. 3 Patients with AS often develop early sacroiliitis and eventual mobile spine manifestations secondary to inflammation of the ligaments spanning the vertebrae, resulting in the formation of syndesmophytes across disk spaces. As the disease continues to progress, patients lose spinal mobility secondary to bridging syndesmophytes, which fuse long vertebral segments. 4
From a clinical perspective, long stretches of fused vertebral segments act as lever arms during hyperextension of the spine. 5 This pathology leads to increased stress at the apex of the spine, increasing the propensity for fracture at that site. 6 Additionally, patients with AS have decreased bone mineral density compared with individuals without rheumatologic disorders, with a reported prevalence of osteoporosis between 19 and 61%.7–12
Low bone mineral density and altered spinal biomechanics in patients with AS result in a fracture risk that is three to four times that of subjects without the condition.13,14 The reported vertebral fracture incidence in this specific study population ranges from 0.4 to 18%,15–19 with most occurring in the cervical spine.20–22 Due to the high thoracolumbar spine fracture incidence present in this population, surgical spine stabilization methods are commonly used to treat patients with AS. However, the presence of a systemic rheumatologic condition presents increased risk of perioperative morbidity and mortality, given that patients with AS have an increased risk for cardiac conduction disturbances and pulmonary complications, among other sequelae intrinsic to the disease course.23–28
Furthermore, the current literature is limited to small, institutional studies that are insufficiently powered to accurately estimate the incidence of postoperative complications following spinal fusion for thoracolumbar fractures in patients with AS. The purpose of the present study was to utilize a national database to study postoperative complication rates following spinal fusion for thoracolumbar fracture in patients with AS compared with patients without AS. Our hypothesis was that patients with AS undergoing spinal fusion for thoracolumbar fracture would have significantly higher rates of most postoperative complications.
Materials and Methods
The PearlDiver Patient Records Database (www.pearldiverinc.com; PearlDiver Inc., Fort Wayne, Indiana, United States) was utilized for data acquisition. The database contains procedure volumes and demographics for patients with International Classification of Diseases, 9th Revision (ICD-9) diagnoses and procedures or Current Procedural Terminology (CPT) codes. A Medicare database within PearlDiver was utilized for the present study, which has over 100 million individual patient records from 2005 to 2012. Access to the database was granted by PearlDiver Technologies for the purpose of academic research, and the data was remotely accessed on a password-protected server maintained by PearlDiver.
Patients who underwent posterior thoracolumbar or lumbosacral fusion from 2005 to 2012 were identified using the following CPT and ICD-9 procedure codes: ICD-9 81.04, 81.05, 81.06, 81.07, and 81.08 and CPT 22612, 22630, 22633, 22842, 22843, and 22844. These patients' records were then queried for procedures performed for thoracolumbar fracture using ICD-9 diagnostic codes 805.2, 805.4, 806.2, 806.20 to 806.29, and 806.4. Patients with AS (ICD-9 720.0) who underwent thoracolumbar fusion for fracture were subsequently identified as the study cohort (968 patients). A control cohort was created from patients who underwent the same procedure without a diagnosis of AS for comparison purposes. The control cohort was matched to the study cohort by age, gender, diabetes mellitus, obesity, smoking, and chronic obstructive pulmonary disease by sequential randomization computational steps to create progressively more selective cohorts.
Each cohort was then queried for postoperative complications within 90 days and revision rates at 6 months, 1 year, 2 years, and after all follow-up after spinal fusion utilizing ICD-9 and CPT codes. The medical complications included myocardial infarction, respiratory failure, pneumonia, urinary tract infection, acute renal failure, and cerebrovascular accident. Surgical site infection and thromboembolism rates were also assessed. The online
Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated for each comparison between the two cohorts. Chi-square tests were calculated to determine the statistical significance, with p < 0.01 considered significant, given the large cohort sizes. For the purposes of matching, however, p < 0.05 was considered a significant difference that was unacceptable, given the necessity of creating matched groups for comparison.
Results
Nine hundred sixty-eight patients with AS were compared with a matched control group of 1,979 patients without AS. All patients were treated with thoracolumbar fusions for thoracolumbar fractures. The demographics for each cohort are summarized in
Demographics and comorbidities of matched cohorts
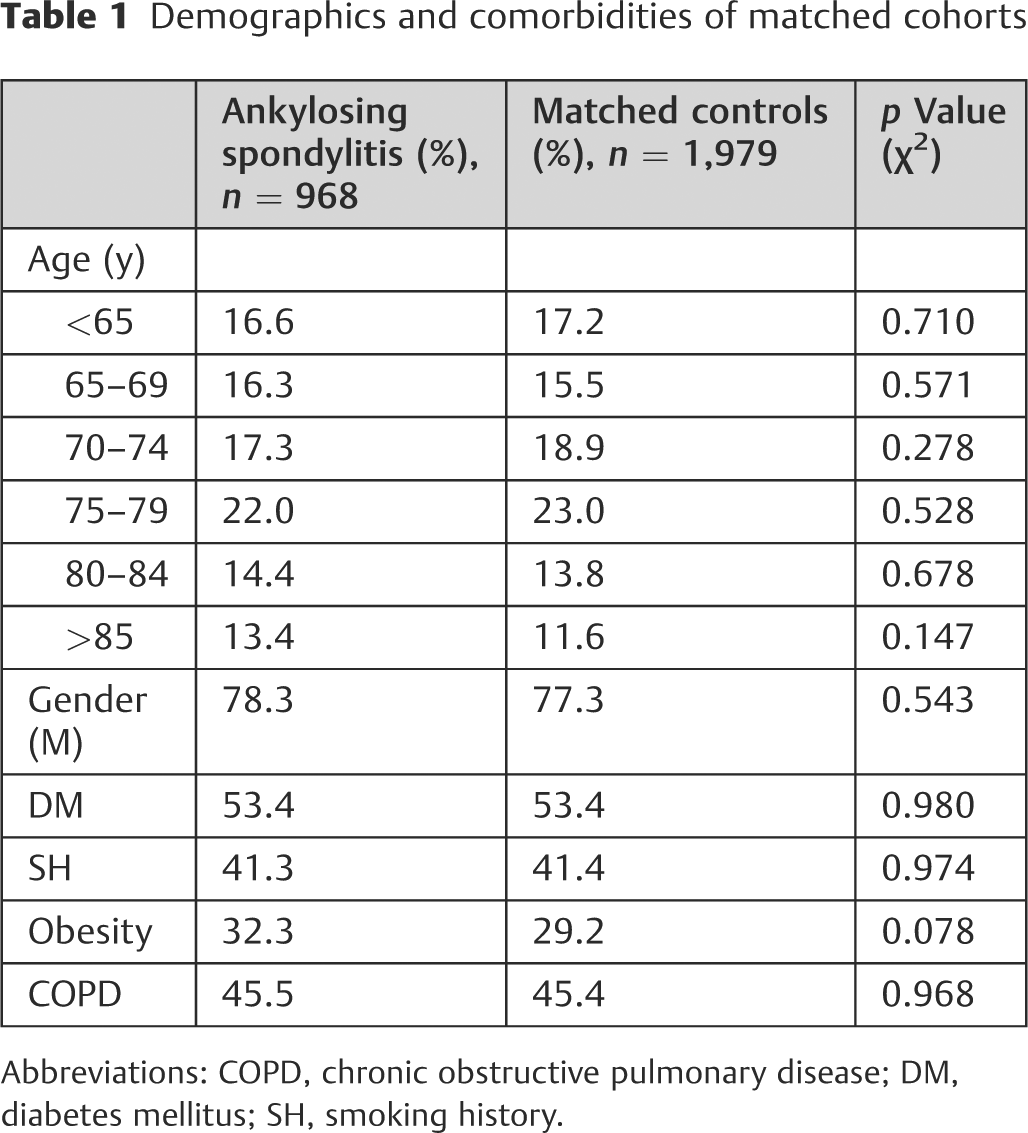
Abbreviations: COPD, chronic obstructive pulmonary disease; DM, diabetes mellitus; SH, smoking history.
When comparing the two cohorts, patients with AS had significantly higher rates of surgical site infection, day-of-surgery transfusion rates, respiratory failure, pneumonia, acute renal failure, and total medical complications. In patients with AS, there was a 7.7% rate of postoperative spinal infection compared with 4.9% in matched controls (OR 1.6, 95% CI 1.2 to 2.2, p = 0.002). On the day of surgery, 29.1% of patients with AS were treated with transfusions, compared with 21.3% of matched controls (OR 1.5, 95% CI 1.3 to 1.8, p < 0.0001). Respiratory failure, pneumonia, and acute renal failure were similarly more common (7.1, 7.7, 6.0%, respectively) in AS patients than controls (4.1, 4.4, 3.7%, respectively). Within the 90-day period following surgery, at least one of the assessed medical complications was present in 18.6% of patients with AS compared with 13.0% of matched controls (OR 1.5, 95% 1.2 to 1.9, p < 0.0001). When comparing thrombosis and embolism rates during the same period, there were no significant differences in incidence between the two groups (p > 0.10). Similarly, the revision rates assessed at 6 months, 1 year, 2 years, and after all follow-up were not significantly different (p > 0.10). The complication rates and statistical comparisons are provided in
Complications after fusion for thoracolumbar fracture
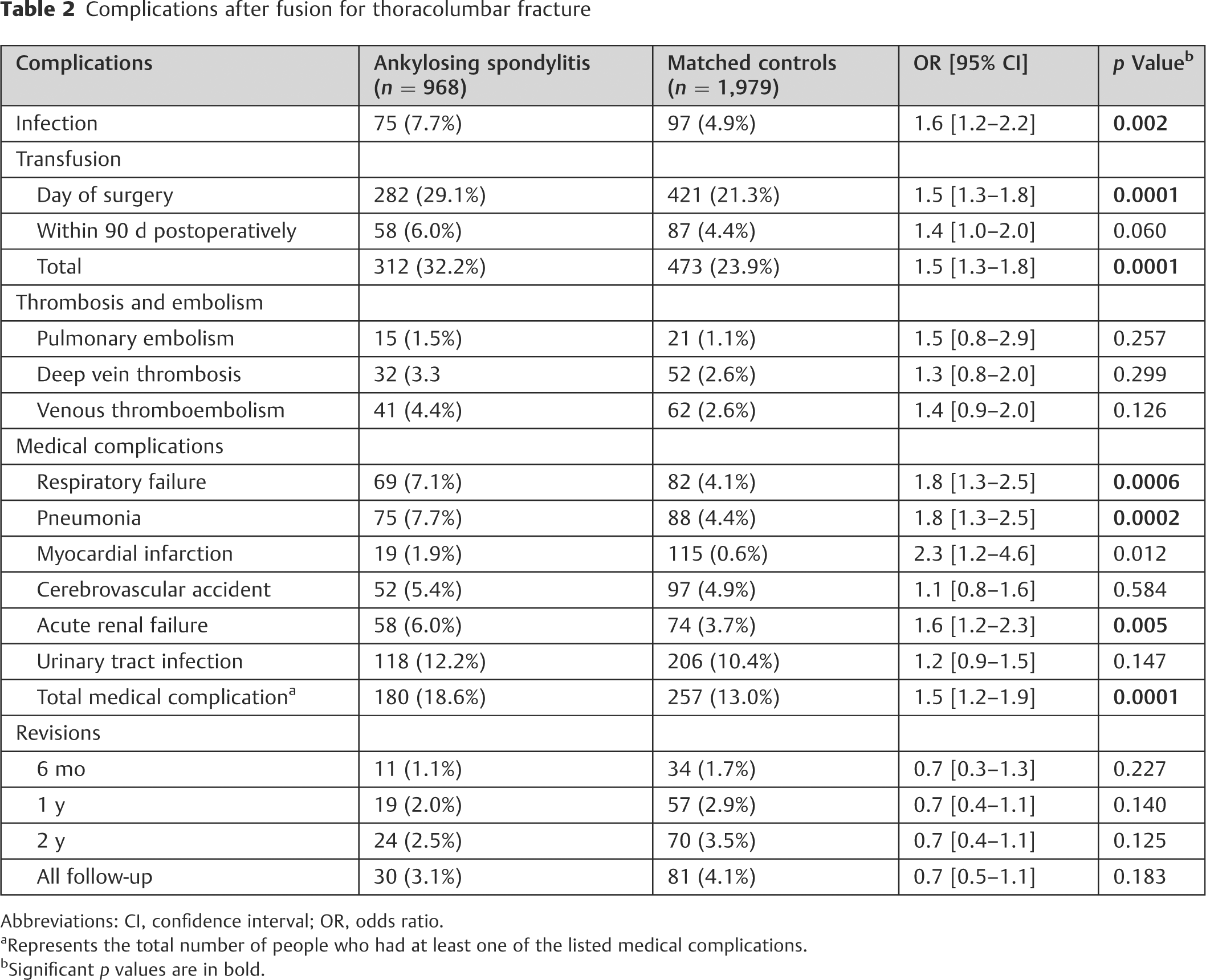
Abbreviations: CI, confidence interval; OR, odds ratio.
aRepresents the total number of people who had at least one of the listed medical complications.
bSignificant p values are in bold.
Discussion
The treatment of thoracolumbar spine fractures in patients with AS is a complex problem. Although closed treatment of three-column fractures has been reported, 29 due to the unstable nature of these fractures with the high association of neurologic injury, nonoperative management of these injuries is largely limited. A recent institutional review by Schiefer et al reported on 92 fractures in patients with diffuse idiopathic skeletal hyperostosis (DISH) or AS. In their series, bracing was chosen as the primary method of treatment in 27.1% of patients, with 52% of these patients failing nonoperative treatment and requiring subsequent surgery. 30 Other groups have also reported similar disappointing results with conservative bracing in this population.21,31 Furthermore, nonoperative treatment with bracing is associated with higher reported rates of mortality in this population. 32 Although it is known that this population is at increased risk for complications, the postoperative complication rates in patients with AS undergoing spinal fusion for fracture have been ill defined due to the small, institutional case series that have attempted to define them. As discussed, AS comprises a systemic rheumatologic disease, and patients, at baseline, carry an increased risk of cardiac and pulmonary complications postoperatively.23–28 It is of high clinical significance to characterize complication rates in this population undergoing fusion. The present study found that spinal fusion for thoracolumbar fracture in patients with AS is associated with significantly higher rates of numerous postoperative complications. In particular, the rates of transfusion, pneumonia, respiratory failure, surgical site infection, and acute renal failure were all significantly higher in patients with AS compared with those without.
Previous studies that have investigated surgical stabilization of spinal fractures in an AS population have been restricted to small case series and as a result have not been able to accurately describe trends in complication rates.33–36 However, several studies have examined the general population of patients with ankylosing spinal disorders, often grouping AS with DISH and other conditions. One such study by Caron et al reported on 112 consecutive patients with either AS (n = 28) or DISH. Although further analysis limits AS-specific data, 67% of all patients received surgical treatment and 84% of all patients experienced at least one complication. The reported medical and surgical complications in this study included infection, adverse pulmonary effects, urinary tract infection, deep vein thrombosis, and the need for either tracheostomy or percutaneous external gastrostomy tube. 32 A similar study by Westerveld et al compared the surgical outcomes between a group of 29 patients with either DISH or AS (n = 8) and 39 controls. Seven AS patients had at least one complication, and again wound infection and pulmonary complications were noted to be particularly prominent. 37 Wound infection and pulmonary complications were also noted in two case series with at least 20 patients, published by Sapkas et al 38 and Lu et al. 39 Of note, in the present study 7.7% of patients with AS contracted pneumonia during the postoperative period, and 7.1% of this cohort experienced respiratory failure. Patients with AS have decreased chest wall excursion and compliance that results in decreased vital capacity and possibly scarring and fibrosis at the top of the lungs. 26 The baseline pulmonary compromise present in this population likely contributes to the increased postoperative pulmonary complications demonstrated in the current literature. Surgical site infection was also observed in 7.7% of patients with AS. Other literature complications that have been reported include aortic dissection,40–43 aortic pseudoaneurysm, 44 and tracheal rupture. 45
The present study has several advantages. This study is the largest evaluating postoperative complications following spinal fusion for thoracolumbar fracture in patients with AS. By utilizing a national database, we are able to generate a large enough cohort to adequately power an analysis of postoperative complications and provide accurate estimates of complications that have yet to be reported in the current literature. Furthermore, this study offers a matched control cohort without AS, which helps to further delineate the complications inherently associated with performing spinal fusion in this population. By employing the PearlDiver database, this study allows tracking of patients to report 90-day postoperative complication rates following hospital discharge, in comparison with other databases such as the National Inpatient Sample, which only allows reporting of in-hospital complications.
This study also has several limitations, many of which are inherent to all studies utilizing a large administrative database such as PearlDiver. The power of our analysis is dependent on the quality of the available data, which includes the accuracy of billing codes and miscoding or noncoding by physicians as potential sources of error. Although we attempted to represent a cross section of a large population of interest within the United States, only Medicare data was included. We restricted the findings in our study to 90 days postoperatively to increase the likelihood that the complications were related to the postoperative management of the spinal fusion and not another medical or surgical condition that subsequently arose. Furthermore, late complications outside of this window are not captured in our data.
Conclusion
The treatment of thoracolumbar spine fractures in patients with AS is a complex problem. Although closed treatment of three-column fractures has been reported in this population, nonoperative management is largely limited. The present study demonstrates that patients with AS treated with thoracolumbar fusion for a thoracolumbar fracture have significantly increased rates of surgical site infection, transfusion, respiratory failure, pneumonia, and acute renal failure postoperatively compared with patients without AS. Patients with AS undergoing spinal fusion for thoracolumbar fracture should be appropriately counseled on the increased perioperative risk of the procedure.