
Abstract
Study Design
Systematic review and meta-analysis.
Objective
The objective of this meta-analysis was to evaluate the current best evidence to assess effectiveness and safety of recombinant human bone morphogenetic protein-7 (rhBMP-7) as a biological stimulant in spine fusion.
Methods
Studies were included if they reported on outcomes after spine fusion with rhBMP-7. The data was synthesized using Mantel-Haenszel pooled risk ratios (RRs) with 95% confidence intervals (CIs). Main end points were union rate, overall complications, postoperative back and leg pain, revision rates, and new-onset cancer.
Results
Our search produced 796 studies, 6 of which were eligible for inclusion. These studies report on a total of 442 patients (328 experimental, 114 controls) with a mean age of 59 ± 11 years. Our analysis showed no statistically significant differences in union rates (RR 0.97, 95% CI 0.84 to 1.11, p = 0.247), overall complications (RR 0.92, 95% CI 0.71 to 1.20, p = 0.545), postoperative back and leg pain (RR 1.03, 95% CI 0.48 to 2.19, p = 0.941), or revision rate (RR 0.81, 95% CI 0.47 to 1.40, p = 0.449). There was a mathematical indicator of increased tumor rates, but with only one case, the clinical meaningfulness of this finding is questionable.
Conclusion
We were not able to find data in support of the use of rhBMP-7 for spine fusion. We found no evidence for increased complication or revision rates with rhBMP-7. On the other hand, we also found no evidence in support of improved union rates.
Keywords
Introduction
Recombinant human bone morphogenetic proteins (rhBMPs) like rhBMP-2 and rhBMP-7 are known to promote bone formation and are being used to augment fusion in spine surgery as alternatives and adjuncts to autologous bone grafts. 1 Additionally, they provide the opportunity to eliminate donor site morbidity of harvesting bone graft. 2 , 3
In October 2001, the U.S. Food and Drug Administration (FDA) issued a Humanitarian Device Exemption (HDE) for the application of the rhBMP-7 as an alternative to autograft in recalcitrant long bone nonunions. 4 , 5 In parallel, studies were able to prove its efficacy as a valuable bone graft substitute in spine fusion in animals. 6 , 7 , 8 , 9 Hence, on April 7, 2004, rhBMP-7 approved by the FDA under a HDE for use as an alternative to autograft in medically compromised patients requiring revision posterolateral (intertransverse) lumbar spinal fusion as well. 10
Despite its published results and its ability to enhance spine fusion rates in animals and healing of long bone nonunions in humans without imposing additional risks, few studies investigated this protein in human spine applications. 3 , 5 , 8 , 11 , 12 Furthermore, its off-label use in primary posterolateral lumbar spine fusion and transforaminal lumbar interbody fusion (TLIF) has predominantly been published in the literature. In an epidemiologic study using national administrative data, 85% of rhBMP-7 use was off-label application in procedures such as TLIF, posterior lumbar interbody fusion, posterolateral lumbar spine fusion, and cervical fusion. 13
Few studies have reported on the potential increased adverse effects of using rhBMP-7. A few authors, such as Paramore et al, reported on the complications including intradural bone formation or calcification of the dura in dogs. The data on complications in human application of rhBMP-7 in spine fusion have only been published in an interspersed fashion in the literature. 14 , 15 , 16 , 17
Hence, the objective of this meta-analysis is to evaluate the current best evidence from the literature to assess the effectiveness and the safety profile of rhBMP-7 in spine fusion. The end points of this study are the union rate, the overall risk of complications, postoperative back and leg pain, the revision rate, and new onset of cancer with the use of rhBMP-7 compared with iliac crest bone graft (ICBG), local bone, or tricalcium phosphate (TCP) in spine fusion. Because this study depends on the published literature and its validity, a separate analysis of the quality of the included studies was performed as well.
Methods
We used a previously described search and analysis protocol following the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) and QUOROM (Quality of Reporting of Meta-Analysis) statements. 18 , 19
Studies were included if they reported on spinal fusion with rhBMP-7 and a minimum of 12 months of follow-up. To be included, the studies had to be controlled human trials reporting the union rate and complication rates. The exclusion criteria were duplicates, studies on rhBMP-2 or rhBMP in general, animal studies, and case reports.
Systematic Search and Strategy
We conducted a systemic search of the literature using the online databases PubMed, CINAHL, EMBASE, Cochrane Central Register of Controlled Trials (CENTRAL), and Cochrane Database of Systematic Reviews (CDSR) for relevant publications. The last search was performed on November 30, 2014.
The search algorithm was “(spine fusion) AND (BMP-7 OR bone morphogenetic protein OR osteogenic protein 1 OR OP-1) AND (complication OR adverse)” using keywords and MeSH (Medical Subject Headings) terms as well. All searches were unlimited (i.e., considering publications in all languages and at all dates).
Extraction of Relevant Data
Title and abstracts from all search results were screened for eligibility. Studies were excluded if title and/or abstract clearly refuted eligibility. The full texts were reviewed for all studies matching the inclusion criteria and all with unclear eligibility. All study selections were done independently in duplicate and cross-referenced. Disagreement was resolved by consensus.
Assessment of Study Quality and Data Validity
The internal validity of each study was further assessed with a modified Jadad scale, which assigns 1 point each for use of randomization, use of blinding, and reporting of attrition (with 0 points representing the worst possible result and 3 points representing the best result). 20
Publication Bias
An important problem that jeopardizes the validity of a systematic review is publication bias, also referred to as “file-drawer” bias. Studies often remain “in a file drawer” because their results are not statistically significant (or “negative”), resulting in an erroneously high proportion of studies with significant (or “positive”) results among published studies. Publication bias among the included studies was assessed graphically with a funnel plot and mathematically with the Egger weighted regression technique. 21
Study Heterogeneity
The presence of between-study heterogeneity was assessed qualitatively with the Cochrane Q test (with a p value of 0.10 to offset the low power of this test in small samples) and quantitatively with the I2 index. 22
Quantitative Data Synthesis
The data were pooled to calculate the pooled risk ratio (RR) and the pooled risk difference by constructing fixed-effects models. Such models postulate that the observed heterogeneity among the studies in a meta-analysis is attributable to normally distributed individual effects around a common effect. This assumption was assessed graphically with a forest plot. We calculated the Mantel-Haenszel pooled RRs with 95% confidence intervals (CIs). The Haldane continuity correction was used for zero cell values. 23 All calculations were performed with Intercooled Stata 10 (StataCorp, College Station, Texas, United States). A p value of 0.05 was considered significant for the pooled estimates.
Results
Study Characteristics
Our search strategy generated 796 studies online and one by citation tracking and hand searching. After exclusion of noncontrolled studies, studies not focusing on fusion or complications of rhBMP-7, and animal studies, six studies including 442 patients (328 experimental, 114 controls) remained for analysis. 16 , 17 , 24 , 25 , 26 , 27 The included studies were published between 2002 and 2010 in English. Fig. 1 shows the flow diagram.
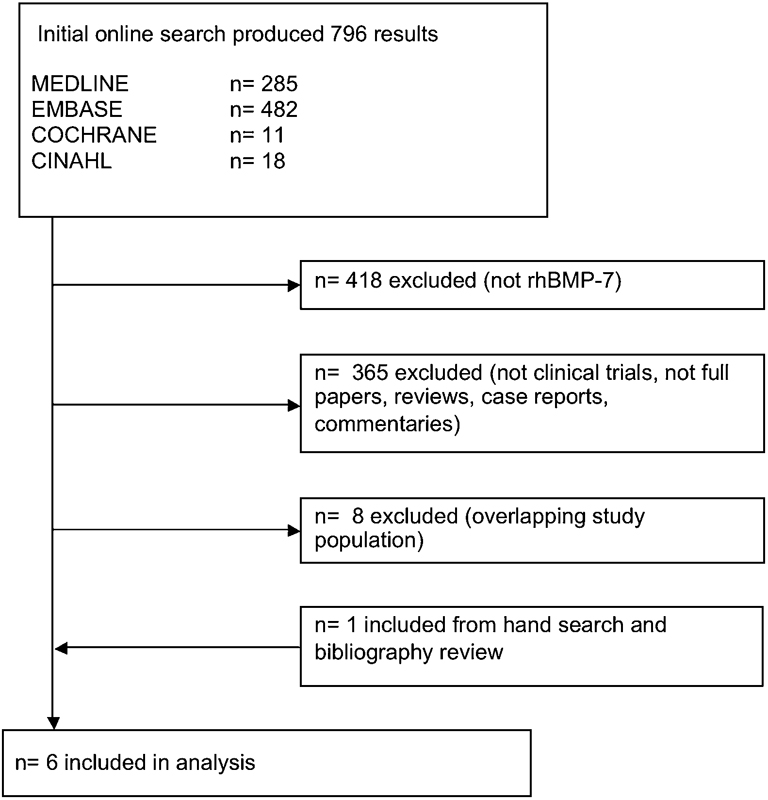
Flow diagram of the included trials. Abbreviation: rhBMP-7, recombinant human bone morphogenetic protein-7.
Description of Included Studies
Johnsson et al published a prospective randomized controlled study to evaluate the efficacy of rhBMP-7. 24 Twenty patients with L5 spondylolysis were divided into two even groups. Uninstrumented posterolateral spine fusion was performed with either rhBMP-7 (3.5 mg osteogenic progein-1 [OP-1] per side) or ICBG. Follow-up after 1 year showed good union rate (90% in the rhBMP-7 group, 100% in the control group). Radiostereometric three-dimensional motion analysis also demonstrated good segmental stability in both groups. No significant differences in persisting back pain (60% in the rhBMP-7 group, 50% in the control group) or revision rate (20% in the rhBMP-7 group, 10% in the control group) were observed. 24
Four years later, Kanayama et al investigated 19 patients with degenerative L3–L4 or L4–L5 spondylolisthesis who underwent posterolateral spine fusion performed with either hydroxyapatite-TCP granules (n = 10) or rhBMP-7 (n = 9, 3.5 mg OP-1 per side). 25 In plain radiographs and computed tomography (CT) scans, fusion was demonstrated in 7 of 9 patients using rhBMP-7 (77.8%) and 9 of 10 controls (90%). During elective, per protocol hardware removal, good bony union could only be confirmed in 4 of 7 (57.1%) of the rhBMP-7 group and 7 of 9 controls (77.8%). The histologic assessment demonstrated viable bone in 6 of 7 investigational patients (85.7%) and all 9 controls (100%). In the authors’ opinion, these results were not encouraging, and they recommended a modification of either surgical technique or carrier. 25
Vaccaro et al conducted a prospective, randomized, controlled, multicenter clinical study comparing rhBMP-7 with ICBG in uninstrumented posterolateral spine fusion. 27 Thirty-six patients with single-level degenerative lumbar spondylolisthesis (grade I or II) at L3–L4 or L4–L5 were randomized to either 3.5 mg OP-1 per side or fusion with ICBG. At the 4-year follow-up, dynamic and static radiographs showed a 68.8% union rate in the investigational group and a 50% union rate in the autograft group. Five cases of pseudarthrosis in the rhBMP-7 group were reported, one of which required revision surgery. Further, adverse events were observed in every single individual in this study, but in the authors’ opinion, none was device-related. 27
The same year, Vaccaro et al published a second, randomized controlled multicenter study including 295 patients with degenerative spondylolisthesis (grade I or II) with spinal stenosis at L3–L4, L4–L5, or L5–S1. 26 All patients underwent uninstrumented posterolateral fusion either with rhBMP-7 (n = 208) or autograft (n = 87). The patients were followed at 6 weeks and 3, 6, 9 12, and 24 months. At 36 months, 202 of the original patients (144 experimental patients and 58 controls) underwent CT and dynamic radiographic studies to assess union rate. The results showed rhBMP-7 to be a safe and effective alternative to ICBG. In plain radiographs, bridging bone was observed in 61.7% of the investigational patients versus 83.1% in the autograft group (p < 0.001). The CT scans showed the presence of new bone in 74.8% of the rhBMP-7 group and 77.4% of the ICBG group, which was not statistically significantly different (p = 0.852). After 24 and 36 months, the rhBMP-7 group experienced a higher proportion of patients without complications than the autograft group, but this difference also was not statistically significant (p = 0.863 and 0.387, respectively). Twenty-one patients in the rhBMP-7 (8.2%) group and 1 in the autograft group (13%) required revision at the index level, but again, this difference was not statistically significant. The investigators concluded that rhBMP-7 is comparable to ICBG and is an effective alternative for PLF. 26
Leach and Bittar in 2009 investigated 123 patients who underwent anterior cervical interbody fusion using rhBMP-7 together with TCP and compared this study group to eight control patients who were treated with TCP alone. 16 Only a slight increase of anterior cervical swelling causing brachialgia, dysphagia, and dysphonia was observed in the investigational group. The authors concluded that rhBMP-7 could be used safely in anterior cervical fusion surgery. 16
In 2010 Delawi et al reported on 36 patients with degenerative or isthmic spondylolisthesis at L3–S1 who underwent single-level instrumented posterolateral lumbar fusion. 17 One group received rhBMP-7 (3.5 mg per side) combined with local allograft (bone from laminectomy), and the controls were fused with ICBG. The union rate was 63% in the experimental group and 67% in the ICBG group (p = 0.95). Adverse events were reported in both groups: 44% in the ICBG group and 56% in the rhBMP-7 group. In the experimental group, one case of new-onset cancer (grade IV glioblastoma) was diagnosed. The authors considered rhBMP-7 as effective as ICBG in posterolateral fusion without the morbidity of harvesting. 17
Union Rate with rhBMP-7
The data on union rate were available from five studies including a total of 294 patients (195 in the rhBMP-7 group, 99 in the control group). There was no evidence for publication bias (p = 0.355) among these publications as well as no evidence for mathematical heterogeneity (p = 0.742, I2 < 1%). The pooled, fixed-effects RR for union was 0.97 (95% CI 0.84 to 1.11), which is not significantly different (p = 0.247; Fig. 2).
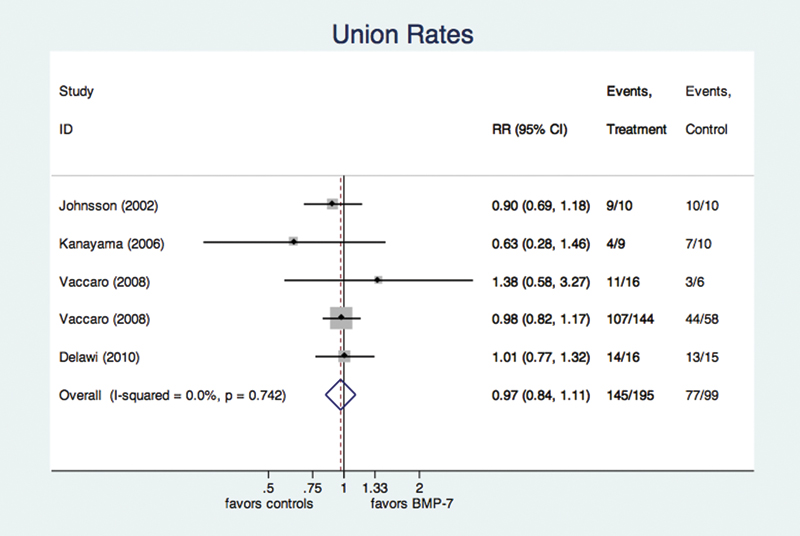
Forest plot for union rate. Risk ratios (RRs) are given with 95% confidence interval (CIs) for the individual studies as horizontal black lines, and the pooled RR as a diamond at the bottom. The vertical black line represents a rate ratio of 1, or no difference between groups. The dashed, vertical line represents the pooled estimate given as a blue diamond in the graph. The overall estimate is given with the I2 estimate for heterogeneity and the p value for the pooled estimate (see text for further explanation). Counts for both groups are given in the right-most columns. The size of the gray square represents the individual weight of a study, based on sample size. The forest plot reveals no significant increase in union rates in the recombinant human bone morphogenetic protein (BMP)-2 group. The I2 estimate showed no evidence for mathematical heterogeneity.
Overall Complication Rate
The data on the overall rate of complications were available from four studies including a total of 406 patients (311 in the rhBMP-7 group, 95 in the control group). There was also no evidence for publication bias (p = 0.723) among these publications, as well as no evidence for mathematical heterogeneity (p = 0.323, I2 = 13.9%). The pooled, fixed-effects RR for overall complications was 0.92 (95% CI 0.71 to 1.20) and was not significantly higher in the rhBMP-7 group (p = 0.545; Fig. 3). Table 1 gives an overview of those complications that were reported individually and not in aggregated form. Of note, there is some overlap because different studies used different terminology for similar complications.
Complications
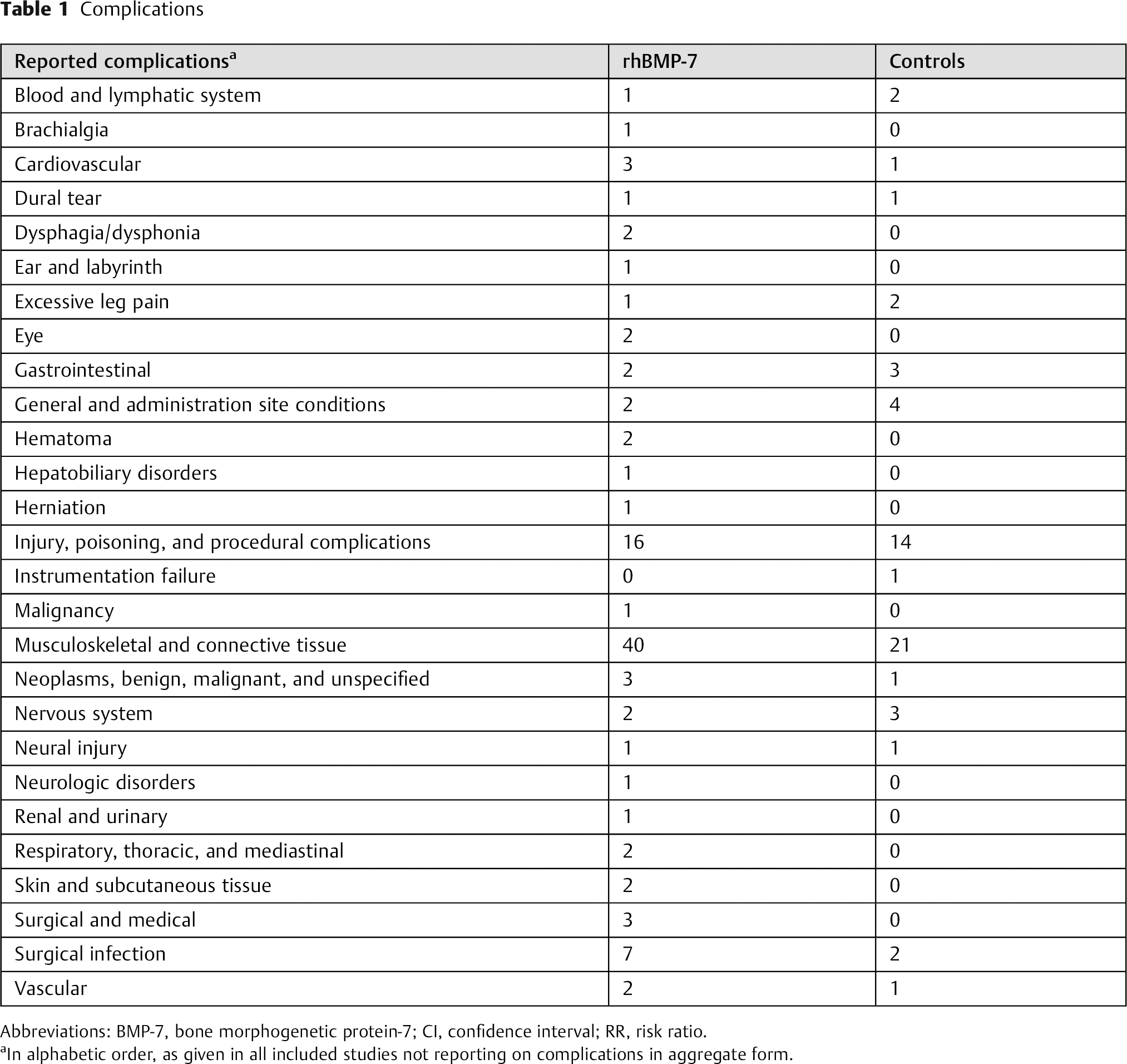
Abbreviations: BMP-7, bone morphogenetic protein-7; CI, confidence interval; RR, risk ratio.
In alphabetic order, as given in all included studies not reporting on complications in aggregate form.
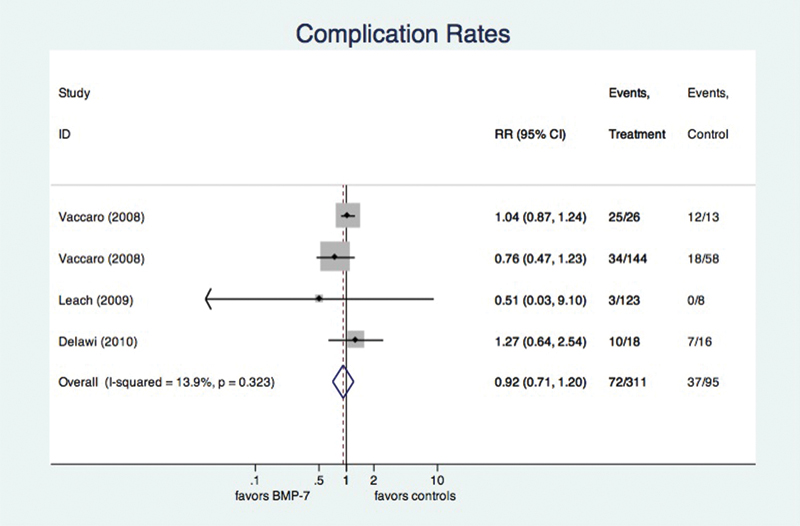
Forest plot for complication rate. A full explanation of the forest plot is given in the caption for Fig. 2. Our analysis revealed no difference in the overall rate of complications. The I 2 estimate showed roughly 14% of mathematical heterogeneity, which is not consistent with a statistically significant result (see text). Abbreviations: BMP-7, bone morphogenetic protein-7; CI, confidence interval; RR, risk ratio.
Rate of Postoperative Back and Leg Pain
The data on rates of postoperative back and leg pain were available from four studies including a total of 111 patients (62 in the rhBMP-7 group, 49 in the control group). There was also no evidence for publication bias (p = 0.727) among these publications as well as no evidence for mathematical heterogeneity (p = 0.868, I2 < 1%). The pooled, fixed-effects RR for rate of postoperative back and leg pain was 1.03 (95% CI 0.48 to 2.19), which again does not indicate a significantly higher risk in the rhBMP-7 group (p = 0.941; Fig. 4).
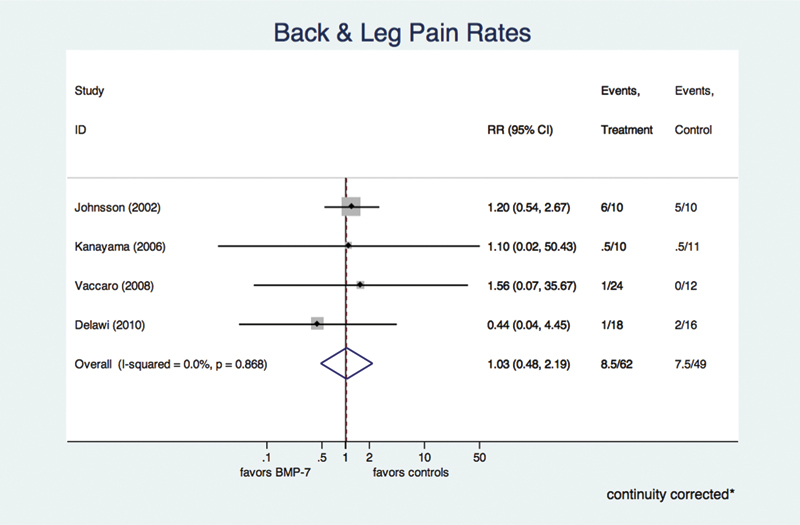
Forest plot for postoperative back and leg pain. Again, a full explanation of the forest plot is given in the caption for Fig. 2. Our analysis revealed no difference in the rate of postoperative back and leg pain. The I 2 estimate showed no evidence for mathematical heterogeneity. Abbreviations: BMP-7, bone morphogenetic protein-7; CI, confidence interval; RR, risk ratio.
Revision Rates
The data on revision rates were available from three studies including a total of 258 patients (178 in the rhBMP-7 group, 80 in the control group). There was evidence for publication bias (p = 0.004) among these publications. However, there was no evidence for mathematical heterogeneity (p = 0.470, I2 < 1%). The pooled, fixed-effects RR for revision rate was 0.81 (95% CI 0.47 to 1.40), indicating no significantly higher risk of revision surgery in the rhBMP-7 group (p = 0.449; Fig. 5).
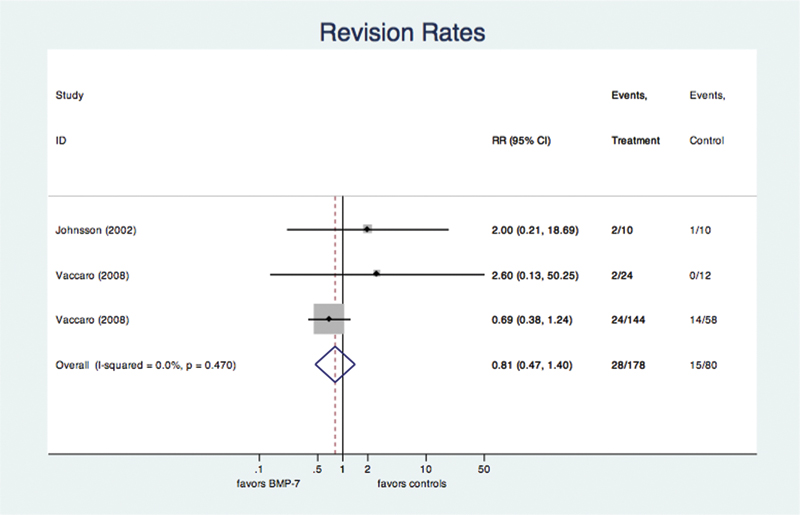
Forest plot for revision rate. Again, a full explanation of the forest plot is given in the caption for Fig. 2. Our analysis revealed no benefit of BMP-7 in reducing revisions. Abbreviations: BMP-7, bone morphogenetic protein-7; CI, confidence interval; RR, risk ratio.
New Onset of Tumor
This subject found only one controlled trail reporting on a single case of new onset of cancer. A grade IV glioblastoma was diagnosed 11 months after surgery with rhBMP-7 in a group of 18 patients, compared with none in a group of 16 controls. 17 Using the Haldane correction for zero cells, this result equates to an estimated RR of 2.6 (95% CI 0.12 to 61.59).
Study Quality and Risk of Bias
Of the six included studies, five reported randomized patient allocation. Five reported on attrition (i.e., on the loss of patients during the course of the study) and had less than 20% attrition. Five studies reported on blinded outcome assessment. The mean Jadad score was 2.5 points (95% CI 1.8 to 3.2). 20
Discussion
Summary of Evidence
The objective of this meta-analysis was to evaluate the current best evidence from the literature to assess effectiveness and safety of rhBMP-7 as a biological stimulus in spine fusion. The end points of this study were the union rate, the overall risk of complications, postoperative back and leg pain, the revision rate, and new onset of cancer with the use of rhBMP-7 compared with ICBG, local bone, or TCP in spine fusion.
Our data showed no significant difference in union rate using 3.5 mg of rhBMP-7 on each side of the spine compared with ICBG, local bone, or TCP. Recent longitudinal cohort studies corroborate our findings. In 2007, Furlan et al assessed rhBMP-7 in 30 patients with potential risks of pseudarthrosis undergoing cervical and lumbar fusion surgery. After 24 months, the authors confirmed an 80% radiographic union rate as well as a significant improvement of physical health, 28 which is in alignment with our findings. Govender et al showed similar results in nine patients who also showed risks for nonunion. 3 Using rhBMP-7, the authors showed solid union in all nine patients after 3 months and considered rhBMP-7 to be a safe and effective alternative in promoting fusion in patients with adverse medical risk factors for nonunion. 3 However, neither of these studies had a control group.
In contrast to these findings, Laursen et al presented disappointing union rates in five patients who were augmented with rhBMP-7 as an intracorporeal bone graft stimulator in thoracolumbar burst fractures. 29 The results showed that this osteogenic protein was incapable of inducing an early sufficient structural bone support. On the contrary, all the cases failed to heal and even severe bone resorption could be observed. 29 Jeppsson et al also reported a poor union rate, showing bridging bone in C1–C2 in only 1 of 4 patients with rheumatism treated with 2.5 mg of rhBMP-7. 30 However, assessing the role of oral corticosteroid medication as a culprit, the authors were able to show that prednisolone did not inhibit union with rhBMP-7 in rats. 30 Again, our data showed no significant difference in union rate using 3.5 mg of rhBMP-7 on each side of the spine compared with ICBG, local bone, or TCP and hence are consistent with previous studies in the recent literature.
Furthermore, we investigated the complication rates of using rhBMP-7 compared with ICBG, local bone, or TCP in spine fusion. In the recent literature, the use of rhBMPs has been associated with ectopic bone formation, carcinogenicity, antibody formation, and bone resorption. 31 It should be noted that less data exists investigating the safety profile of rhBMP-7 than of rhBMP-2. 32 Our data showed no significant difference in the RR for overall complications using rhBMP-7. Recent publications confirm these findings. Furlan et al reported asymptomatic heterotopic ossification of the soft tissue after successful occipitocervical fusion as well as two superficial wound infections that were treated with wound revision and antibiotics. In their opinion, these adverse events were not related to the use of rhBMP-7. 28 In 2010, Kim et al reported excessive ectopic bone formation to the left superior pubic ramus extending through the left rectus sheath and into the left psoas muscle after having performed anterior and posterior reconstruction surgery using rhBMP-7. No local recurrence after revision surgery was reported. 33 Our analysis was not able to assess the differences between the investigational and the control groups regarding ectopic bone formation, as no controlled studies exist investigating this specific complication.
Another severe complication is the onset of new cancer. In 2004, the FDA reported on seven patients who were diagnosed with new onset of cancer after treatment with rhBMP-7. Six of these seven cases were nonosseous cancers in elderly patients, and the other was recurrence of a chondrosarcoma. 34 To our knowledge, only one controlled study reported on one case of new-onset cancer after the specific use of rhBMP-7 in spine fusion. Delawi et al published this case of new diagnosis of a grade IV glioblastoma 11 months after lumbar fusion with 3.5 mg of rhBMP-7. There is no follow-up data as the patient refused to be part of the study any longer. 17 We did analyze this study by Delawi et al and were able to show a mathematical indicator of increased tumor rates, but with only a single case, the clinical meaningfulness of this finding remains questionable. As we identified in our query only the one study mentioning cancer as a complication, we were not able to do any further meta-analysis on this topic.
In our analysis, we did not include antibody formation as a complication because of unproven clinical impact. 34 Hwang et al conducted a controlled, multicenter study on 336 patients who underwent decompression and uninstrumented posterolateral spinal arthrodesis with either rhBMP-7 or ICBG. The results showed that rhBMP-7 induced an immune response, but also showed that this effect was only temporary and decreased over time. The building of neutralizing anti-OP-1 antibodies did not affect the complication rate. 35 Vaccaro et al showed similar results in proving no significant associations between neutralizing activity status, clinical success, and adverse events. 26 Because of unproven sequelae, we excluded this topic in our analysis. Our data showed no significant difference in the RR for overall complications using rhBMP-7 compared with ICBG, local bone, or TCP.
We also assessed the rate of postoperative back and leg pain. Our results showed no significant difference between the groups. Johnsson et al reported on postoperative back pain at the 1-year follow-up in 60% of patients receiving rhBMP-7. Revision surgery had to be performed because of persisting back or leg pain in two patients using rhBMP-7 and in one control patient. 24 Vaccaro et al reported on 1 of 36 patients who developed excessive back pain after surgery with rhBMP-7. Revision surgery had to be performed. 27
Finally, we analyzed the revision rates across the groups. Our data showed no statistical difference in revision rate between the use of rhBMP-7 and the use of ICBG, local bone, or TCP. We did find some evidence for publication bias (p = 0.004) among these publications, indicating that revisions might not have been included as an end point in all studies. Vaccaro et al did report revision rates of 8.2% in the patients using rhBMP-7 compared with 13% in the autograft group for pseudarthrosis. 26 In their second study in 2008, 27 the authors demonstrated an even lower revision rate. Only one investigational patient showed a symptomatic pseudarthrosis that was treated with a TLIF. Of note, the other four cases of pseudarthrosis of the rhBMP-7 group did not have to undergo salvage procedure. In contrast, Furlan et al reported a 13.3% revision rate after using rhBMP-7 due to a hardware problem. Additionally, there were two superficial wound infections that required surgical intervention. 28
Limitations
The most important shortcoming of any meta-analysis is its dependence on the data extracted from the primary studies. In our case, although not abundant in number, the included studies showed high levels of quality, reflecting in high Jadad scores.20 Also, we found no evidence for mathematical heterogeneity, a fact that is a strong indicator for a true biological effect. Finally, confidence intervals were very narrow, suggesting only little variability in surgical outcomes.
Another big shortcoming of studies like ours is clinical heterogeneity (i.e., meaningful differences in treatment regimens that are not always described with unequivocal clarity). The studies at hand commendably invested a considerable amount of effort in describing type, technique, and dosage of rhBMP-7, helping us to better understand where they were similar and where they were not. However, it should be pointed out that Leach and Bittar reported on cervical fusion and all others reported on lumbar fusion. 16 However, every single mathematically included study reported on off-label use as no study protocol was consistent with the FDAs HDE for rhBMP-7 application. But because we wanted to focus on systemic effects, or rather side effects of rhBMP-7, we chose to pool the data nevertheless.
Conclusion
In conclusion, we were not able to find data in support of the use of rhBMP-7 for spine fusion. We found no evidence for increased complication or revision rates with rhBMP-7. On the other hand, we also found no evidence in support of improved union rates. There was a mathematical indicator of increased tumor rates, but with a single case, the clinical meaningfulness of this finding is questionable.
Disclosures
Julia Vavken, none
Patrick Vavken, none
Alexander Mameghani, none
Stefan Schaeren, none