
Abstract
Study Design:
Review of the literature.
Objectives:
Anterior column realignment (ACR) is a powerful but relatively new minimally invasive technique for deformity correction. The purpose of this study is to provide a literature review of the ACR surgical technique, reported outcomes, and future directions.
Methods:
A review of the literature was performed regarding the ACR technique. A review of patients at our single center who underwent ACR was performed, with illustrative cases selected to demonstrate basic and nuanced aspects of the technique.
Results:
Clinical and cadaveric studies report increases in segmental lordosis in the lumbar spine by 73%, approximately 10° to 33°, depending on the degree of posterior osteotomy and lordosis of the hyperlordosis interbody spacer. These corrections have been found to be associated with a similar risk profile compared with traditional surgical options, including a 30% to 43% risk of proximal junctional kyphosis in early studies.
Conclusions:
ACR represents a powerful technique in the minimally invasive spinal surgeon’s toolbox for treatment of complex adult spinal deformity. The technique is capable of significant sagittal plane correction; however, future research is necessary to ascertain the safety profile and long-term durability of ACR.
Keywords
Introduction
Adult spinal deformity (ASD) has a high prevalence in the elderly population, such that surgical management of ASD has increased 3.4-fold among patients 60 years of age or older from 2004 to 2011. 1 ASD prevalence in a volunteer adult population with an age greater than 60 years was found to be 68% in a recent epidemiologic study. 2 Surgical correction of deformity has been found to dramatically improve quality of life in patients with ASD; in particular, sagittal balance had been found to demonstrate a linear relationship with the severity of symptoms and impairment of the quality of life. Sagittal realignment is therefore critical to maximally improve surgical and quality-of-life outcomes. 3 -5 Traditionally, surgical correction of ASD has been performed with use of a posterior open approach.
However, in recent decades, several advances have been achieved in surgical treatment of ASD through minimally invasive surgery (MIS) approaches. In the past, MIS techniques have been useful in the restoration of coronal balance but have been more limited in achieving sagittal correction. Anterior column realignment (ACR) represents a relatively new MIS technique for treatment of sagittal imbalance that provides significant correction of segmental lordosis comparable to that achievable via pedicle subtraction osteotomy (PSO). ACR consists of anterior longitudinal ligament (ALL) release with partial anterior annulotomy and anterolateral discectomy via a lateral transpsoas surgical corridor (Figure 1). 6,7 Combining the benefits of indirect ALL release and hyperlordotic lateral cage placement, ACR can significantly restore sagittal balance with use of minimally invasive techniques or minimally invasive techniques that serve as an adjunct to traditional open approaches.
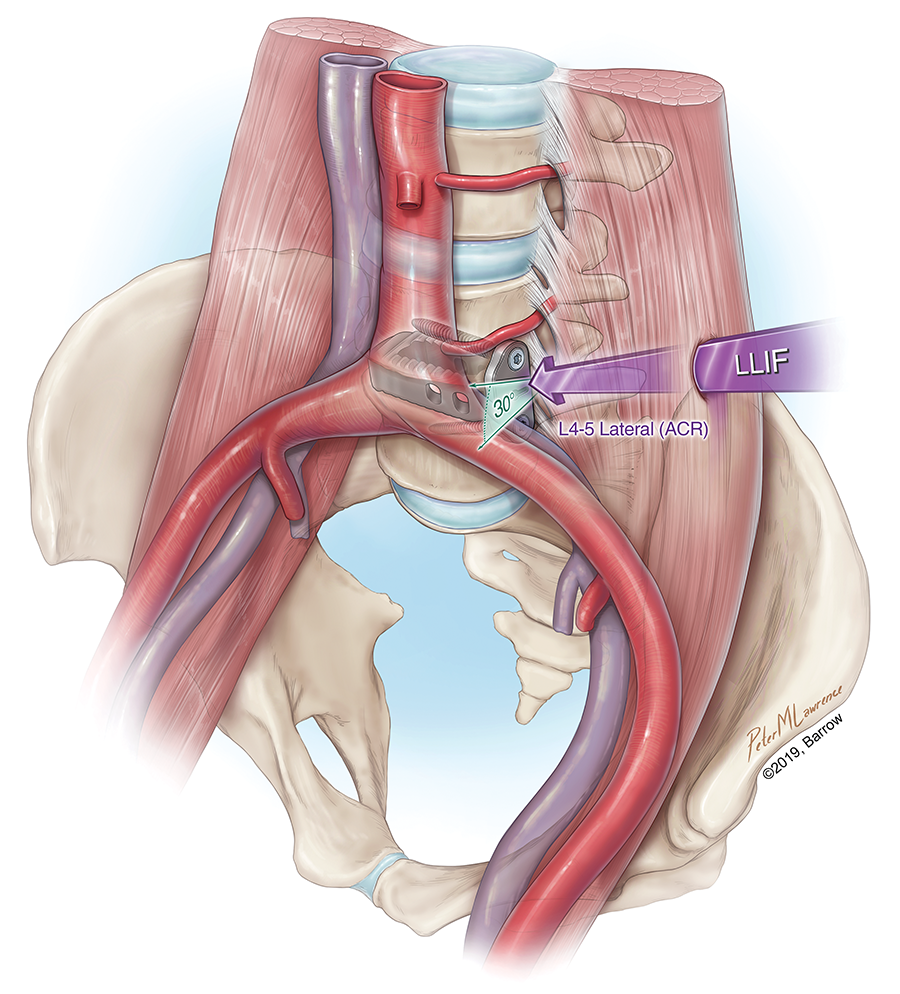
Illustration of the transpsoas approach to the anterior column realignment (ACR) technique. The L4-5 disc space is approached via a transpsoas corridor (arrow), posterior to the great vessels and inferior to segmental arteries and veins. A hyperlordotic interbody cage is placed (20° to 30°) with superior and inferior 2-screw anterolateral plate fixation. LLIF, lateral lumbar interbody fusion. Illustration used with permission from Barrow Neurological Institute, Phoenix, Arizona.
Outcomes
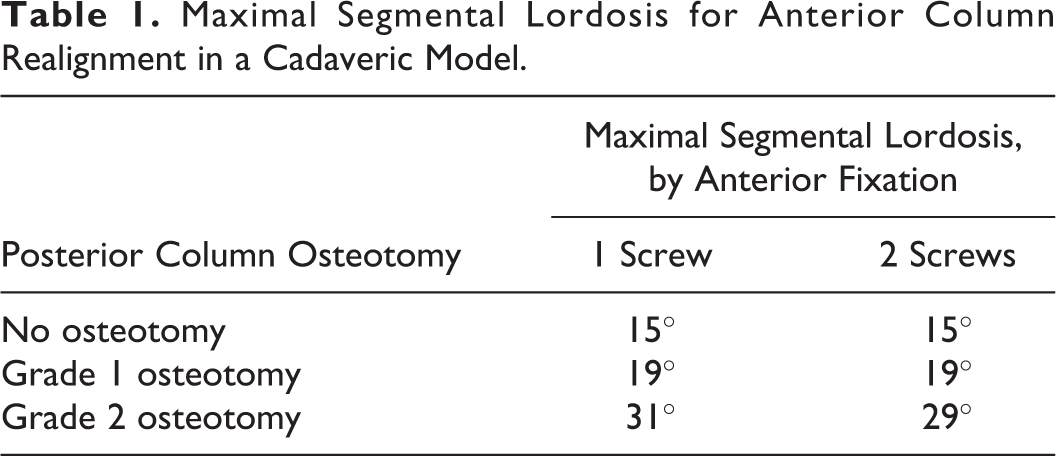
ACR can effectively restore lumbar lordosis (LL) and thereby significantly improve spinopelvic mismatch. 8,9 Complimentary posterior column osteotomies (PCOs) may be performed to increase the amount of segmental lordosis possible during ACR. 10 The amount of lordosis gained varies according to the angle of the cage used and the extent of adjunct PCO. According to the Schwab osteotomy classification system, grade I osteotomy consists in resection of the inferior facet and entire joint capsule at a given spinal level. 11 Grade II consists of removal of both inferior and superior facets of an articulation at the index level as well as the flavum ligament; other posterior elements of the vertebra, including the lamina and the spinous processes, can also be removed. 12
With the posterior elements intact, ACR can result in an increment of 10° in segmental lordosis. 13 A multicenter analysis reported that the addition of PCO to an ACR increased the segmental lordosis gain by 72.7%. 10 Grade I osteotomy can lead to 21° to 27° of angle change in segmental lordosis, whereas grade II osteotomy can afford segmental LL to match the cage lordosis, in this case 32° to 33° when a 30° cage is used. 13 In different studies, the increase in overall LL with a single-level ACR ranges from 25° to 27°. 14,15 The traditional 3-column osteotomy, or PSO, has been used as a gold standard tool for sagittal realignment and yields approximately 25° to 30° of lordosis restoration. Several studies have demonstrated similar radiographic outcomes in matched cohorts of patients with ACR versus PSO. 16 Notably, there is significant variability across procedures for ACR in terms of location, interbody choice, and technique for posterior fixation and arthrodesis. Authors have described both percutaneous and open approaches, and the influence of this on lordosis and complication rates is not well delineated in the literature.
Biomechanics
From a biomechanical perspective, the ACR is highly destabilizing due to ALL release but also facilitates the placement of a large-footprint lordotic invertebral device. It is critical to emphasize that the ALL provides significant stability in extension and has contributions during lateral bending and axial rotation. 17 As a result, the requisite ALL transection significantly reduces the stability of the spine. 8 This instability may, to a certain extent, be counteracted by the addition of a hyperlordotic interbody device (anterior column lengthening), anterolateral fixation via plating, and posterior segmental fixation. 18
Nonetheless, it is likely that the ACR holds a theoretical advantage in terms of biomechanical stability and rod protection compared with open techniques due to stress reduction and anterior load-sharing capacity. The combination of the wide-footprint intervertebral support, anterolateral plate fixation, and the anterior lengthening effect of ACR may ultimately grant improved stability and facilitate load-bearing capacity through the anterior column. 18 Earlier finite element modeling studies have suggested an inherent biomechanical advantage of the ACR construct over a PSO deformity construct. In their study, Januszewski et al 19 found that the anterior lengthening approach of ACR results in less acute rod bending and may contribute to decreased posterior rod strain. This can be compared with a lack of anterior lengthening effect and the posterior shortening feature of the PSO, which leads to hyperacute sharp-contoured posterior rods, as opposed to ACR, and makes it more vulnerable to rod fracture because of the strain concentration. A recent study investigating the risk of rod fracture across ACR constructs demonstrated a 4% rate of rod fracture with 1-year follow-up, potentially representing a lower risk of rod fracture. 20 However, to date no cadaveric biomechanical studies of ACR have been performed to corroborate these findings.
Target/Patient Selection
Although ACR is an MIS technique that is growing in popularity with the capacity for significant sagittal correction, it is important to keep in mind the limitations of this procedure. Appropriate patient selection remains paramount in regard to patient safety and health outcomes. Several publications have suggested treatment algorithms for approaching the management of ASD with MIS techniques. 21 The ACR technique, while capable of significant sagittal plane correction, is limited to free segments and is constrained by lumbosacral plexus anatomy and risk of neurological deficit from direct trauma or retraction injury.
Those patients with severe deformity are less likely to achieve restoration of sagittal alignment and clinical improvement. 22 Patients with mild to moderate sagittal deformity are candidates for ACR, while those with fixed or severe deformity are typically not considered surgical candidates for ACR (Figure 2). The minimally invasive spinal deformity surgery algorithm has suggested that treatment with MIS benefits patients who meet the following parameters: LL-PP mismatch less than 30°, pelvic tilt less than 25°, thoracic kyphosis less than 60°, sagittal vertical axis less than 6 cm, and Cobb angle less than 20°. 21 Patients who have sagittal vertical axis of more than 6 cm but flexible curves are also candidates. Restoring LL and sagittal balance also takes precedence over scoliosis correction during ASD surgery. 23
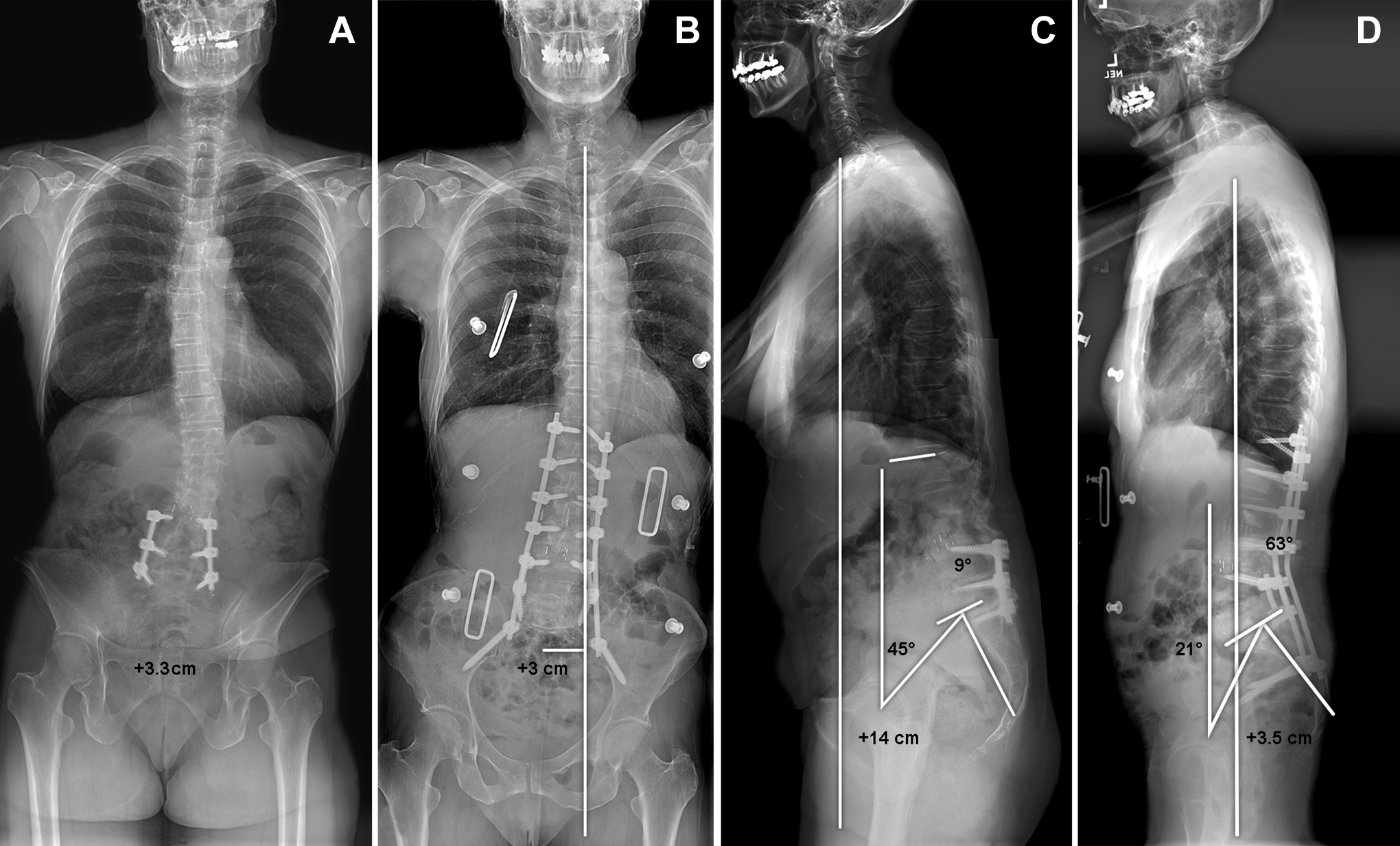
Preoperative (A) and postoperative (B) anteroposterior and preoperative (C) and postoperative (D) lateral standing radiographs showing use of a minimally invasive approach for adult spinal deformity in a patient with significant sagittal imbalance and spinopelvic mismatch. The patient underwent a multilevel lateral interbody fusion with anterior column realignment at the adjacent free level with inferior mini-open pedicle subtraction osteotomy with posterior percutaneous pedicle screw fixation. Postoperative radiographic imaging (right) demonstrates improved sagittal balance with resolution of spinopelvic mismatch. A persistent coronal imbalance is observed postoperatively, without effect on patient quality of life. Used with permission from Barrow Neurological Institute, Phoenix, Arizona.
Evaluation for appropriateness, including thorough preoperative radiographic assessment, is necessary to ascertain the working surgical corridor at the level of interest in terms of vascular, neurological, and bony anatomy. Imaging modalities, such as computed tomography (CT) and magnetic resonance imaging (MRI), can provide information regarding the anatomy of the great vessels, segmental vessels (that may preclude safe docking of retractor or annular release contralaterally), or potentially scarred vessels to annulus. Notably, a preoperative MRI provides reliable information about the location of the vessels anterior and the lumbar plexus (Figure 3). Patients with ASD may have displacement of the psoas muscle and the surrounding neurovascular structures. Additionally, we recommend evaluation of segmental vasculature on sagittal MRI to identify large segmental arteries or veins across the disc space that may represent a surgical bleeding risk.
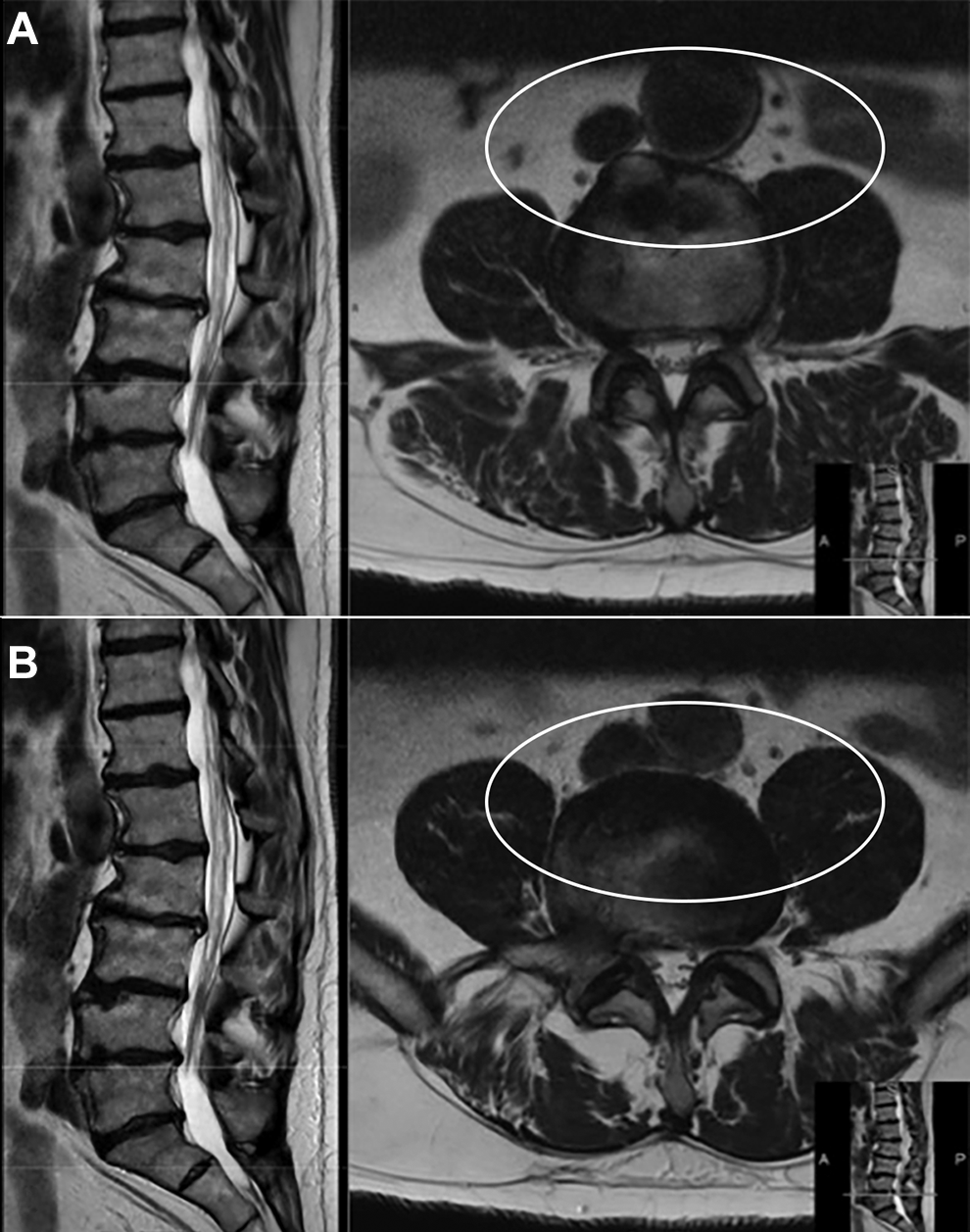
Preoperative T2-weighted magnetic resonance imaging (MRI) sequence lateral (left) and axial (right) views at the L3-4 (A) and L4-5 (B) levels. Axial MRI shows unfavorable vascular anatomy across the adjacent disc spaces of interest (oval). The lack of a clear hyperintense border around the vessel is concerning for scarring or adherence that would make mobilization of the great vessels a high-risk procedure. Such a finding necessitates an alternative approach. Used with permission from Barrow Neurological Institute, Phoenix, Arizona.
Contraindications for ACR are shared with any lateral transpsoas approach. These include a history of retroperitoneal surgery, presence of scar tissue on this region, and evidence of fusion across the disc space (Figure 4). Patients should undergo bone-quality evaluation with dual-energy X-ray absorptiometry before ACR. Severe osteopenia and osteoporosis, with a T-score less than −2.0 at the femoral neck, should also contraindicate lateral ACR, because intervertebral subsidence represents an important concern and can cause failure of the treatment. 12
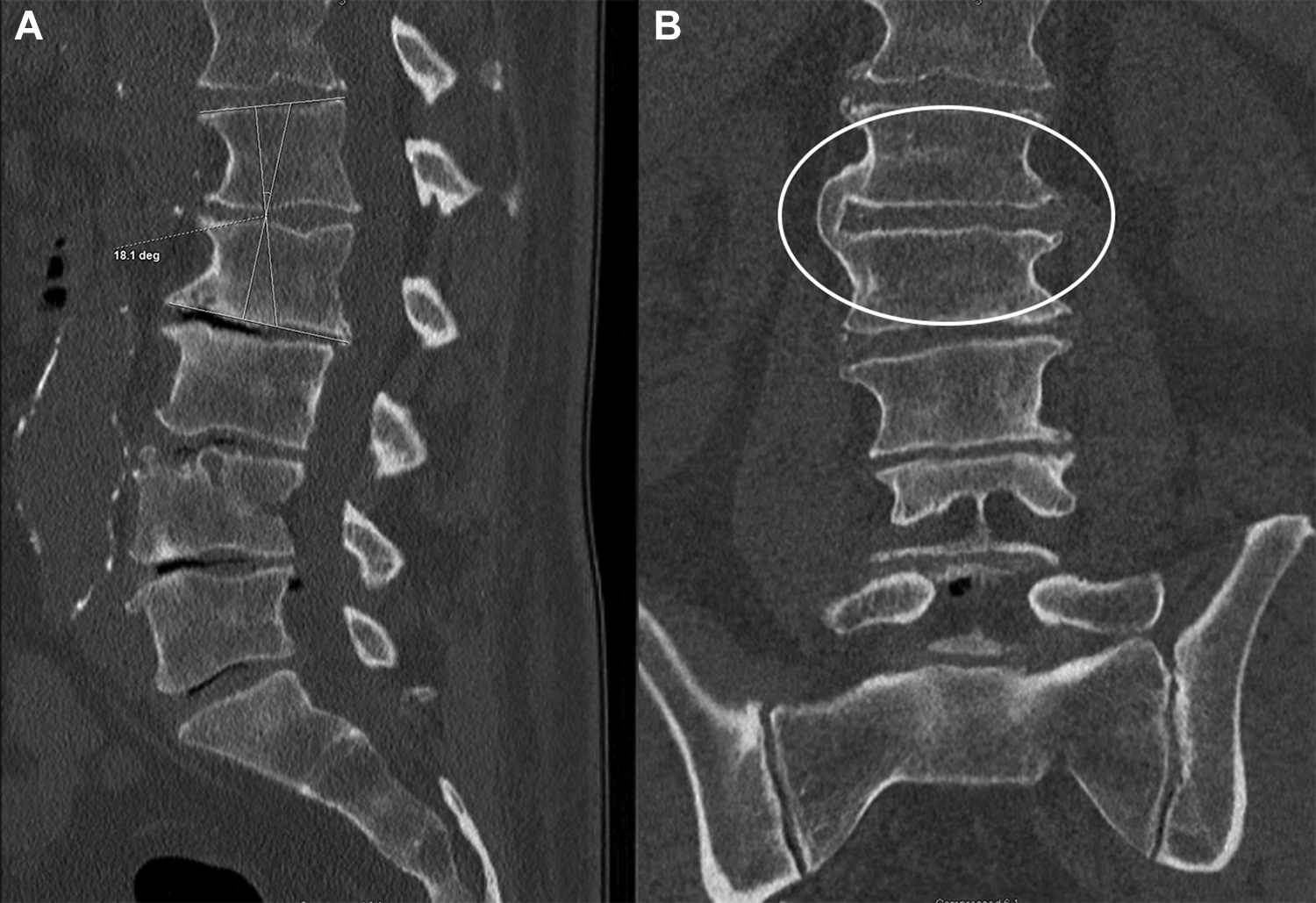
Sagittal (A) and coronal (B) computed tomography (CT) across a potential anterior column realignment (ACR) level due to preexisting kyphosis. On further inspection, CT demonstrates a fused bridging osteophyte (oval), which creates a situation that is unsuitable for ACR. Used with permission from Barrow Neurological Institute, Phoenix, Arizona.
Surgical Technique
The ACR surgical technique consists in using the traditional lateral transpsoas approach described by Akbarnia et al. 6 Access to the lateral spine is obtained via the traditional lateral transpsoas corridor. Using radiography or neuronavigation, the location of the spinal level of interest is identified and marked on the surface of the skin. Lateral incision is performed overlaying the disc space, followed by subcutaneous dissection, facial opening with coagulation, blunt abdominal wall muscle dissection sparing the traversing neurovascular structures, retroperitoneal dissection, and safe identification of the lateral aspect of the lumbar spine. After confirmation of appropriate location and verification of safe dilation, a tubular dilator is positioned and rigidly fixed to the surgical bed to facilitate access to the lumbar spine. Next, a blunt dissection tool is placed anterior to the ALL. The discectomy is then performed in the standard fashion: (1) annulotomy, (2) contralateral annulotomy, and (3) discectomy. Next, blunt dissection is performed by progressive blunt dissector advancement, carefully developing the plane between the adventitia tunica of the anterior vessels and the ALL, which has been previously studied by means of MRI to discover a safe plane. Once a safe plane has been developed, a sharp blade is advanced over the grooved anterior retractor to perform sharp dissection of the ALL with radiographic verification.
Once sharp release of the ALL has been performed on approximately 75% of the ALL, the retractor is removed, and a manual indirect distracting tool is placed (Figure 5). Under fluoroscopic guidance, the distracting tool is advanced and progressively opened to complete the ALL release indirectly. Oftentimes, an audible pop will be heard, and a sudden loss of resistance will be felt. It is critical at this point to visually inspect for bleeding. Following discectomy, a hyperlordotic interbody device implant is placed and fixated anterolaterally with either 1 or 2 screws (Figure 6). Although debate exists regarding the use of a buttress plate (which requires 1 screw) or plate fixation (which requires 2 screws), in our experience, plate fixation does not significantly limit achievable lordosis. The fascia overlying the abdominal musculature and skin incision are reapproximated in standard fashion to avoid abdominal wall herniation. Posterior construct supplementation with pedicle screws and rods should follow ACR, and posterior osteotomy can be used to increase lordosis gain if needed (Table 1). 12
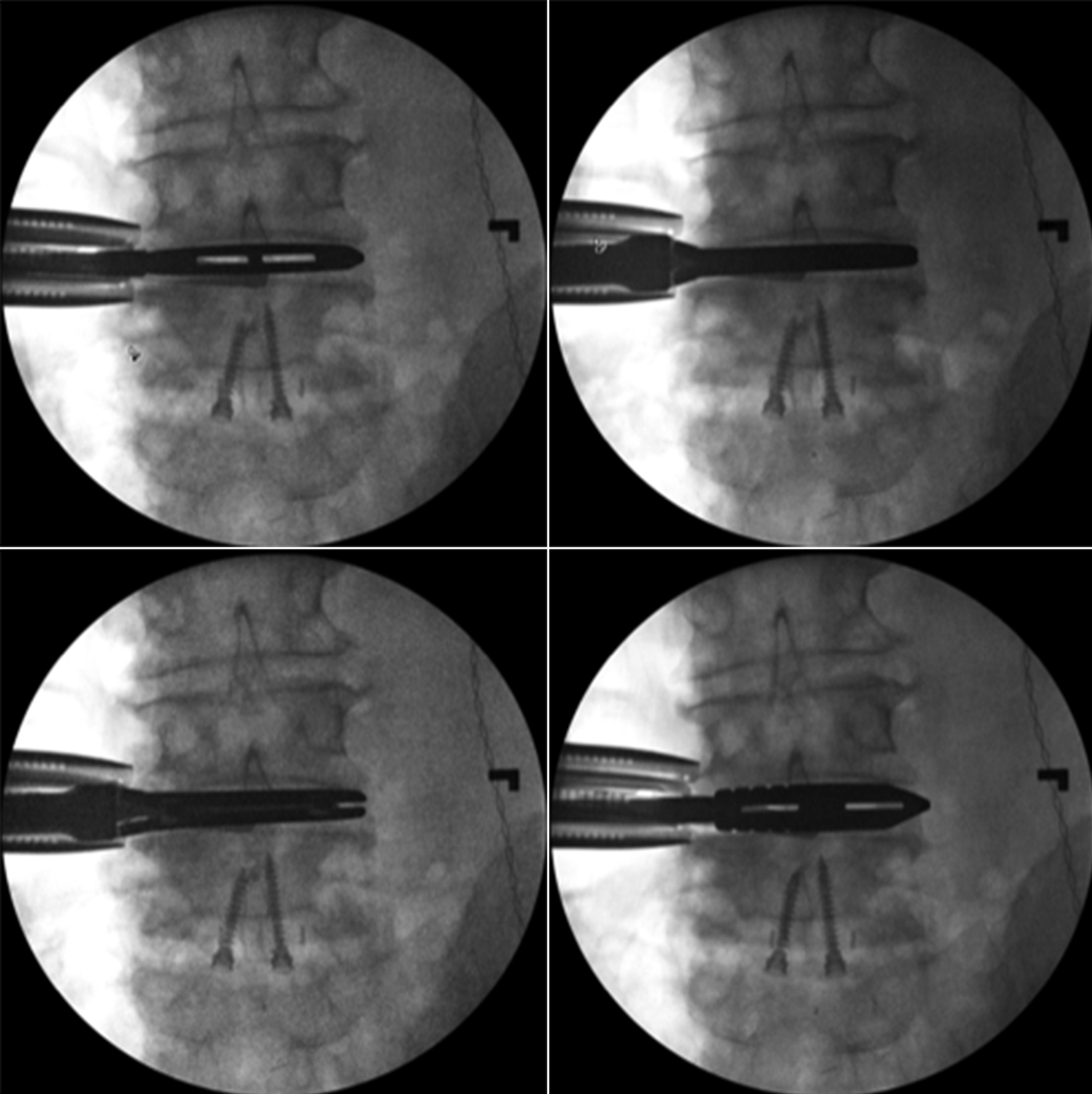
Anteroposterior fluoroscopic imaging demonstrating indirect release of remaining anterior longitudinal ligament using manual serial distraction. Note anterior lumbar interbody cage inferiorly. Used with permission from Barrow Neurological Institute, Phoenix, Arizona.
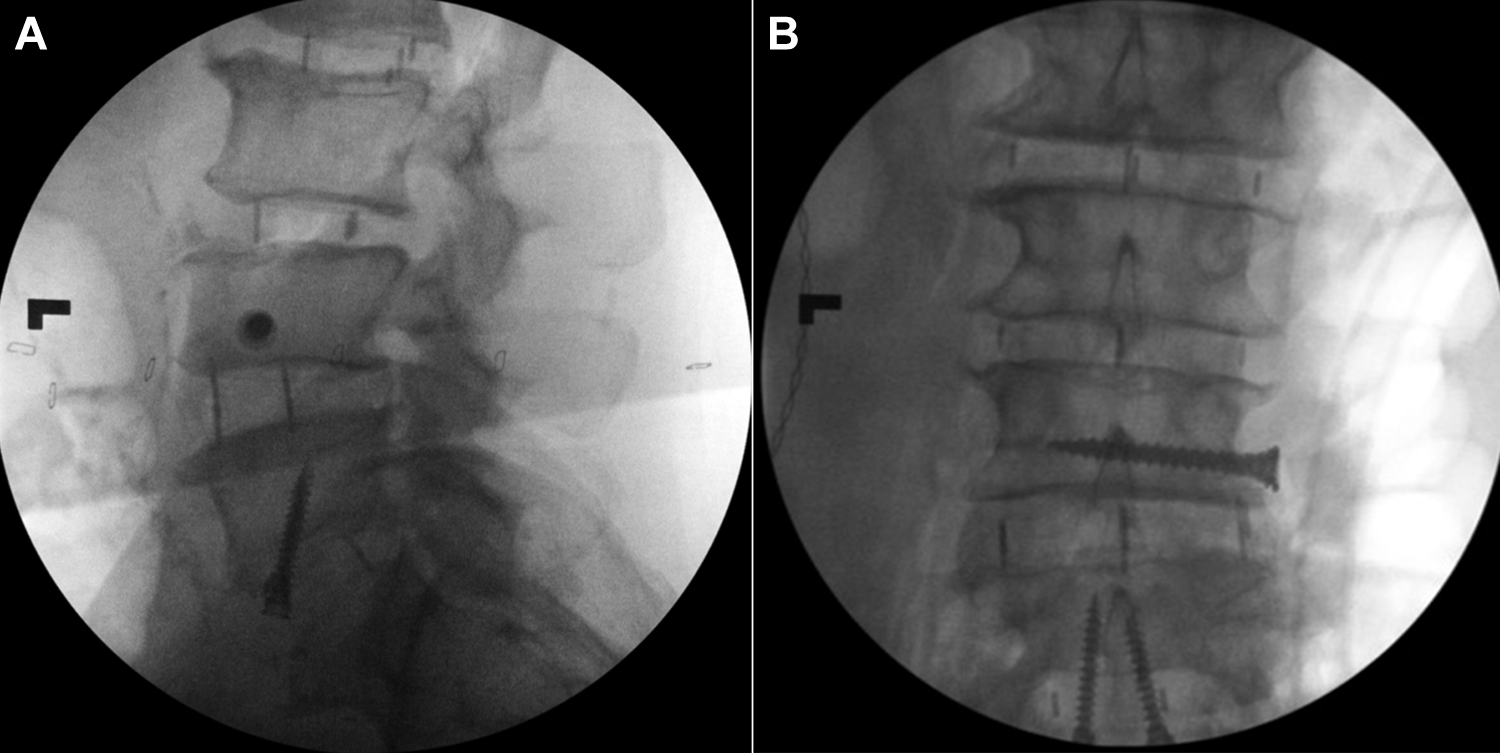
Lateral (A) and anteroposterior (B) intraoperative fluoroscopic imaging of anterior column realignment with hyperlordotic polyetheretherketone interbody cage with buttress plate (1 integrated plate/screw) in superior vertebral body. Used with permission from Barrow Neurological Institute, Phoenix, Arizona.
Maximal Segmental Lordosis for Anterior Column Realignment in a Cadaveric Model.
Technology
Minimally invasive surgery, particularly lateral corridor surgery, is heavily reliant on imaging and monitoring technology. Reliable and accurate neuromonitoring is a prerequisite for safe and efficient lateral access surgery. Due to the likely prolonged retraction on the psoas muscle, identification and protection of the lumbosacral plexus is of paramount importance in reducing the incidence of neural injury. Use of imaging technology is crucial, and fluoroscopy, low-dose image-enhanced fluoroscopy, 24 -26 or potentially combined CT and radiographic imaging can be of assistance. 27
Neuromonitoring
Electrical neurophysiological monitoring is a necessary part of minimally invasive lateral transpsoas approaches to the lumbar spine. The nerve roots that contribute to the lumbar plexus and the genitofemoral nerve are at risk of injury when the surgeon crosses the psoas muscle with dilators and also during the retractor positioning. The nerves forming the plexus run obliquely outward, enclosed by the psoas muscle, from a dorsal situation at L1 to a ventral situation at L5; at the lower levels, they are heavier and denser, the roots conjoin, and the main motor branches originate. 28,29
The use of directional dynamically triggered electromyography (t-EMG) with discrete threshold responses is a high-sensitivity method that has been associated with a decrease in the neural complication rate from 30% to less than 1%. 30,31 Use of t-EMG provides threshold results of lower limb nerve root function on bilateral vastus medialis, tibialis anterior, biceps femoris, and medial gastrocnemius myotomes while manipulating the psoas muscle, spanning responses from the L2-S2 spinal nerves. t-EMG is integrated with dilator apparatuses and can provide rotational 360° information on the position and distance of the motor nerves surrounding the instrumentation, where a lower response threshold indicates closer nerve proximity compared with a higher response threshold.
Once docking has safely proceeded, plexus injury may still occur, induced by compression or distention by the retractor blade, which causes microvascular and electrophysiological changes that may result in neurological deficit or pain. 32,33 The magnitude and duration of the distortion are decisive in the occurrence and severity of iatrogenic nerve injury. 34 The retractor blade can contain a t-EMG test to quantify changes in threshold throughout the surgery and can indicate whether an ongoing compression and retractor should be released. 35 Spontaneous unremarkable (free-run) EMG monitoring has relatively low sensitivity to sustained retraction of nerve roots.
t-EMG provides real-time electrophysiological feedback of the situation of the nerves. In addition to allowing the anatomy of the lumbar plexus and safety zones to be perceived, t-EMG increases the elementary basement for a safe navigation and is an integral and necessary part of ACR. 29
Imaging
Similarly, imaging is critical for performing the ACR safely and effectively. Fluoroscopy is considered the gold standard for ACR during positioning, marking the skin, confirming the level, and implanting. However, increased radiation exposure to the patient and surgeon is a disadvantage associated with MIS. Even with frequent use of fluoroscopy, there is a risk for inappropriate cage positioning. Spinal navigation with 3-dimensional CT is an option to decrease the incidence of implant misplacement and amount of radiation exposure. 27 Once discectomy and endplate prep have been achieved, a navigated trial is inserted under stereotactic guidance for sizing. The cage is then attached to a navigated holder that allows insertion with image guidance. Navigation can also be used during the psoas muscle phase for positioning the retractor. In multilevel surgery, a significant concern is shifting the anatomy after the first cage insertion, which may potentially cause decreased accuracy. In such cases, use of fluoroscopy is helpful to verify accuracy.
Complications
A recent study from the International Spine Study Group that reviewed 953 patients treated surgically for ASD reported a major complication rate of 7.6%. 36 Major complications were defined according to Carreon et al, 37 with the most common complications being excessive blood loss (defined as the loss of >4 L of blood), deep wound infection, and pulmonary embolism. Although the ACR is an MIS technique that may potentially decrease complications related to large exposures and extensive soft-tissue disruption, overall complications can occur. Notably, ACR is associated with significantly less blood loss than traditional 3-column osteotomy. 16,38
Most important, neurological deficit associated with lumbosacral plexus neuropraxia caused by psoas muscle retraction represents an important concern with use of the lateral transpsoas approach. In the largest series of cases in the literature, among 600 patients who underwent surgery with the lateral transpsoas approach, only 0.7% had neurological deficits, and these deficits were transient in all cases. 39 However, in the same study, 62.7% of patients experienced some postoperative thigh-related symptoms. 39 Prolonged retraction time is a predictor of decreasing nerve function and decreasing retraction time, and use of t-EMG throughout retraction may reduce the incidence of this complication. 40 The majority of postoperative transpsoas thigh symptoms are temporary; half of those patients with such symptoms will recover in 3 months, and 90% will recover within 1 year. 39,40
Surgeons must be experienced and familiar with the retroperitoneal and abdominal anatomy when performing lateral approaches to safely identify and separate the ALL from the anterior structures before releasing it. The direct and indirect ALL transection is an extremely advanced technique that exposes spine surgeons to unfamiliar regional anatomy, risking injury to the autonomic plexus, visceral organs, or the great vessels (femoral artery and femoral vein). 41 Visceral or major retroperitoneal vessel injuries are rare but are some of the most feared complications. 42 Bowel injuries have been previously reported in the literature and require prompt repair via laparotomy and potentially colostomy to avoid peritonitis, which can be fatal. 43 Injury to the great vessels can also occur, which demands immediate repair with assistance from a vascular surgeon.
The most common mechanical complications in patients with ASD are proximal junctional kyphosis (PJK) and proximal junctional failure (PJF). 44 Others causes of revision surgery are pseudarthrosis, rod fracture, and loss of correction. 45 PJK is a concern in ASD surgery regardless of the approach used, and its prevalence is 20% to 40%. 46 PJK results from failure of the proximal junction caused by mechanical stress concentration at the upper instrumented level and its adjacent level. Consequently, the posterior ligament complex, bone elements, and instrumentation are affected at this site. Age greater than 65 years is a major risk factor for PJK, and other factors that may also be associated with PJK include disruption of the posterior tension band, bone quality, severity of preoperative deformity, extent and rigidity of construct, and incomplete realignment. 46 -49 Gandhi et al 47 reported a series of cases in which, among patients with ACR only, the incidence of PJK was 30% and that of PJF was 11%. Among patients with ACR plus PCO, the incidence of PJK was 42.9% and that of PJF was 40%. The addition of PCO is associated with an increased incidence of PJK and PJF; nevertheless, the patients who require ACR plus PCO are usually those who have the most severe sagittal imbalance and require greater reduction. Recent investigation into combining ACR with adjacent PSO did not report any events of PJK or PJF in an average 1.9-year follow-up; importantly, however, this was not the primary objective of the study. 50
Additional complications have also been reported. These include rod fracture and subsidence. A retrospective review from several institutions found rod fracture in 4.4% of cases treated with ACR at a mean of 8.6 months after surgery across 98 patients (follow-up range, 1-7.4 years), with the length of the surgical construct an independent predictor of rod failure. 20,51 Subsidence of the interbody graft into the adjacent vertebral bodies is another risk associated with use of lateral approaches and can result from high mechanical stress at the endplate. Subsidence of the interbody graft can cause severe pain, impaired fusion, and even fracture of the vertebral body itself. Over-distraction, insufficient cage width, and endplate violation have been described in the literature as potential risk factors. 52,53 An increased incidence of subsidence has been reported among patients with impaired bone mineral density, but ACR is feasible in this population. 54 All patients who will undergo ACR should be screened with dual-energy X-ray absorptiometry.
Pearls and Pitfalls of ACR
The ACR technique represents a powerful, recently introduced MIS option to address ASD and has a strong potential for correction of sagittal imbalance and restoration of alignment. It is, however, an advanced technique and should be performed by surgeons experienced with lateral approaches to the spine. The surgeons who perform ACR would ideally be familiar with the lateral approach and retroperitoneal anatomy, and they also must be prepared to control, or at least slow, bleeding in case of vascular tearing (affecting major or minor vessels). Once the retractor is docked, the surgeon should be able to operate efficiently and promptly to decrease the opened retractor time to avoid or limit the extent of neurological deficits.
Preoperative evaluation of patient-specific anatomy with MRI to ensure a safe surgical corridor is paramount, particularly in assessing the potential for adherence of vascular structures to the ALL. In addition, a requisite for ACR is a nonfused disc space; in this regard, we recommend evaluation of the intended disc space with both standard radiography and CT. Although performing a discectomy for a standard lateral approach is possible with angled instruments, we advise against use of angled instruments for ALL release. Therefore, evaluation of the crest line in relation to the L4-5 level on standing anteroposterior radiographs is crucial to assess feasibility of an L4-5 ACR.
Conclusions
ACR represents a powerful technique in the minimally invasive spinal surgery armamentarium for sagittal plane correction in ASD or as a less invasive adjunct to traditional open techniques. This technique is heavily dependent on technology but represents a fascinating and exciting new chapter in spine surgery. Although studies demonstrate good radiographic outcomes with a complication profile comparable to that associated with traditional 3-column techniques, further investigation is necessary to better characterize and develop this technique.
Footnotes
Acknowledgments
The authors thank the staff of Neuroscience Publications at Barrow Neurological Institute for assistance with manuscript preparation.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Juan S. Uribe serves as a consultant for Misonix, SI-Bone, and NuVasive, Inc. In addition, he receives non–study-related research support and stock options from NuVasive, Inc. Dr Jay D. Turner serves as a consultant for SeaSpine as well as NuVasive, Inc. Additionally, he receives non–study-related research support from NuVasive, Inc.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This supplement was supported by funding from the Carl Zeiss Meditec Group.