
Abstract
Study Design
Retrospective cohort study.
Objective
Determine if the use of a Wilson kyphosis frame during single level minimally invasive transforaminal lumbar interbody fusion (MIS TLIF) at L4-5 or L5-S1 impacts postoperative lumbar lordosis.
Methods
A retrospective analysis of patients who underwent a single level MIS TLIF at L4-5 and L5-S1 from 1/1/2016 to 1/1/2021 was performed. Patient demographics were collected, and radiographic measurements preoperatively and 6 months postoperatively were performed. Our primary outcome was “delta lumbar lordosis” (delta LL), or the difference between pre-operative and 6 month postoperative lumbar lordosis. Statistical analysis was performed using step-wise multivariate linear regressions.
Results
A total of 180 patients were included. Mean age was 58.5 ± 11.8 years and 48.3% were female. Mean BMI was 28.6 ± 5.6. Wilson positioning frames were used in 96/180 (53.3%) procedures. Use of a Wilson Frame was independently predictive of 2.5° reduced delta LL (Coeff −2.5, 95% CI -4.1 to −0.9). However, use of a Wilson frame was not found to be independently associated with postoperative mismatch between pelvic incidence and lumbar lordosis.
Conclusions
Use of a Wilson kyphosis frame during single level MIS TLIF at L4-5 and L5-S1 resulted in a loss of 2.5° of lordosis compared with those patients who had a MIS TLIF without a Wilson frame. The clinical impact of this loss over long-term follow-up will be the subject of future studies.
Keywords
Introduction
Transforaminal lumbar interbody fusion (TLIF) is a useful technique for achieving indirect lumbar decompression through restoration of disc height and unbuckling of hypertrophic ligamentum flavum. Minimally invasive TLIF (MIS TLIF) can achieve both fusion and decompressive goals through a posterior approach while minimizing blood loss and soft tissue disruption.1,2 Advances such as expandable cages have permitted the introduction of taller cage height and lordosis without an increased risk of injury to the exiting nerve root. 3
While the fusion benefits of TLIF are clear, detractors point to the reduced lordosis produced by the procedure. 4 This may be particularly impactful in the distal lumbar spine (L4-5 and L5-S1 levels), which has been shown to provide 2/3 of physiologic lumbar lordosis. Iatrogenic flatback due to poor restoration of lordosis at these levels can result in altered adjacent level pressures, potentially leading to adjacent segment disease and long-term sagittal malalignment.5,6
To improve navigation fidelity and provide positional distraction of the disc space without the need for pedicle screw-based distractors, our group has performed single level MIS TLIF procedures using a Wilson kyphotic positioning frame. 1 While anecdotally we have not seen a corresponding decrease in the postoperative lordosis of patients operated on using a Wilson Frame, no work to our knowledge has objectively evaluated the postoperative alignment of these patients in relation to those who were positioned on an open Jackson table. This work sought to achieve this using our large single-institutional cohort.
Methods
This was an institutional review board-approved retrospective analysis of patients who underwent a single level MIS TLIF at L4-5 or L5-S1 at a large tertiary referral academic spine center from 1/1/2016 to 1/1/2021. Informed consent was not required as this was a retrospective study without impact on the patient’s medical record. Inclusion criteria were patients >18 years of age without a history of prior spine fusion who underwent a single level MIS TLIF during the study period. Patients with a history of spine malignancy, trauma rheumatic disease or infection, with scoliosis involving the lumbar spine >10 deg or who failed to present for post-operative follow-up were excluded. No disc space distractor was used on patients who underwent a MIS TLIF on a Wilson frame, while those on an open Jackson table required a pedicle screw-based distractor. An illustrative example of the results of the use of an MIS TLIF with Wilson frame vs pedicle screw-based distractor before and 1-year after surgery are shown in Figure 1. Lateral Lumbar Spine X-Rays Illustrating Preoperative and 1-Year Postoperative Changes in Sagittal Alignment in Four Patients Who Underwent TLIF Using Either a Wilson Frame A–D or a Jackson Table E–H. Preoperative A, C and 1-Year Postoperative B, D X-Rays are From Two Patients Positioned With a Wilson Frame. Preoperative E, G and 1-Year Postoperative F, H X-Rays are From Two Patients Positioned With a Jackson Table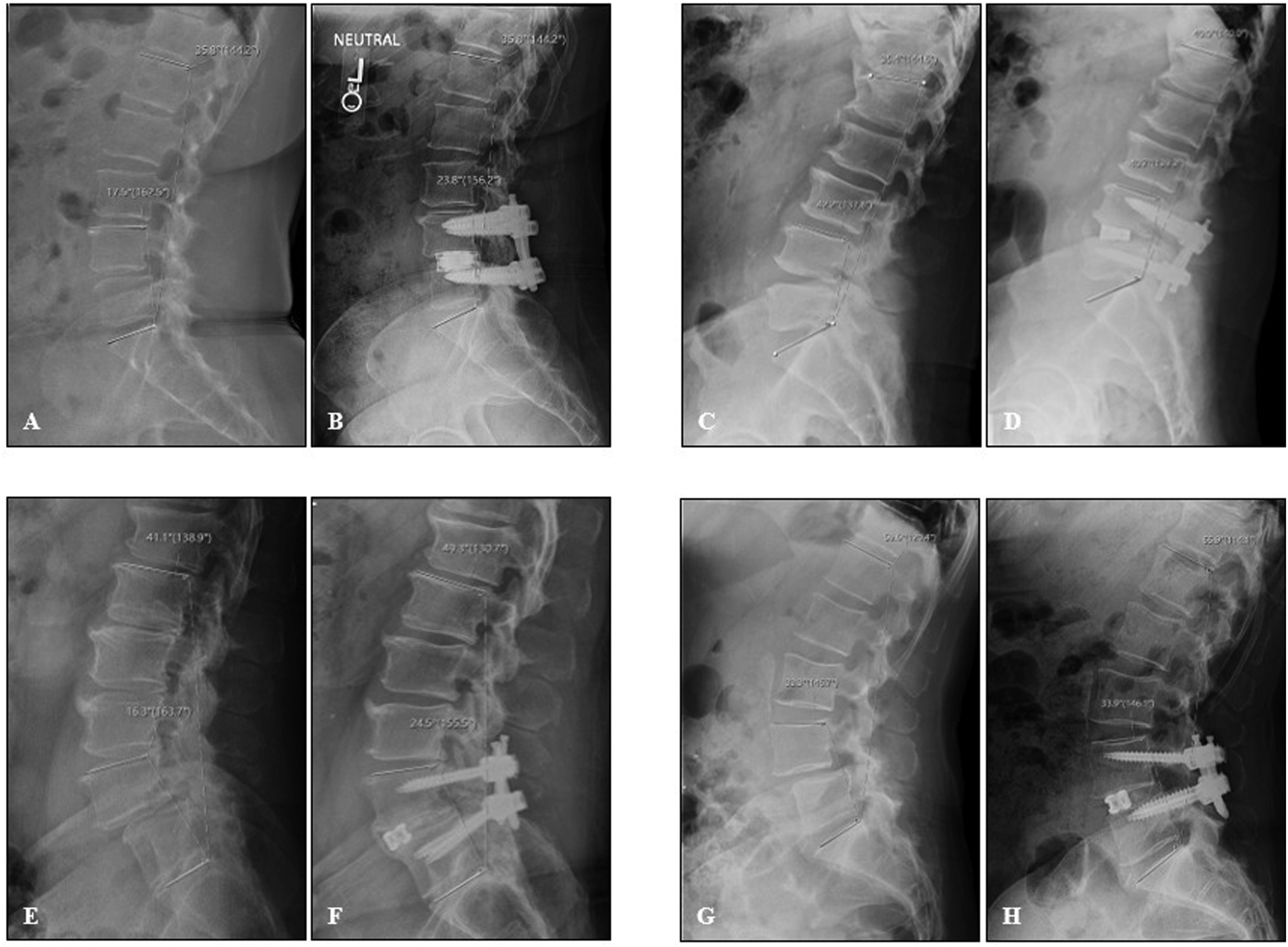
Data collected from the medical record included patient age, sex and BMI as well as implant characteristics, including type (expandable vs static cage), height and lordosis. All TLIF implants used in this study were titanium. Radiographic measurements included pelvic incidence (PI), lumbar lordosis (LL), proximal lumbar lordosis (PLL), distal lumbar lordosis (DLL) and implant position (center of implant in the anterior or posterior half of the disc space). All radiographic measurements were recorded as the average of measurements made by two fellowship-trained orthopaedic spine surgeons using ClinicView.
Our primary outcome was post-operative “delta lumbar lordosis” (delta LL), or the difference between pre-operative lumbar lordosis and that measured 6 months postoperatively. The 6-month timepoint was selected as this was the longest postoperative timepoint at which the full cohort had postoperative imaging. Secondary outcomes were: “delta distal lumbar lordosis” (delta DLL), defined as the angle measured from the superior L4 endplate to the superior S1 endplate; “delta proximal lumbar lordosis” (delta PLL), defined as the angle measured from the superior endplate of L1 to the superior endplate of L4; and change in the mismatch between pelvic incidence and lumbar lordosis (PI-LL mismatch). Changes in absolute LL, DLL and PLL were also analyzed.
Statistical analysis was performed using SPSS 28 (IBM, Armonk NY). Independent associations between the measured variables and delta LL, delta PLL and delta PLL were quantified using a step-wise multivariate linear regression and are written as coefficient (95% confidence interval). Absolute post-operative LL, DLL and PLL were compared with pre-operative measurements using paired students’ t-tests, with P < 0.05 considered statistically significant. Data are expressed as mean ± standard deviation and proportion (percentage) as indicated.
Results
Cohort Demographic, Implant and Baseline Radiographic Characteristics (n = 180)
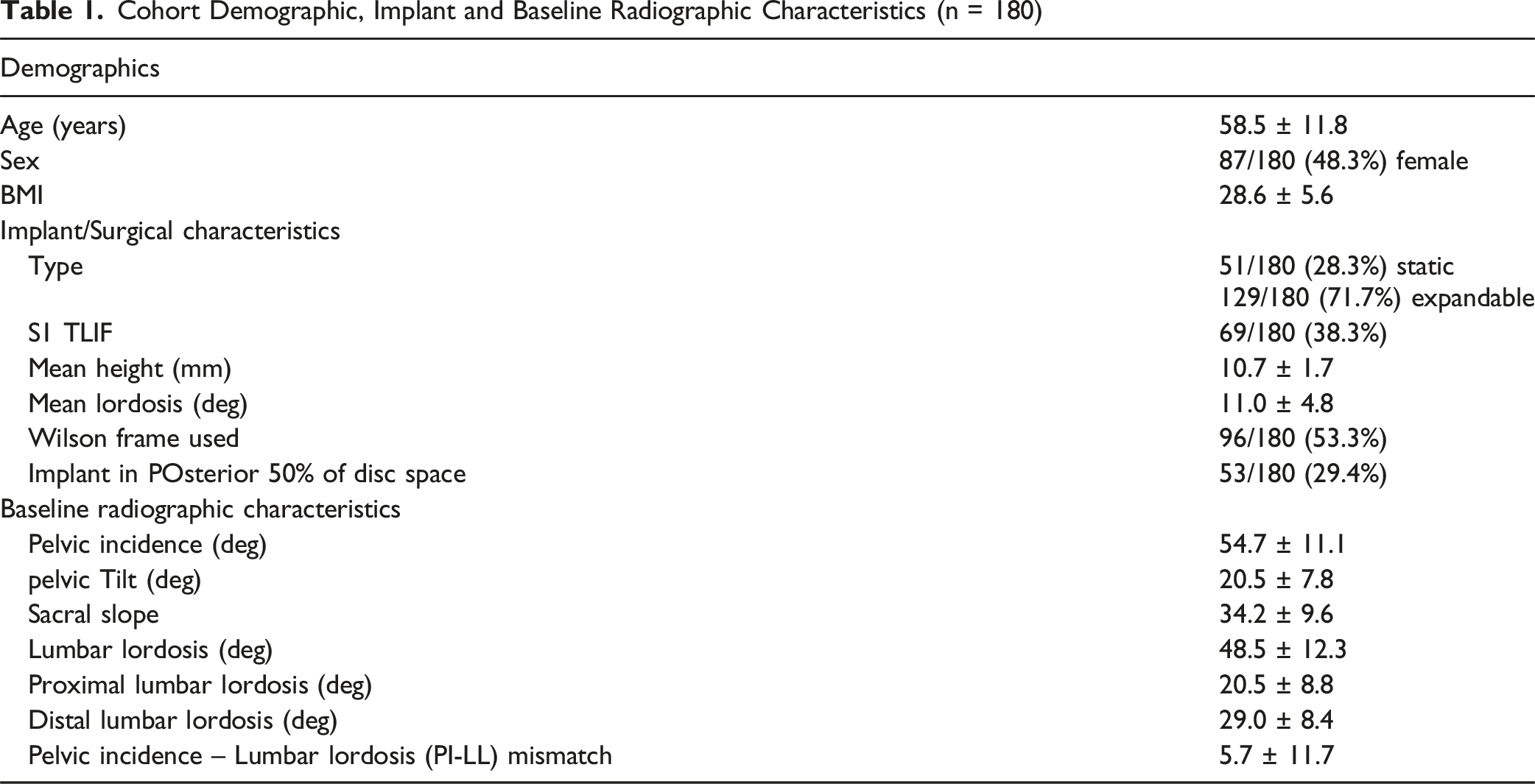
Wilson positioning frames were used in 96/180 (53.3%) procedures. Expandable implants were used in 129/180 (71.6%) cases. Most (123/129, 95.3%) were expandable articulating cages. Mean implant height was 10.8 ± 1.7 mm and mean implant lordosis was 11.9 ± 10.3 deg. Implants were posteriorly placed in 53/180 (29.4%) of cases.
Lumbar Lordosis and PI-LL Mismatch Pre-vs 6-Month after MIS TLIF

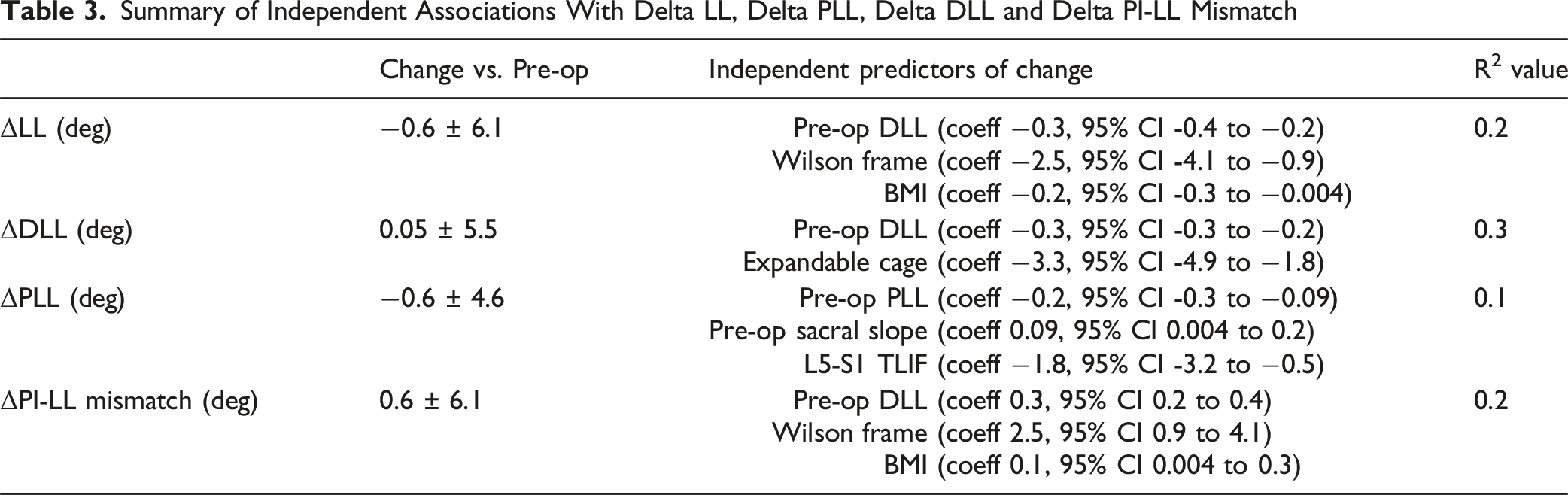
Summary of Independent Associations With Delta LL, Delta PLL, Delta DLL and Delta PI-LL Mismatch
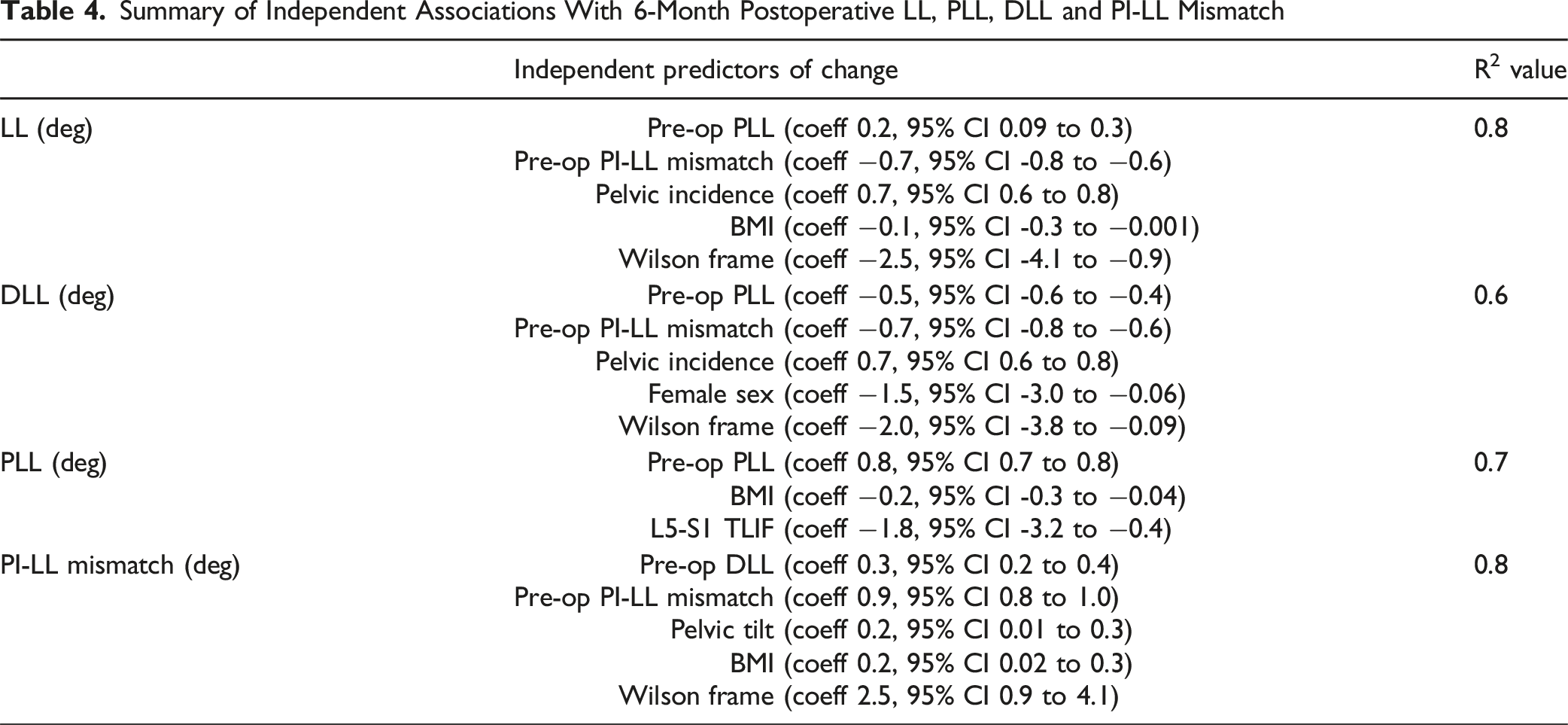
Summary of Independent Associations With 6-Month Postoperative LL, PLL, DLL and PI-LL Mismatch
Discussion
Patient positioning can impact surgical ease and postoperative sagittal alignment. Our group has opted to use a Wilson kyphosis positioning frame during single level MIS TLIF procedures to distract our disc space. In a retrospective comparison of single level MIS TLIFs performed at L4-5 and L5-S1 at our institution over a 5-year period, we found that while the use of a Wilson frame was associated with a decrease in lumbar lordosis improvement 6 months postoperatively by approximately 2.5°, it did not impact the sagittal malalignment (PI-LL mismatch) of our cohort.
TLIF is not considered a lordosis-producing procedure. 4 Techniques designed to create lordosis with TLIF, in particular bilateral facetectomies, have not been found to consistently produce this result. 7 Snyder et al in their cadaveric study found a difference of approximately 1° between the segmental lordosis of TLIFs performed from L3-S1 via unilateral vs bilateral facetectomy approaches. 8 Utilization of an open technique does not appear to impact the benefit of bilateral facetectomies. Le et al 9 in their comparison of open vs minimally invasive TLIF with bilateral facetectomies reported no difference in sagittal alignment but reduced blood loss and increased surgical time in the minimally invasive cohort. Tye et al 10 support the radiographic conclusions of Le et al, although of note do report improved 1-year Patient Health Questionnaire-9 (PHQ-9) scores in patients who underwent bilateral facetectomies.
Expandable cages were designed to permit a greater magnitude of disc height and lordosis restoration. 11 While prior work by our group supports the improved degree of lordosis correction provided by expandable implants, 12 we do note across multiple MIS techniques that interbody cage lordosis has variable impact on postoperative alignment. 13 Prior work also highlights the increased risk of the subsidence of expandable implants, especially in those TLIFs performed without a contralateral facetectomy. 14 Our opinion remains that TLIF is inferior to anterior lumbar interbody fusion (ALIF) and lateral lumbar interbody fusion (LLIF) as a lordosis-producing approach, regardless of the technique that is utilized. We therefore avoid this procedure in patients in whom sagittal malalignment is a concern.
This lack of sagittal alignment benefit influenced our patient indications for the procedure. Our cohort has minimal evidence of sagittal malalignment, with a mean PI-LL mismatch of approximately 5°. Less than a third of our cohort had a PI-LL mismatch >15° prior to surgery. Patients indicated for single level MIS TLIF by our service had no or minimal (Meyerding Grade I or II) spondylolisthesis, and had degenerative disease that was largely isolated to the operative levels. 15 While the present work does show a 2.5° decrease in lumbar lordosis 6 months after surgery in patients treated using a Wilson frame compared with an open Jackson table, it is questionable if the statistical significance of this finding translates into clinical significance. The measurements of differences this small using conventional software tools may fall within statistical noise, making the observed difference in lordosis purely the result of the specific patients on which it was used. We also note that we did not use pedicle-based distractors on patients who had surgery using a Wilson frame, thereby introducing a kyphotic vector to patients who underwent fusions without a Wilson frame. In this case we are essentially comparing two techniques that both include a kyphotic vector: either via patient positioning or physical disc space distraction. Given this rationale, we support the findings of the present work that the use of a Wilson frame has a minimal impact on radiographic outcome. However, by extension this work cannot conclude that the use of a Wilson frame in patients with more extensive degenerative disease and/or severe sagittal malalignment is similarly benign.
There are several limitations to this work beyond those intrinsic to retrospective cohort studies. We specifically studied a cohort at a single academic hospital that had generally isolated degenerative disease at L4-5 or L5-S1, requiring single level surgery. We cannot attest to the impact of a Wilson frame on patients who require multilevel fusions, as noted previously. Further, the overwhelming majority of our patients received an expandable articulating cage. We are therefore unable to determine if a Wilson frame differently impacts patients who receive static or non-articulating cages. Finally, we feel that a 6-month follow-up period is sufficient to give us a good idea of what the patient’s final sagittal alignment has become after surgery. However, we concede that our lack of longer-term outcomes does not allow us to determine if the 2.5° impact of a Wilson frame truly has no long term clinical impact on sagittal alignment, revision surgery rates and patient-reported outcomes. 16 We also did not compare patient-reported outcomes between those who had surgery with vs without a Wilson frame, which omits a significant factor in considering the overall clinical impact of this technique. Finally, we used a 6-month timepoint due to the availability of imaging for our patients out to that timepoint. This is likely suboptimal for assessing the long-term outcomes of this technique, and we do not believe that this work confirms the lack of long-term consequences when using a Wilson frame. This may be better assessed in a future long term observational or recall study. While our service will continue to use a Wilson positioning frame on subsequent surgeries, further long-term prospective analyses are necessary to fully settle the impact of this technique.
Conclusion
Use of a Wilson kyphotic positioning frame during MIS TLIF allows for distraction of the disc space without the need for mechanical adjunct, thereby preserving the fidelity of intraoperative navigation. In a retrospective analysis of 180 patients treated with a single level MIS TLIF at L4-5 or L5-S1, we found that use of a Wilson frame resulted in an under-correction of lumbar lordosis by 2.5° 6-month after surgery without an impact on PI-LL mismatch over this period. Future work will evaluate the longer-term impact of the use of a Wilson frame during single level MIS TLIF.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Deidentified data used in this work can be obtained from the corresponding author upon reasonable request.
IRB Approval
Human subjects approval was obtained for the protocol described in this work (2021-1890) Outcomes after Lumbar Decompression and Interbody Fusions.