
Abstract
Study Design:
Narrative review.
Objectives:
Robotic systems in spinal surgery may offer potential benefits for both patients and surgeons. In this article, the authors explore the future prospects and current limitations of robotic systems in minimally invasive spine surgery.
Methods:
We describe recent developments in robotic spine surgery and minimally invasive spine surgery. Institutional review board approval was not needed.
Results:
Although robotic application in spine surgery has been gradual, the past decade has seen the arrival of several novel robotic systems for spinal procedures, suggesting the evolution of technology capable of augmenting surgical ability.
Conclusion:
Spine surgery is well positioned to benefit from robotic assistance and automation. Paired with enhanced navigation technologies, robotic systems have tremendous potential to supplement the skills of spine surgeons, improving patient safety and outcomes while limiting complications and costs.
Introduction
Robotic systems are rapidly changing the landscape of modern surgery, offering potential benefits for both patients and surgeons. Since its approval by the Food and Drug Administration (FDA) in 2000, the da Vinci Surgical System (Intuitive Surgical, Sunnyvale, CA) has been used in complex, minimally invasive intracavitary surgical procedures. 1 Although the application of robotic systems in spine surgery has been gradual, the past decade has seen the arrival of several novel robotic systems for use in spinal procedures, indicating renewed enthusiasm in this field. Spine surgery is particularly well positioned to benefit from robotic assistance and automation, as procedures in this subspecialty often require repetitive movements during lengthy operations, as well as fine manipulation of vital structures in constricted surgical corridors. 2 Along with enhanced navigation technologies, robotic systems have tremendous potential to improve patient safety and outcomes while limiting complications and costs. In this article, we explore the expanding horizon and prospects of robotic systems in spine surgery.
Current State of Robot-Assisted Minimally Invasive Spinal Surgery
Robot-Assisted Pedicle Instrumentation
During spinal fusion procedures, pedicle screws are routinely used for internal spinal fixation and stability. Although the freehand technique, which relies solely on anatomical landmarks, has proven to be safe and accurate, the malposition of screws can inadvertently injure adjacent structures, resulting in devastating vascular, neurological, and mechanical consequences. The development and adoption of fluoroscopy-guided and computer-assisted navigation have resulted in more accurate placement of pedicle screws, and many studies have demonstrated the improved precision and safety of screw placement with these technologies. 3,4 However, the risk of nerve and vascular injuries remains, even with the use of image guidance. 5 Additionally, the use of continuous intraoperative fluoroscopy places patients, surgeons, and operating room staff members at risk for exposure to harmful radiation. These concerns have prompted the demand for trajectory assistance in pedicle implantation with robotic systems. Incorporating robotic systems in pedicle instrumentation may increase consistency, reduce inaccuracy, minimize radiation exposure, and decrease operative time. As expected, instrumentation guidance remains the most well-studied application of robotics in spine surgery.
Computer-Assisted Navigation Systems for Spinal Surgery
Intraoperative navigation technologies have become indispensable in cranial neurosurgery. 4 An important technological addition to spinal surgery is the arrival of computer-assisted navigation systems based on computed tomography (CT). Fundamentally, these technologies rely on real-time generation of a 3-dimensional (3D) spinal map from CT imaging with reference clamps. This map can then be used to guide screw placement with high precision. Currently, multiple computer-assisted navigation systems have been approved by the FDA. The Airo Mobile Intraoperative CT-based Spinal Navigation system (Brainlab, Munich, Germany) uses a mobile circular scanner attached to the operating table that allows for full 360° imaging and a scanning stereotactic camera for instrument registration. The Stealth Station Spine Surgery Imaging and Surgical Navigation with O-arm system (Medtronic, Minneapolis, MN) uses similar technology, but opens at 90° to allow for mobilization around the patient. The Ziehm Vision FD Vario 3D with NaviPort Integration system (Ziehm Imaging, Orlando, FL) obtains images via a 190° rotation with a C-arm around the patient. Importantly, reference clamps must not be moved after the registration process; otherwise, repeat CT scanning is required for re-registration. The Stryker Spinal Navigation with SpineMask Tracker and SpineMap Software system (Stryker, Kalamazoo, MI) circumvents these concerns by using a rectangle of trackers applied directly on the patient with an adhesive glue for referencing. The 7D Surgical Spine Navigation system (7D Surgical, Toronto, Ontario, Canada) allows for radiation-free intraoperative navigation with Flash imaging, which uses high-intensity light and an overhead camera to image the surgical field and align with preoperative CT. If the reference clamp is moved, re-registration can be performed radiation-free with the same technique. This technique requires significant exposure of the bony anatomy to be effective, and cannot be used for percutaneous procedures.
The advantage of navigation techniques in spine surgery has been established across various platforms. 3 Two large meta-analyses demonstrated significantly greater accuracy with computer-assisted navigation pedicle screw placement compared to freehand placement. 6,7 Patients who underwent computer-assisted navigation pedicle screw placement consequently had lower neurological complication rates than those who underwent freehand placement (odds ratio [OR] 0.25, 95% CI 0.06, 1.14, P = .07). 6 The risk of pedicle perforation for screw insertion with computer-assisted navigation is also significantly lower than freehand technique (risk ratio [RR] 0.39, P < .001). 7 Although less well investigated, the use of navigation technologies has been extended to spinal tumor resection, with encouraging early results. 8 -11
Current Spinal Robotic Systems
Currently, 3 robotic systems in the United States have been cleared by the FDA for use in spine surgery: Mazor X Stealth Edition (previous models include the Mazor X, SpineAssist, and Renaissance; Mazor Robotics, Caesareas, Israel), ExcelsiusGPS (Globus Medical, Audubon, PA), and ROSA (Zimmer Biomet, Warsaw, IN). ROSA has had very limited use in spine surgery. Key features of these 3 systems are compared in Table 1. Essentially, these platforms are based on shared-control models, in which both the surgeon and the robot concurrently control motions. 12 Highly accurate screw placement can be achieved by integrating computer-assisted trajectory planning guidance of a robotic arm.
Robotic Systems Approved by the Food and Drug Administration for Use in Spine Surgery.
Abbreviations: FDA, Food and Drug Administration; CT, computed tomography; K-wire, Kirschner wire; RCT, randomized controlled trial; MR, Mazor Renaissance; MX, MazorX.
The original Mazor robotic system (SpineAssist) was approved by the FDA in 2004, and is the most extensively studied system to date. 5,13,14 The next-generation Mazor Renaissance is attached directly to a spinous process in open surgery, or to a frame triangulated by percutaneously placed guide wires for minimally invasive surgery (MIS). Virtual templating and trajectory planning are performed with preoperative CT. After the optimal implant trajectory is determined, a cortical punch is drilled at the desired entry point, and a guidewire is inserted into the vertebral body to steer the drilling of a screw pilot hole. The most recent model (Mazor X) incorporates both intraoperative fluoroscopy and 3D surface scanning, but still requires fixation to the operative bed and bone mounting to the patient.
The ROSA system is a mobile, floor-fixable base with an attached robotic arm. Like the Mazor, the ROSA must be affixed to the patient’s bony anatomy. The ROSA system has been used more in cranial neurosurgical applications, and for a handful of spinal procedures. Planning of screw trajectory can be performed using either intraoperative fluoroscopy or intraoperative CT. The system integrates a navigation camera and image-guided reference, allowing for intraoperative tracking of instruments.
The latest addition to robotic spine surgery is the ExcelsiusGPS system, approved by the FDA in 2017. 15 It comprises a highly rigid robotic arm with 6 degrees of freedom mounted to a floor unit. Trajectory planning can be performed with preoperative or intraoperative imaging, including both fluoroscopy and CT, which permits real-time intraoperative navigation for instrument placement and improved imaging versatility (Figure 1). Screws are deployed directly via the rigid tubular robotic arm, eliminating dependence on patient-mounted frames and Kirschner wires (K-wires), which is a drawback associated with the Mazor and ROSA systems. The end effector is interchangeable, which allows for potential adaptation of additional tools to be mounted to the robotic arm. 16
Accuracy of Pedicle Screw Placement
As previously described, robotic assistance in spinal surgery has gained interest because of its potential for improving accuracy of instrument implantation. Recent literature reviews have shown that the accuracy of pedicle screw placement with robotic platforms is on par with, if not superior to, fluoroscopic-guided or conventional freehand techniques. 5,13 The Gertzbein-Robbins scale (GRS) has been used to assess accuracy in most studies. The GRS evaluates pedicle/cortical breach based on an idealized and optimized trajectory. 17 -19
As the first robotic system to be developed for spinal surgery, the Mazor robots remain the most well investigated to date. Several randomized controlled trials (RCTs) have been conducted to validate the accuracy of these systems. Ringel et al 20 published the results of the first RCT in 2012, evaluating 60 patients who received 298 pedicle screws. Interestingly, the Mazor SpineAssist was associated with less accurate screw placement, with an 85% rate of acceptably placed screws (GRS Grade A or B), compared with 93% acceptably placed screws in the freehand group. In this study, the robot was attached cranially to a spinous process via a K-wire and caudally to the operating table. The diminished accuracy of the robotic group was attributed to relative movement of the robot due to insufficient fixation, and dislocation of the implantation cannula at the screw entry point. As a result, malpositioned screws tended to deviate laterally.
A similarly designed study by Hyun et al 21 examined the accuracy of the Mazor Renaissance model; in that study, the robotic group achieved an accuracy rate of 100% (130 pedicle screws placed in 30 patients), compared with 98.6% in the freehand group (140 screws placed in 30 patients). The authors also observed a proximal facet joint violation in the freehand group, which was not seen with the robotic arm. More recent RCTs have echoed comparable or improved accuracy of screw placement with robotic systems, compared with fluoroscopy-guided freehand screw placement. 22 -24 In 2013, Roser et al 2 performed a 3-arm RCT comparing patients who underwent SpineAssist screw placement (n = 18), fluoroscopy-guided placement (n = 9), and freehand screw placement (n = 10). They found accuracy rates (GRS A) of 99.0%, 92.0%, and 97.5% for robot-assisted, fluoroscopy-guided, and freehand placement, respectively. 2
Although not as well studied as the Mazor system, preliminary studies using the ROSA system have shown promising results. 25 -27 Of note, Lonjon et al 25 conducted the only prospective, nonrandomized case-matched study comparing ROSA (40 screws in 20 patients) to freehand pedicle screw placement (50 screws in 10 patients). A higher accuracy rate was observed in the robotic group (97.3%), compared with the freehand group (92.0%), although this difference was not statistically significant (P = .639). In this study, placement of 4 additional screws was attempted robotically, but these attempts were aborted due to technical difficulties. 18,19
No prospective, randomized studies of the ExcelsiusGPS have been reported, although initial case reports and small case series indicate high accuracy and safety with rates similar to those of other robotic systems (Figure 2). 15,18,28 -30 Additionally, with spinal robotics, the accuracy of screw placement can be judged not only with the conventional GRS but also by measuring deviation from a pre-planned trajectory. Using this novel metric to quantify accuracy, preliminary results suggest that the ExcelsiusGPS allows for precise screw placement. 18
Radiation Exposure
Fluoroscopy plays a crucial role in localization and guidance of instrumentation for spinal surgery. Therefore, patients, surgeons, and staff members in the operating suite during a spinal surgery are exposed to significantly more harmful ionizing radiation than they are in other neurosurgical subspecialties or in orthopedic surgery. Robotic spine surgery can minimize or even eliminate radiation exposure to the surgeon and operating room personnel during the procedure, although at present the patient still receives radiation as part of the procedure. 20 Some robotic systems utilize a preoperative CT, although intraoperative CT or even a single anteroposterior and lateral radiograph can be used for registration in some systems. Several studies have evaluated radiation exposure associated with robot-assisted screw instrumentation; however, radiation exposure seems to vary between studies and platforms. 5,13 Combining results from 2 RCTs, Gao et al 24 found that the use of robotic assistance could significantly lessen intraoperative radiation time (mean difference −12.38, 95% CI −17.95 to −6.80; P < .0001) and intraoperative radiation dosage (standard mean difference −0.64, 95% CI −0.85 to −0.43; P < .00001). Importantly, radiation time tends to decrease in robot-assisted groups as the total number of cases increases, indicating a learning curve effect and potential for further reduced radiation risk as surgeons become more familiar with these emerging techniques. 5,13
Expanding Uses of Robotic Systems in Spine Surgery
The best-studied application of robotics in spine surgery still lies in the domain of guidance for pedicle screw fixation at thoracic and lumbar levels; however, other uses are within reach. The Mazor systems have been adapted for S2-alar-iliac screws, 31,32 and transpedicular, transdiscal screws have been developed for guided oblique lumbar interbody fusion. 33 In addition to degenerative diseases, robot-assisted instrumentation has been used in the treatment of primary spine tumors and osteolysis associated with metastatic spinal disease. 34 The ExcelsiusGPS system has modular end effector attachments that can be used in posterior cervical instrumentation as well. The initial cost of acquisition is high, and data is still needed to evaluate the long-term financial implications of these new technologies. However, the application of robotic systems in spine surgery can be cost-effective, as these technologies could possibly reduce revision surgery and potentially shorten length of stay and operative time. 35 Further studies are crucial to understand the economic impact of robotic spine surgery.
Robotic systems have also found increasing applications in minimally invasive spine procedures. Open spine surgeries usually require extensive muscle dissection and, compared with MIS, patients who have open surgery have higher estimated blood loss, greater postoperative pain, longer hospital stays, and worse scarring. 36 -39 Robot-assisted percutaneous instrumentation with stereotactic navigation can limit ionizing radiation, while also amplifying the benefits of MIS, particularly in percutaneous instrumented lumbar fusion. This approach requires only small para-median incisions, so the transverse processes do not need to be fully exposed. This minimizes muscle dissection and reduces related complications. In an RCT with the Mazor robot, robot-assisted percutaneous instrumentation in posterior lumbar interbody fusion resulted in similar patient outcomes with significantly reduced radiation exposure and hospital convalescence compared to the conventional open technique. 21 The ExcelsiusGPS robot has been used for pedicle screw fixation in percutaneous single-position lateral interbody fusion 29 and transforaminal interbody fusion procedures. 28
Importantly, robotic systems can be integrated seamlessly into MIS procedures. After percutaneous screw placement is performed with robotic assistance, decompression can be achieved through the same incisions—for example, with an MIS retractor for laminectomy, or with an expandable tubular retractor for facetectomy and interbody placement. In robotic systems that offer real-time image guidance, this technology can be used to assess extent of bone and disc resection, as well as identify various structures. Finally, robotic spine surgery offers the potential to improve outcomes by systematically reproducing procedures and improving workflow.
Limitations of Robot-Assisted Spinal Surgery
The field of robotic spinal surgery is still in its infancy. Although multiple studies have demonstrated the improved accuracy of robotic assistance in pedicle screw instrumentation over freehand or fluoroscopy-guided techniques, the superiority of later systems, including ROSA and ExcelsiusGPS, is not well established given the dearth of prospective studies. The high cost of acquisition and learning curve currently limit more widespread clinical application.
What the Future Holds
First, navigation failure can be an issue, which could result in conversion to conventional fluoroscopy-guided or open, freehand techniques, highlighting the importance of a spine surgeon’s mastery of these traditional methods. Second, soft-tissue pressure on the instruments through a robotic arm can lead to skiving or deflection. Better-integrated software systems can enhance the robotic interface and give real-time feedback on how precisely a robotically implanted screw deviates from a preplanned trajectory. In addition, technique and tool refinements will be made specifically for use in robotic surgery. Artificial intelligence, augmented reality, and machine learning will become integral components of robotics; as these become more sophisticated, surgical robot platforms may be able to anticipate dynamic changes intraoperatively, further enhancing their accuracy and efficiency. 40 In addition, these technologies could lead to machine-guided planning of optimal pedicle screw placement based on anatomy, biomechanics, and even analysis of similar patients who have undergone surgery.
There is a learning curve for robot-assisted surgical procedures of all types. Existing user interface software can be cumbersome and unintuitive, especially to older learners. 41 -43 However, many studies have shown that as the number of procedures performed increases, accuracy of pedicle screw placement with robots improves and operating time decreases. 44,45 Success rates usually improve after 30 procedures, with less frequent conversion to nonrobotic techniques. 34 Training is imperative not only for the surgeons but also for other staff members in the operating room, highlighting the importance of teamwork and an optimized workflow. 46
Undoubtedly, the indications for robot-assisted spine surgery will continue to expand beyond pedicle instrumentation. Evolving from open and percutaneous placement of thoracic and lumbar pedicle screws, more complex applications (eg, C1-2 posterior fusion and the placement of S2-pelvic screws) will soon be achievable. Supported by advancements in navigation technology, future robots will likely be able to facilitate surgical decompression (eg, in laminectomies and osteotomies), aid in revision and deformity surgeries, and even potentially guide extra- or intradural tumor resection.
Research into robotic spine surgery will also expand over time. Specifically, large, well-designed RCTs and/or prospective registries are necessary to enrich the evaluation of these new technologies. Several studies have not found evidence for a significant difference in intraoperative and postoperative complication rates between robotic assistance and conventional techniques. 47,48 The lack of data on postoperative complications, patient-centered clinical end points and cost-effectiveness must be addressed, especially in the modern era of medicine, when quality, cost, and accessibility are key requirements for any new technology. 46 With its expanding applications and potential for reduced fluoroscopy time, shorter operating time, lower hospital length of stay, and decreased complication rates, robot-assisted spine surgery may have a positive impact on long-term health care economics.
Conclusion
The introduction of new navigation systems and robotic platforms herald a new era for spine surgery. Since the days of freehand screw placement without image guidance, spine surgery has witnessed remarkable technological advancements that have resulted in drastically improved safety and quality of care. However, the risks of complications due to instrument malpositioning, and hazardous exposure to radiation remain significant concerns. Robotic guidance for pedicle screw instrumentation is well positioned to address these issues, with multiple studies validating its accuracy and performance outcomes. Furthermore, robotic systems have the distinct advantage of refining surgical dexterity and augmenting human capability. Indisputably, the number of robot-assisted spinal surgeries will continue to rise, with more applications being added to the repertoire of this technology. Current limitations create room for further innovations, including better software systems and improved designs. Future studies should address the steep learning curve for surgeons and support staff, incorporate patient-centered clinical outcomes, and measure the cost-effectiveness of these new technologies—critical areas for patient acceptance and widespread use.
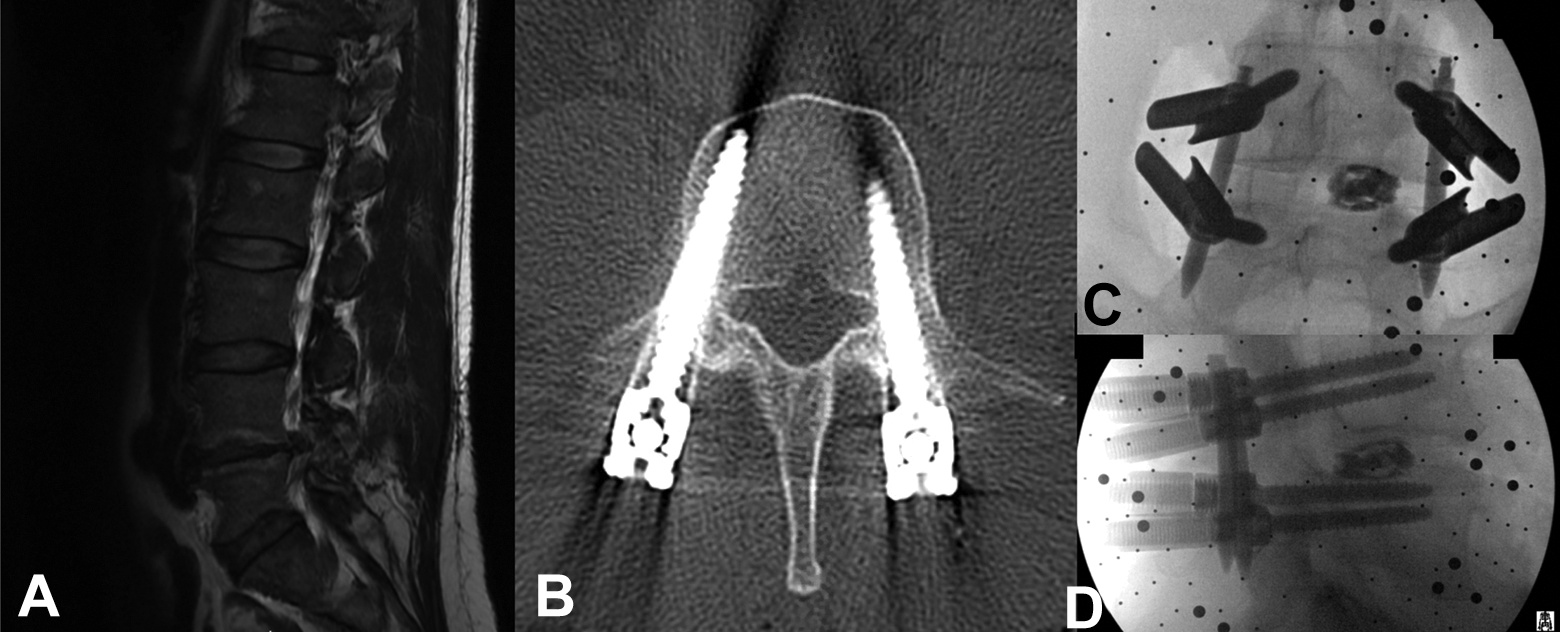
Representative case of minimally invasive surgery (MIS) for a transforaminal lumbar interbody fusion (TLIF). A man with history of right L4-L5 disc herniation and right L5 radiculopathy status-post 3 prior right-sided microdiscectomies who presented with recurrence of radicular pain. He underwent a right L4-L5 MIS TLIF with robotic guidance using the Globus ExcelsiusGPS system. (A) Lateral magnetic resonance image shows re-herniation of the right L4-L5 disc with significant lateral recess and foraminal stenosis. (B) Axial postoperative computed tomogram shows ideal placement of a transpedicular screw. (C) Postoperative frontal radiograph of L4-L5 instrumented TLIF. (D) Postoperative lateral radiograph.
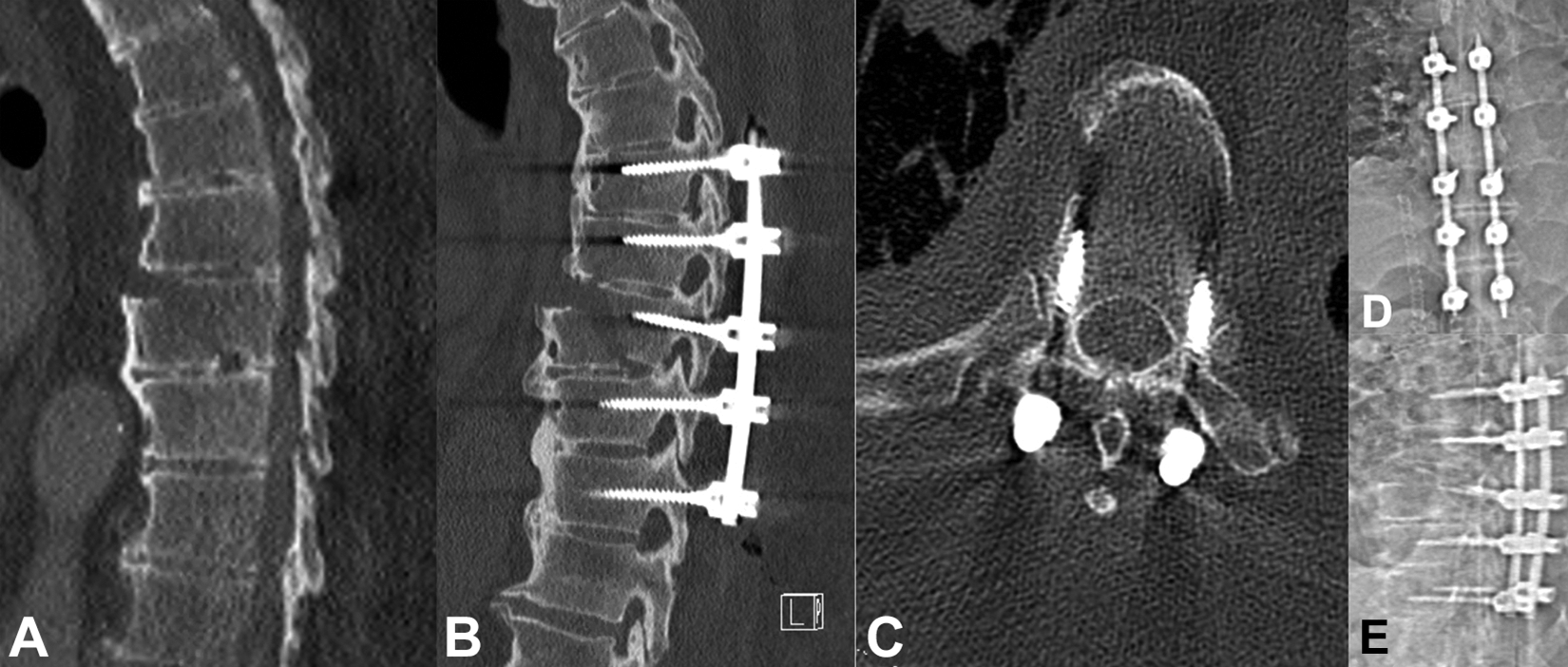
Representative case of percutaneous instrumentation for traumatic burst fracture of the thoracic spine. A man presented with back pain after significant trauma and was found to have a traumatic burst fracture of the T8 vertebral body. He underwent percutaneous T6-T10 segmental pedicle screw fixation with robotic guidance using the Globus ExcelsiusGPS system. (A) Lateral computed tomogram (CT) shows traumatic burst fracture of the T8 vertebral body. (B) Lateral postoperative CT shows T6-T10 instrumentation. (C) Axial postoperative CT shows transpedicular screw placement at the T8 vertebral body. (D) Postoperative frontal radiograph. (E) Postoperative lateral radiograph.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The Excelsius GPS robot described in this presentation was invented by Drs Theodore and Crawford and is manufactured by Globus Medical. They are both entitled to royalty payments on sales of the robot. Dr Theodore is also a paid consultant to Globus Medical and owns Globus Medical stock. Dr Crawford is an employee of Globus Medical.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This supplement was supported by funding from the Carl Zeiss Meditec Group.