
Abstract
Study Design
Prospective multicenter cohort study.
Objectives
Integration of robotic guidance with navigation represents a natural evolution in spine surgery technologies. Both modalities have independently demonstrated improved implant accuracy, reduced radiation exposure, and expanded minimally invasive capabilities, yet data on integrated platforms remain limited. The Prospective Robotic-Guided Registry of Spine Surgery (PRoGRSS) evaluates surgical, clinical, and patient-reported outcomes across a broad range of procedures performed with an integrated robotic-assisted navigation system.
Methods
Adults undergoing navigated robotic thoracolumbar surgery between 2020 and 2024 were enrolled by six surgeons across four centers. Demographic, surgical, and robot-related metrics were collected. Patient-reported outcomes included ODI and PROMIS Global Health, Physical Function, and Pain Interference. Complications, revision surgery, inpatient resource utilization, and return-to-work metrics were analyzed.
Results
Of 657 enrolled patients, 606 completed 12-month follow-up (92%). Median age was 60 years; 49.9% were female. Of 5166 planned screws, 99.2% were placed, with 98.4% accurately positioned and 1.5% malpositioned. Robot abandonment occurred in 0.6% of cases. Robot-related intraoperative or postoperative adverse events occurred in 0.3% of cases. Twelve-month revision surgery rate was 4.8%, including 0.3% robot-related revisions. Resource utilization was low: 5.2% required transfusion, 2.1% postoperative CT, median length of stay was 3 days, and 88.4% were discharged home. Patients demonstrated significant, clinically meaningful improvement across all PRO domains.
Conclusions
This large prospective evaluation of an integrated navigation–robotic platform demonstrates high accuracy, low complication and revision rates, efficient resource use, and substantial patient-reported outcome improvement, establishing a contemporary benchmark for navigated robotic spine surgery.
Keywords
Introduction
As operating room technologies continue to advance, processes that were once highly variable are becoming increasingly automated in spine surgery. Yet, the true cost and value of these innovations remain under scrutiny.1,2 Since the first robotic spine platform received FDA clearance in 2004, multiple generations and new models of robotic and navigation systems have been developed, each accompanied by studies demonstrating improved implant placement accuracy, reduced radiation exposure to the surgical team, and expanded applications for minimally invasive surgery.3–21
The most recent evolution of integrating robotic guidance with real-time navigation confirmation represents a pivotal step toward more consistent and reliable outcomes across a broad spectrum of spinal fusion procedures, including complex deformity and revision cases. These technologies allow for detailed preoperative planning that accounts for anatomical variations, potentially enhancing both surgical precision and patient outcomes.4,7,15,22–25 As the market for integrated navigation and robotic platforms in spine surgery continues to expand, available data remain limited, largely derived from earlier-generation systems, and with limited insight into their economic value (Figure 1).1,2,7,8,26–29 Timeline of FDA approvals and US launches of robotic-navigation spine systems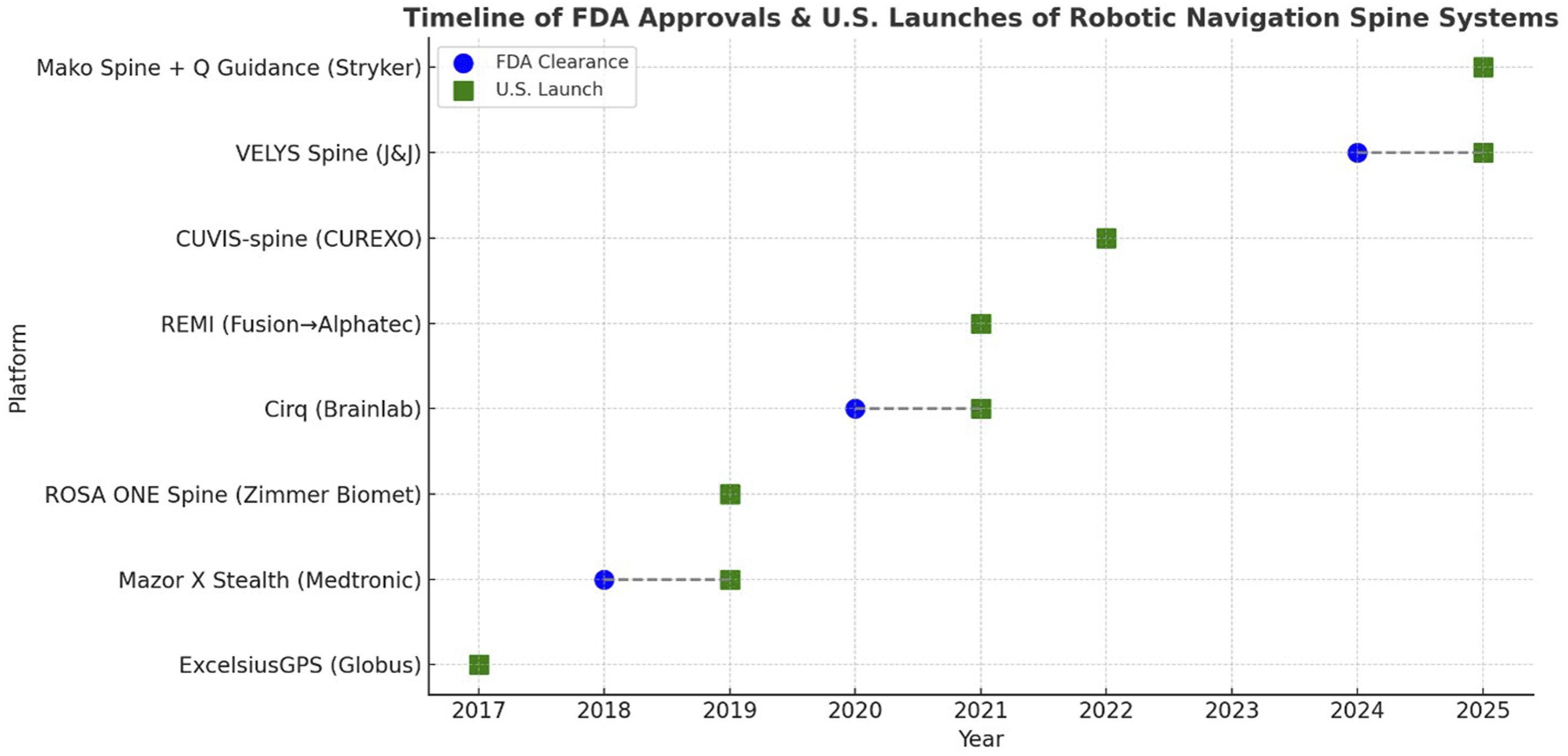
The Prospective Robotic-Guided Registry of Spine Surgery (PRoGRSS) was established to address this gap. This first-of-its-kind, multicenter study brings together experienced users from geographically diverse institutions to evaluate outcomes specific to a single integrated platform, the Mazor X Stealth Edition (MXSE). Beyond accuracy and complication rates, PRoGRSS assesses patient-reported outcomes, return-to-work metrics, and inpatient healthcare resource utilization to provide a comprehensive understanding of the real-world impact of navigated robotic spine surgery which can be used for future benchmarking.
Materials and Methods
Study Design and Patient Selection
This multicenter cohort study analyzed data collected between 2020 and 2024, which included data from 6 fellowship trained spine surgeons at 4 distinct centers spanning 3 US regions. Each surgeon’s experience using navigation and robotics was advanced, defined as years of regular use. Adult patients (18 years or older) undergoing thoracolumbar fusion surgery using the bone-mounted robotic-navigation confirmation platform (MXSE) were screened for study participation. Patients with a primary diagnosis of trauma, tumor, or infection were excluded. Patients were followed for 12 months after surgery. Study data was collected at six timepoints, including preoperatively, intraoperatively, during the hospitalization, and postoperatively at approximately 2 weeks, 3 months, and 12 months. Institutional Review Board approvals for PRoGRSS were obtained by the sponsor, the National Spine Health Foundation, and each contributing site. The published interim analysis for PRoGRSS reports 90-day medical and surgical complications and revision surgery rates. 30 This study is registered with the NIH National Library of Medicine on https://ClinicalTrials.gov as: Prospective Robotic-Guided Registry of Spine Surgery (PRoGRSS) ID# NCT05181098.
Data Collection
Patient demographics, comorbid factors, primary diagnosis, and preoperative Patient Reported Outcomes (PROs) were collected. In addition to the Oswestry Disability Index (ODI), PROMIS short forms for Physical Function (PF), Pain Interference (PI), and Global Health (GH), the latter including both physical and mental health domains, were collected. Intraoperative variables were collected including operative details, instrumentation data, fluoroscopic time, and adverse events. Postoperatively, surgical complications, revision surgeries, and PROs were also collected. Surgical complications were recorded per patient and per unique event to differentiate between those with more than one complication. Surgical complications and revision surgeries were categorized as being robot related or not. There is currently no standardized, validated classification system for defining “robot related” surgical complications in spine surgery. In this study, events were defined as robot related when they were attributable to device malfunction, registration or targeting error, workflow interruption, or other technical fault specific to the robotic system or its interface with navigation. Examples include implant related durotomy, robot associated durotomy, and robotic related vascular injury.
Instrumentation data specific to the navigated robotic system were collected. Variables included the total number of planned screws using the robotic planning software, the number of screws successfully registered intraoperatively, the number of screws placed with robotic guidance and navigation confirmation, and the number of screws that were either not registered or not placed. Planned screws that were not registered or placed were classified as either robot related or non–robot related. Non–robot related screws included those designated in the preoperative plan as backup or optional, to be used at the surgeon’s discretion based on intraoperative findings. For instance, screws planned for backup at the level above the upper instrumented vertebra were counted as non–robot-related, as they were not intended or executed within the robotic plan. Robot related screws referred to those intended for placement but not captured during registration, typically due to image-registration mismatch, tracking or communication errors, or system safety interlocks, reflecting both the technical sensitivity and built-in safeguards of the platform.
Following physical attachment of the robotic arm to the patient, “robot time” was defined as the interval beginning with activation of the mount function, which initiates system recognition and confirmation of the mechanical connection, and ending after completion of the final screw trajectory movement. This period encompassed the registration and verification processes but excluded instrumentation planning. For CT-to-Fluoroscopy (“scan-and-plan”) cases, planning was performed intraoperatively after image acquisition and therefore preceded robot time. For preoperative CT-based cases, the robotic plan was imported and registered intraoperatively prior to the onset of robot time. Accordingly, this definition consistently represented the active robotic phase across both workflows.
Robot time per screw was calculated as the total robot time (end time minus start time) divided by the number of screws placed with robotic guidance. Consequently, the calculated robot time per screw includes registration and verification, resulting in a longer total time than the actual period required for robotic trajectory guidance, screw placement, and navigation confirmation. Similarly, total case fluoroscopy time included all intraoperative exposures, including those obtained for robotic registration and verification. As a result, fluoroscopy time per screw reflects total case exposure and includes registration and confirmation imaging in addition to screw placement.
As part of the PRoGRSS protocol, intraoperative 3D imaging was performed after completion of instrumentation. Screw placement accuracy was assessed by the operating surgeons through review of the 3D scan in conjunction with neuromonitoring screw stimulation data. Screws were classified as either acceptable or malpositioned. A screw was considered acceptable if it was contained within the pedicle on 3D imaging. A screw was considered malpositioned if it was revised, replaced, or removed before completion of the index procedure. Both malpositioned screws and screws not executed due to registration failure were categorized as robot related.
Statistics
Statistical analysis and sample size calculations were performed using SAS software (Version 9.3; SAS Institute Inc, Cary, NC). Categorical data was summarized using frequencies and percentages, median and interquartile range for nonparametric data, and mean with standard deviation for parametric data. Variables with missing data were not imputed. ODI change scores were calculated as the difference between 12-month and preoperative values (Δ = 12 mo. – preop), with negative values indicating improvement. The magnitude of change was interpreted relative to published minimal clinically important difference (MCID) thresholds for lumbar spine surgery, typically ranging from 10 to 15 points, with 12.8 points commonly cited for lumbar fusion procedures. 31 PROMIS measures were scored as T-scores, which are standardized to a U.S. general population mean of 50 and a standard deviation (SD) of 10. Higher scores indicated better functioning for Physical Function and Global Health, and greater symptom burden for Pain Interference. For each domain, 95% confidence intervals (CIs) were calculated around the T-scores using standard error estimates derived from item response theory–based scoring algorithms.
Within-subject change was calculated as the difference between the 12-month postoperative and preoperative T-scores (Δ = 12 mo. – preop). The mean change and corresponding 95% CIs were then derived from these individual change scores. To aid interpretation, changes were evaluated against published MCID reference values and also expressed in SD units of the PROMIS T-score metric, allowing comparison of effect magnitude across domains. Effect sizes were interpreted according to conventional thresholds described by Jacob Cohen with values of 0.2 SD, 0.5 SD, and 0.8 SD representing small, moderate, and large effects, respectively. 32 These thresholds have been shown to correspond broadly to minimally important within-person changes across health measures and align with the 2-6 T-point within-group minimal important change range suggested for PROMIS instruments.33,34 Accordingly, a 5-point T-score change represents approximately a moderate (0.5 SD) effect, while a 10-point change represents a large (1.0 SD) effect.
Results
Enrollments
PRoGRSS had 791 patients screened for inclusion, of which 720 patients were enrolled in the study. While 688 of 720 patients completed the preoperative visit, a total of 657 went on to have their fusion using navigated robotic guidance. Of those, 97.2% completed the first postoperative visit at approximately 2 weeks and 92.2% completed the 3- and 12-month postoperative visits (Figure 2). The study completion rate (surgery to final follow up) for PRoGRSS was 92%. Study flow diagram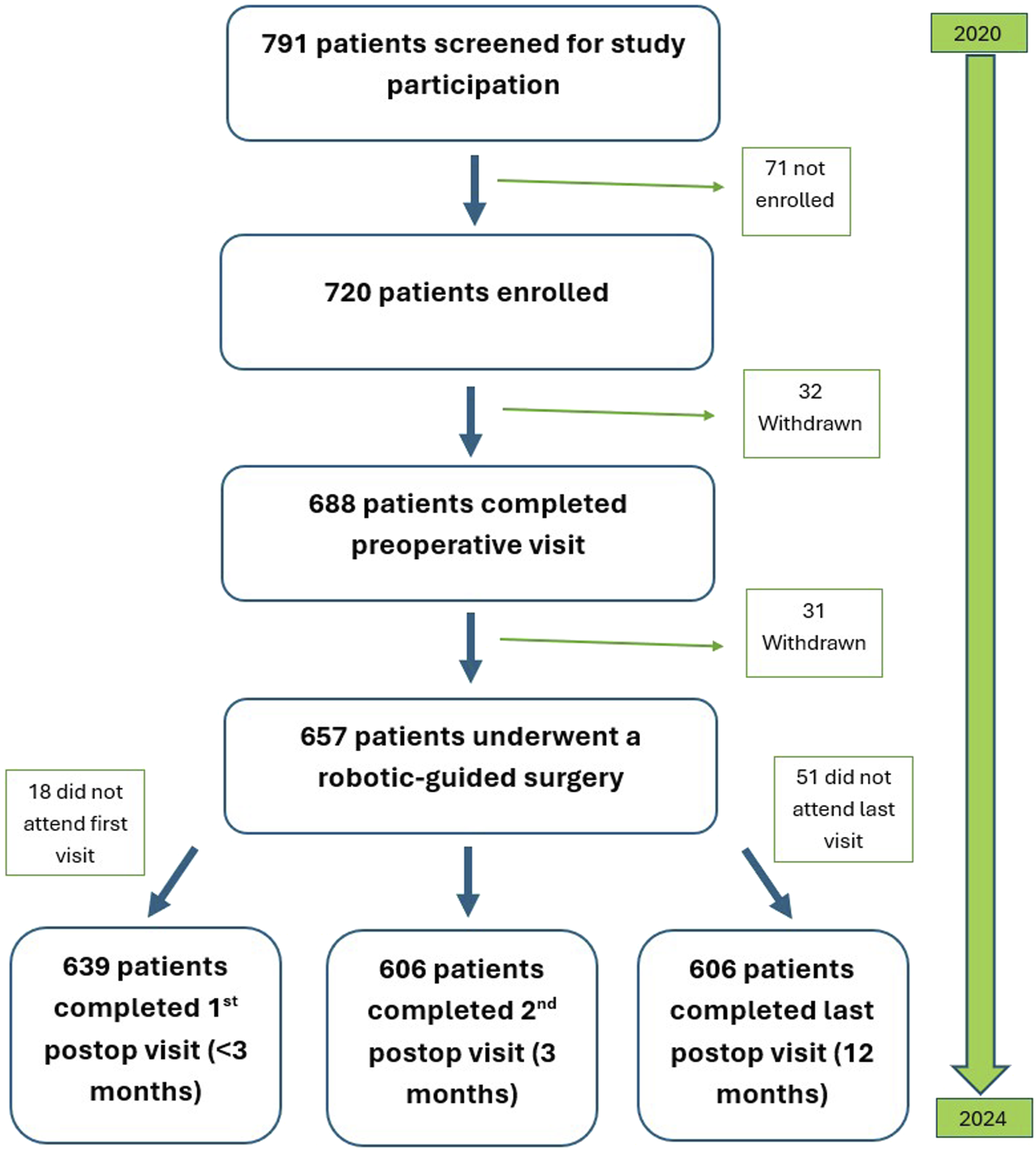
Demographic Factors
Patient Characteristics
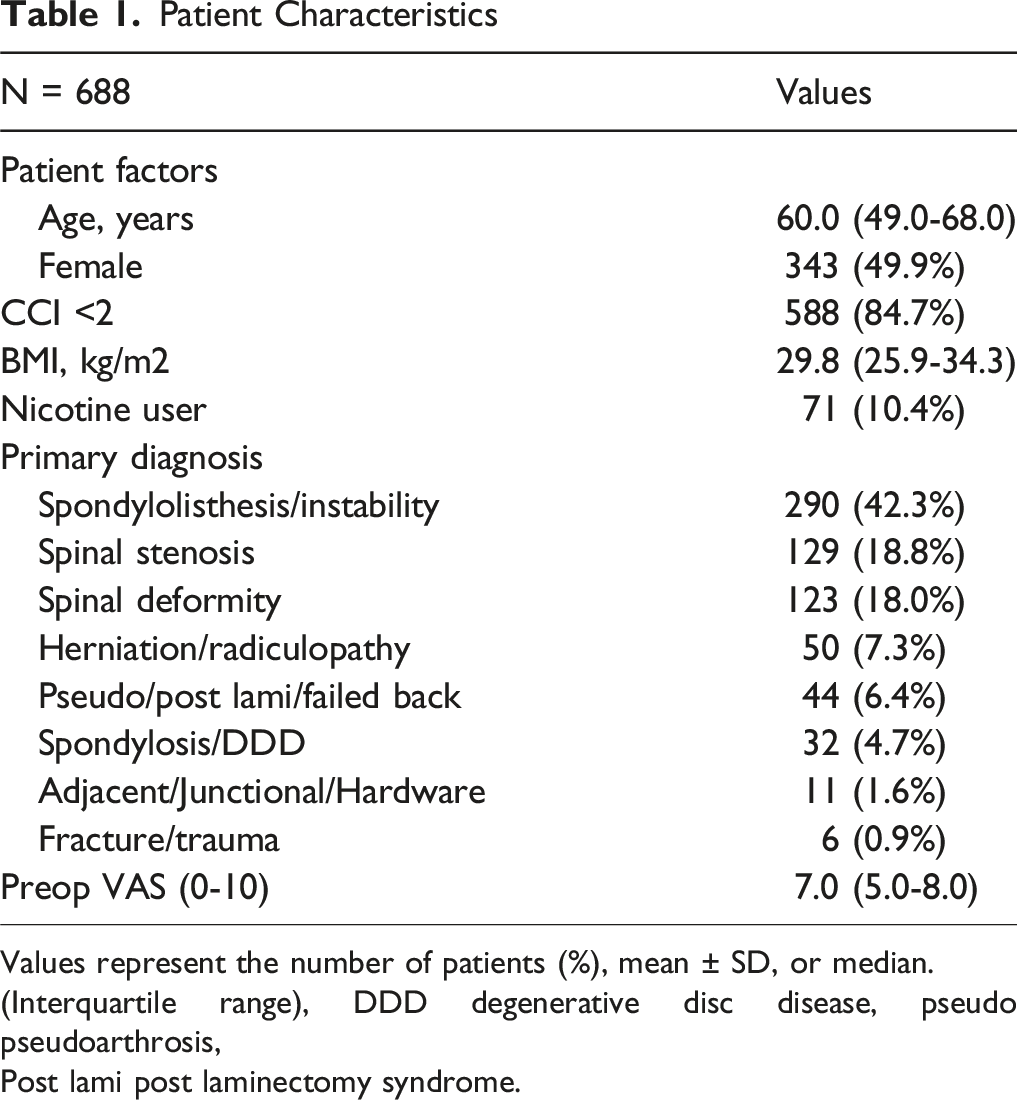
Values represent the number of patients (%), mean ± SD, or median.
(Interquartile range), DDD degenerative disc disease, pseudo pseudoarthrosis,
Post lami post laminectomy syndrome.
Surgical Details
Operative Factors
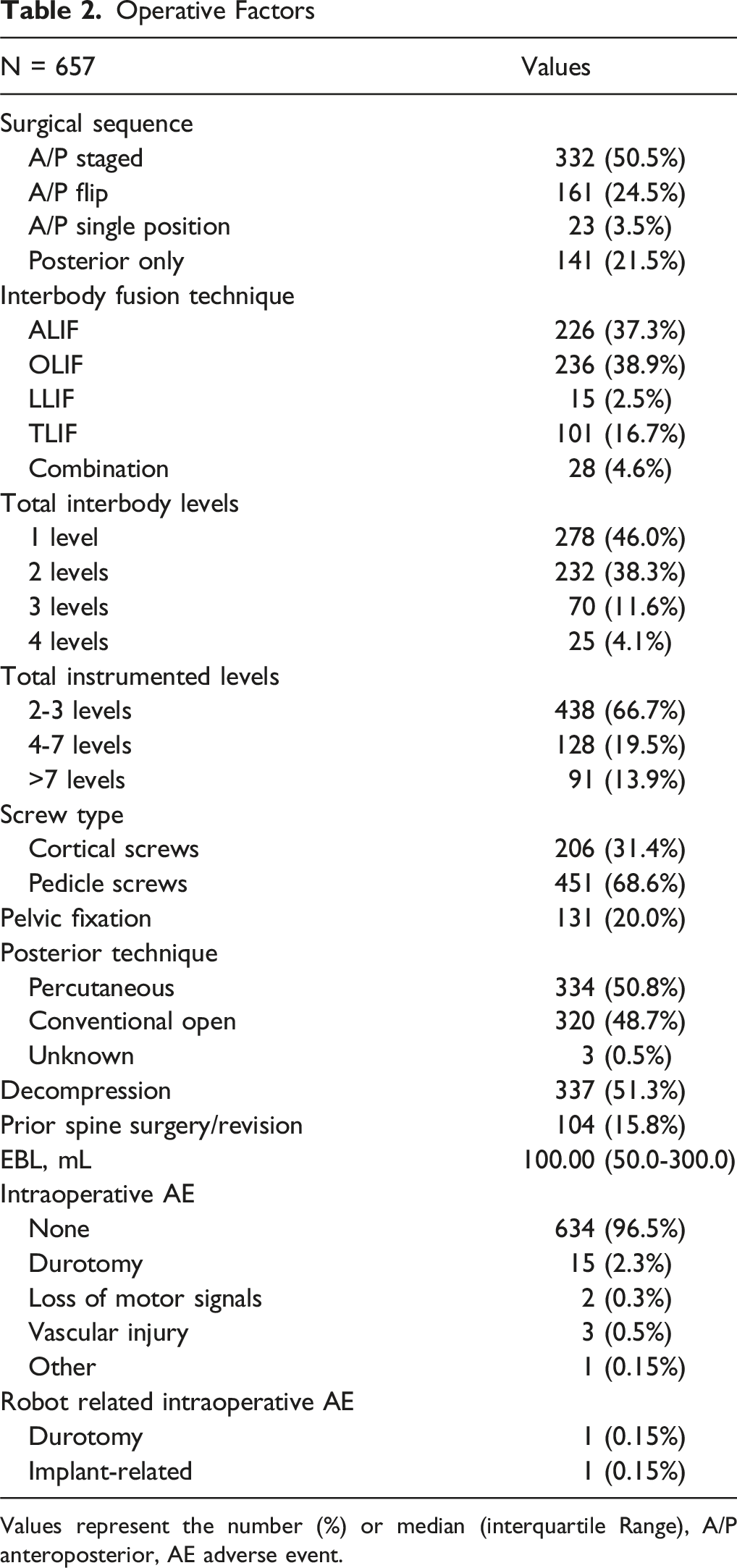
Values represent the number (%) or median (interquartile Range), A/P anteroposterior, AE adverse event.
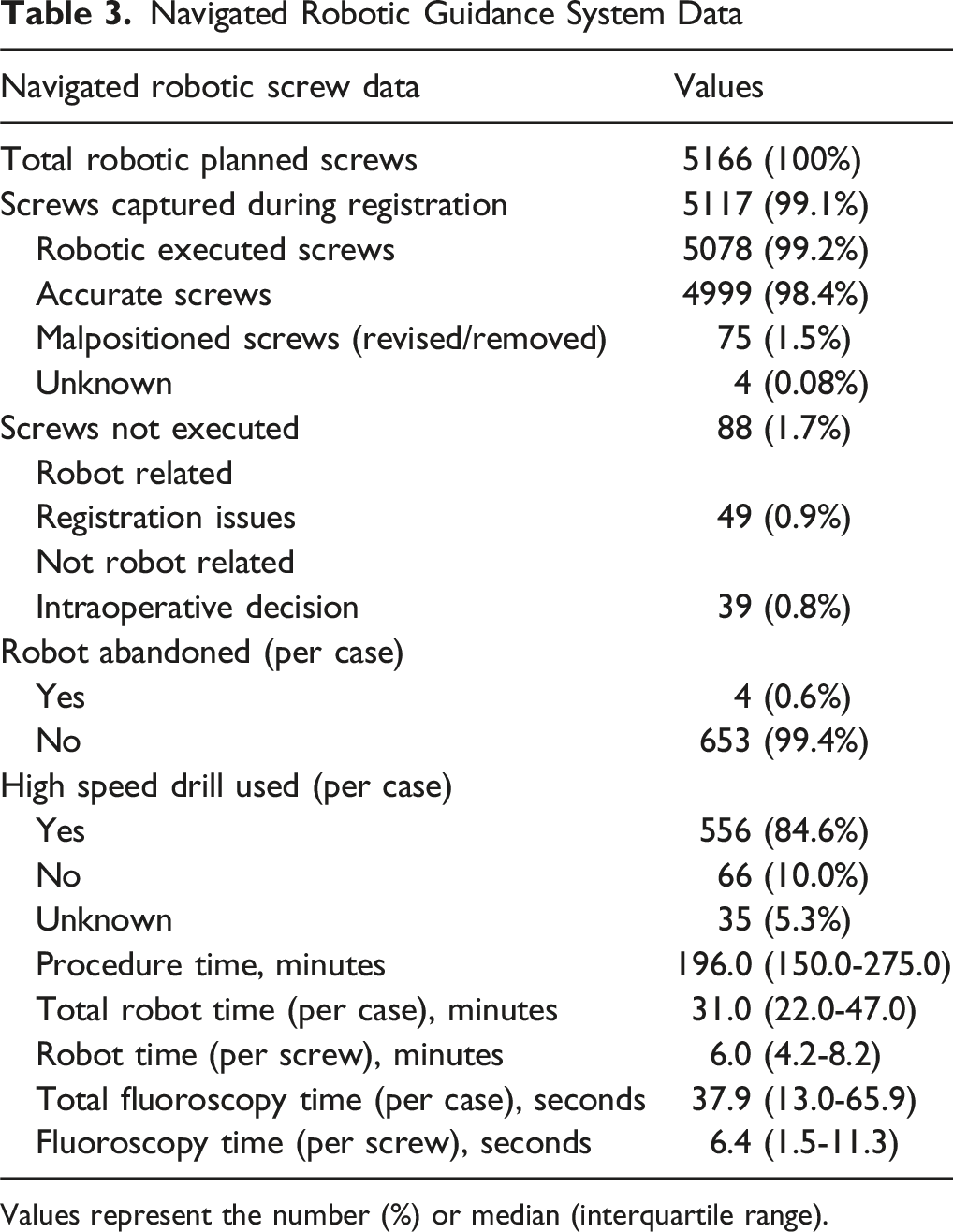
Navigated Robotic Guidance System Data
The median robot time per case was 31.0 (22.0-47.0) minutes, robot time per screw was 6.0 (4.2-8.2) minutes, and the robot was abandoned in 0.6% of cases that were due to registration issues in all four cases. There were 5166 planned screws and of those, 5117 (99.1%) were captured during the registration process. The total number of executed screws using navigated robotic guidance was 5078 (99.2%), of which 75 (1.5%) screws were revised, replaced, or removed, resulting in a 98.4% intraoperative acceptability rate for screw placement (Figure 3). Of 5166 planned screws, 88 (1.7%) screws were either not captured during registration (0.9%) or not executed at the surgeon’s discretion (0.8%). Screws not executed due to registration issues were categorized as robot related. The high-speed drill, introduced after study initiation with the MXSE platform, was used in 84.6% of cases. Median fluoroscopy time per case was 37.9 seconds and per screw was 6.4 seconds (Table 3). Horizontal bar chart illustrating the navigated robotic screw workflow, including the number of screws planned preoperatively, captured during robotic registration, executed using navigated robotic guidance, and the corresponding placement accuracy breakdown Navigated Robotic Guidance System Data Values represent the number (%) or median (interquartile range).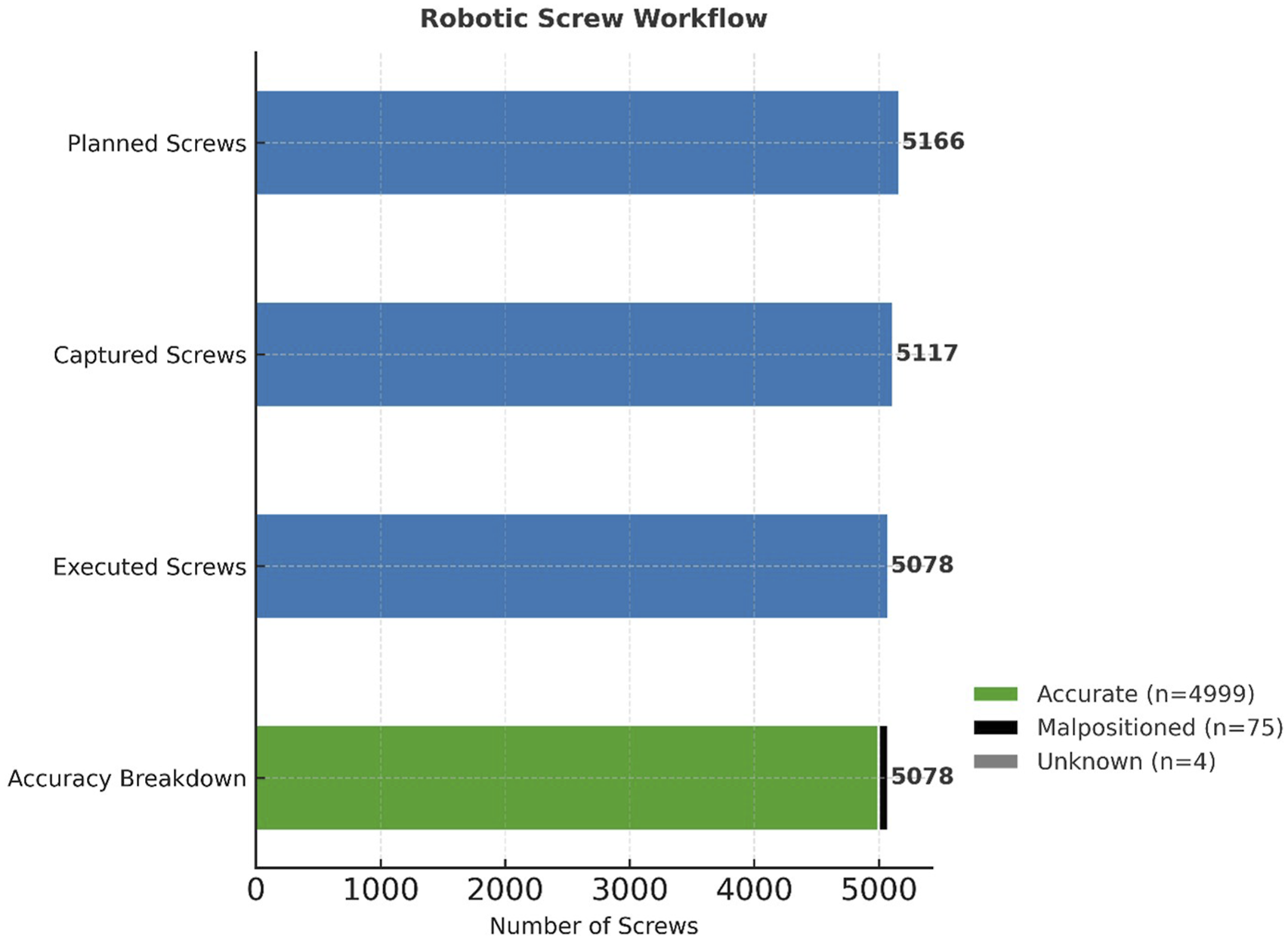
Surgical Complications and Revisions
Complications and Revisions
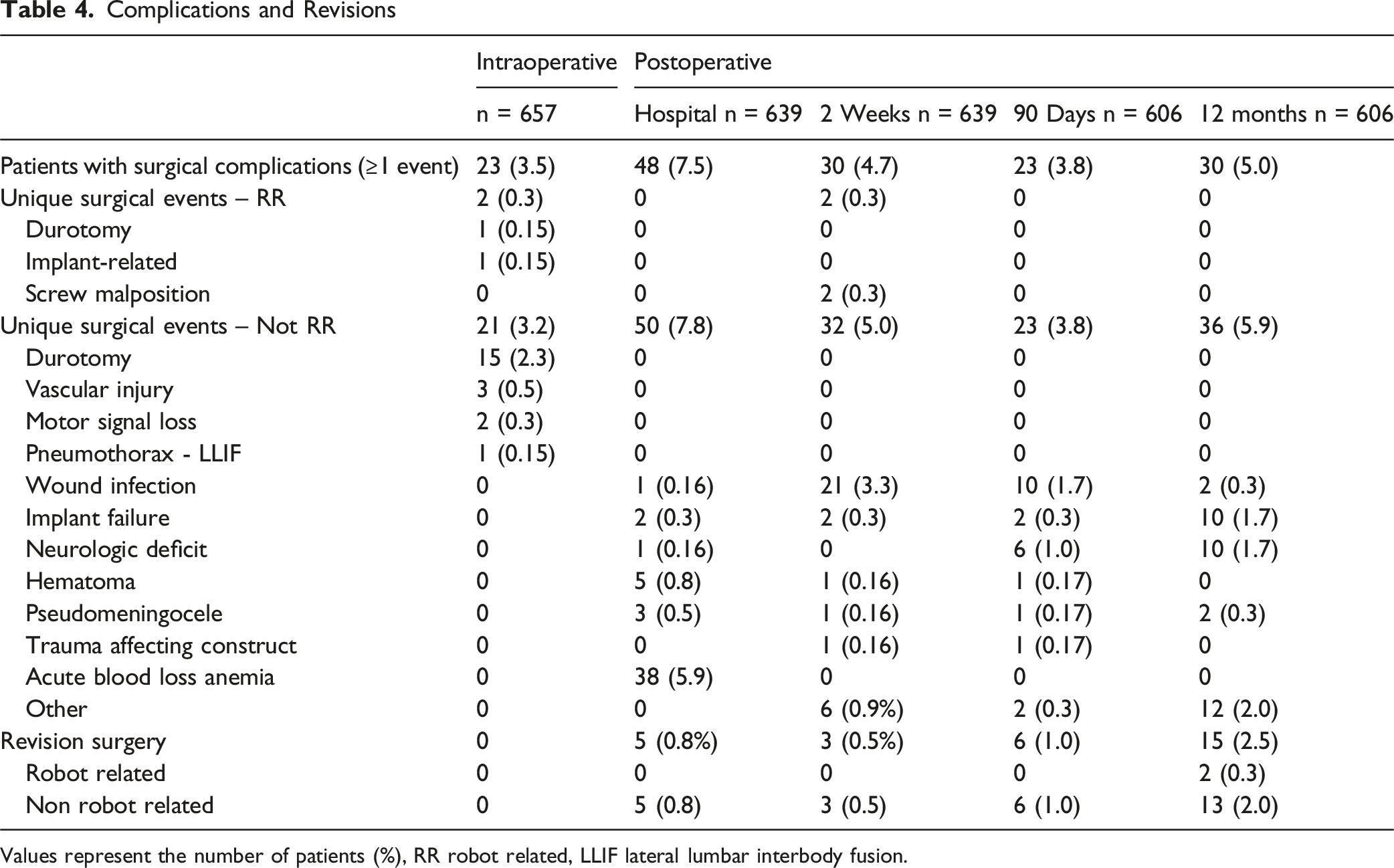
Values represent the number of patients (%), RR robot related, LLIF lateral lumbar interbody fusion.
The most common postoperative surgical events not related to the robot included acute blood loss anemia in 38 patients (5.9%) during the index hospitalization, wound infection in 21 patients (3.3%) by the first postoperative visit and 10 patients (1.7%) within 90 days, and 12 events (2.0%) classified as “other” up to 12 months. Events in the “other” category included proximal junctional kyphosis or failure, adjacent segment disease, pseudoarthrosis, leg pain without neurologic deficit, and stenosis (Table 4).
A total of 29 revision surgeries were performed within 12 months of the index procedure. Five revisions (0.8%) occurred during the index hospitalization for subsidence, cage repositioning, or hematoma evacuation. Three revisions (0.5%) were performed by the first postoperative visit (∼2 weeks) for wound incision and drainage or seroma evacuation. At 90 days, six revisions (1.0%) were required for subsidence, decompression, wound incision and drainage, or extension of fusion. Between 90 days and 12 months, 15 revisions (2.5%) were performed, including decompression, extension of fusion, coronal alignment adjustment, instrumentation removal, and revision fusion. Two (0.3%) revision procedures for hardware removal were attributed to robotic factors (Table 4).
Hospital Course and Inpatient Resource Utilization
Inpatient Resource Utilization Outcomes
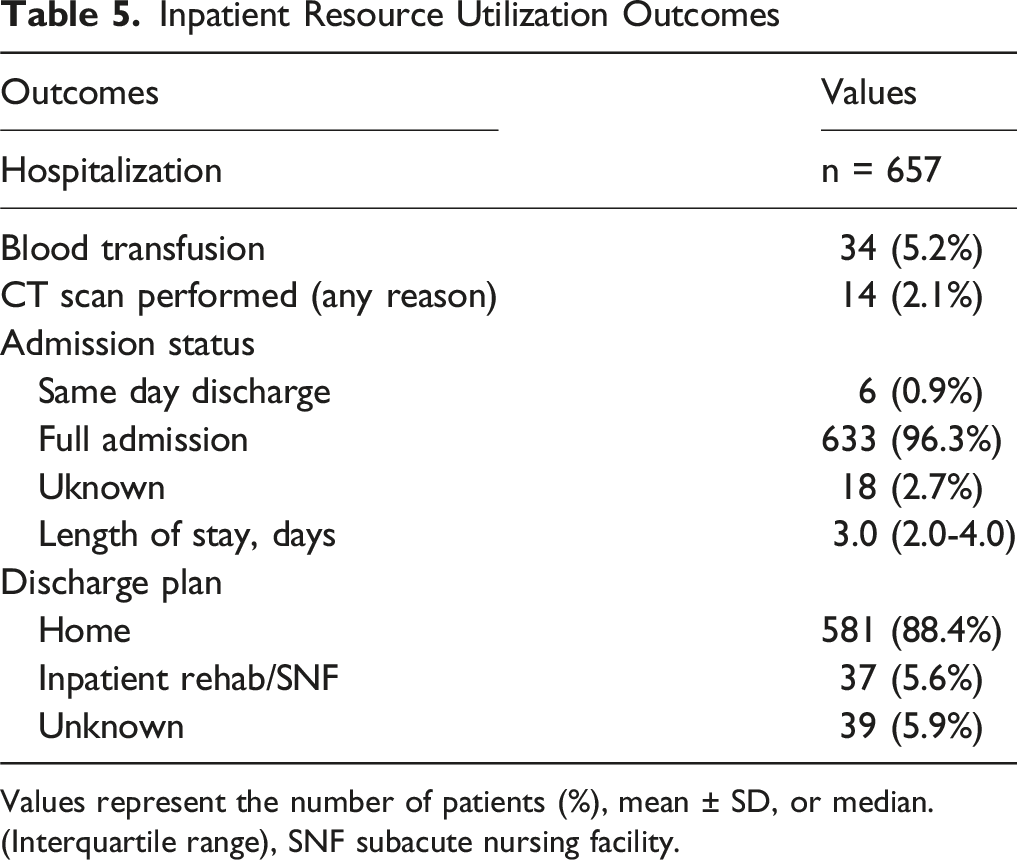
Values represent the number of patients (%), mean ± SD, or median.
(Interquartile range), SNF subacute nursing facility.
Return to Work
Work Status Outcomes
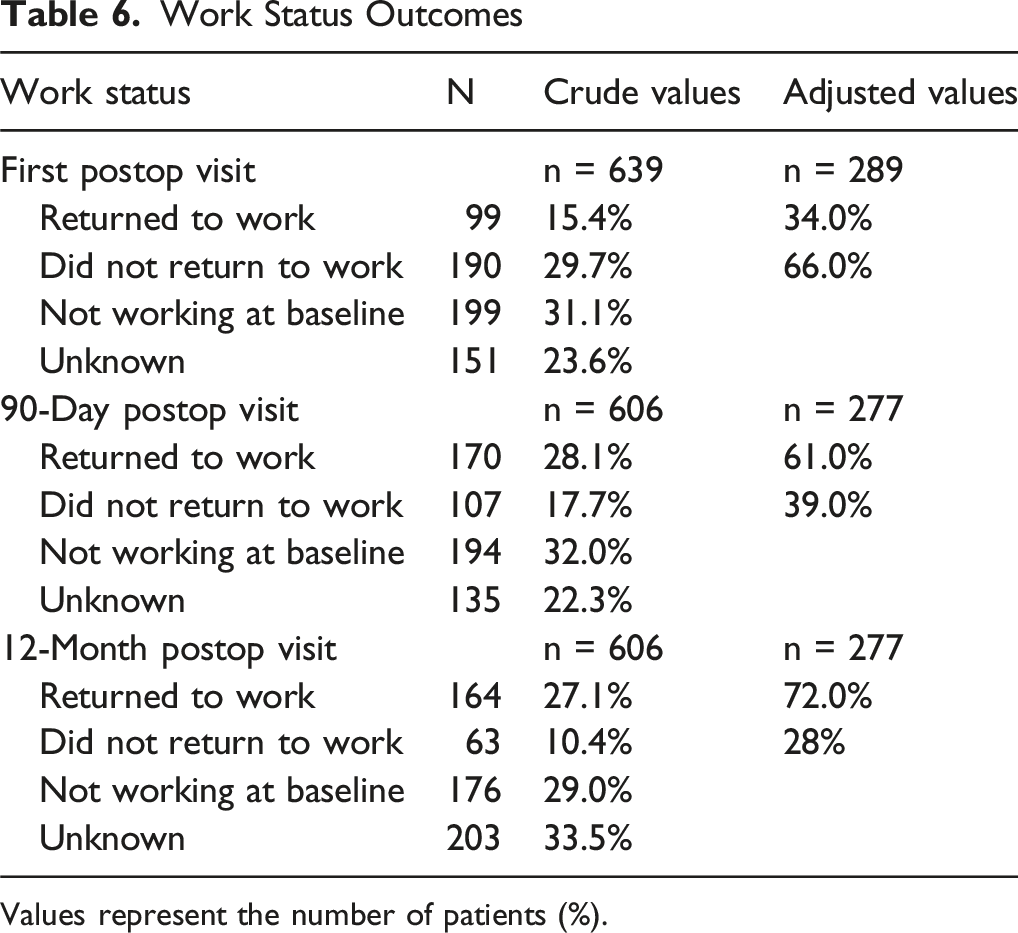
Values represent the number of patients (%).
To account for these limitations, return-to-work rates were recalculated excluding patients not working at baseline and those with unknown work status. Using this adjusted denominator, 34% of eligible patients returned to work at the first postoperative visit, increasing to 61% at 90 days and 72% at 12 months. The corresponding proportions of eligible patients not returning to work were 66% at the first postoperative visit, 39% at 90 days, and 28% at 12 months (Table 6, Figure 4). Return-to-work status following surgery. Crude percentages (relative to the full cohort) are shown alongside adjusted rates, which exclude patients not working at baseline and those with unknown work status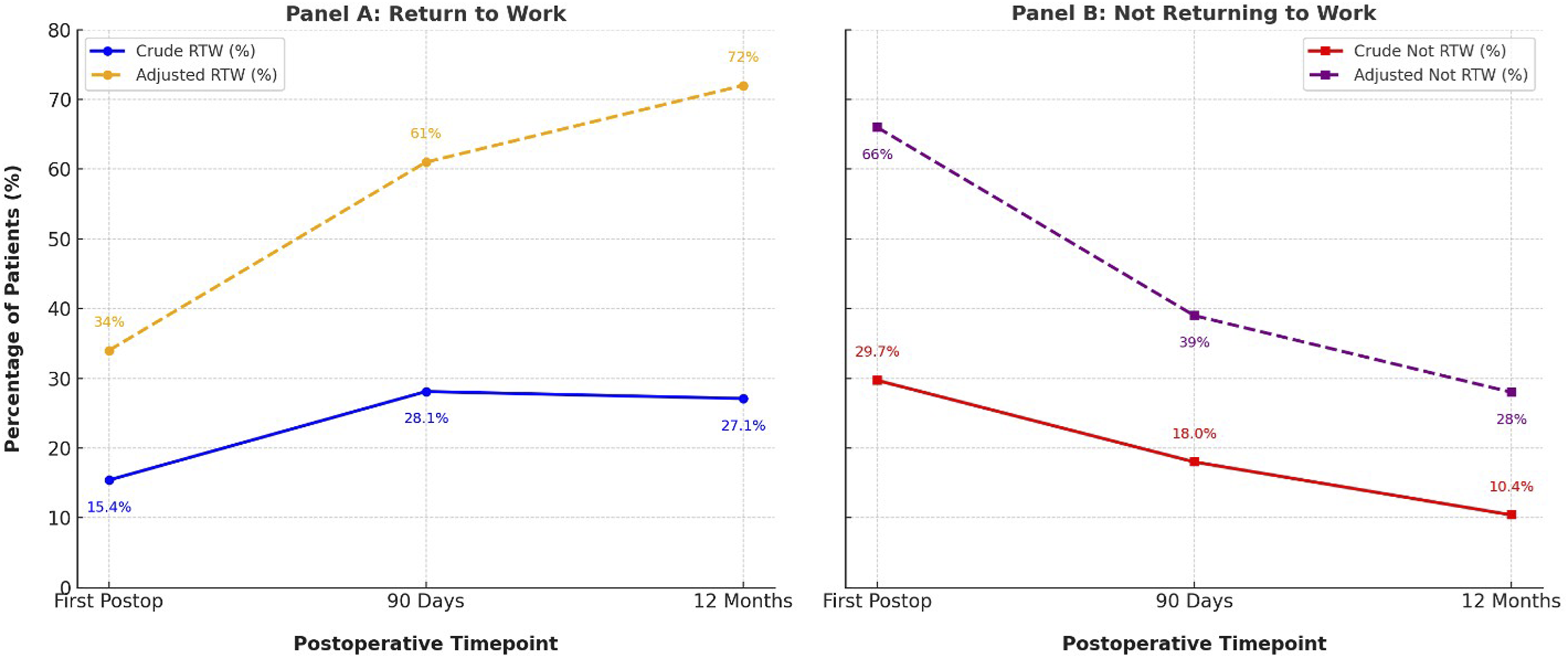
Patient Reported Outcomes
The median Oswestry Disability Index (ODI) score was 44.0 preoperatively, consistent with moderate disability as classified by standard interpretive thresholds. Scores increased slightly at 2 weeks (46.7) and improved to 20.0 at 12 months, representing a median reduction of 18.0 points. This exceeds the commonly cited MCID (10-15 points; 12.8 for lumbar fusion), indicating a clinically meaningful improvement in disability one year after surgery (Table 7).
The mean PROMIS Pain Interference score was 65.4 preoperatively, approximately 1.5 SD above the population norm of 50. Scores increased slightly at 2 weeks (66.1) and improved to 55.7 at 12 months, representing a mean change of −10.1 T-score points (1.0 SD, large effect size). This reduction exceeds both the spine surgery–specific MCID (3-5 T-points) and the general PROMIS minimal important change range (2-6 T-points), indicating a large and clinically meaningful decrease in pain interference by one year postoperatively (Table 7).
Patient Reported Outcomes
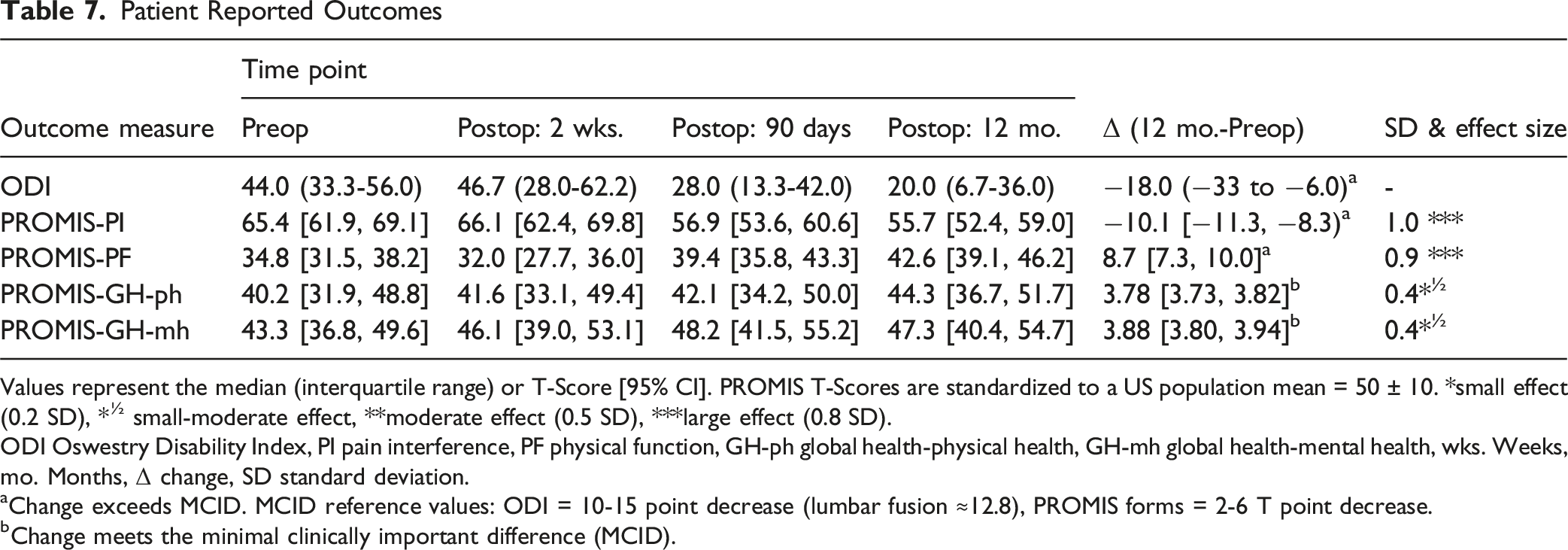
Values represent the median (interquartile range) or T-Score [95% CI]. PROMIS T-Scores are standardized to a US population mean = 50 ± 10. *small effect (0.2 SD), *½ small-moderate effect, **moderate effect (0.5 SD), ***large effect (0.8 SD).
ODI Oswestry Disability Index, PI pain interference, PF physical function, GH-ph global health-physical health, GH-mh global health-mental health, wks. Weeks, mo. Months, Δ change, SD standard deviation.
aChange exceeds MCID. MCID reference values: ODI = 10-15 point decrease (lumbar fusion ≈12.8), PROMIS forms = 2-6 T point decrease.
bChange meets the minimal clinically important difference (MCID).
The mean PROMIS Global Health–Physical Health score was 40.2 preoperatively, approximately 1 SD below the population norm of 50. Scores improved to 44.3 at 12 months, representing a mean change of +3.78 T-score points (0.4 SD, small-moderate effect size). Mean PROMIS Global Health–Mental Health scores increased from 43.3 preoperatively to 47.3 at 12 months, a mean change of +3.88 T-score points (0.4 SD, small-moderate effect size). Both global health domains demonstrated improvements consistent with the minimal important change range (2-6 T-score points) reported for PROMIS measures, indicating clinically meaningful gains in patient perceived physical and mental health by one year postoperatively (Table 7).
Discussion
PRoGRSS is the first, prospective, large-scale study focused solely on spine surgery outcomes using an integrated robotic-assisted navigation system in an optimized-use setting. Among 5166 planned screws, 99.2% were placed using robotic guidance, with 98.4% intraoperative acceptability rate (1.5% revised, replaced, removed) and a robot abandonment rate of 0.6% of cases. Median fluoroscopy time per case was 37.9 s and per screw was 6.4 s. Robot related adverse events were rare (0.3% intraoperative, 0.3% postoperative). The 12-month revision rate was 4.8%, with 0.3% robot related. Inpatient resource utilization was low, with 5.2% transfusions, 2.1% CT imaging, median 3-day stay, and 88.4% home discharge. Patients presented with substantial disability and pain but achieved clinically meaningful improvements in all domains, exceeding minimal important differences for ODI and PROMIS Pain Interference and Physical Function.
In addition to reaffirming the safety and accuracy of navigated robotic spine surgery, the final PRoGRSS analysis identifies measurable outcomes that may translate into healthcare value. Hospital course metrics reflect efficient inpatient recovery and judicious resource use, with a median length of stay of three days, low transfusion (5.2%) and limited postoperative imaging (2.1%) rates despite multilevel constructs and 13.9% with more than seven instrumented levels. These findings suggest that the integration of robotic guidance with real-time navigation may facilitate more precise surgical execution, reducing intraoperative variability and postoperative resource requirements, factors that can affect cost containment and care efficiency. The high proportion of patients discharged home (88.4%) further underscores the potential for navigated robotics to contribute to rapid functional recovery and minimize downstream utilization.
Functional restoration is a critical dimension of value-based care, and the return-to-work trajectory observed in PRoGRSS suggests socioeconomic benefit. When restricted to patients working preoperatively, 61% had resumed employment within 90 days and 72% by one year, reflecting reintegration of patients into productive activity. This finding provides real-world evidence of postoperative functional recovery in this cohort and may serve as a hypothesis-generating observation for future comparative or cost-effectiveness studies.
Patient-reported outcome measures reinforce these value-based trends. Improvements across ODI and PROMIS domains exceeded MCID thresholds, indicating meaningful gains in physical function, pain reduction, and overall health perception. The magnitude of change, particularly the 18-point median improvement in ODI and one SD improvement in PROMIS Pain Interference, demonstrates that patients derive significant quality-of-life benefits from navigated robotic fusion beyond technical success alone. From a value perspective, this alignment of safety, functional restoration, and patient-reported benefit supports the argument that advanced surgical technologies can yield durable, patient-centered returns when deployed effectively.
When considered alongside these clinical and functional benefits, the markedly lower exposure to fluoroscopy observed in PRoGRSS, approximately 50-60% less than robotic-guided and 75% less than fluoroscopic-guided cases in MIS ReFRESH, further illustrates the efficiency and safety advantages that contribute to overall procedural value. 16 By combining navigation confirmation with robotic guidance, the integrated MXSE platform contributes to both workflow precision and meaningful reductions in radiation exposure to the surgical team, aligning technological reliability with measurable improvements in patient-centered and system-level outcomes.
As experienced users of this technology, the surgeon authors note the practical advantage of the high resolution, 3D, segmental preoperative planning robotic software. The ability to pre-plan implant location, trajectory, and size, screw head cadence for easier rod passage, rod size and contouring, deformity correction, precise bone cutting, facet decortication, osteotomies, and skin incision to minimize tissue disruption all contribute to the predictability and success of the surgery. In addition, surgeon expertise in using the technology plays another significant role.
No study is without limitations, including limitations inherent to prospective registries and studies with 12 months of follow up. The outcome of intraoperative acceptability of screw placement was defined as the absence of intraoperative screw revision or removal after surgeon review of intraoperative 3D imaging and screw stimulation neuromonitoring data which may overestimate true anatomic accuracy. By limiting PRoGRSS to surgeons with advanced experience and including only one robotic platform, variability associated with surgeon experience and different platforms was minimized, however PRoGRSS is unable to capture details or outcomes associated with the learning curve, which is commonly discussed in relation to screw guidance systems and findings may not be generalizable across other platforms with different architectures, workflows, or learning curves. PRoGRSS does not include a matched control cohort, therefore the observed outcomes cannot be directly compared to alternative techniques. Finally, PRoGRSS measures surrogate indicators of healthcare value rather than direct financial metrics such as cost per case, reimbursement data, or cost-effectiveness ratios.
Conclusion
The final analysis of PRoGRSS suggests that experienced surgeons using an integrated navigation and robotic platform achieve low complication and revision surgery rates in thoracolumbar spine surgery. Collectively, the PRoGRSS findings extend beyond conventional measures of implant accuracy to encompass dimensions of efficiency, recovery, and patient-perceived benefit, key pillars of value-based spine care. By demonstrating low complication and revision rates alongside efficient inpatient resource utilization and meaningful functional recovery, this study provides early evidence that integrated navigation–robotic systems have the potential to achieve both clinical reliability and economic relevance while serving as a useful benchmark for clinical outcomes under similar experienced-use conditions. Future work linking these outcomes to direct cost analyses and longer-term productivity measures will be essential to fully define the value proposition of navigated robotics within contemporary spine surgery.
Footnotes
Acknowledgements
The National Spine Health Foundation extends its sincere appreciation to the numerous interns who contributed to the PRoGRSS project over the course of its development. Individuals from diverse stages of training—including high school, undergraduate, and postgraduate programs—provided valuable assistance to various aspects of this work. Their collective efforts, professionalism, and commitment meaningfully supported the advancement of this project, and we gratefully acknowledge their contributions.
Ethical Considerations
This study was conducted in accordance with the 1964 Declaration of Helsinki, its amendments, and other equivalent ethical standards. The study was approved by Advarra (central IRB; Pro00045812, August 27, 2020) and by the local IRBs of all participating sites. Informed consent was obtained from all participants in written or electronic form.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: PRoGRSS is supported by a research grant funded by Medtronic USA to the National Spine Health Foundation (#12497). The funder was not involved in the study design, collection, analysis, interpretation of the data or decision to publish.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: LDO and RTR: Research grants from Medtronic, Amgen, UCB, Innovasis, Medimaps, Alphatec, Acuity Surgical, Spinal Stabilization Technologies. NJL: Consulting fees from Medtronic. JLG: Grants from Edwards LifeSciences; Royalties from Acuity, Medtronic, Globus; Consulting fees from Acuity, Depuy, Medtronic, Globus, Stryker, FYR Medical, and Expanding Innovation; Payment or honoraria from Broadwater, NASS, Pacira Pharmaceutical, Baxter, MiMedx, Kyana; Support for attending meetings/travel from Fischer Owens Funds; Patents planned, issued, or pending from Medtronic; Stock in Cingulate Therapeutics, FYR Medical; Other Financial Interests from the Alan L. Jacqueline B. Stuart Spine Research Center, Biom’Up; Cerapedics, Inc, Empirical Spine, Inc, Medtronic, National Spine Health Foundation, Scoliosis Research Society, Stryker, The International Spine Study Group Foundation, Department of Defense. RAL: Grants from the Department of Defense; Royalties and consulting fees from Medtronic. CMH: Consulting fees from Medtronic, Globus Medical, Spineart, and Innovasis. GTP: Consulting fees from Medtronic. EJ: Consulting fees from Stryker, Medtronic, and Innovasis. CRG: Consulting fees from Medtronic and Stryker; Royalties from Medtronic and Stryker; Advisory board for Medtronic and Stryker; Sock in Augmedics and N-Site; Board of Directors, National Spine Health Foundation.
Data Availability Statement
Registry data are not publicly available due to IRB and data-use restrictions. De-identified data may be requested from the corresponding author with appropriate approvals.