
Abstract
Study Design:
Broad narrative review.
Objective:
To review and summarize the current literature on guidelines, outcomes, techniques and indications surrounding multiple modalities of minimizing blood loss in spine surgery.
Methods:
A thorough review of peer-reviewed literature was performed on the guidelines, outcomes, techniques, and indications for multiple modalities of minimizing blood loss in spine surgery.
Results:
There is a large body of literature that provides a consensus on guidelines regarding the appropriate timing of discontinuation of anticoagulation, aspirin, nonsteroidal anti-inflammatory drugs (NSAIDs), and herbal supplements prior to surgery. Additionally, there is a more heterogenous discussion the utility of preoperative autologous blood donation facilitated by erythropoietin and iron supplementation for healthy patients slated for procedures with high anticipated blood loss and for whom allogeneic transfusion is likely. Intraoperative maneuvers available to minimize blood loss include positioning and maintaining normothermia. Tranexamic acid (TXA), bipolar sealer electrocautery, and topical hemostatic agents, and hypotensive anesthesia (mean arterial pressure (MAP) <65 mm Hg) should be strongly considered in cases with larger exposures and higher anticipated blood loss. There is strong level 1 evidence for the use of TXA in spine surgery as it reduces the overall blood loss and transfusion requirements.
Conclusion:
As the volume and complexity of spinal procedures rise, intraoperative blood loss management has become a pivotal topic of research within the field. There are many tools for minimizing blood loss in patients undergoing spine surgery. The current literature supports combining techniques to use a cost- effective multimodal approach to minimize blood loss in the perioperative period.
Introduction
Over the past few decades, the number of spinal procedures performed in the United States has increased dramatically, with growth exceeding 200% since the 1990s. 1 -4 As the volume and complexity of spinal procedures rise, intraoperative blood loss management has become a pivotal topic of research within the field. 5 -7 Many spinal procedures are associated with substantial blood loss. Notable are revision surgeries to treat deformity, which also have the highest incidence of postoperative transfusion, ranging from 8% to 30%. 8 -10 Certain patient characteristics, namely advanced age, higher body mass index (BMI), greater surgical complexity, and longer fusion constructs are all associated with more extensive blood loss. 6
Transfusions—the traditional answer to clinically relevant blood loss—are themselves associated with a myriad of complications, including the transmission of bloodborne infection, immunologic cross-reactions, thromboembolic events, and immunosuppression. 11 -13 These complications can lead to longer hospital stays, increased direct costs, and higher inpatient mortality. 5,14,15 To this end, postoperative transfusion has been demonstrated by several recent, large retrospective reviews in spine and nonspine population to increase perioperative mortality, complication rate, and overall care costs. 11,16 -20 Among the most concerning complications include significant fluid shifts capable of damaging the heart, lung, and kidneys, such as circulatory overload, transfusion-related acute lung injury, and acute kidney injury.
Owing to this significant side-effect profile, it is incumbent upon the practicing spine surgeon to possess in their armamentarium those interventions capable of reducing intraoperative blood loss and transfusion needs. Here, we provide a narrative review of the recent evidence, highlighting both the preoperative and intraoperative techniques demonstrated to best reduce perioperative blood loss in spine surgery.
Preoperative Prevention
More than 90% of aged Americans currently use one or more prescription medications, over-the-counter medications, or dietary supplements. 21 Many of these either directly or indirectly affect the intraoperative bleeding risk through inhibition of the coagulation pathways or platelet function. Therefore, a thorough, timely review of medications prior to elective spine surgery is recommended to decrease otherwise avoidable blood loss.
Nonsteroidal Anti-Inflammatory Drugs
The most common medications of concern are the nonsteroidal anti-inflammatory drugs (NSAIDs), including aspirin (acetyl salicylic acid [ASA]), ibuprofen, naproxen, and celecoxib. These medications inhibit the cyclo-oxygenase (COX) enzymes, decreasing the production of thromboxane A2 (TXA2), a key upstream trigger of platelet activation and aggregation. Despite conventional wisdom recommending their perioperative discontinuation, there remain no actual guidelines as to the optimal timing for cessation. Most recommendations are based on the pharmaceutical half-lives of these drugs, yet there is a lack of high-quality evidence in the field of spine surgery to suggest the optimal timing of discontinuation. 22 Consequently, it is observed that most surgeons agree to an arbitrarily defined number of days prior to surgery. 23 In a recent survey of the Canadian Spine Society, the majority agreed that discontinuation of antiplatelet agents 7 days prior to surgery was one of the most important measures for limiting intraoperative blood loss, with nearly all members endorsing routine use of this practice. 7
Here, it is worth emphasizing the influence of aspirin on intraoperative bleeding. With the increased prevalence of coronary vascular disease and the documented ability of regular aspirin usage to lower the risk for coronary events, aspirin holds a unique place within the NSAID family. While it is generally held that aspirin should be discontinued on the same time frame as other antiplatelet agents, the preponderance of evidence has failed to demonstrate an appreciable effect on either blood loss or overall complication rate among patients undergoing spinal surgery. 24 -26 Therefore, we provide only a weak recommendation for its discontinuation in patients with no reasonable indication for continued use. This may help decrease postoperative bleeding from the wound site. 27
Antiplatelet Agents
Many NSAIDs, aspirin in particular, also function as antiplatelet agents owing to their ability to impair thromboxane A2 production, of chief concern here are P2Y12 antagonists (eg, clopidogrel, prasugrel, ticagrelor, and ticlopidine). These agents have elimination half-lives of 6 to 15 hours 28 and their discontinuation is recommended by the vast majority of spine surgeons. 23 However, prior evidence has failed to correlate a significant intraoperative bleeding risk with preoperative antiplatelet agent review. One meta-analysis of 46 studies found that continuing either aspirin or a P2Y12 antagonist (clopidogrel) during the perioperative period was not associated with a significant increase in intraoperative blood loss or transfusion risk. 29 Level II evidence from a nonblinded clinical trial also failed to demonstrate a difference in blood loss, transfusion rate, or complication rate between patients taking clopidogrel and controls. 30 Because of this, as well as the presence of inconsistency among guidelines on the necessity of perioperative discontinuation of antiplatelet therapy, we believe it is safe to continue patients on antiplatelet therapy prior to spine surgery. However, for those desiring to minimize the risk of massive intraoperative blood loss, the recommended discontinuation time frames can be found in Table 1.
Drugs that May Increase Surgical Blood Loss.
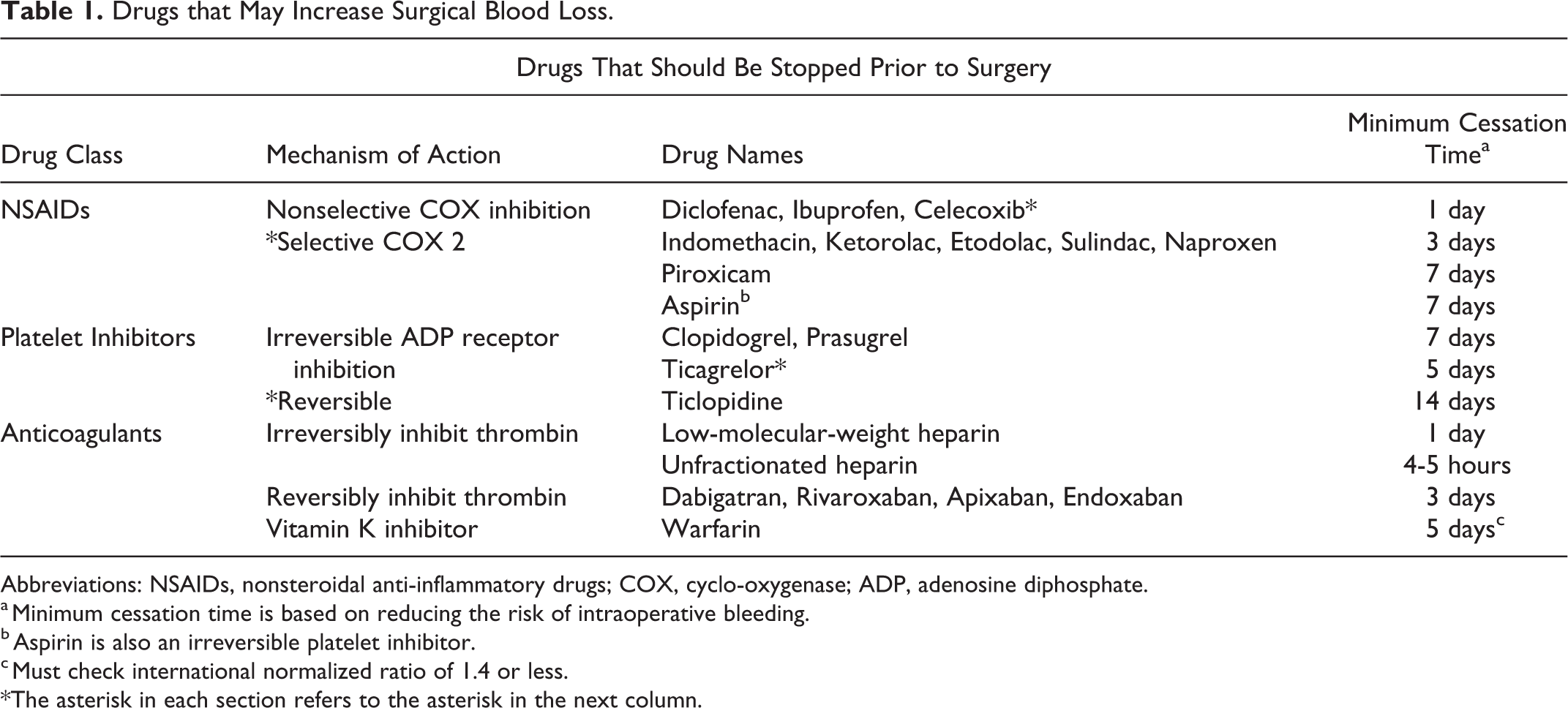
Abbreviations: NSAIDs, nonsteroidal anti-inflammatory drugs; COX, cyclo-oxygenase; ADP, adenosine diphosphate.
a Minimum cessation time is based on reducing the risk of intraoperative bleeding.
b Aspirin is also an irreversible platelet inhibitor.
c Must check international normalized ratio of 1.4 or less.
*The asterisk in each section refers to the asterisk in the next column.
Anticoagulants
Unlike NSAIDs, a clear consensus exists on the decision to discontinue therapeutic anticoagulants preoperatively. Warfarin should be stopped 5 days prior to surgery with a target international normalized ratio (INR) of 1.4 or less; heparin bridging therapy can then be implemented to prevent venous thrombotic events (VTEs) in high-risk patients. Newer anticoagulants—direct thrombin inhibitors (eg, dabigatran, argatroban) and Xa inhibitors (eg, apixaban, rivaroxaban)—may be continued until 3 days prior to surgery due to their shorter half-lives. Heparin bridging is not as well described after the halting of these medications, but it may be indicated for patients at high risk of thromboembolic events. Work-up with the CHADS2, CHADS2-VASc (clinical prediction rules for estimating the risk of stroke in patients with nonrheumatic atrial fibrillation), or HAS-BLED scoring system (developed to assess 1-year risk of major bleeding in patients taking anticoagulants with atrial fibrillation), 31 and consultation with hematology may be considered for these patients (Table 2). Table 1 provides current guidelines where available on when to stop specific medications in order to minimize intraoperative blood loss caused by these medications.
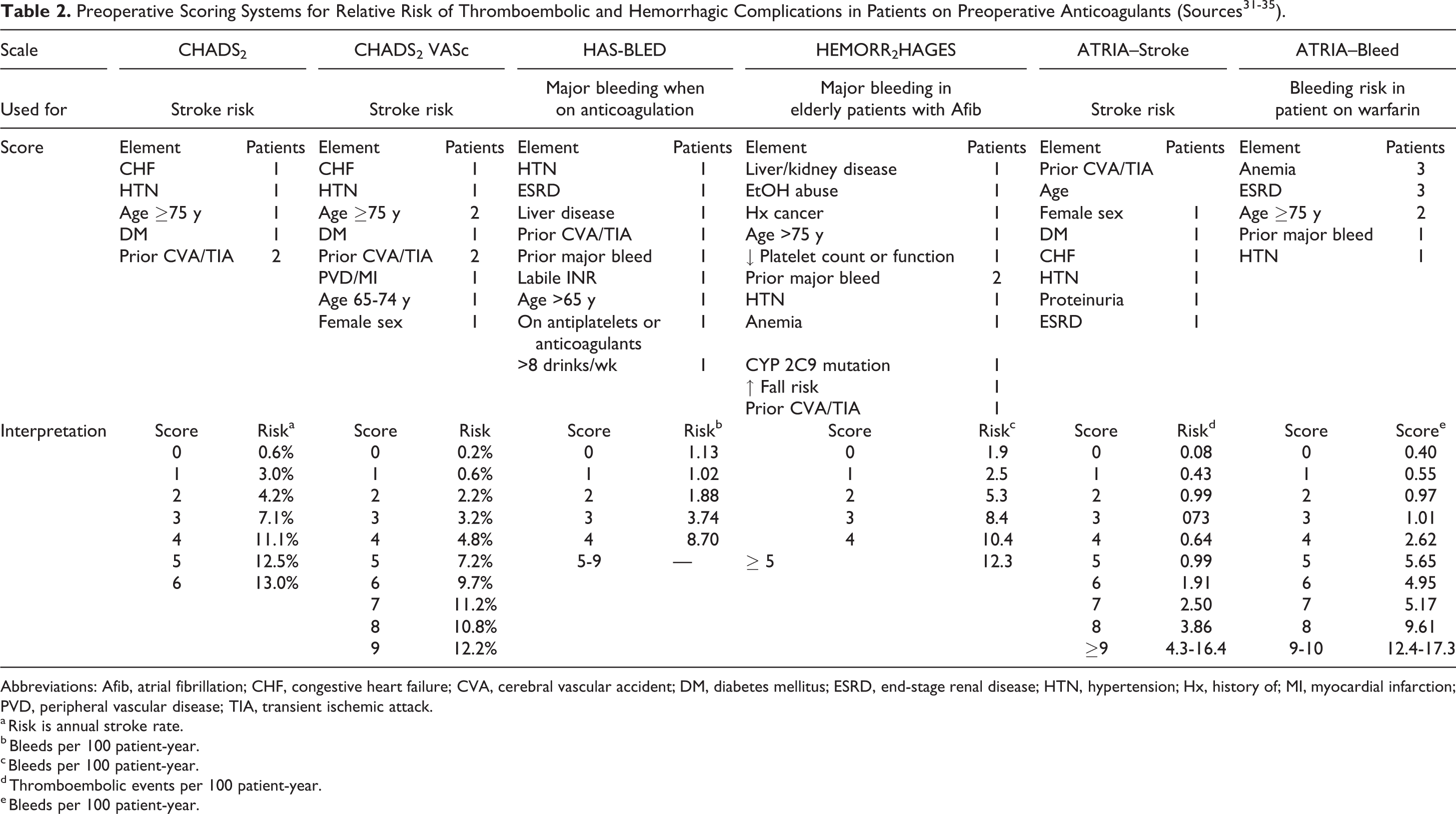
Abbreviations: Afib, atrial fibrillation; CHF, congestive heart failure; CVA, cerebral vascular accident; DM, diabetes mellitus; ESRD, end-stage renal disease; HTN, hypertension; Hx, history of; MI, myocardial infarction; PVD, peripheral vascular disease; TIA, transient ischemic attack.
a Risk is annual stroke rate.
b Bleeds per 100 patient-year.
c Bleeds per 100 patient-year.
d Thromboembolic events per 100 patient-year.
e Bleeds per 100 patient-year.
It should be noted that numerous other prescription and non-prescription medications (eg, multivitamins) can significantly alter successful coagulation cascade function. Typically, any anti-inflammatory medication or nutritional supplement can induce more bleeding. Particularly important are herbal and dietary supplements, which are used by more than 60% of Americans 36 and commonly missed during medication reviews. 21 Many herbal and dietary supplements have been associated with increased surgical and postoperative bleeding, including St John’s wort, garlic, ginseng, saw palmetto, and fish oil. 37 -39 We suggest also discontinuing these supplements prior to planned spine surgery.
Preoperative Autologous Blood Transfusion and Erythropoietin
Another method proposed to reduce transfusion risks for elective cases with high anticipated blood loss is preoperative autologous blood donation (PABD). Though valuable in theory, the evidence supporting this method has been mixed with some studies reporting decreases in allogeneic transfusion rate by up to 50%, 40,41 while others found an increased rate of transfusion and no difference in outcomes. 42 The latter likely reflects the use of PABD in patients with inadequate compensatory erythropoiesis between phlebotomy and surgery. To avoid this, we recommend 2 steps. In patients considering PABD, a hemoglobin (Hb) level should be obtained 3 to 4 weeks prior to surgery; those found to be anemic (Hb < 11 g/dL) should be dissuaded from PABD or optimized using erythropoietin and iron supplementation. Similarly, for those pursuing PABD that subsequently demonstrate signs of PABD-induced anemia, erythropoietin (40 000 units SQ q7d beginning 4 weeks before surgery) and iron supplements (FeSO4—325 mg orally thrice a day for 4 weeks before surgery) can be administered preoperatively. 43 Erythropoietin (EPO) significantly improves preoperative Hb levels, decreases allogeneic transfusion requirements, and decreases hospital length of stay. 44 However, PABD with preoperative EPO treatment is insufficient to eliminate the risk of perioperative transfusion and up to 40% of patients may still require transfusion of one or more units of allogeneic blood products. 45 One should note that EPO use is considered off-label for patients willing to preoperatively donate autologous blood; Food and Drug Administration (FDA) approval is only for those with perioperative hemoglobin levels between 10 and 13 g/dL who are unwilling to donate blood preoperatively. 46 Consequently, PABD with concomitant EPO administration may be one strategy for reducing transfusion requirements. However, the overall recommendation for its use is based largely on retrospective series from the pediatric deformity literature and may not be applicable to adult patients. This is especially true for older patients with a lower baseline hematocrit in whom PABD may simply shorten the time to first transfusion. Additionally, evidence suggests that red cell viability and function decrease semilinearly with storage time, 47 so it may be that the extent of red cell degeneration seen during the preoperative period required for anemia resolution nullifies any potential benefit. For these reasons, as well as the risk of transfusion reaction secondary to clerical error, the use of PABD has fallen out of favor over the past 2 decades.
Intraoperative Blood Loss Management
Positioning
Appropriate surgical positioning is an underappreciated means of decreasing intraoperative blood loss. Two considerations include (1) the relative positions of the surgical site and right atrium and (2) the intra-abdominal pressure (IAP). For operations on the lumbar and lower thoracic spine, placing the patient into a Trendelenburg position can reduce pressure in the inferior vena cava and consequently decrease bleeding from the epidural and vertebral venous plexuses; reverse Trendelenburg offers similar benefits in cervical procedures.
Appropriate table selection can also help facilitate hemostasis for requiring prone positioning. Conventional surgical tables elevate IAP, in turn causing congestion of the epidural venous plexus—a common source of bleeding. 48 To avoid this, a Jackson table or a Wilson frame with wide interpad spacing can be employed, as both allow free suspension of the abdomen, decreasing IAP and draining blood away from the operative site. Alternatively, for those centers without this option, adoption of the jackknife position can reduce IAP and blood loss relative to standard prone positioning for single level lumbar surgery. 49,50
Normothermia
Maintaining core temperature at physiological levels has also been proposed to reduce blood loss by preventing hypothermia-induced coagulopathy. The intervention has been only poorly explored in spine, and several groups have failed to document an impact of core temperature on blood loss. 51,52 Paradoxically, a meta-analysis of studies from other surgical fields reported even mild hypothermia to reduce total blood loss and decrease transfusion rates. 53 Consequently, the ability of hypothermia to reduce blood loss is questionable. Perioperative hypothermia is associated with increased complication rates and mortality though, 54 recommending its use for all patients despite its questionable link to superior hemostatic outcomes. Strategies to prevent hypothermia include forced air warming, 55 warm socks, 56 warmed intravenous fluids, and warmed irrigation fluids. 57
Hypotensive Anesthesia
Control of the mean arterial pressure (MAP) is a constant dialogue between surgeon and anesthesiologist. An experienced anesthesiologist is often able to strike a balance between the perfusion demands of vital organs and the surgeon’s request for a low MAP due to its ability to minimize intraoperative blood loss.
Verma et al 58 reported that maintaining a MAP of 65 mm Hg or less reduced blood loss in deformity cases by 33%. However, such low MAPs can place the spinal cord at risk of infarction, especially in cases whereby the spinal cord is previously injured or already under compression (eg, cervical spondylotic myelopathy). To prevent this rare, but catastrophic event, intraoperative neuromonitoring should be used as it allows for early detection of spinal cord hypoperfusion and can consequently prevent permanent neurological deficits in the overwhelming majority of cases. 59 -61 Hypotensive anesthesia (MAP ≤70 mm Hg) may be best reserved for the approach and instrumentation, where bleeding risk is highest. However, we recommend maintaining the MAP above 80 mm Hg while manipulating the neural elements to decrease the likelihood of ischemic tissue injury. This recommendation is strongest for patients with increased risk of ischemic complications at baseline, such as those with peripheral vascular disease, a history of ischemic events (e.g., stroke), chronic renal failure, or uncontrolled diabetes mellitus. 62 Overall, we caution against the use of hypotensive anesthesia when there is risk of neurologic injury from poor perfusion.
Surgical Approach
The conventional, midline approach is the most common approach employed for posterior spine surgeries. During dissection, care is taken to remain in the avascular plane formed by the fascial sheaths of the 2 paraspinal muscular bundles. This is then continued laterally in a subperiosteal dissection to the facets, past which dissection begets more bleeding. Use of a Wiltse or paraspinal, muscle-splitting approach has been suggested to decrease blood loss relative to the midline approach. 63 However, the evidence to support this is relegated to a single retrospective study. Consequently, we make no recommendations regarding surgical approach for the reduction of operative blood loss.
Electrocautery
Since its introduction by Harvey Cushing in the early 1900s, electrocautery has helped reduce blood loss in neurosurgical procedures. Conventional techniques have made use of both monopolar and bipolar cautery for the dissection of soft tissues and coagulation of bleeding vessels, respectively. In 2008, premarket approval was granted for a bipolar sealer device, which employs radiofrequency energy with concomitant saline irrigation. 64 The use of saline helps significantly reduce surgical site temperatures relative to conventional electrocautery methods, and consequently may reduce trauma to the dissected tissues.
Multiple studies evaluating this device have demonstrated reductions in blood loss, operation duration, and transfusion requirements. 65 -68 At the same time, these same studies documented no difference in major complications, hospital length of stay, or infection rate between patients operated using the bipolar sealer and conventional electrocautery tools. 65,66,69,70 Furthermore, a recent meta-analysis by Lan and colleagues 69 suggested that the use of a bipolar sealer can reduce operative times, intraoperative blood loss, and transfusion rates. Last, a randomized controlled trial published by Wang et al 71 on a series of patients undergoing surgery for degenerative scoliosis of the lumbar spine also found the use of a bipolar sealer to reduce operation time, intraoperative blood loss, transfusion rates, and mean transfusion requirements. Therefore, the use of a bipolar sealer in larger exposure spine surgery may be recommended, with the given that meticulous surgical techniques are employed to control bleeding throughout surgery.
Antifibrinolytics
One of the greatest advancements in minimizing blood loss during spine surgery has been the introduction of antifibrinolytic agents, which in select studies have been demonstrated to reduce blood loss by up to 50%. 72 With the withdrawal of aprotinin from the US market in 2008, the 2 main antifibrinolytics in clinical practice are tranexamic acid (TXA) and ∊-aminocaproic acid (EACA). Both compounds are lysine analogues that bind to and prevent activation of plasminogen, thereby inhibiting fibrinolysis and promoting clot stabilization. Despite concern that such a procoagulation mechanism of action may increase the risk of postoperative VTEs, this concern has failed to be borne out in the literature. 73,74 The few FDA-defined contraindications to the use of these agents include active bleeding (.g, epidural hematoma, subarachnoid hemorrhage), acquired defective color vision (TXA only), active intravascular clotting, and known hypersensitivity to the anti-fibrinolytic acid being used.
∊-Aminocaproic Acid
EACA has been found to be a safe and effective antifibrinolytic agent in spine surgery by multiple prospective randomized controlled trials (RCTs). 75 -78 Studies examining its use have typically employed a loading dose of 100 mg/kg with a maintenance dose of 10 mg/kg/h. EACA has been used with both anterior and posterior surgical approaches for multiple indications, including pediatric deformity and adult degenerative pathologies. In the most recent study examining EACA use in patients operated for adolescent idiopathic scoliosis, EACA did not lower intraoperative blood loss (EBL), but it was associated with significantly decreased total blood loss during the hospital stay with the treatment group averaging 2400 ml/case compared to 4100 mL/case in controls (P < .0007). 76 It is speculated that this benefit is derived from the continuous effect of the EACA infusion, as both intraoperative blood loss and postoperative drainage were only marginally lower, but the cumulative effect was statistically significant. Other RCTs all demonstrated significantly lower estimated blood loss with use of EACA without any significant difference in complications between groups.
Tranexamic Acid
TXA has many applications in minimizing blood loss outside surgery, including leukemia, ocular hemorrhage, trauma with active hemorrhage, severe hemoptysis, and menorrhagia. TXA was first introduced surgically in the setting of high-risk cardiac surgery where it successfully reduced blood transfusion requirements and cost. It was soon widely adopted in the field of orthopedic arthroplasty, where it demonstrated similar benefits. TXA is 7 to 10 times more potent than EACA, 79 allowing for commensurately lower doses. On review of the current literature, the most commonly used regimen employs a loading dose of 10 mg/kg and maintenance dosing of 1 to 2 mg/kg/h. As with EACA, class I evidence exists supporting the ability of TXA to reduce intraoperative blood loss. A recent meta-analysis of pooled data of 6 randomized placebo-controlled trials demonstrated a mean decrease in intraoperative blood loss of 229 mL (P < .00001). 74 As with EACA, TXA may continue to provide hemostatic benefits postoperatively. A prospective randomized, controlled trial of patients undergoing cervical laminoplasty failed to demonstrate a significant decrease in intraoperative blood loss with TXA administration. However, the authors did find total blood loss to be significantly lower (P < .01). 80 As with the aforementioned studies assessing its use in thoracolumbar fusion, the authors observed no significant difference in the VTE rates. 73,76,80 -85 In the past year, Lin et al 86 published on the use of a high-dose TXA (50 mg/kg loading dose with a 5 mg/kg/h maintenance infusion), which they found to have complication rates comparable to historical cohorts using a conventional, low-dose regimen. Subsequent to this, a prospective, randomized controlled trial (NCT02053363) has been initiated comparing the two regimens, with results expected in mid-2019. 87
Both TXA and EACA are powerful agents in minimizing blood loss compared with placebo controls. Meta-analysis pooling results from 12 prospective randomized trials using either TXA or EACA for adults undergoing spinal fusion 74 found antifibrinolytic use to reduce intraoperative blood loss by a mean of 127 mL (P < .002) and postoperative blood loss by a mean of 95 mL (P < .009). The use of either antifibrinolytic also significantly lowered both the rate of allogeneic red blood cell (RBC) transfusion (odds ratio = 0.58, P < .04) and the mean units transfused. Ultimately, the use of these agents is supported by a high level of evidence (Table 3) and should be strongly considered in patients undergoing surgery with high anticipated blood loss. We express no strong preference between the two antifibrinolytics, although TXA has been demonstrated to provide superior hemostatic benefits in at least one recent study. 88 From a cost-effectiveness aspect, TXA may be preferable as it is readily available in generic form and has been found to be a cost-effective method of minimizing blood loss. 84
Antifibrinolytics Literature Review.
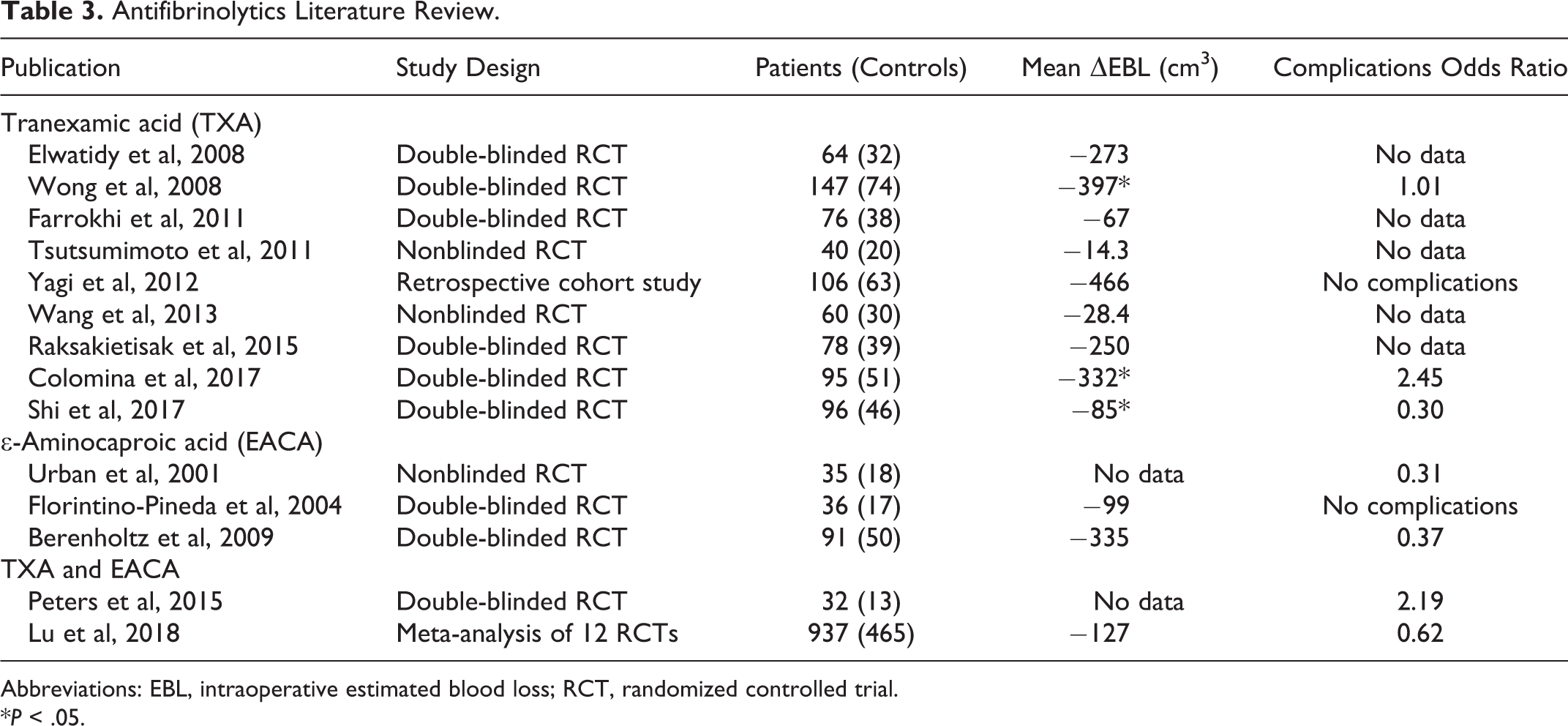
Abbreviations: EBL, intraoperative estimated blood loss; RCT, randomized controlled trial.
*P < .05.
Of note, topical and oral formulations of tranexamic acid are now available. Prior meta-analyses in the joint arthroplasty literature have demonstrated topical, oral, and intravenous formulations to have similar effects on intraoperative blood loss as well as similar complication rates. 89,90 Similar evidence is not yet available in the field of spine surgery though. 91 Additionally, the use of topical TXA in addition to intravenous TXA may further decrease blood loss, hemoglobin decrease, and transfusion requirement. 92 Insufficient evidence exists to compare complication profiles in patients with high preoperative risks of thromboembolic events; however, we speculate that the topical formulation may be more advantageous for this population owing to its more local effects.
Topical Hemostatic Agents
Although the use of topical hemostatic is ubiquitous, the evidence establishing their ability to minimize blood loss or need for allogeneic blood transfusion is sparse with only mild evidence supporting their efficacy at reducing blood loss. This may be due to the tendency to employ them in larger procedures with higher anticipated blood loss. These agents mechanistically reduce blood loss through a combination of mechanical occlusion of bleeding vessels (bone wax, gelatin sponge), platelet coagulation (microfibrillar collagen), and/or activation of the common clotting pathway (flowable matrix). Of note, expandable cellulose hemostatic agents should be used with caution in the absence of posterior spinal elements as they may cause neural compression. 93 All have been deemed relatively safe, and in the authors’ experience, they are all effective at safely reducing blood loss. 94 A summary of the most commonly employed agents and their efficacy is presented in Table 4.
Topical Hemostatic Summary (Source 95 ).
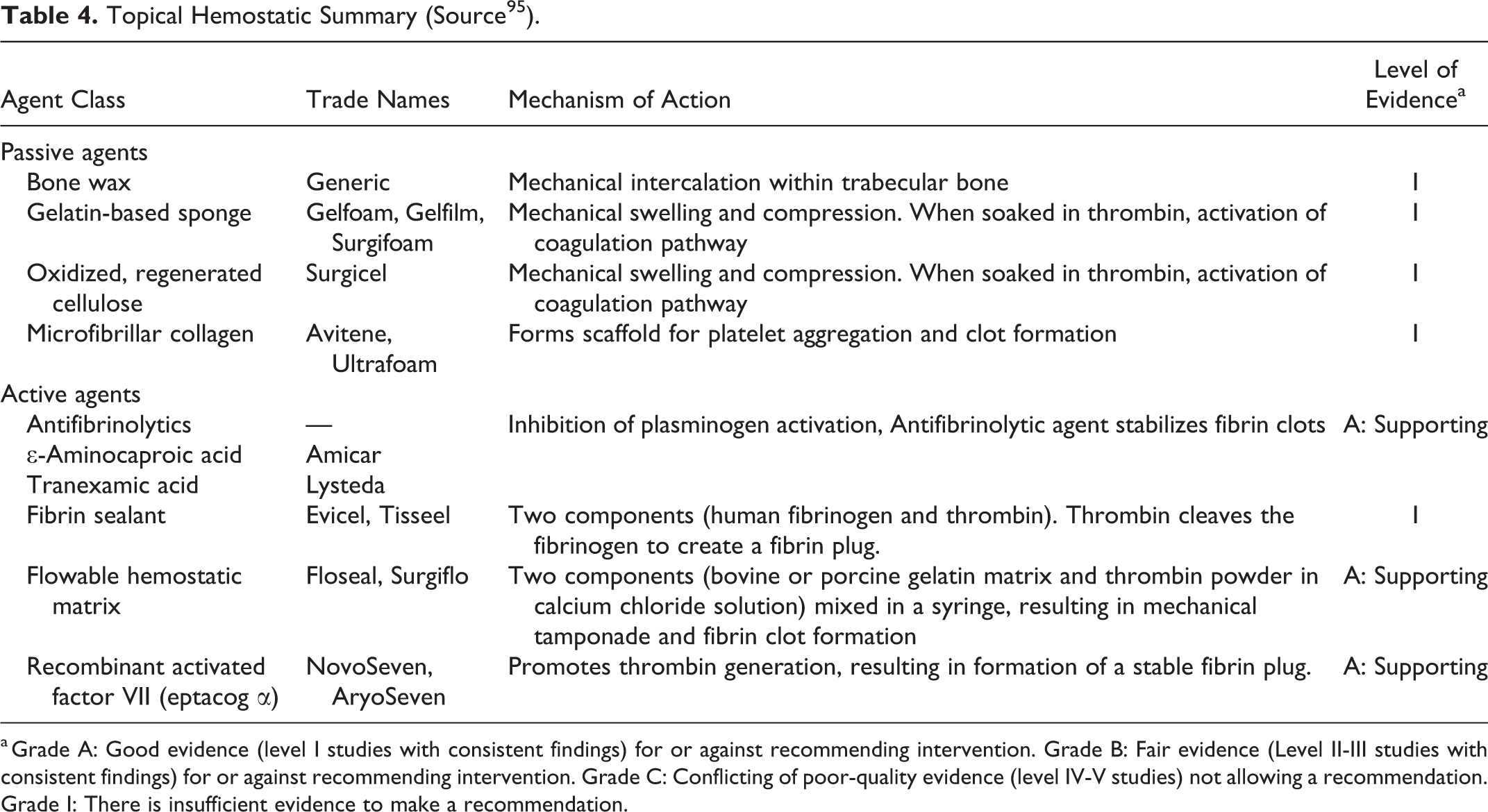
a Grade A: Good evidence (level I studies with consistent findings) for or against recommending intervention. Grade B: Fair evidence (Level II-III studies with consistent findings) for or against recommending intervention. Grade C: Conflicting of poor-quality evidence (level IV-V studies) not allowing a recommendation. Grade I: There is insufficient evidence to make a recommendation.
Intraoperative Cell Salvage
A final intervention capable of minimizing the effect of blood loss during spine surgery is the use of intraoperative cell salvage (ICS). ICS works by draining fluid and blood from the dissection cavity and filtering out clotting factors, platelets, and other debris to form an RBC-enriched unit that can then be returned to the patient. The use of this technology has been most thoroughly reported in the field of pediatric deformity, where ICS has been demonstrated to reduce the need for allogeneic blood transfusion. 96,97 One recent study on the use of ICS in scoliosis surgery showed a significant decrease in the rate of allogeneic blood transfusion—6% versus 55% in those not treated with ICS. 98
One caveat of ICS is that it requires a minimum blood loss in order to produce a transfusable unit; the size of the blood loss is dictated by the size of the transfusion bowl. Because of this minimum transfusion requirement, the cost-effectiveness of ICS depends on the expected transfusion volume. In patients with high expected blood loss, such as those undergoing surgery for adolescent idiopathic scoliosis, ICS has been found to be cost-neutral compared to allogeneic blood transfusion. 99 Most studies have found ICS to have a very low complication profile, though at least one study has reported acute kidney injury in the setting of ICS transfusion. 100
Viscoelastic Testing: Rotational Thromboelastometry and Thromboelastography
The ability to monitor the coagulation properties of a patient’s blood in real time can potentially make a substantial difference in the overall blood loss and risk of allogeneic transfusion. Failure to recognize increasing bleeding diathesis can lead to run-away hemorrhage. Conventional means of assessing a patient’s coagulation status focus on the use of periodic blood draws, which are then tested to determine the activated partial thromboplastin time (aPTT)—a measure of the intrinsic and common coagulation pathways—and the international normalized ratio (INR)—a means of testing the extrinsic and common pathways. Unfortunately, these tests are often slow to result and possibly inaccurate, especially in the operating room. 101 Viscoelastic methods are an alternative to these that is gaining attention in spine literature. 102 -104
Viscoelastic methods describe 2 classes of point-of-care tests that emulate sluggish venous blood flow in a small sample of patient blood obtained intraoperatively. 105 The size, stiffness, and time to clot are measured and interpreted to provide an estimate of the adequacy of the patients clotting ability. Two variations of this technology—rotational thromboelastometry (ROTEM) and thromboelastography (TEG)—exist. The technologies differ slightly in their set-up and required reagents but have been demonstrated to be similarly accurate in direct comparisons. 106 Two recent reviews found both technologies were associated with decreased rates of transfusion of red cells, plasma, and platelets compared with other means of assessing a patient’s transfusion needs intraoperatively. 107,108 Additionally, Guan et al 102 and Naik et al 104 have published their experiences using ROTEM for patients undergoing elective spine surgery. Naik and colleagues 104 reported that the use of ROTEM significantly decreased intraoperative plasma transfusion requirements and was associated with a cost savings of nearly $2000 per patient. By comparison, Guan et al 102 observed a significant decrease in total intraoperative red cell, plasma, and total blood product transfusion volumes. Additionally, the impact of ROTEM remained significant on multivariate analysis, independent of surgical invasiveness, preoperative INR and hematocrit, and TXA use. These results have been replicated in other surgical fields, including pediatric neurosurgery, 109 cardiac surgery, 110 and liver transplantation. 111
The biggest drawback of viscoelastic testing methods is that they require additional machinery and training of the anesthesia personnel. To our knowledge, the ability of the small interval costs savings to offset these hardware and personnel training costs has not been evaluated. As a result, we believe insufficient evidence exists to recommend the use of these interventions at small volume centers. However, we do recommend that surgeons at high volume centers with viscoelastometry-trained anesthesia staff, consider using ROTEM or TEG to help reduce transfusion requirements and total care costs.
Postoperative Drain Use
Postoperative, “hidden” blood loss may also substantially contribute to postoperative anemia and the need for transfusion, with prior studies suggesting that these losses may account for 40% to 47% of total blood loss. 112,113 The use of closed suction drains postoperatively is one intervention that has been suggested to decrease these hidden losses. The theoretical benefits of drains derive from the avoidance of neural element compression and excessive subfascial fluid pressure. Unfortunately, the same negative pressure changes that mediate these effects may also increase incisional drainage and surgical site hematoma formation. For this reason, the current state of spine literature does not allow for a general recommendation. 114,115 However, we generally place drains for patients undergoing open posterior procedures involving more than 2 levels owing to their ability to decrease rates of wound infection and return to the operating room for wound revision. 116
Conclusion
Major spine surgery can be associated with significant intraoperative blood loss. Factoring in the expected operation duration, surgical approach/exposure employed, and surgical complexity is extremely important in planning hemodynamics perioperatively; every effort should be made to minimize blood loss and to avoid transfusion (we weakly recommend a threshold of 7-8 g/dL unless symptomatic). Aside from patient counseling, preoperative optimization includes discontinuation of anticoagulation prior to surgery; the exact timeframe for discontinuation is dictated by the elimination half-life of the drug. Additionally, many surgeons advise discontinuation of aspirin and other NSAIDs at least 1 week prior to surgery, though the evidence substantiating this recommendation is mixed. Finally, in healthy patients slated for procedures with high anticipated blood loss and for whom allogeneic transfusion is likely, preoperative autologous blood donation may help to reduce the rates of transfusion. However, when this is pursued, it should be done early enough to allow resolution of the post-phlebotomy anemia, which could be facilitated by erythropoietin and iron supplementation.
Intraoperative maneuvers available to minimize blood loss include positioning to reduce intraabdominal pressure and maintenance of normothermia. The use of TXA, bipolar sealer electrocautery, and topical hemostatic agents (eg, oxidized regenerated cellulose, microfibrillar collagen, gelatin sponges, flowable agents) should be strongly considered in cases with larger exposures and higher anticipated blood loss. Hypotensive anesthesia (MAP <65 mm Hg) can also facilitate lower blood loss, though we caution against its routine use due to potential catastrophic ischemic neural injury. In our opinion, the MAP should be maintained above 80 mm Hg while manipulating neural elements to avoid neuromonitoring abnormalities. Finally, cell salvage should be considered in patients with high estimated blood loss, especially where allogeneic transfusion is not an option (eg, due to patient beliefs or rare patient blood type).
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Many of the authors have affiliations with organizations with financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in some of the products mentioned in the study. There are no conflicts of interest in reference to any product mentioned in the content of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This supplement was supported by funding from AO Spine North America.