
Abstract
Study Design:
Retrospective study of prospectively collected data.
Objective:
To evaluate learning curve of tubular microendoscopic discectomy (MED) in lumbar prolapsed intervertebral disc (PIVD) patients based on surgical and clinical parameters and delineate the challenges faced in early cases while practicing MED in large series of patients.
Methods:
This study was an institutional review board–approved retrospective study of the first 125 consecutive patients with single-level lumbar PIVD managed with tubular MED from 2008 to 2016 with a minimum 2-year follow-up. A total of 120 patients available at final follow-up were divided into quartiles (30 each) as per the date of surgery, with each consecutive group serving as a control for the previous group. Preoperatively and postoperatively clinical parameters (pain scores [Visual Analogue Scale; VAS], functional disability [Oswestry Disability Index; ODI] score, modified MacNab criteria), perioperative parameters (operative time, blood loss, hospital stay), technical issues (guide wire migration, tube docking–related problems, dural tear), and postoperative complications (postoperative leg pain, neural injury, infection, recurrence) were evaluated. Statistical analysis—logarithm curve-fit regression analysis and ANOVA test.
Results:
The sample consisted of 75 males and 45 females (mean age: 42.54 years) with no significant difference among the quartiles. There was significant difference (P < .005) noted in mean operative time (quartile 1, 87.33 minutes; quartile 2, 58.5 minutes) and mean blood loss (quartile 1, 76.33 mL; quartile 2, 32.66 mL) between quartile 1 and quartile 2, with no further significant reduction in quartile 3 and quartile 4. Significant difference (P < .005) in clinical parameters (VAS preoperative/postoperative 5.28/0.99; ODI preoperative/postoperative 32.18/12.08) were noted but was not associated with surgical experience. Overall, 90% (108 out of 120) of the patients had good to excellent results according to the modified MacNab criteria. The mean hospital stay did not show any significant difference among the quartiles. Guide wire migrated issues, neural injury, dural tear, and tube docking–related problems were significantly reduced after quartile 1. However, recurrence occurred at any phase. Infection occurred in one patient in quartile 1. Although blood loss and operative time showed a declining trend, it was not significant after quartile 2. So asymptote lay in quartile 1 and we recommend that novice surgeon should perform 25 to 30 cases to achieve mastery in this technique.
Conclusion:
For mastering the art of tubular MED for lumbar PIVD and to reduce its learning curve, novice surgeons can avoid the challenges and problems faced during initial cases with improvement in surgical skills by practicing on cadavers, wet labs, and bone-saw models following certain recommendations that we have after achieving asymptote. Familiarity with instrumentation, communication between surgical team, and defined expectations from radiology technicians are key to reduce the learning curve.
Introduction
Lumbar disc prolapse is the most common spinal problem affecting the young age group (30-50 years) at mainly lower lumbar levels. Lumbar disc herniation 1 causing radicular pain with or without neurological deficit, those refractory to conservative management for minimum 4 weeks, and having their activities of daily living affected are dealt surgically. Discectomy performed using open or minimal invasive techniques remains the gold standard treatment of choice, including hemilaminotomy, flavectomy, and discectomy. 2 -4 Advantages of minimal invasive surgery includes less perioperative pain, minimal blood loss, early ambulation, shorter length of hospital stay, and early return to work with smaller incision. 5 -7
However, introduction of microscope or endoscope through a tubular retractor system in terms of illumination and magnification with less muscular retraction, called microendoscopic discectomy (MED), has gained popularity. 8 -10
Various others intradiscal procedures such as laser discectomy and automated percutaneous discectomy 11 -13 cannot deal with extruded disc fragments and bony and ligamentous compression. However, MED can be done in patients with bony and ligamentous compression with removal of lateral, foraminal, extraforaminal disc, and extruded disc fragment as well as for fusion surgeries. The learning curve of MED is very steep; thus, understanding it properly would benefit new learners and clinical spine fellows to delineate the problems faced during initial cases to reduce complication rates. The authors aim to set guidelines for safe discectomy surgery performed with MED through educational and training workshops on saw-bone models, cadavers, and wet labs to improve surgical skills and to enhance health care standards.
The purpose of this study is to evaluate the learning curve of tubular MED in lumbar prolapsed intervertebral disc (PIVD) based on clinical and surgical parameters and to delineate the challenges encountered during initial cases in a large series of patients with some recommendations to avoid these problems.
Methods
After permission from the institution review board, data was retrieved of the first 125 consecutive patients with single-level lumbar PIVD operated by tubular MED between 2008 and 2016 by a 2-year fellowship trained surgeon at a single institute with a minimum 2-year follow-up period.
Methodology
Following strict inclusion and exclusion criteria, 120 patients formed the study cohort. These patients were arranged as per sequence of their dates of surgery and divided into 4 quartiles, with 30 patients in each quartile and each consecutive group serving as a control group for the previous group. We evaluated, preoperatively and postoperatively, clinical parameters (leg pain scores [Visual Analogue Scale; VAS], functional disability [Oswestry Disability Index; ODI] score, modified MacNab criteria), perioperative parameters (operative time, blood loss, hospital stay), technical issues (guide wire migration, tube docking–related problems, dural tear), and postoperative complications (postoperative leg pain, neural injury, infection, recurrence).
Inclusion Criteria
Symptomatic single-level lumbar PIVD with correlating magnetic resonance imaging [MRI] findings
Patients with minimum 2-year follow-up period.
Exclusion Criteria
Radiological signs of instability/deformity
Revision surgery
≥2 levels involved (multilevel PIVD)
Patients with degenerative scoliosis or spondylolisthesis
Patients requiring concomitant fusion or instrumentation
Acute spinal fracture, tumor, or infection
Operative Procedure
Under general anesthesia, the patient was positioned prone on a radiolucent table with bolsters below the chest and pelvis keeping the abdomen free, head on soft jelly pad with head end raised, and pressure points well padded. Using AP/lateral fluoroscopy imaging, an 18-G spinal needle was inserted at the diseased level 1 cm lateral to midline at the spino-laminar junction. Then, 10 cc normal saline was injected through needle into soft tissue and the needle withdrawn. Then, 2 cm incision kept at the needle site till the fascia just 1 cm lateral to midline. The blunt end of the guide wire was inserted under fluoroscopic guidance at spino-laminar junction targeted at the center of the disc involved. The initial dilator was inserted over the guide wire and the wire was removed. Then, sequential dilators were inserted separating the muscles while palpating the bony landmarks. The final tubular retractor, either 18 mm or 20 mm in diameter, was docked as a final working channel centering over the disc at the base of the spinous process at the spino-laminar junction. The operating microscope was then bought into field. Muscles covering the lamina were carefully resected and the bony structures were exposed. The midline was confirmed first by resecting the base of the spinous process with a high-speed burr of 4 mm. Laminotomy with flavectomy was done with discectomy. The epidural bleeding was controlled using a bipolar cautery or gelfoam with neurosurgical patty. The thoracolumbar fascia and subcutaneous tissue were closed by 2-0 vicryl suture. The skin was closed using 3-0 monocryl suture.
A single dose of intravenous antibiotic was given preoperatively and postoperatively as a standard protocol, and most of the patients were discharged within 24 to 48 hours postsurgery. The patients were followed-up at 12 to 14 days postsurgery for removal of stitches and allowed to resume daily activities except lifting heavy weights and bending forward for 3 weeks. Gradual back muscles strength exercises were started at 3 weeks.
The patients were followed-up at regular intervals of 2 weeks, 6 weeks, 3 months, 6 months, and yearly and evaluated for clinical outcomes by VAS for leg pain and ODI for back pain, and MacNab questionnaire and technical issues such as tube docking problems, guide wire migration issues, and postoperative complications. Parameters in different quartiles were compared using ANOVA test. Logarithm regression curve-fit analysis was used to find the asymptote. P value <.005 was considered significant.
Results
The mean age of patients was 42.54 years, with male-to-female ratio of 75:45. Out of 120 patients, L3-L4 = 17, L4-L5 = 63, and L5-S1 = 40 levels were operated. The cohort of each quartile was thus homogenous and comparable with regard to demographics.
The mean operative time was 65.83 minutes. The cases done in the first quartile (Q) took longer time; however, after gaining experience, the average time taken for surgery was less than the mean average (mean Q1 87.33 minutes, Q2 58.5 minutes, Q3 57.33 minutes, Q4 60.16 minutes), that is, significant difference (P < .005) between the first and second quartiles.
The average blood loss was 42.66 mL (mean Q1 76.33 mL, Q2 32.66 mL, Q3 30 mL, Q4 31.66 mL). The cases done in first quartile bled more with compared the second quartile (P < .005, ie significant difference), but after achieving mastery in the procedure, estimated blood loss does not further decline significantly after the second quartile.
Dural punctures occurred in 4 cases (3 in the first quartile and 1 in the second quartile) in our study. All cases were treated with watertight closure of the wound. No delayed cerebrospinal fluid leaks or pseudomeningoceles developed.
Guide wire migrated issues occurred in 5 patients in the first quartile. Tube docking–related problems occurred in 3 patients in the first quartile and in 1 patient in the second quartile. Facet joint violation was diagnosed intraoperatively in 3 patients (2 patients in the first quartile and in 1 patient in the second quartile).
Four patients developed postoperative leg pain. We found conjoint roots in 1 case in quartile 1 and in 1 case in quartile 2 causing leg pain. Two patients in quartile 1 with postoperative leg pain had guide wire migrated injury. All patients completely recovered within 4 months of surgery.
One patient showed postoperative neurological deficit in terms of foot drop in the first quartile due to guide wire migration, which was observed and treated conservatively and had complete recovery at final follow-up.
Two patients showed postoperative wound infections. One patient in the first quartile had deep wound infection. The patient needed debridement, antibiotics with serial dressings, and recovered completely without further complications. One patient had developed discitis in the second quartile treated with fusion surgery after 3 months.
Two patients (one in the first quartile and one in the third quartile) showed recurrence of symptoms after 3 months of surgery diagnosed with computed tomography myelogram. Both patients were considered for re-surgery. Two patients (one in the first quartile and one in the fourth quartile) had no relief in symptoms postoperative and diagnosed as residual disc herniation with MRI imaging at 3 weeks treated with MED. Thus, complications like recurrence and residual disc can occur at any phase even after gaining experience in the procedure.
In 1 patient in the first quartile, surgery was converted to open procedure due to difficulty in identification of anatomical and surgical landmarks intraoperatively.
The mean VAS scale for leg pain improved significantly from a preoperative value of 5.28 to 0.99 (P < .05) postoperatively. The mean ODI changed significantly from 32.18 to 12.08 (P < .05) but there is no significant difference between the quartiles as extent of decompression and technique followed was the same in all patients. Overall, 90% (108 out of 120) patients had good to excellent results according to the modified MacNab criteria.
Discussion
Discectomy was first reported by Mixter and Barr in 1934 for the management of lumbar disc herniation. 14,15 Previously different surgical approaches 11 -13 were available; however, in 1973, Kambin and Savitz 16 introduced the concept of endoscopic lumbar discectomy.
Microsurgical discectomy was introduced by Yasargil 17 and Casper 18 in 1977, which became the gold standard treatment.
In 1997, Foley and Smith 19 introduced an operated endoscope with tubular retractors termed as “endoscopic discectomy,” and in 2003, they introduced a microscope, also called “microendoscopic discectomy.”
The asymptote of any operation is determined by the operative time, intraoperative blood loss, operation effectiveness through clinical parameters, and intraoperative and postoperative complications.
In the case of MED in lumbar canal stenosis patients, Nowitzke 20 reported that the asymptote of operating time was reached at 30 cases. In another report about the learning curve for MED, the operation time and blood loss tended to become steady after the first 20 cases, and then declined gradually. 21
In our study, the learning curve of MED is steep with asymptote in the first quartile of around 25 to 30 cases, that is, similar to the studies of Ranjan and Lath, 22 Kulkarni et al, 23 and Nowitzke. 20 Mcloughlin and Fourney 24 and Wang et al 25 concluded that 15 cases are required to achieve expertise in endoscopic discectomy; however, Mcloughlin and Fourney evaluated operative time only and Wang et al 25 observed operative time and complications only.
Table 1 shows the comparison of mean operative time and mean blood loss of our study with other studies.
Comparison of Mean Operative Time and Mean Blood Loss of Our Study With Other Studies.
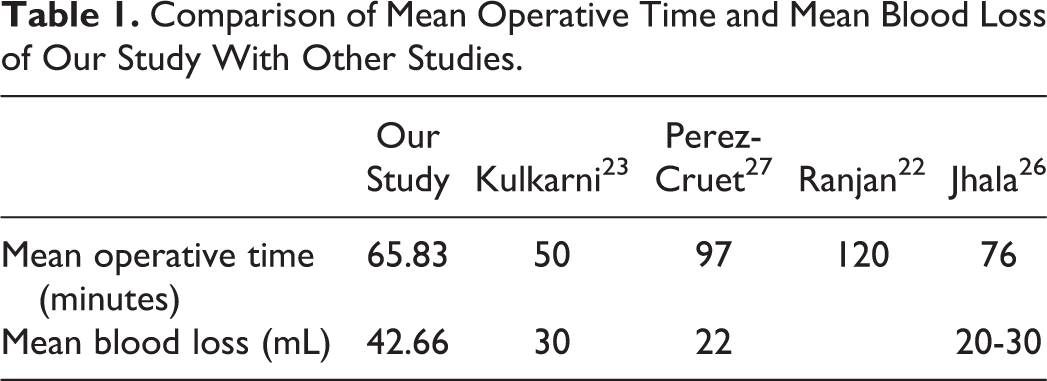
Figure 1 and 2 show scatter diagrams of mean blood loss and mean operative time in our study.
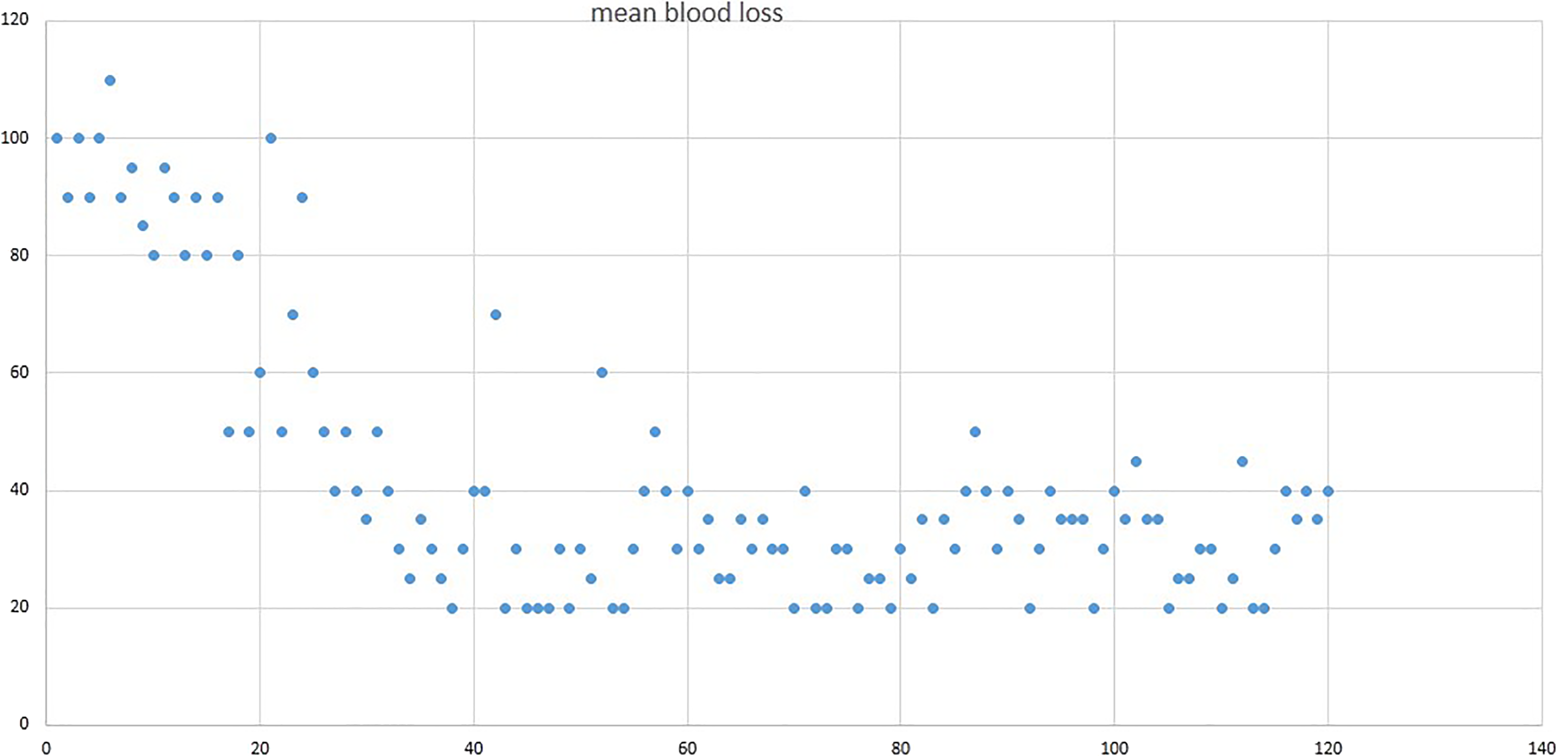
Scatter diagram of mean blood loss in our study.
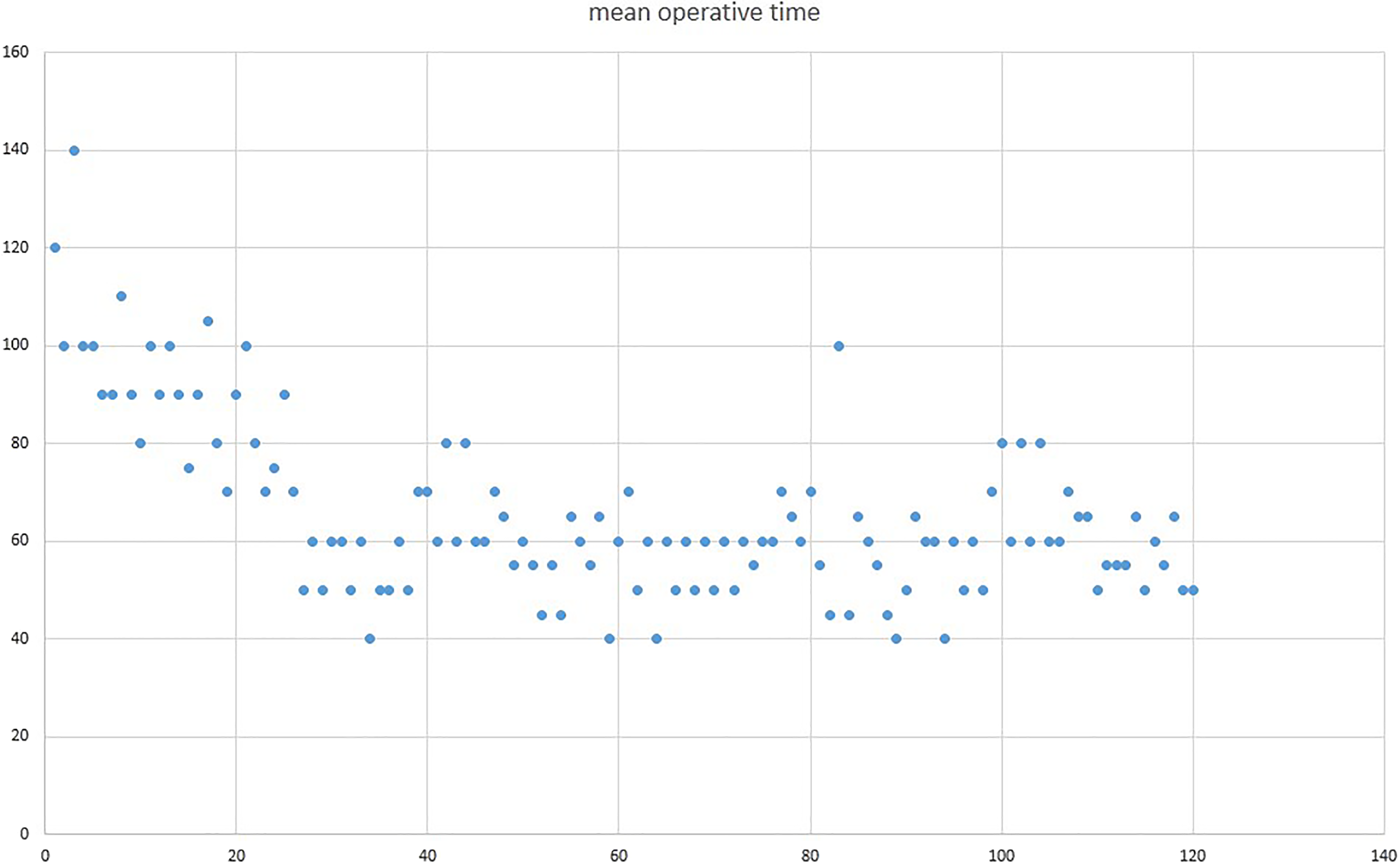
Scatter diagram of mean operative time in our study.
Figures 3 and 4 show values of mean blood loss and mean operative time in different quartiles of our study.
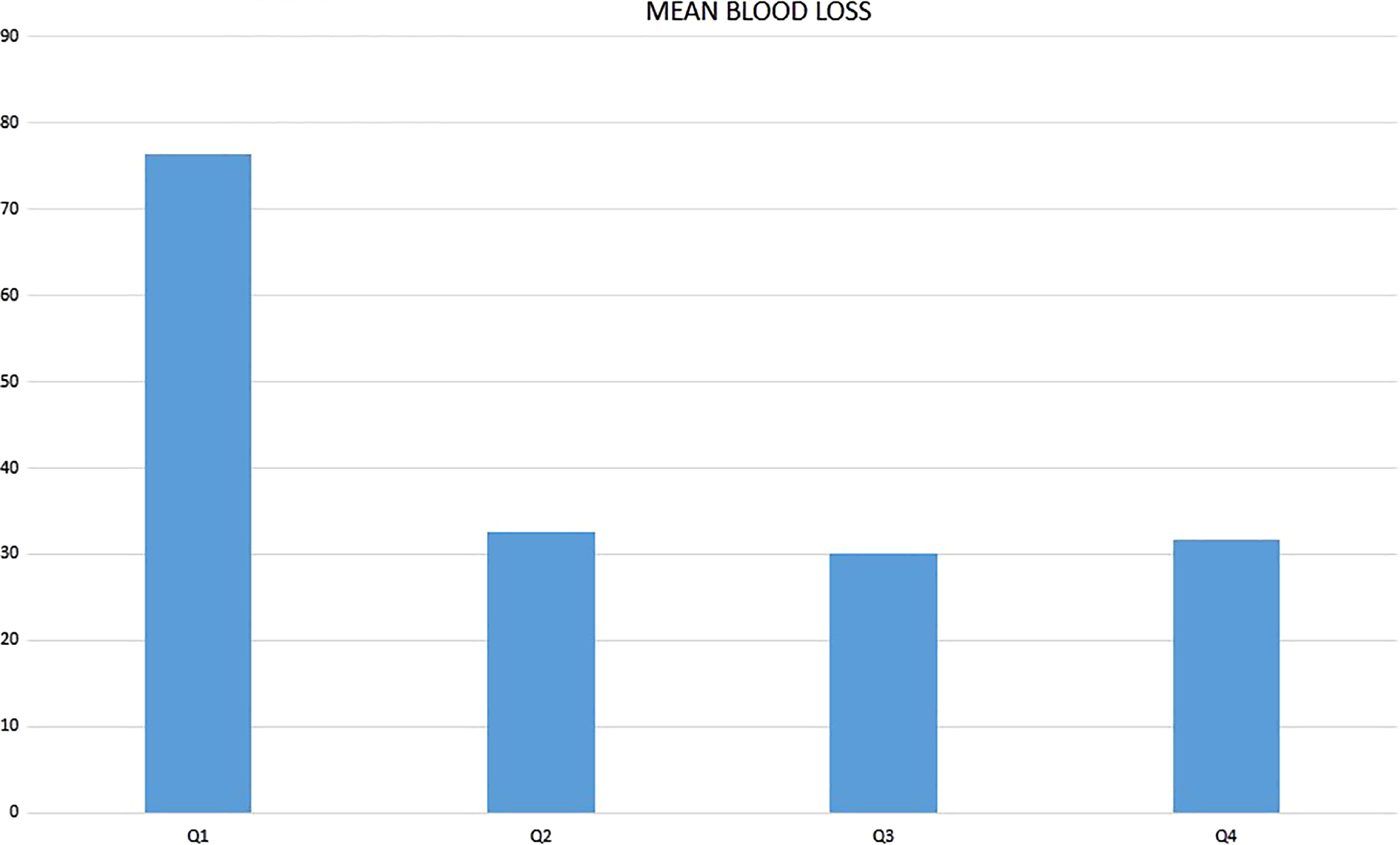
Values of mean blood loss in different quartiles of our study.
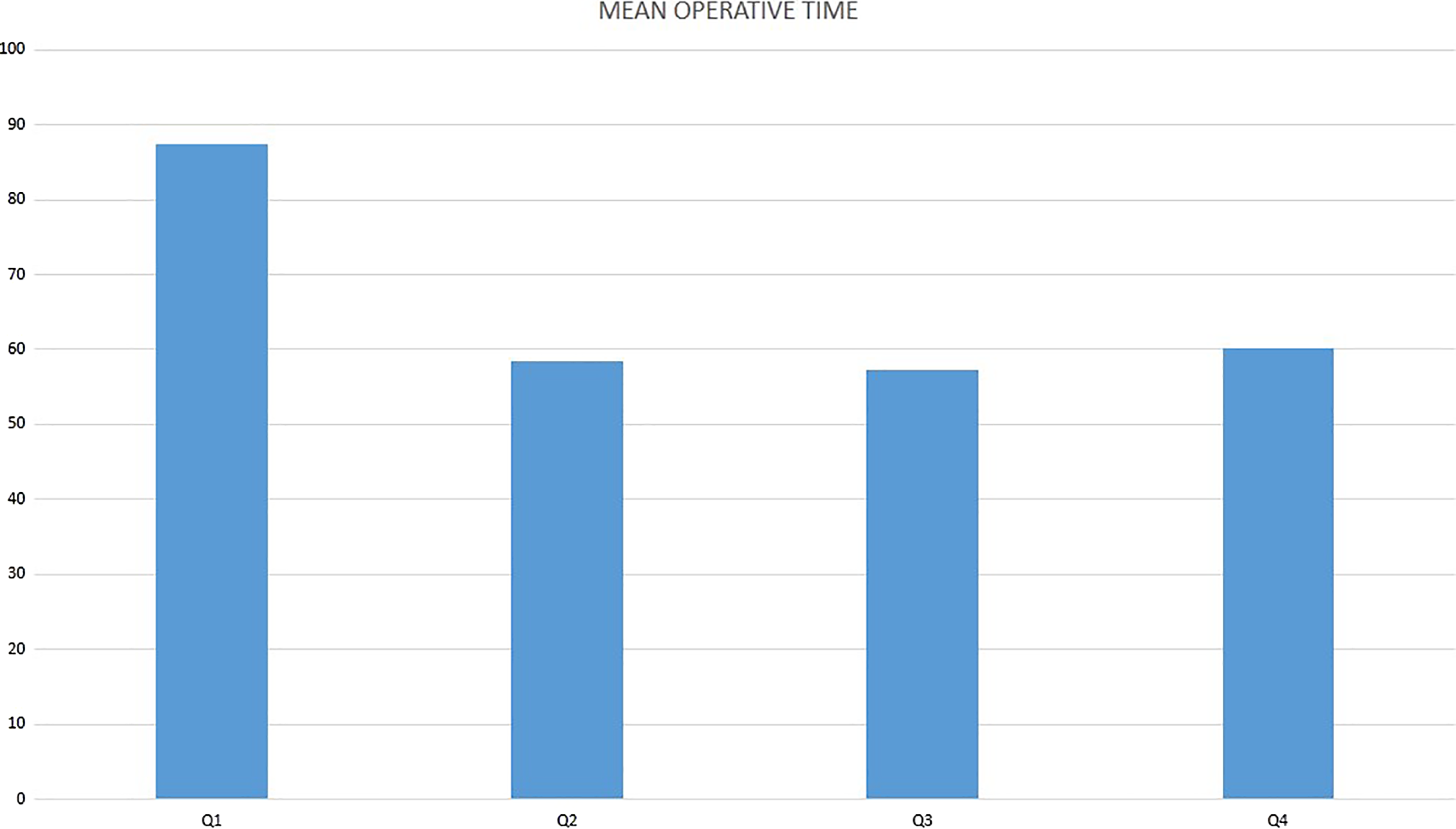
Values of mean operative time in different quartiles of our study.
Also, the steep decline in the operating time and blood loss during initial cases till the second quartile in our study may be attributable to the accurate placement of a tubular retractor at the desired level. The tubular dilator should be exactly at the center of the disc level involved at base of spinous process at the spino-laminar junction. We did not use guide wire in the second quartile after gaining enough experience, leading to reduction in all guide wire–migrated complications such as dural tear, neural injury, and postoperative leg pain, ultimately leading to reduced blood loss and operative time. At the start of surgery, normal saline was injected through the spinal needle at the level involved that helps in dilatation of the soft tissue with the tubular dilator.
Guide wire migration issues occurred in 5 patients in the first quartile. Tube docking–related problems occurred in 3 patients in the first quartile and in 1 patient in the second quartile. Facet joint violation was diagnosed intraoperatively in 3 patients (2 patients in the first quartile and 1 patient in the second quartile).
Out of 3 patients in the first quartile who had tube docking problems, 2 patients had facet joint violation diagnosed intraoperatively, and in 1 patient, superior docked tube led to difficulty in identifying the anatomical landmarks. In all the patients, we removed all the tubes and reinsert again at correct positions, which indirectly increased our surgical time and blood loss intraoperatively. One patient in the second quartile had inferior docked tube due to more inclination of lamina in that patient. One patient also had facet capsule injury in the second quartile as the patient was having very narrow lamina. However, our study showed out of 120 patients, 3 patients had facet joint violation as compared to Jhala and Mistry, 26 which had 5 facet joint injuries in 100 patients.
Therefore, technical problems like tube docking and guide wire migration issues significantly reduced after the first quartile as we had stopped using guide wire and we became much aware of taking True AP/lateral images in fluoroscopy during tube docking with more preoperatively planning of surgical and anatomical landmarks.
Figures 5 and 6 show intraoperative fluoroscopic images with dead AP and lateral view with tube docking site.
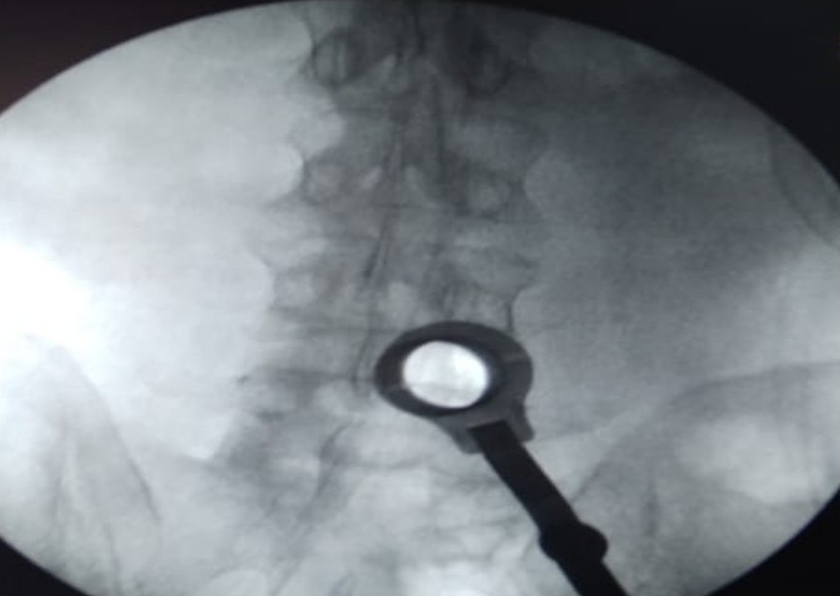
Intraoperative fluoroscopic images with dead AP view with tube docking site.
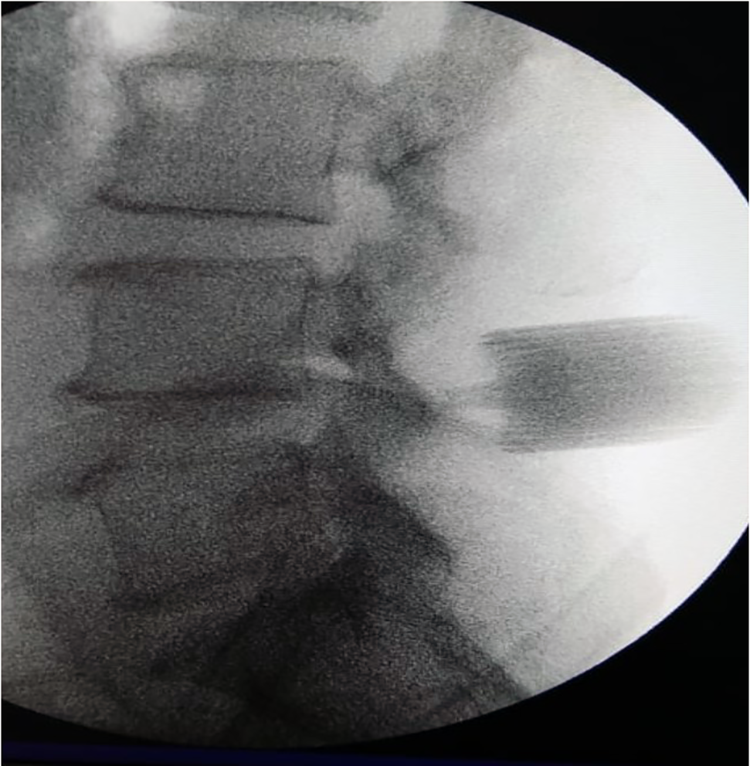
Intraoperative fluoroscopic images with dead lateral view with tube docking site.
The mean hospital stay time in our study was 33.8 hours (no significant difference among quartiles) while in Perez-Cruet et al 27 study it was 7.7 hours and in the Garg et al 28 study it was 72 hours.
Table 2 shows the dural leak percentage in our study and other studies.
Dural Leak Percentage in Our Study and Other Studies.

Four dural leaks had occurred in our study, 3 cases were in quartile 1 due to guide wire migration and 1 case in quartile 2 due to inappropriate handling of dura. None of the patients developed postoperative cerebrospinal fluid leak due to water tight closure with less dead space left in tubular technique.
In our study, 50% to 60% patients returned to work in 3 to 4 weeks when compared with Bookwalter et al, 29 where 40% patients return to work in <5 weeks. The mean time return to work in the Perez-Cruet et al 27 study was 17 days, in the Palmer study 30 was it was 32 days, and in the Casper 18 study it was 18.6 weeks.
Table 3 shows the comparison of recurrence rate in our study with other studies indicating similar results.
Comparison of Recurrence Rate in Our Study With Other Studies Indicating Similar Results.

Length of the tube used is of utmost importance. Longer tube length leads to increase in working length of the instruments intraoperatively, and shorter tube length leads to continuous soft tissue herniation throughout the tube. In initial cases we tended to use shorter length tube causing continuous soft tissue herniation through the tube with more blood loss and increased operative time.
In addition, during initial cases, the surgeon found difficulties in handling the microscope with less eye and hand coordination but became efficient after certain cases.
Therefore, many pitfalls that beginners encounter in this procedure can be avoid easily while considering certain technical points during surgery, such as the following:
Proper preoperative planning about anatomical and surgical landmarks.
True AP/lateral fluoroscopic image intraoperatively.
Infiltrate the tissues with normal saline for easy dilation of muscles.
Guide wire should not be used.
Tube should be in line with the center of disc involved in lateral view.
Dock the tube at base of spinous process at the spino-laminar junction.
Avoid soft tissue herniation through the tube by using appropriate length of the tube.
Surgeon should practice handling the microscope on models for better eye-hand coordination.
Also, practicing on cadavers and bone-saw models can help us reduce technical problems during surgery such as guide wire migration and tube docking–related issues. However, practicing in wet labs on live guinea pig models can reduce other complications such as facet joint violation and dural tear.
The limitations of our study included its retrospective nature; however, the database was constructed prospectively. Certain nonmodifiable confounding factors were present, which include individual surgeon’s learning ability as some surgeons are slow while some are quick learners and other minimally invasive surgery procedures performed by the surgeon during this duration. The number of operations done per month by a surgeon also has an influence on final outcome.
Conclusion
For mastering the art of tubular MED for PIVD and to reduce its learning curve, novice surgeons can avoid the challenges and problems faced during initial cases and improve surgical skills by practicing on cadavers, wet labs, and bone-saw models while following the aforementioned guidelines. Familiarity with instrumentation, communication between surgical teams, and defined expectations from radiology technicians are key to reduce the learning curve.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.