
Abstract
Study Design
Literature review.
Objective
The aim of this literature review was to detail the effects of smoking in spine surgery and examine whether perioperative smoking cessation could mitigate these risks.
Methods
A review of the relevant literature examining the effects of smoking and cessation on surgery was conducted using PubMed, Google Scholar, and Cochrane databases.
Results
Current smokers are significantly more likely to experience pseudarthrosis and postoperative infection and to report lower clinical outcomes after surgery in both the cervical and lumbar spines. Smoking cessation can reduce the risks of these complications depending on both the duration and timing of tobacco abstinence.
Conclusion
Smoking negatively affects both the objective and subjective outcomes of surgery in the lumbar and cervical spine. Current literature supports smoking cessation as an effective tool in potentially mitigating these unwanted outcomes. Future investigations in this field should be directed toward developing a better understanding of the complex relationship between smoking and poorer outcomes in spine surgery as well as developing more efficacious cessation strategies.
Introduction
With an estimated 42.1 million cigarette smokers in the United States, leading to 480,000 deaths annually, smoking is a major public health concern. 1 Although the cardiovascular and respiratory complications are well documented, an emerging body of literature suggests that tobacco addiction predisposes users to an increased incidence of postoperative complications in most surgical disciplines. Of particular interest to the practicing spine surgeon are the increased risks of nonunion, postoperative wound complications, and diminishment of both objective and subjective postoperative outcomes. The purpose of this article is to detail the effects of tobacco use and cessation on spine surgery within the current medical literature.
Arthrodesis
Smoking increases the risk of nonunion in both lumbar and cervical spine procedures. 2 , 3 , 4 , 5 , 6 , 7 , 8 , 9 Though the mechanism of tobacco-related inhibition on bony fusion is not completely understood, the three most commonly accepted theories for the phenomena include a decrease in systemic bone mineral density, osteoblastic cellular metabolism, and local blood flow and angiogenesis. 10 In combination, these negative effects create a challenging fusion environment that has been documented by numerous investigators in both human and animal studies.
Multiple animal models have demonstrated a correlation between nicotine exposure and diminished bone healing. 11 , 12 , 13 In a study examining single-level posterior lateral lumbar fusion in New Zealand white rabbits, Silcox et al reported significantly higher rates of fusion in control specimens than those exposed to systemic nicotine (56 versus 0%, p = 0.02). 11 Additionally, the bone formed in specimens exposed to nicotine exhibited significantly less relative fusion strength and stiffness than bone formed in the control population. 11 In a contradictory rabbit study, Daffner et al reported increased fusion rates and enhanced biomechanical bone quality in subjects with continual low-dose nicotine exposure (5.25-mg patch). 14 Interestingly, the specimens exposed to higher doses of nicotine (10.5 and 21 mg) did not demonstrate higher fusion rates than controls. 14 The contradiction in these similar studies demonstrate the complex and possibly dose-dependent effect nicotine plays in spinal fusion and may suggest that other chemicals contained in cigarette smoke play a role in the inhibition of spinal fusion seen in human studies. 14 , 15
Lumbar Spine
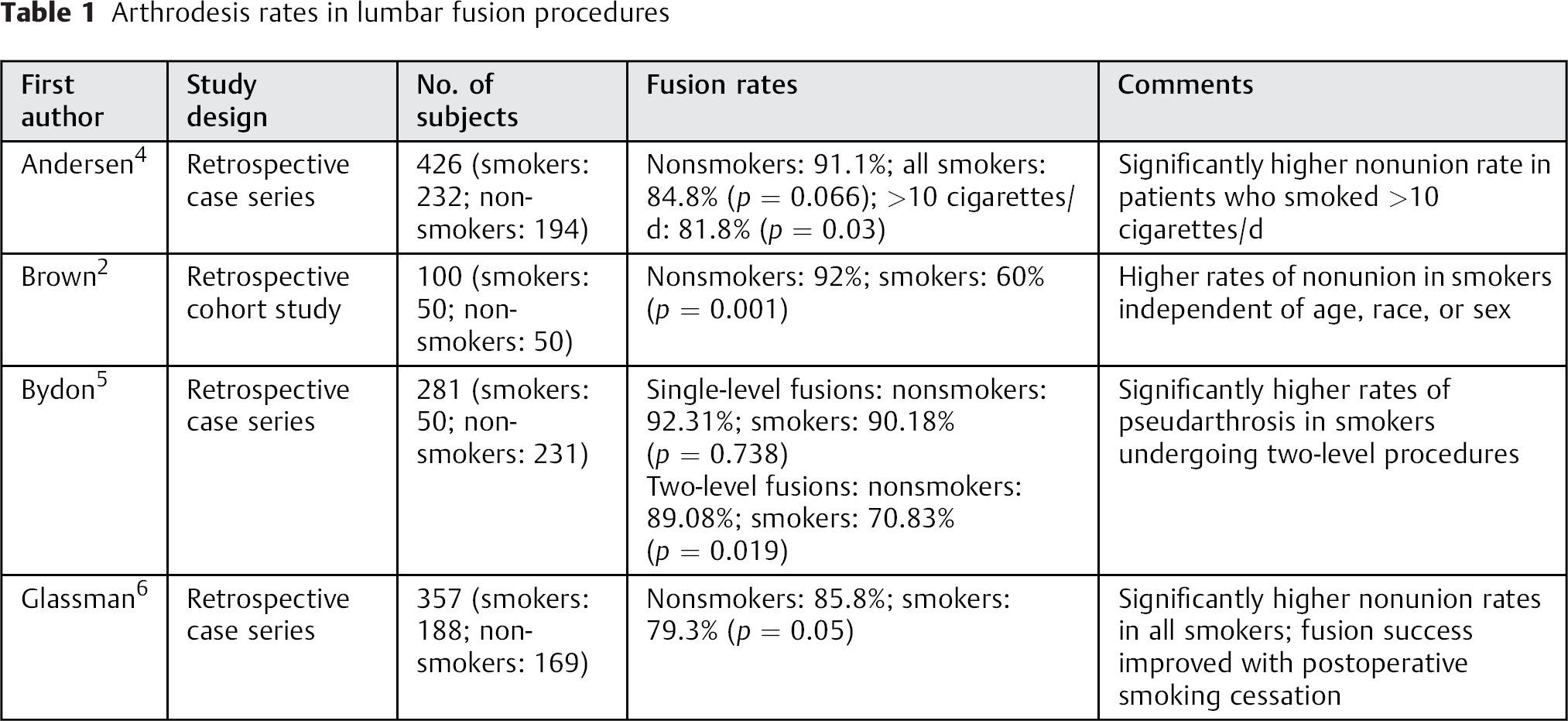
Multiple investigators have reported cigarette use as a major independent risk factor for the development of a lumbar pseudarthrosis (Table 1). 2 , 3 , 4 , 5 , 6 In a review of 357 patients undergoing one- or two-level lumbar fusion, Glassman et al reported a statistically significant increased risk of nonunion in smokers (26.5 versus 14.2%, p < 0.05). 6 This higher observed rate of nonunion in smokers may be influenced by both the amount smoked per day and the number of levels fused. 4 , 5 In a case series of 426 patients, Andersen et al reported a nonunion rate of 18.2% in individuals using more than 10 cigarettes per day compared with a 9.8 and 8.9% rate of pseudarthrosis, respectively, in people who smoked fewer than 10 cigarettes per day and nonsmokers (odds ratio [OR] 2.01, p < 0.016). 4 In a similar review of 281 patients undergoing one- or two-level lumbar fusion, Bydon et al found no significant difference in the rate of nonunion between smokers and nonsmokers in single-level procedures (7.69 versus 9.82%, p = 0.738). 5 However, when analyzing two-level procedures, smokers had a significantly higher rate of nonunion than their nonsmoking counterparts (10.92 versus 29.17%, p = 0.019). 5 In combination, the results of these studies seem to suggest that the risk of lumbar pseudarthrosis associated with cigarette use is multifactorial and at least partially dependent upon the number of cigarettes consumed daily as well as the number of levels fused.
Arthrodesis rates in lumbar fusion procedures
Cervical Spine
Although the effects of cigarette use may be less detrimental in cervical fusion than lumbar procedures, 10 , 16 , 17 multiple investigators have demonstrated a link between smoking and cervical nonunion (Table 2). 7 , 8 , 9 In a retrospective review of 132 patients who underwent anterior cervical diskectomy and fusion, Bishop et al reported a nonunion rate of 14% in smokers compared with 0% in smokers. 7 Additionally, the investigators noted significantly higher rates of delayed union, greater disk space collapse, and diminishment of the disk angle in the smoking population. 7 Although two large retrospective reviews by An et al and Bohlman et al both demonstrated trends toward higher rates of pseudarthrosis in smokers undergoing anterior cervical interbody fusion, neither reached statistical significance. 18 , 19 However, it should be noted that in each of these studies ∼50% of patients had a single-level fusion. Similarly, in a population of 573 patients undergoing single-level anterior cervical diskectomy and fusion with allograft bone and rigid fixation, Luszczyk et al reported no significant difference in the fusion rates among smokers and nonsmokers. 20 In an attempt to determine the effects of smoking on 131 multilevel anterior cervical interbody fusions, Hilibrand et al reported a significantly higher fusion rate in nonsmokers (76 versus 50%, p < 0.02). 21 In combination, the results of these studies suggest that the negative effects of smoking pose a greater risk of nonunion in patients undergoing multilevel interbody cervical fusion than those undergoing single-level procedures.
Arthrodesis rates in cervical fusion procedures
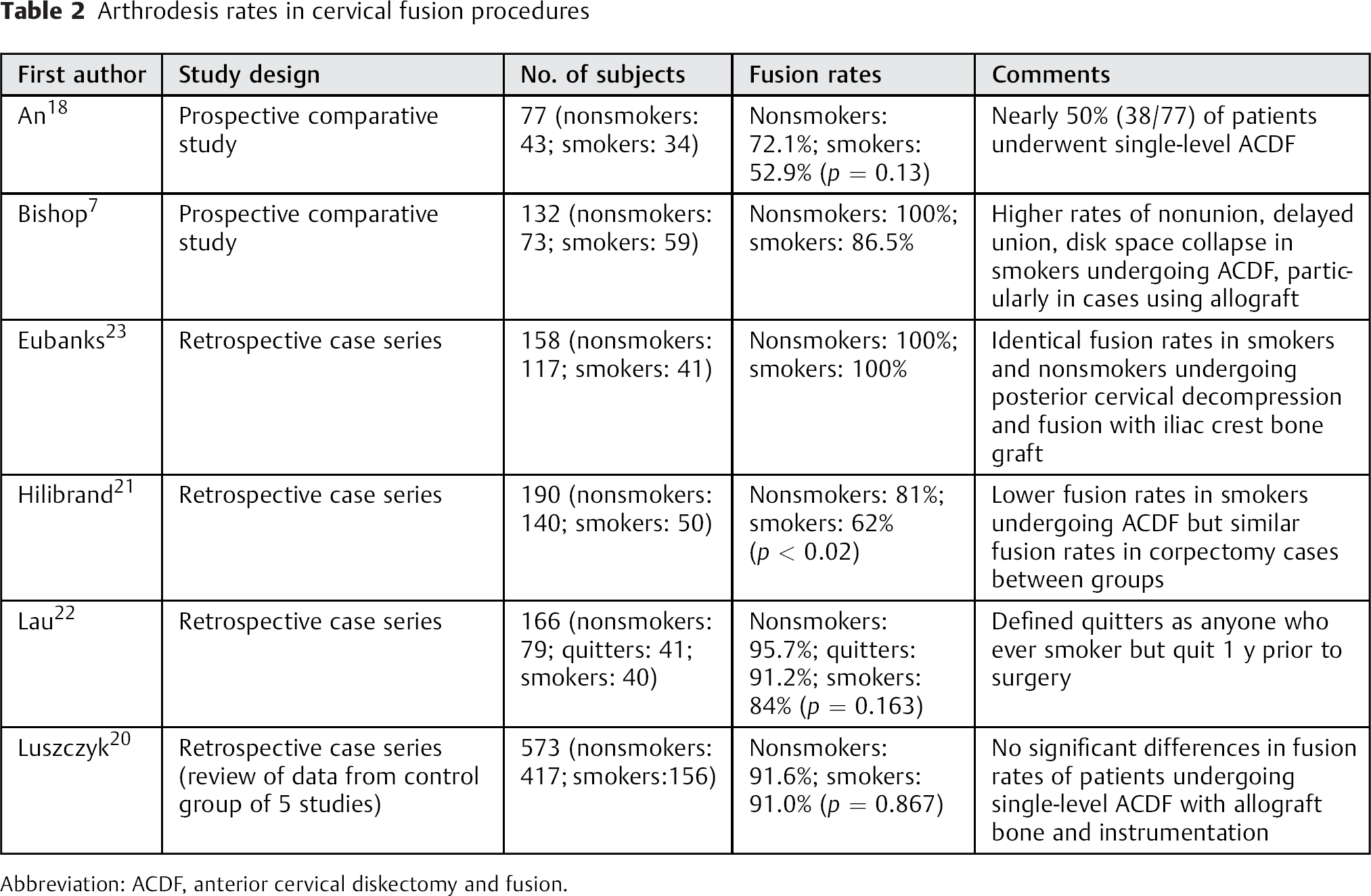
Abbreviation: ACDF, anterior cervical diskectomy and fusion.
Smoking's effect on fusion rates in individuals undergoing multilevel fusion through an anterior cervical corpectomy or a posterior cervical fusion may not be as profound. In a review of 59 patients undergoing corpectomy and strut grafting, Hilibrand and colleagues reported identical rates of fusion between smokers and nonsmokers (93%). 21 However, in a study of 132 patients undergoing cervical corpectomy, Lau et al reported pseudarthrosis rates of 16% in smokers versus 4.3% in nonsmokers at 1 year. 22 Although this difference failed to reach statistical significance, a possible explanation for the trends toward higher rates of pseudarthrosis may be that the average follow-up for this investigation was only 1 year after surgery as opposed to the 2-year period used in the Hilibrand review. This shorter follow-up may be significant; at least two investigators have reported that smoking decreases the rate of fusion even in individuals who ultimately develop a stable union. 7 , 17 In a retrospective case series of 158 patients undergoing posterior cervical fusion with lateral mass screw fixation, Eubanks et al noted identical fusion rates among smokers and nonsmokers (100%). 23 The results of these investigations seem to suggest that in patients who smoke with multiple-level pathology, considering corpectomy or posterior-based procedures when appropriate may provide higher fusion rates than performing multiple-level anterior interbody fusions.
Clinical Outcome Measures
Multiple investigators have reported a correlation between smoking and diminished clinical outcomes with both operative and nonoperative treatment for spinal conditions. 6 , 21 , 23 , 24 , 25 , 26 Although increases in surgical complications such as pseudarthrosis and infection undoubtedly contribute to the diminished postoperative results seen in the smoking population, the systemic effects of nicotine are likely also significant. 6 , 23 , 27 One of the documented effects of smoking is increased rates of disk degeneration in both the cervical and lumbar spine. 27 , 28 , 29 The most commonly proposed mechanism for this phenomenon is that smoking decreases the blood flow to the disk tissue, which leads to decreased cellular metabolism within the intervertebral disk tissue and earlier disk degeneration. 29 , 30 This process likely continues into the postoperative period, potentially predisposing cigarette users to increased rates of recurrent pathologic changes at the operated levels and adjacent-level disease. This smoking-related disk degeneration provides a likely explanation for the higher rates of recurrent or adjacent-level disease requiring reoperation observed in numerous studies. 31 , 32 , 33 , 34 , 35 Nicotine is also a central pain-modulating agent and individuals with higher rates and intensity of spine-related pain may be predisposed to addiction to help mitigate their symptoms. 6 , 36 , 37 , 38 Finally, the higher incidence of depression among smokers predisposes this population to increased back-related disability, which could negatively affect postoperative outcome measures. 6 , 39 , 40 The combination of these factors likely contributes to the differences between smokers and nonsmokers in clinical outcomes with both operative and nonoperative treatment of spinal pathology.
Lumbar Spine
Multiple investigators have demonstrated an association between smoking and worse clinical outcome measures and return to work rates in individuals undergoing lumbar spine procedures. 6 , 24 , 30 , 41 In a review of 825 patients undergoing microdecompression for degenerative lumbar stenosis, Gulati et al noted a significant difference in Oswestry Disability Index (ODI) score change from the preoperative baseline levels in smokers versus nonsmokers (4.2 points, 95% confidence interval [CI] 0.98 to 7.34, p = 0.01). 41 In this study, smokers were also significantly less likely to have achieved a minimal clinically important difference in ODI scores 1 year after surgery than nonsmokers (60.8 versus 69.6%, p = 0.008). 41 From a review of the Swedish Spine Register examining 4,555 patients who underwent decompression with or without fusion for lumbar stenosis, Sandén et al demonstrated that active smokers were more likely to report dissatisfaction with their outcome 2 years after the operative intervention (OR 1.79, 95% CI 1.51 to 2.12). 30 In addition, smokers were more likely to continue to require regular analgesic use (OR 1.86, 95% CI 1.55 to 2.23) and were significantly less likely to improve their walking ability after surgery (OR 0.65, 95% CI 0.51 to 0.82). 30 Additionally, smokers also demonstrated worse preoperative ODI, EuroQol, and Short Form-36 health survey scores and lower return to work rates than their nonsmoking counterparts. 30 Similarly, in a subgroup analysis of the Spine Patient Outcomes Research Trial (SPORT), Pearson et al found that in patients treated for lumbar spinal stenosis, smokers were the only subgroup (of 53 analyzed) in whom the treatment effect of operative management was not significantly different than nonoperative treatment. 24 In this investigation, the treatment effect (measured using the ODI) for smokers was −1.6 compared with −11.7 for nonsmokers (p < 0.001). 24 Because all of the patients in the Gulati study and the majority of the patients in both the SPORT study and the Swedish Spine Register had decompressive surgery without fusion, the results of these studies indicate that smoking is associated with poor results even in the patient populations not undergoing fusion procedures. 24 This data suggests that the diminished postoperative outcomes after surgery seen in the smoking population is not entirely attributable to higher rates of nonunion.
Smoking has also been correlated to worse surgical outcomes and lower return to work rates in procedures involving lumbar fusion. Glassman et al reported significantly higher return to work rates (71 versus 53%, p < 0.001) and mean patient satisfaction scores (2.47 versus 2.78, p < 0.05) in nonsmokers at an average of 49.4 months after surgery. 6 In a prospective cohort study, smokers also noted less relief of their preoperative leg pain 1 year after undergoing lumbar decompression and instrumented fusion. 42 In lumbar spine procedures, regardless of whether a decompression was used alone or with fusion, a pattern of worse surgical outcomes in smokers undergoing surgery seems to prevail in most of the published literature.
Cervical Spine
In cervical spine procedures, smokers appear more likely to experience a suboptimal clinical outcome than nonsmokers irrespective of the approach employed. Hilibrand et al noted significantly higher rates of excellent or good functional outcomes in nonsmokers undergoing multilevel anterior cervical diskectomy and fusion compared with nonsmokers (89 versus 72.5%, p < 0.02) at 2 years after surgery. 21 The authors attributed these differences primarily to the higher incidence of nonunion observed in the smoking population. Eubanks et al reported a similar diminishment in desired outcomes of patients undergoing posterior cervical decompression and fusion. 23 In this review, smokers were five times more likely to report fair or poor results (Odom criteria grade 3 or 4) at an average follow-up of 14.5 months. 23 In a prospective cohort study of 278 individuals undergoing surgical treatment for cervical spondylotic myelopathy, Tetreault et al found that smokers were significantly less likely to experience a successful outcome than nonsmokers, defined by a modified Japanese Orthopaedic Association score ≥16 at 1 year after surgery. 43 In both the study by Eubanks et al and the study by Tetreault et al, fusion rates were equivalent between smokers and nonsmokers, suggesting that factors other than higher rates of pseudarthrosis likely contribute to the diminished postoperative outcomes seen in smokers.
Postoperative Infection
Postoperative infection represents one of the greatest fears for the practicing spine surgeon due to its association with increased costs, longer hospitalization times, and higher rates of secondary surgeries and nonunion. 44 , 45 , 46 , 47 , 48 Tobacco use increases the risk of wound complications and infection by creating a temporary reduction in tissue oxygenation and blood flow and decreasing the effectiveness of inflammatory cell function and oxidative bactericidal mechanisms; in addition, reparative cell function is inhibited. 49 Researchers from multiple surgical disciplines have correlated smoking with higher rates of wound complications and infections. 49 , 50 , 51 , 52 , 53 , 54 , 55 More specifically, these effects have been illustrated in spine surgery by multiple investigators (Table 3). 47 , 48 , 54 , 55 In a review of the Department of Veterans’ Affairs National Surgical Quality Improvement Program database, Veeravagu et al reported that smokers had a statistically significant higher rate of infection than nonsmokers (OR 1.19, 95% CI 1.02 to 1.37). 47 In a retrospective review of 1,629 procedures, Fang et al reported a postoperative infection rate of 4.4%. 48 In this study, smokers represented 33% of the population who developed infections compared with only 16.8% of those who healed uneventfully (p = 0.03). 48 The results of these large retrospective reviews point to tobacco use as a significant potentially modifiable risk factor for the development of postoperative infection in spine surgery.
Risk of infection with smoking in spine surgery
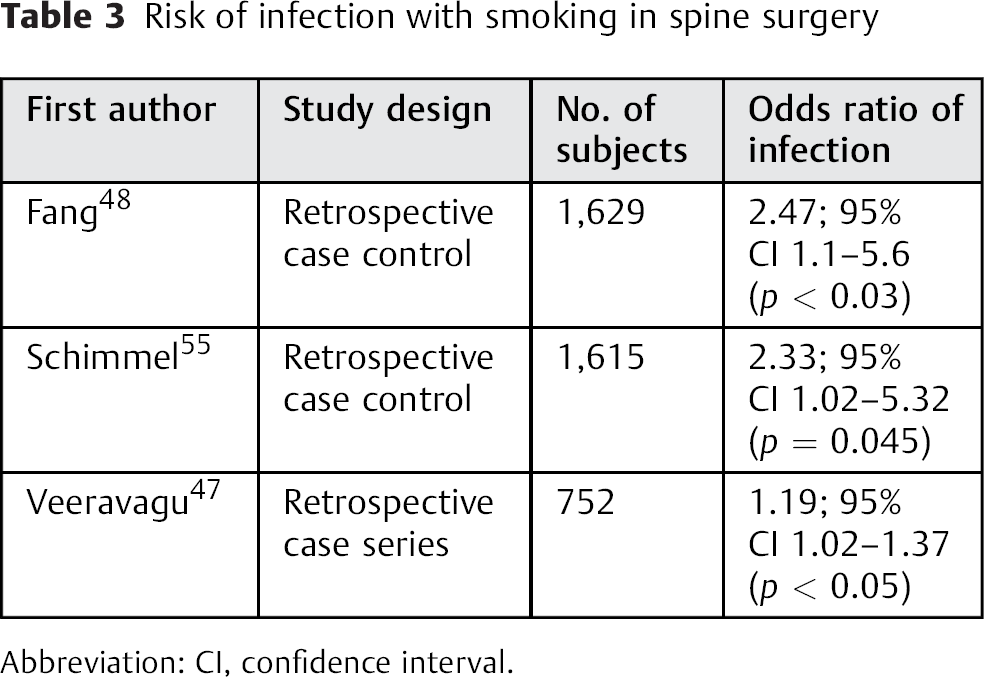
Abbreviation: CI, confidence interval.
Smoking Cessation
The overall health benefits related to smoking cessation are well documented and include decreased risks of multiple types of primary malignancies, coronary and peripheral arterial disease, respiratory infection, cerebral vascular accident, and chronic pulmonary disease. 56 , 57 , 58 , 59 Similarly, multiple investigators have reported significant benefits associated with tobacco cessation in patients undergoing spine surgery. In a retrospective analysis of 86 patients with documented nonunion at 88 levels, Carpenter et al noted that smoking cessation significantly affected patient outcome scores on a questionnaire that addressed pain, functional status, progress after the surgery, and postoperative satisfaction. 60 In this study, individuals who successfully stopped smoking scored 65/100 and patients who continued smoking scored 45/100 (p = 0.03). 60 The investigators also noted a significantly greater likelihood of returning to full-time work in patients who stopped smoking. 60 In a retrospective analysis containing 188 smokers, Glassman et al also demonstrated more favorable outcomes in patients who quit smoking postoperatively. 6 Within this population, the investigators noted nonunion in 26.5% (18/68) of patients who did not stop smoking after surgery compared with 18.2% (8/44) and 17.1% of patients who stopped smoking 1 to 6 months and greater than 6 months after surgery, respectively. 6 Individuals who were able to stop smoking for longer periods of time after surgery also had higher rates of return to either full or light duty. Nonquitters returned to work at a rate of 53.4% and those who abstained 1 to 6 months and greater than 6 months after surgery returned to work at rates of 58.6 and 74.6%, respectively. 6 The differences in return to work rates in nonquitters and patients who quit smoking for up to 6 months reached statistical significance (p < 0.005). Postoperative patient satisfaction also demonstrated trends toward improvement with the ability to quit smoking after surgery. The reported satisfaction score for nonquitters was 3.03 compared with scores of 2.64 and 2.63 in patients who quit smoking for longer than 1 month or greater than 6 months, respectively. 6 The differences in patient satisfaction and return to work rates remained present after cases of nonunion were excluded, indicating that higher rates of pseudarthrosis in nonquitters does not fully explain the discrepancies in postoperative outcomes.
When to quit and how long to refrain from smoking are important questions for the practicing clinician to answer when advising patients considering elective spine surgery. Although there is no definitive data, several investigators have provided meaningful information on which to base recommendations. Glassman et al noted significant improvements in fusion rates, satisfaction scores, and return to work rates in patients who refrained from smoking postoperatively, 6 with results tending to be better in individuals who quit for more than 6 months after surgery. 6 Interestingly, preoperative smoking cessation did not significantly alter the postoperative outcomes. 6 Notably, the investigators found no association between preoperative smoking cessation and fusion rates, satisfaction scores, or return to work rates. 6 Despite these findings, preoperative smoking cessation for 4 weeks is associated with a decreased risk of infection, perioperative respiratory, and wound complications. 49 , 61 , 62 In a meta-analysis of studies from a range of surgical specialties, Mills et al reported a 41% risk reduction of postoperative complications for patients who quit smoking before surgery. 63 Within the studies analyzed, trials that consisted of smoking cessation for 4 weeks or greater had a significantly larger treatment effect than those investigating shorter periods of abstinence from tobacco. 63 A patient's ability to stop smoking preoperatively may also be an important predictor of their ability to refrain from smoking after surgery. 6 To this end, Glassman et al noted that less than 10% of patients who smoked up until the day of surgery were able to stop postoperatively. 6 As a result of these findings in our own practice, we request patients be free of tobacco 4 weeks before undergoing elective spine surgery and continue to refrain from smoking for 6 months after surgery.
With reported success rates as low as 8 to 27.5% in the general population, 64 , 65 , 66 many spine surgeons are skeptical of a patient's ability to reliably quit smoking around the time of surgery. 67 In a retrospective review of 426 patients who underwent lumbar fusion, Andersen et al noted that only 13% of patients were able to stop smoking after surgery with counseling alone. 4 Of the individuals who did quit, 50% experienced a relapse at some point during their postoperative course. 4 Although these abysmal rates of success lead some to question the value of time invested in tobacco cessation attempts, conflicting evidence suggests that patients preparing for elective spine procedures may quit at higher rates than the general smoking population. To this end, Glassman et al reported that 63.8% of smokers quit for at least 1 to 6 months and 40.4% quit for at least 6 months after surgery. 6 Impressively, 90% of this population did not need the aid of nicotine-containing gums or patches or other medications. 6 These findings may indicate that individuals considering spine surgery represent a portion of the population more likely to quit if counseled appropriately on the risk of continuing to smoke in the postoperative period. However, given the conflicting data of the efficacy of counseling alone, physicians should consider offering any of the host of validated cessation aids in conjunction with preoperative patient education to maximize the success rate.
Conclusion
Due to its association with higher rates of postoperative infection and pseudarthrosis and lower clinical outcome measures, smoking presents a major challenge to the practicing spine surgeon. Fortunately, these risks appear to be mitigated to some extent with tobacco cessation in the perioperative period. As a result, surgeons should counsel smokers on their elevated risk prior to surgery and assist in the development of a comprehensive cessation program that ideally would start at least 4 weeks prior to surgery and continue 6 months postoperatively. Future investigations in this field should be directed toward developing a better understanding of the complex relationship between smoking and its effect on individuals undergoing spine surgery as well as the development of more efficacious cessation strategies.
Disclosures
Keith L. Jackson II: none
John G. Devine: none
Footnotes
Disclaimer
The views expressed herein are those of the author(s) and do not reflect the official policy of the Department of the Army, Department of Defense, or the U.S. Government.