
Abstract
Postoperative discal pseudocyst (PDP) is a rare complication that can occur after percutaneous endoscopic lumbar discectomy (PELD), microendoscopic discectomy, and laminectomy. The PDP pathogenesis and pathological process remain unclear. We described two PDP cases following PELD, with long-term follow-up results. The first patient was an Asian male, 30 years old, who experienced unbearable low back pain with right lower limb radiating pain for 2 years. The second patient was also an Asian male, 21 years old, who experienced low back pain with bilateral lower limb numbness. Both patients were diagnosed with lumbar disc herniation, underwent PELD, and relapsed after discharge. The diagnosis was PDP in each case, and conservative treatment was initiated with oral anti-inflammatory drugs and rest. Eventually, the symptoms in both patients resolved. Magnetic resonance imaging showed that the discal cysts had disappeared. The follow-up of these two PDP cases after PELD showed good results, demonstrating that PDP may be a self-healing disease. Conservative treatment is effective, and surgery should be performed only in an emergency. These case reports and literature review can help improve the understanding of PDP.
Keywords
Introduction
Compared with traditional simple laminectomy and discectomy, percutaneous endoscopic lumbar discectomy (PELD) is minimally invasive and associated with rapid recovery in lumbar disc herniation treatment. 1 PELD is also associated with numerous complications, such as cerebrospinal fluid leakage, nerve injury, and postoperative nucleus pulposus protrusion. However, complications are less common with PELD than with microdiscectomy. Post-discectomy discal pseudocyst (PDP) is a rare complication that consists of a cystic lesion with or without symptoms after protruding nucleus pulposus removal.1,2 In this report, we present two cases of PDP after PELD in patients who received long-term follow-up after laminectomy. The reporting of this study conforms to the CARE guidelines. 3
Case 1 presentation
Clinical presentation
The first patient was an Asian male, 30 years old, who came to our hospital because of unbearable low back pain with right lower limb radiating pain for 2 years. Medication and conservative treatment were ineffective. Physical examination revealed positive right straight-leg-raising test results of 40°, and that muscle strength and limb tension, skin tactile sensation and prickling pain, and bilateral tendon reflexes were normal. The patient had a history of several years of hyperuricemia and hyperlipidemia and had been prescribed daily nifedipine.
Radiological evaluation
Magnetic resonance imaging (MRI) revealed L5/S1 disc herniation (right central) (Figure 1a, b).

Preoperative T2-weighted magnetic resonance image (MRI), sagittal view, showing disc herniation at the L5–S1 disc level (a) and axial view showing right-sided herniation (b).
Treatment
Transforaminal PELD was performed under epidural anesthesia.
Outcome and follow-up
After surgery, the patient’s lower back pain with right lower limb radiating pain subsided on the second day. Physical examination revealed normal right straight-leg-raising test results. After 3 days, he was discharged and resumed work after 2 weeks. However, 6 weeks later, he presented with recurrent low back and mild right leg pain. MRI showed a 5- × 8-mm high-intensity signal on T2-weighted imaging and a low-intensity signal on T1-weighted imaging in the original operation segment (Figure 2a, b). We prescribed oral nonsteroidal anti-inflammatory and analgesic drugs and advised continued rest. After 3 months, the low back and right leg pain disappeared, and he returned to work. MRI showed a 1- × 2-mm discal cyst (Figure 3a, b). After another 3 months, he had almost no low back and right leg pain, and almost no discal cyst could be visualized on MRI (Figure 3c, d).

Postoperative radiographic findings after 6 weeks showing a cystic lesion in the L5–S1 disc, right side, on magnetic resonance imaging (MRI) (a, b).

Eighteen weeks postoperatively, axial and sagittal magnetic resonance images (MRI) showing a small cystic lesion (a, b) and at week 30, axial and sagittal MRI showed almost no cystic lesion (c, d).
Case 2 presentation
Clinical presentation
The second patient was also an Asian male, 21 years old, who came to our hospital because of low back pain with bilateral lower limb numbness, mainly in the left leg, lateral side, and the right leg, posterior side. One year of medication and conservative treatments were ineffective. Physical examination revealed bilateral positive straight-leg-raising test results (30°), and that muscle strength and limb tension, skin tactile sensation and prickling pain, and bilateral tendon reflexes were normal. The patient had been healthy, with no other diseases.
Radiological evaluation
MRI showed L5/S1 disc herniation (central) (Figure 4a, b).

Preoperative magnetic resonance image (MRI), sagittal view, showing disc herniation at the L5–S1 disc level (a) and axial view showing central herniation (b).
Treatment
Transforaminal PELD was performed under epidural anesthesia.
Outcome and follow-up
After surgery, low back pain subsided on the second day. On day 6, the lower limb numbness also subsided. Physical examination revealed normal bilateral straight-leg-raising test results. The patient resumed work after 2 weeks; however, 7 weeks later, he developed recurrent mild bilateral leg numbness. MRI showed a 5- × 7-mm high-intensity signal on T2-weight imaging and a low-intensity signal on T1-weighted imaging in the original operation segment (Figure 5a, b). We prescribed oral nonsteroidal anti-inflammatory and analgesic drugs and rest. After 19 weeks, the bilateral leg numbness disappeared, and no discal cyst was visualized on MRI (Figure 5c, d).

Magnetic resonance imaging (MRI) findings 7 weeks postoperatively showing a central cystic lesion in the L5–S1 disc (a, b) and Axial and sagittal MRI 26 weeks postoperatively showing no cystic lesion (c, d).
Discussion
PDP is a rare complication after PELD, microendoscopic discectomy (MED), and laminectomy. 2 We searched the PubMed database using the following search terms: “disc pseudocyst” and “annular pseudocyst”. We found seven studies, including five Asian (Japan, Korea, China) studies, that reported 34 PDP cases (a partial reference list is provided in Table 1).2,4–7 In 2001, Chiba et al. 8 named intraspinal extramedullary cysts as disc cysts. In 2009, Young et al. 2 were the first to report two cyst cases after nucleus pulposus enucleation. Owing to the incomplete cyst wall, this condition was named PDP. Kang and Park 9 reported 15 PDP cases in 1503 PELD patients, with an incidence rate of 1%. Shiboi et al. 5 reported 2 PDP cases in 359 PELD patients (0.28% incidence rate). In these studies, 94.12% (32 cases) of PDP patients were Asian and only 5.88% (2 cases) were White. The White patients underwent laminectomy, not PELD or MED.
Summary of some of the previous cases of postoperative discal pseudocyst (PDP).
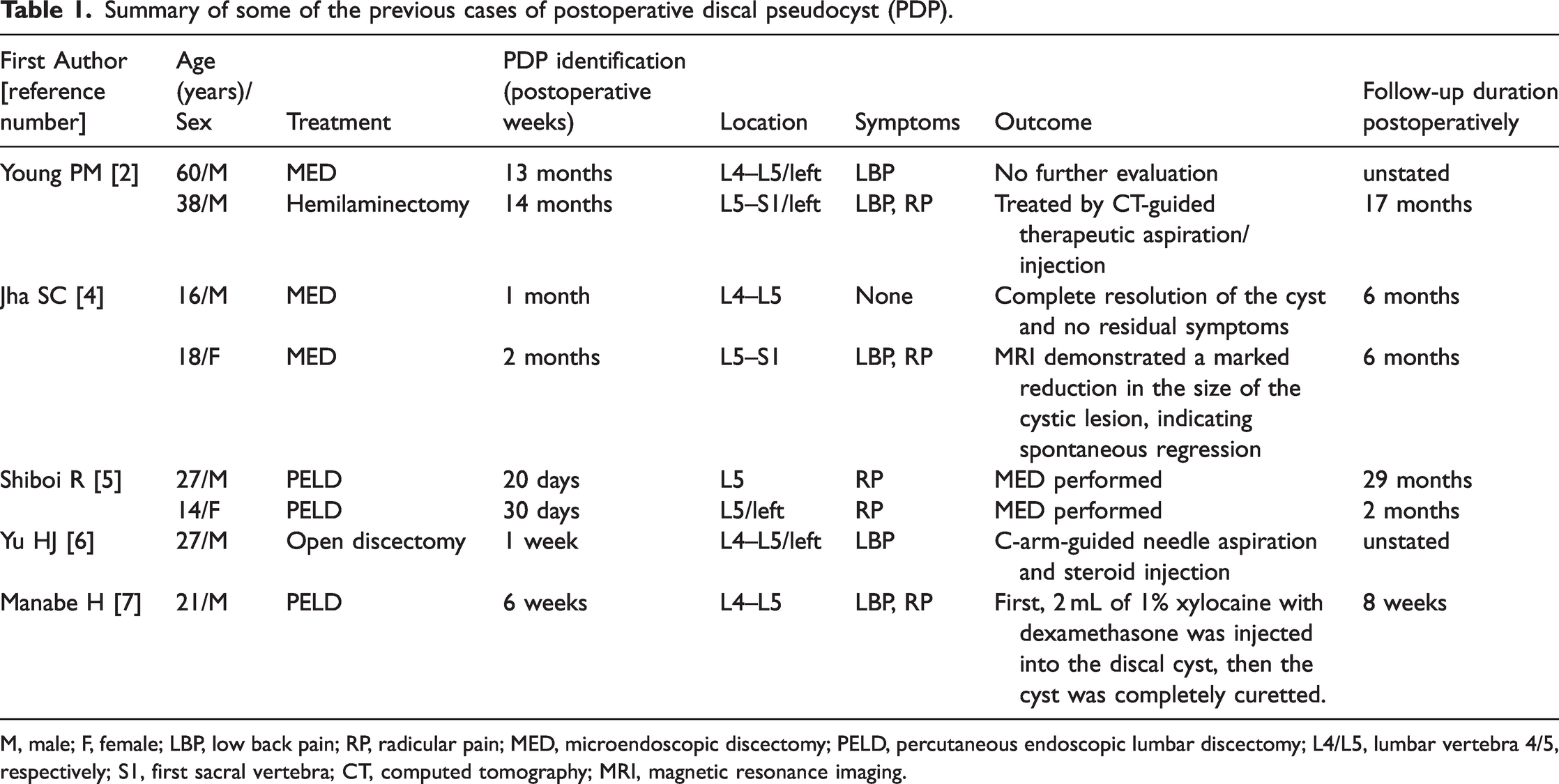
M, male; F, female; LBP, low back pain; RP, radicular pain; MED, microendoscopic discectomy; PELD, percutaneous endoscopic lumbar discectomy; L4/L5, lumbar vertebra 4/5, respectively; S1, first sacral vertebra; CT, computed tomography; MRI, magnetic resonance imaging.
How does PDP develop? The disc cyst is formed following intervertebral disc injury or blood vessel rupture in the spinal canal. 1 A PDP is a disc cyst formed after PELD, MED, or laminectomy. 2 Chung et al. 10 and Young et al. 2 hypothesized that a protruding intervertebral disc induces granulation tissue to wrap around the annulus fibrosus surface forming a pseudomembrane. PELD destroys part of the annulus fibrosus but does not remove the pseudomembrane outside the annulus fibrosus. After operation, fluid and blood in the intervertebral disc are squeezed by axial load and form a PDP and the pseudomembrane. Kang and Park 9 reported 1503 PELD cases, and the incidence rate of PDP at L4/5 was 0.54%; the incidence at L5/S1 was 2.73%, and that in other segments was 0%. These results showed that PDP might be more prone to occur at the L5/S1 disc. Kang and Park 9 believed that electrocoagulation, hemostasis, and vaporization during PELD aggravate the inflammatory reaction between the posterior longitudinal ligament, annulus fibrosus, and surrounding tissues, which then induces PDP. However, the PDP pathogenesis is unclear, and we speculate that the channel gap formed by the endoscope and vaporization by electrocoagulation provide favorable conditions for its formation.
On the basis of the data from the 32 previous cases and our two cases, the average PDP formation time after PELD and MED is approximately 41 days. However, the time to PDP detection by MRI does not represent the time to PDP formation. PDPs identified by MRI may have been present for some time. The best treatment for PDP is controversial; both conservative and surgical results are satisfactory.2,4,11 Manabe et al. 7 reported a good outcome and low recurrence rate following aspiration and surgical treatment. However, the two cases of PDP that we reported received conservative treatment and achieved good results. The cyst in our first case disappeared after 30 weeks and in the second case, after 24 weeks. Therefore, according to the literature and our treatment experience, we consider that the predicted prognosis of this disease is good. For most PDP patients, conservative treatment can be indicated, such as with oral anti-inflammatory drugs and osmotic diuretics. For patients with acute and severe symptoms, computed tomography-guided puncture and aspiration can be performed.
In conclusion, in this article, we presented two PDP cases that developed after PELD. The follow-up showed good results, demonstrating that PDP may be a self-healing disease. Conservative treatment is effective, and surgery should be performed only when necessary. The details of our cases and those identified in the literature review can help in understanding PDP.
Research Data
Research Data for Postoperative discal pseudocyst caused by percutaneous endoscopic lumbar discectomy: two case reports and a literature review
Research Data for Postoperative discal pseudocyst caused by percutaneous endoscopic lumbar discectomy: two case reports and a literature review by Kun Gao, Yafei Cao, Weiji Yu, Weidong Liu, Shufen Sun and Yihong Wu in Journal of International Medical Research
Footnotes
Acknowledgements
We are grateful to the patients and all the researchers, including the physicians, nurses, and technicians, who participated in this case.
Author contributions
Each of the authors contributed significantly to this manuscript. All authors are responsible for the contents, and all have read and approved the manuscript for submission. Kun Gao: Data curation, Writing-Original draft preparation. Weiji Yu and Weidong Liu: Writing-Reviewing and Editing. Shufen Sun and Yihong Wu: Visualization, Resource, Data curation. Yafei Cao: Supervision, Project administration.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Ethics statement
Ethics approval is not required in our institution for case reports. Written informed consent for treatment and publication of this case report were obtained from the patient and Shenzhen Traditional Chinese Medicine Hospital.
Funding
The authors disclose receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Shenzhen Science and Technology Program (No. JCYJ20210324111205015) and the Sanming Project of Medicine in Shenzhen (No. SZSM201812066).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.