
Abstract
Study Design:
Narrative review.
Objectives:
The purpose of this article is to perform a review of the literature assessing the efficacy of opioid alternatives, multimodal pain regimens, and rapid recovery in pediatric spine surgery.
Methods:
A literature search utilizing PubMed database was performed. Relevant studies from all the evidence levels have been included. Recommendations to decrease postoperative pain and expedite recovery after posterior spinal fusion in adolescent idiopathic scoliosis patients have been provided based on results of studies with the highest level of evidence.
Results:
Refining perioperative pain management to lessen opioid consumption with multimodal regimens may be useful to decrease recovery time, pain, and complications. Nonsteroidal anti-inflammatory drugs, acetaminophen, gabapentin, neuraxial blockades, and local anesthesia alone offer benefits for postoperative pain management, but their combination in multimodal regimens and rapid recovery pathways may contribute to faster recovery time, improved pain levels, and lower reduction in total opioid consumption.
Conclusion:
A rapid recovery pathway using the multimodal approach for pediatric scoliosis correction may offer superior postoperative pain management and faster recovery than traditional opioid only pain protocols.
Keywords
Introduction
Postoperative pain after posterior spinal fusion (PSF) for adolescent idiopathic scoliosis (AIS) has recently seen changing trends in management. By using effective postoperative pain regimens, surgeons can significantly improve patient satisfaction, facilitate early mobilization, promote oral intake, lower postoperative pain, and shorten length of hospital stay. 1 -3 Customary practice utilized opioids as its cornerstone, but this practice is associated with adverse side effects. 3,4 These complications delay patient mobilization and lengthen patient stay thus encouraging a transition to a more balanced regimen. Multimodal pain control in orthopedic surgery has been especially well described in adult reconstruction literature and studies have shown reduced opioid consumption, improved pain control, and shorter hospital stays. 5 Kurd et al 6 provided a comprehensive review of the literature and found a growing body of evidence supporting the use of multimodal analgesia in adult spine surgery; however, the role of multimodal analgesia in pediatric spine surgery is not as well established. The purpose of this article was to review current literature supporting multimodal pain regimens and rapid recovery pathways in AIS surgery.
Multimodal Pain Management
Expedient recovery of patients following posterior spinal fusion is intimately related to pain control and mobilization. Conceptually, a multimodal approach to pain control stems from the ills associated with opioid medications. There is variability in the medications utilized in multimodal approaches across institutions. In this section, we review several cornerstone medications that have been associated with multimodal pain regimens, including nonsteroidal anti-inflammatory drugs (NSAIDs), intravenous (IV) acetaminophen, gabapentin, epidurals, intrathecal morphine, and local medications.
Opioids
Opioids remain a mainstay in postoperative pain control after AIS surgery. Although effective in pain control, they are associated with well-established side effects. These adverse effects include the following: somnolence, pruritis, respiratory depression, ileus, nausea, and urine retention. 7 Currently, there is no consensus on what dose of opioid is the optimum dose to control postoperative pain, but controlling pain while minimizing opioid administration is a ubiquitous goal. Traditionally, intravenous opioids were the primary medication for pain relief after PSF for AIS; however, authors have described new protocols to minimize opioid use. In a recent best practice guideline for postoperative care after PSF for AIS, Fletcher et al 8,9 describe a protocol in which patients are prescribed intravenous morphine-based patient-controlled analgesia (PCA) for 1 day postoperatively. The PCA is then discontinued and patients are transitioned to oral narcotics. These authors attribute a decrease in intravenous opioids as a factor in quicker rehabilitation and recovery for their patients postoperatively.
The duration of oral narcotic prescription after discharge has not been studied and is variable based on surgeon preference. At our institution, patients are prescribed oral hydrocodone/acetaminophen 5/325 mg every 4 hours as needed for pain for 7 days after discharge. Patients are encouraged to transition to oral acetaminophen or ibuprofen after the 7-day period. Further studies are needed to create a guideline for appropriate prescribing of opioids after discharge.
Nonsteroidal Anti-Inflammatory Drugs
NSAIDs have shown promise in reducing postoperative opioid requirements in the pediatric population (Table 1). Michelet et al 15 performed a meta-analysis of the use of NSAIDs for pediatric postoperative pain in general pediatric surgery and found that perioperative NSAID administration significantly reduced opioid consumption and nausea. Hayes et al 16 surveyed 61 anesthesiologists from international academic pediatric hospitals and found that 59% routinely use NSAIDs in the postoperative period following pediatric scoliosis surgery. In this survey, IV ketorolac was the most commonly reported agent. 16 Munro et al 10 performed a prospective randomized double-blinded placebo-controlled trial studying the effect of low-dose ketorolac following PSF. Patients who received ketorolac had significantly lower pain scores on postoperative days (POD) 1 and 2 and consumed less morphine in the postanesthesia care unit through POD 2. Patients in the ketorolac group also tolerated activity better on POD 1 than the patients in the control group. There was no difference in the incidence of pruritus, nausea, vomiting or constipation. 10
NSAIDs and Acetaminophen Studies.
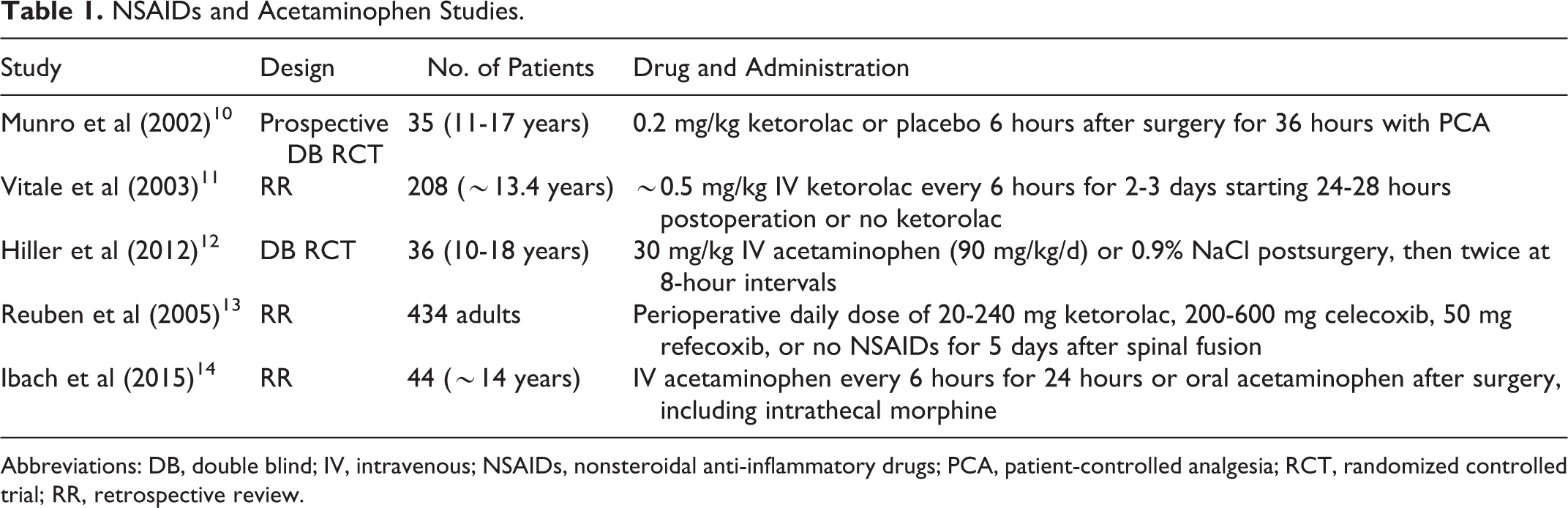
Abbreviations: DB, double blind; IV, intravenous; NSAIDs, nonsteroidal anti-inflammatory drugs; PCA, patient-controlled analgesia; RCT, randomized controlled trial; RR, retrospective review.
Despite the benefits, NSAID use has not been unanimously adopted in spinal fusion surgeries because of the potential risk of pseudoarthrosis and postoperative bleeding. 17,18 Two key studies evaluated these risks but did not find the same risks in pediatric populations. Sucato et al 19 performed a retrospective review comparing patients who had postoperative ketorolac and those who did not following PSF for AIS. The overall incidence of pseudoarthrosis was 2.5% for all patients. There was no difference in the incidence of pseudoarthrosis comparing a patient receiving ketorolac (1.9%) and one who did not (3.1%). They subsequently concluded that ketorolac may be useful to supplement pain management postoperatively in AIS surgery and did not increase the risk of pseudarthrosis. 19
Additionally, the risk of postoperative bleeding following NSAID administration has not been validated. Vitale et al 11 performed a retrospective review to determine whether there is any association between the use of ketorolac and postoperative complications in a group of children who underwent scoliosis surgery. These investigators looked at postoperative transfusion and reoperation rates for any reason, including pseudoarthrosis. They found that out of 208 children undergoing spine surgery, postoperative use of ketorolac did not significantly increase the incidence of blood transfusion and reoperation for any reason. They concluded that the use of ketorolac was safe in the postoperative period following pediatric scoliosis surgery. 11
Intravenous Acetaminophen
IV acetaminophen has shown promise in reducing opioid requirements and decreasing postoperative pain in adult studies; however, evidence in pediatric patients has been lacking. Oral and intravenous acetaminophen are beneficial for their anti-inflammatory, antipyretic, and analgesic effects. 20 Hiller et al 12 performed a randomized, placebo-controlled, double-blind study to evaluate the effect of IV administered acetaminophen on postoperative pain in children and adolescents undergoing surgery for idiopathic scoliosis or spondylolisthesis (Table 1). Patients in this study were given 30 mg/kg of IV acetaminophen or normal saline postoperatively at 8-hour intervals. The authors found that IV acetaminophen administered at 90 mg/kg/d as an adjuvant to oxycodone improved analgesia, but did not diminish oxycodone consumption 24 hours postoperatively after major spine surgery in children and adolescents. 12 Considering the relative safety of IV acetaminophen, using it for controlling postoperative pain may be beneficial; but further studies are needed to determine its efficacy.
Gabapentin
The neuromodulatory agent gabapentin is an antiepileptic medication thought to improve pain through reduction of sensory nerve excitability. Studies have demonstrated efficacy in the following adult spine surgery, but results in pediatric spine deformity population have been mixed (Table 2). Mayell et al 21 performed a randomized control trial to study the effects of a single preoperative dose of gabapentin 600 mg versus placebo on postoperative morphine consumption in the first 24 hours after surgery. They found that a single preoperative dose of gabapentin was not associated with a significant difference in opioid consumption or pain scores in adolescents undergoing idiopathic scoliosis surgery. 21 Rusy et al 22 performed a randomized double-blind controlled trial to determine the effect of gabapentin on acute pain in the immediate postoperative period, specifically morphine consumption and opioid side effects, in the pediatric spinal fusion patient with idiopathic scoliosis. Patients in this study were randomized to receive a preoperative dose of oral gabapentin at 15 mg/kg followed by 5 mg/kg of oral gabapentin 3 times daily postoperatively or a placebo. They found that preoperative gabapentin with continued administration is effective in reducing morphine consumption and pain scores in the early postoperative period. Benefits were observed for the immediate postoperative period through day 2, but no benefits were observed after POD 2. No significant differences in opioid side effects were found between the gabapentin and placebo groups. 22 These studies show that preoperative and postoperative gabapentin may help reduce immediate postoperative opioid consumption, but no benefit after the immediate postoperative period.
Neuromodulatory Agent Studies.

Abbreviations: DB, double blind, PCA, patient-controlled analgesia; RCT, randomized controlled trial; RR, retrospective review.
Neuraxial Blockades—Epidural Analgesia
Efficacy of neuraxial blockade for postoperative pain control after adult spine surgery has been demonstrated with level 1 evidence, but efficacy or safety have not been shown to be superior compared with IV medication after pediatric scoliosis surgery. There have been several retrospective studies assessing the efficacy of epidural analgesia after pediatric spine surgery (Table 3). Hong et al 32 retrospectively reviewed the charts of 56 children who had epidural analgesia after AIS surgery. They found that none of these children had any neurologic or respiratory adverse event, ambulation occurred on PODs 1 or 2, and that mean length of stay was 3.95 days. They concluded that epidural analgesia was a safe and effective way to control postoperative pain after AIS surgery.
Epidural Analgesia Studies.
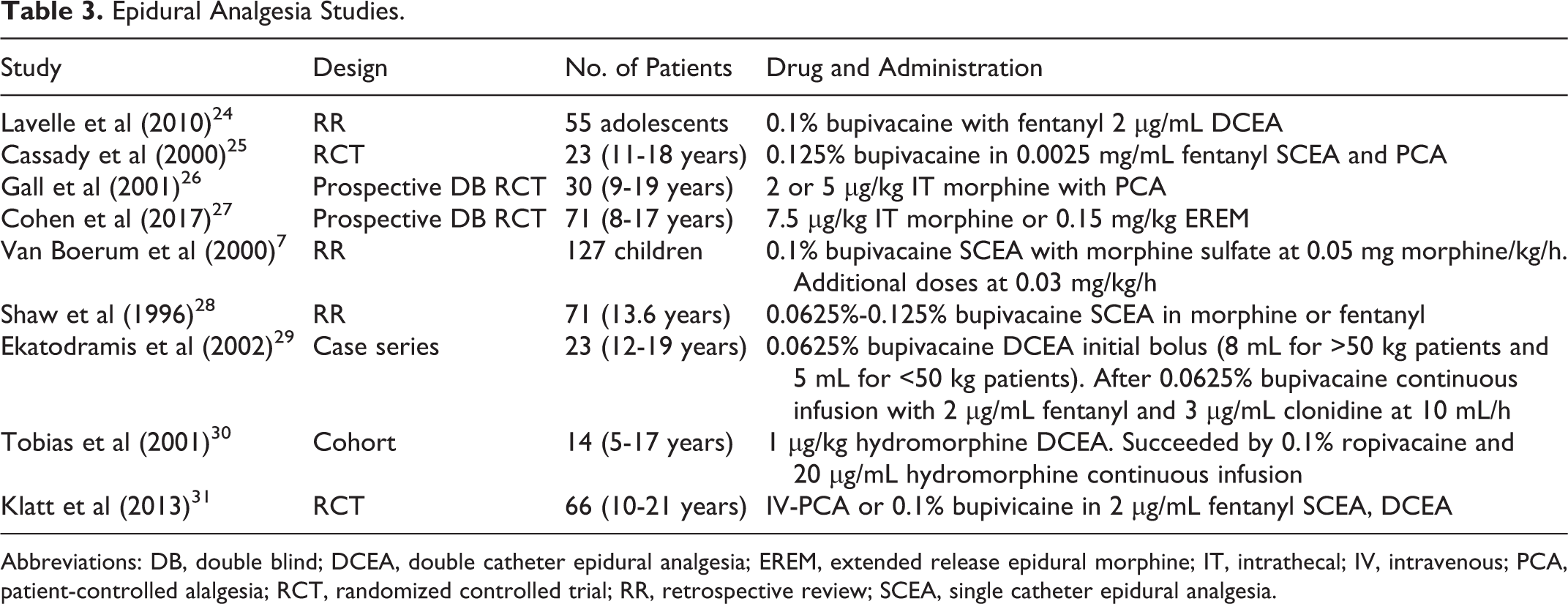
Abbreviations: DB, double blind; DCEA, double catheter epidural analgesia; EREM, extended release epidural morphine; IT, intrathecal; IV, intravenous; PCA, patient-controlled alalgesia; RCT, randomized controlled trial; RR, retrospective review; SCEA, single catheter epidural analgesia.
Cassady et al 25 performed a prospective randomized control trial comparing the effects of continuous epidural anesthesia (CEA) with PCA after posterior spinal fusion for AIS. These investigators randomized 33 patients into either the CEA or PCA group and measured pain intensity with self-reported visual analogue scale (VAS), postoperative resumption of bowel sounds, liquid intake, and adverse effects. They found that there was no significant difference in VAS scores, liquid intake, or adverse effects; however, return of bowel sounds was significantly faster in the CEA group. The authors concluded that both CEA and PCA are comparable in terms of efficacy and safety.
O’Hara et al 33 also performed a prospective double-blinded randomized controlled trial studying the effect of epidural versus intravenous analgesia following PSF for AIS. They randomized 31 patients into 3 groups: a low-dose epidural group, high-dose epidural group, and a placebo group. They found no difference in postoperative pain control, oral intake, bowel sounds, ambulation, or length of stay between the 3 groups. 33 They concluded that there was no difference in in outcomes when using epidural or intravenous analgesia after PSF in adolescents.
Intrathecal Morphine
Intrathecal morphine has shown promise in decreasing intraoperative blood loss and opioid requirement after AIS surgery. Blackman et al 34 administered intrathecal morphine to 33 pediatric patients undergoing PSF and found that the mean duration of postoperative pain relief was 18.8 hours. They concluded that intrathecal morphine administration was effective in controlling postoperative pain after AIS surgery; however, this study did not include a control group. Goodzari 35 evaluated the efficacy of lumbar intrathecal morphine and intrathecal sufentanil administration preoperatively and compared it with intrathecal sufentanil administration alone in 80 pediatric patients undergoing PSF. He found that intraoperative blood loss was almost 50% lower in the intrathecal morphine group than in the control group. He also found that the need for postoperative analgesia was delayed by 14.5 hours in the intrathecal morphine group whereas the control group needed postoperative analgesia immediately. Additionally, postoperative mobilization was tolerated better in the intrathecal morphine group. 35 Gall et al 26 studied the effect of intrathecal morphine in 30 pediatric patients undergoing PSF. They compared a high dose of intrathecal morphine (5 µg) with a lower dose of intrathecal morphine (2 µg) and a saline control group. They found that intraoperative blood loss was lower in the high-dose group than in the low-dose and control groups. 26 They also found that the first 24-hour morphine consumption by PCA was lower in the intrathecal morphine groups compared with the control group.
A noteworthy concern from neuraxial blockades, especially intrathecal use, is respiratory depression, which is potentially fatal. 6 In the study by Blackman et al, 34 the authors found that respiratory depression was noted in 8 out of the 33 patients in their study, but they attribute this to the large volume of fluid used for the infusion rather than the intrathecal morphine itself. Goodzari 35 did not report any incidence of respiratory depression in the 80 patients in their study, though they found that carbon dioxide levels were higher in the intrathecal morphine group compared with the control group. Gall et al 26 did not find any statistical difference in the adverse effects between the high-dose, low-dose, or control groups. Intrathecal morphine, therefore, is a safe and effective way to control early postoperative pain following PSF in pediatric patients. 26,34,35
Local Anesthesia—Bupivacaine
Bupivacaine provides analgesia by infusion through catheters in paraspinal muscle, subfascial area, or subcutaneous areas adjacent to spinal instrumentation. There has been only 1 study to date evaluating the use of bupivacaine in pediatric spine surgery (Table 4). Ross et al 36 stated that continuous basal infusion of morphine was required in 85.2% of patients without bupivacaine and only 32.6% of patients with continuous bupivacaine 1 day after surgery (18.9 vs 26.4 mg). The depth of catheter insertion did not influence postoperative opioid use, but ideal depth needs future investigation. Pain scores were equivalent in treatment and placebo groups at 6, 12, and 24 hours postoperatively but was significantly higher by 1 point at 18 hours.
Local Anesthesia—Bupivacaine Studies.
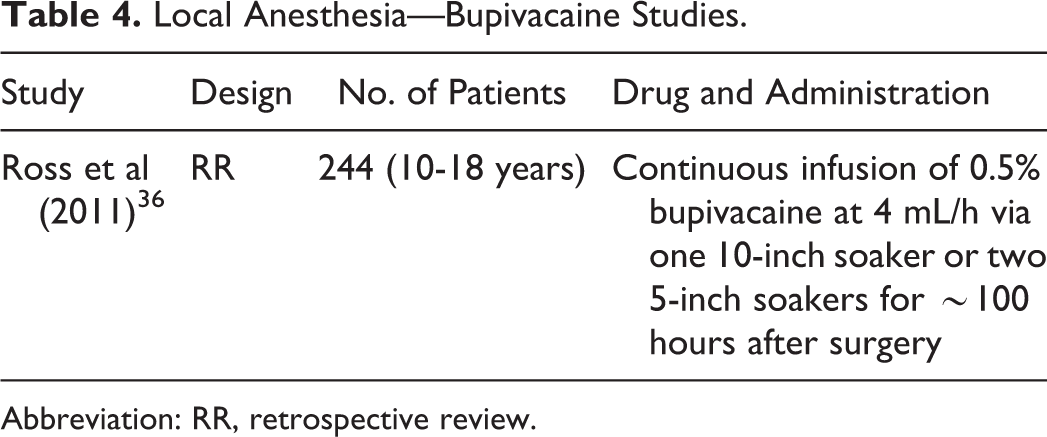
Abbreviation: RR, retrospective review.
The Rapid Recovery Pathway
In recent years, the immediate postoperative period has been a primary focus of change in pain management for patients undergoing orthopedic surgery, including PSF for AIS. Traditional postoperative regimens often involved 24 hours of bed rest or limited activity; however, there have been studies reporting early mobilization in combination with multimodal analgesia may decrease hospital stay. Multimodal analgesia incorporates the assortment of nonopioid agents previously discussed in this review. Given at predetermined intervals, these agents act synergistically with opioids to accelerate recovery time, lower pain levels, decrease the incidence of adverse effects, and reduce total opioid consumption. Multimodal practices have received praise in orthopedic procedures, especially joint arthroplasty 5,37 ; but there is little research on pediatric scoliosis correction. This treatment promotes faster recovery and early mobilization associated with the decrease in opioid requirements.
In a quality improvement project at the Children’s Hospital of Philadelphia, Muhly et al 38 standardized a rapid recovery pathway to promote early mobilization after posterior spinal fusion for AIS. In this pathway, patients were started on PCA on POD 0. On POD 1, they were taken off the PCA and started on oral pain medication with intravenous hydromorphone for breakthrough pain. Oral diazepam and gabapentin are also included in the oral regimen. IV ketorolac was added at the discretion of the surgeon. Ambulation was started three times daily. On POD 2, the oral pain regimen and physical therapy for ambulation three times daily is continued. On POD 3, discharge is finalized once the patient is tolerating oral analgesia, has clearance from physical therapy, and is tolerating a diet. After implementing this pathway, they noticed a significant decrease in hospital stay, from 5 days to 4 days. They also noted a decrease in numerical pain score on PODs 0 to 2 with the rapid recovery pathway implementation. These authors concluded that implementing this rapid recovery pathway reduced time to functional recovery and maintained effective analgesia postoperatively following PSF for AIS.
Fletcher et al 8 published a study in which they retrospectively compared 105 patients treated with an accelerated discharge (AD) pathway to 45 patients treated with a traditional discharge (TD) pathway. The TD pathway consisted of transition from PCA to oral pain medication on POD 3, mobilization with physical therapy once on POD 1, transition to solid diet on POD 2, and discharge on PODs 4 to 5. The AD pathway consisted of transition from PCA to oral medication on POD 1, mobilization with physical therapy twice-daily starting POD 1, transition to a solid diet on POD 1, and discharge PODs 2 to 3. They retrospectively compared the following characteristics between the 2 groups: Cobb angles, surgical times, estimated blood loss, length of stay, readmissions, and wound complications. They found that length of stay was 48% lower in patients treated with the AD pathway compared to the TD pathway without any difference in complications. In another study looking at financial implications of this AD pathway, Fletcher et al 9 found that the AD pathway led to a small but significant decrease in hospital cost when compared with the TD pathway. These authors concluded that the AD pathway not only may decrease hospital stay, but total hospital cost associated with PSF for AIS as well. 9
At our institution, we modeled our postoperative regimen after that established by Fletcher et al.
8,9
Our patients are started on PCA on POD 0. At 6
Summary
Pediatric scoliosis patients are a unique population as they often enter the hospital generally healthy and functional but find themselves leaving in a debilitated condition. As such, the employment of an effective pain management protocol should be a priority. Although a consensus has not been reached regarding on a postoperative protocol, earlier transition to oral pain medication, earlier ambulation, and earlier discharge are current trends in the perioperative care of AIS patients undergoing posterior spinal fusion. 8 Studies have shown that managing pain with adjuvants to opioid treatment may provide good outcomes by lowering opioid use, shortening length of stay, and increasing patient satisfaction. This has the added benefit of a quicker return to mobilization after surgery, which accelerates recovery allowing ambulation to begin sooner. Although NSAIDs, acetaminophen, neuraxial blockades, local anesthesia, and neuromodulatory agents alone offer many benefits, more emphasis should be laid on utilizing them in multimodal practices to yield the best result. Multimodal analgesic regimens may be used as part of a rapid recovery pathway to facilitate faster recovery in patients undergoing PSF for AIS.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.