
Abstract
Objective
To evaluate the impact of adding epidural dexmedetomidine to low-concentration patient-controlled epidural analgesia (PCEA) on pain control and side effects in total knee arthroplasty (TKA).
Methods
In this double-blind study, American Society of Anesthesiologists I to II patients undergoing TKA were assigned to receive 0.125% bupivacaine + fentanyl 4 µg/mL (group R) or 0.1% bupivacaine + fentanyl 2 µg/mL with an epidural injection of dexmedetomidine 1 µg/kg (group D). The primary outcomes were the effectiveness of postoperative pain control as assessed by the numeric pain rating scale (NRS) and the incidence of side effects. Secondary outcomes included hemodynamic parameters (systolic and diastolic blood pressure, heart rate), motor block assessment, sensory block duration, analgesia duration, and the need for additional analgesia.
Results
Both groups achieved similar pain control as indicated by NRS scores. However, group D experienced lower rates of urinary retention and pruritus, whereas sedation in the recovery room was greater in group D. Group R had significantly higher systolic pressure in the recovery room. group D exhibited significantly lower heart rates at 5 and 10 minutes.
Conclusions
Low-concentration PCEA with epidural dexmedetomidine provides similar analgesia after TKA as high-concentration PCEA with fewer side effects.
Keywords
Introduction
The number of patients undergoing total knee arthroplasty (TKA) is increasing, and effective postoperative pain control is essential because of the severity of pain experienced after surgery. Numerous studies and various attempts at pain management have been performed. 1 Studies indicated that approximately 40% to 58%2,3 of patients report moderate-to-severe pain on the first postoperative day, with 44% to 57%4,5 experiencing pain and insomnia from days 1 to 3 after surgery. Pain peaks up to 48 hours after surgery. 6 Patient-controlled epidural analgesia (PCEA) and continuous femoral nerve block are common pain management strategies, with studies demonstrating their effectiveness.7,8 Numerous studies have reported the analgesic effects of continuous femoral block (CFB) and continuous epidural block (CEB), achieving comparable effects with slight variations between the studies. 9 Additionally, iPACK block combined with adductor canal block (ACB) is also an effective motor-preserving technique that has been demonstrated to provide adequate analgesia while preserving motor function. 10 Although these techniques have advanced pain management, achieving optimal analgesia with minimal motor impairment remains a clinical challenge.11,12 iPACK block is ideal for patients requiring posterior knee pain relief, such as those with postoperative pain following tibial osteotomy or knee ligament reconstruction. CFB is suitable for procedures that require anterior knee analgesia, although its impact on quadriceps strength might limit its use in patients requiring immediate ambulation. CEB is applicable in situations requiring comprehensive pain management for both anterior and posterior knee regions, such as bilateral knee surgeries or cases involving high pain intensity. Table 1 provides a comparative overview of various analgesic techniques, highlighting their effectiveness, side effects, and implications for postoperative recovery. The side effects are influenced by the concentrations of local anesthetics and opioids used. 13 If CEB is considered a better option than iPACK block, it is necessary to identify the agents that can effectively reduce its side effects. In this study, dexmedetomidine was chosen as an alternative to opioids to minimize side effects while maintaining adequate analgesia. 14
Comparative summary of analgesic techniques.

CFB, continuous femoral block; ACB, adductor canal block.
Recent studies15,16 reported that epidural analgesia facilitates earlier motor recovery than peripheral nerve blocks. In this study, we aimed to preserve motor function and extend pain relief by using a selective alpha-2 adrenergic receptor agonist (dexmedetomidine) in the epidural space, which extended pain relief while minimizing motor impairment.
Dexmedetomidine also provides stable hemodynamics and pain relief without significantly increasing motor impairment, making it a more suitable choice for epidural anesthesia in this context. 17 Dexmedetomidine, which specifically targets alpha-2 receptors in the nervous system, is used as an adjuvant in epidural anesthesia to enhance analgesic effects and reduce pain. 18 Dexmedetomidine enhances pain relief by targeting alpha-2 receptors and reduces urinary retention by preserving bladder function. Furthermore, because of its lack of action on µ-opioid receptors, dexmedetomidine is associated with a lower incidence of pruritus.19–21
This study hypothesized that low-concentration PCEA combined with epidural dexmedetomidine can provide analgesic effects equivalent to those of high-concentration PCEA while significantly reducing side effects such as motor weakness, urinary retention, nausea, vomiting, and pruritus. By addressing the limitations of high-concentration agents, this approach aimed to optimize pain management and minimize complications.
Materials and methods
Study approval and patient selection
The study was approved by the Ethical Committee of the Catholic Medical Center (approval number: VC15MISI0144, approval date: 13 August 2015) and the Austrian Agency for Health and Food Safety (EudraCT2012-000030-19). Patient enrollment was performed from 25 August 2015 to 1 September 2016. The clinical trial registration date was 21 October 2019. Informed consent was obtained from all participants. The reporting of this study conforms to the CONSORT statement. 22 Patients with American Society of Anesthesiologists grade I to II undergoing primary TKA, including both unilateral and bilateral procedures, were included. The exclusion criteria were cardiac disease, chronic obstructive respiratory disease, coagulation abnormalities, spinal deformities, and allergies to amide-type local anesthetics. A per-protocol analysis was performed, and only patients who adhered to the study protocol were included in the final analysis.
Epidural anesthesia and sedation
Patients were monitored (electrocardiogram, SpO2, noninvasive blood pressure) and positioned laterally with lumbar flexion. Epidural anesthesia was administered at the L4 to L5 level using an 18 G Touhy needle (B. Braun, Melsungen, Germany) and confirmed by the loss of resistance technique. A test dose of 3 mL of 2% lidocaine with 1 mL of 1:200,000 epinephrine was given. Upon arriving at the operating room, patients were randomly divided into two groups by selecting a concealed envelope containing the group name. This process ensured randomization without any prior knowledge of group assignment, and the medications were prepared by a separate research participant who was not involved in data collection or analysis to maintain blinding throughout the study. Group R received 10 mL of 0.75% ropivacaine, 5 mL of 2% lidocaine, 50 µg of fentanyl, and 1 mL of normal saline. Group D received the same solution plus dexmedetomidine 1 µg/kg, which was administered as a single bolus dose based on the patient’s ideal body weight (IBW), and no continuous infusion followed. IBW was estimated using Broca’s index as follows: IBW (kg) = height (cm) − x, where x is 100 for adult men and 105 for adult women. 23 The epidural catheter was secured, and patients were sedated with propofol, maintaining a bispectral index (BIS) of 40 to 60. Epidural anesthesia was used for surgical anesthesia in combination with light sedation. A BIS range of 40 to 60, which does not indicate general anesthesia but reflects sedation management, was used to monitor sedation levels. Hemodynamic parameters were recorded at specified intervals.
Operation and post-anesthesia unit care
When the tourniquet was inflated, 50 mL of 1% propofol were infused using a target-controlled infusion mode to maintain a concentration of 1.0 to 2.0 µg/mL and BIS of 40 to 60 for sedation. Upon tourniquet deflation, 500 mL of 6% hydroxyethyl starch were infused. At the end of surgery, patients in group R received 0.125% bupivacaine + 4 µg/mL fentanyl, whereas those in group D received 0.1% bupivacaine + 2 µg/mL fentanyl. PCEA was administered as a 2-mL bolus at a rate of 5 mL/hour with a lockout interval of 20 minutes. Hemodynamic parameters were recorded at the time of tourniquet inflation, at the time of tourniquet deflation, and at 30 and 60 minutes after the initiation of the surgery. Atropine and ephedrine use was recorded. Atropine (0.25–0.5 mg) was intravenously injected when the intraoperative heart rate was ≤45/minute, and ephedrine (5 mg) was intravenously injected when systolic blood pressure was ≤80 mmHg.
Primary and secondary outcomes
The primary outcomes of this study were the effectiveness of postoperative pain control, as measured by the numeric pain rating scale (NRS), and the incidence of side effects such as urinary retention, nausea, vomiting, pruritus, and sedation. Secondary outcomes included hemodynamic parameters (systolic and diastolic blood pressure, heart rate), motor block assessment, sensory block duration, analgesia duration, and the need for additional analgesic use.
Parameters and recordings
Preoperative, intraoperative, and postoperative parameters included systolic and diastolic blood pressure, heart rate, NRS, urinary retention, numbness, nausea, vomiting, pruritus, the sedation score, and motor power. The sensory block duration and analgesia duration were recorded, along with any additional analgesic use. Patients were instructed to press the PCEA button at the onset of pain, and the time spent educating the patients on this procedure was recorded. Additionally, patients were informed to request further analgesics if they experienced moderate-to-severe pain. The data were directly recorded by the research physicians and nurses involved in the study. Data were collected using a case report form on paper for immediate observations, and outcomes were documented preoperatively, postoperatively in the recovery room, and at 24 and 48 hours post-surgery. Additionally, data at 24 and 48 hours were stored electronically through computer records.
Definition and grade
NRS: pain at rest on a scale of 0 to 10 (0 = no pain; 10 = pain as bad as you can imagine)
Urinary retention: graded 0 to 4 (0 = none; 1 = mild hesitancy; 2 = moderate, 3 = straight catheter required; and 4 = foley catheter required) 24
Numbness: graded 0 to 3 (0 = none; 1 = mild, not bothersome; 2 = moderate, somewhat bothersome; 3 = severe, very bothersome) 25
Sedation: assessed by the Richmond Agitation–Sedation Scale (RASS) (+4, combative; +3, very agitated; +2, agitated; +1, restless; 0, alert and calm; −1, drowsy; −2, light sedation; −3, moderate sedation; −4, deep sedation; −5, unarousable) 26
Nausea: graded 0 to 3 (0 = none; 1 = mild [does not interfere with activities of daily living]; 2 = moderate [sometimes interferes with activities]; 3 = severe [inability to undertake any activities or vomiting three or more times]) 27
Pruritus: graded 0 to 4 (0 = none; 1 = mild; 2 = moderate; 3 = severe; 4 = unbearable) 28
Motor power: Assessed using the Bromage scale (Grade 0 = free movement of legs and feet; Grade I = just able to flex knees with free movement of feet; Grade II = unable to flex knees but free movement of feet; Grade III = unable to move legs or feet)
Definition of time points
The duration of sensory block was defined as the time from the injection of epidural drugs to the complete recovery of cold and pain sensation. Sensory assessment was conducted by asking the patients and testing with an alcohol swab and pinprick on the knee. The duration of analgesia was defined as the interval from the completion of epidural drug administration until the first need for rescue analgesia, which was identified by the patient pressing the PCEA button.
Although this study demonstrated the efficacy and safety of epidural dexmedetomidine in postoperative analgesia, the lack of measurements for the onset of sensory and motor blocks is a notable limitation. Future studies should address this aspect to provide a more comprehensive understanding of the temporal dynamics of block onset and their impact on clinical outcomes.
Power analysis
The sample size calculation was based on the findings of Vercauteren et al., in which the control group had a urinary retention grade of 1.9 ± 1.2, and the low-dose bupivacaine–sufentanil group had a grade of 1.0 ± 1.0. 29 Based on these results, we hypothesized that the low concentration of PCEA in our study would reduce urinary complications by approximately 45%. This 45% reduction estimate was based on existing literature and considered a reasonable assumption for the purposes of this study. Using these data, we calculated the required sample size for the difference in urinary retention grades between the two groups to be significant with α = 0.05 and β = 0.2, which necessitated 27 participants per group. Assuming a 10% dropout rate, an enrollment size of 60 patients, with 30 patients in each group, was targeted. This sample size calculation was also supported by Kim et al., who examined the effect of epidural sufentanil in ropivacaine on urinary retention in patients undergoing gastrectomy. 24
Statistical analysis
Statistical analysis was performed using IBM SPSS 20.0 (IBM Corp., Armonk, NY, USA). Numerical variables were presented as the mean and standard deviation, while categorical data were presented as counts and percentages. Data normality was assessed using Kolmogorov–Smirnov and Shapiro–Wilk tests. Comparisons between the two groups were made using Student’s t-test, the independent two-sample t-test, and the chi-square test for normally distributed data. P < 0.05 was considered statistically significant.
Results
Demographic data and baseline characteristics
Sixty patients were randomly divided into two groups between 25 August 2015 and 1 September 2016. Data from five patients were excluded from the analysis, including three patients in group R and two patients in group D. The reasons for exclusion in group R included incomplete epidural block, postoperative pulmonary embolism, and inadvertent epidural puncture. In group D, exclusions were attributable to spinal block and PCEA catheter dislocation. The remaining 55 patients were analyzed (group R: n = 27, group D: n = 28). Patient characteristics are presented in Table 2. There were no significant differences between the groups (P > 0.05).
Baseline characteristics.
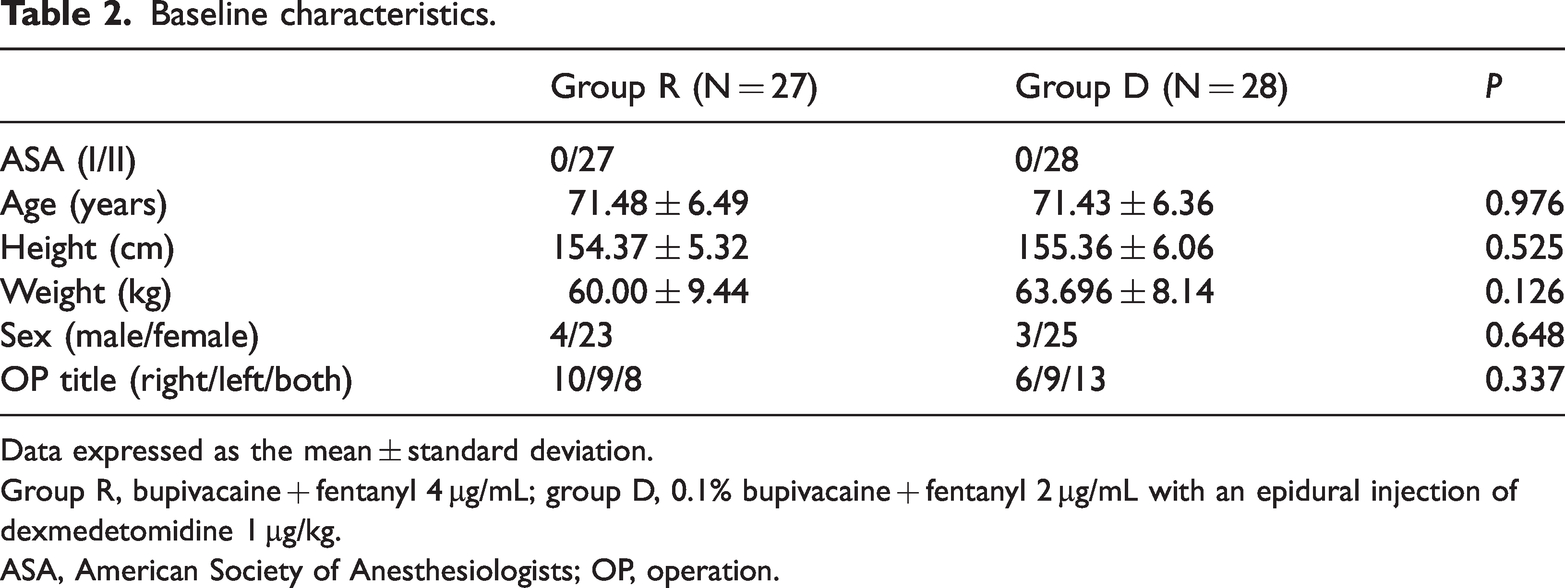
Data expressed as the mean ± standard deviation.
Group R, bupivacaine + fentanyl 4 µg/mL; group D, 0.1% bupivacaine + fentanyl 2 µg/mL with an epidural injection of dexmedetomidine 1 µg/kg.
ASA, American Society of Anesthesiologists; OP, operation.
Primary outcomes
Postoperative pain control (NRS scores)
The NRS scores between the two groups did not differ at any measured time points (P > 0.05). Both groups experienced effective postoperative pain control (Figure 1).

NRS scores over time. Data are presented as the mean. Statistically significant differences are marked with asterisks (P < 0.05). Group R, bupivacaine + fentanyl 4 µg/mL; group D, 0.1% bupivacaine + fentanyl 2 µg/mL with an epidural injection of dexmedetomidine 1 µg/kg. NRS, numeric pain rating scale.
Incidence of side effects
The incidence and severity of side effects were evaluated up to 48 hours postoperatively. The findings revealed distinct differences between the two groups in terms of urinary retention, sedation, pruritus, and motor weakness.
The rate of urinary retention was significantly higher in group R at 24 hours after surgery (59.3% vs. 28.6%, P = 0.022). The mean grade of urinary retention was also higher in group R, particularly at 18 and 24 hours, where it was 1.19 ± 1.36 and 1.22 ± 1.28, respectively, compared with 0.50 ± 0.92 and 0.54 ± 1.04, respectively, in group D (P = 0.045 and P = 0.02, respectively).
Sedation levels were assessed using RASS. In the recovery room, 7 of 28 patients (25.0%) in group D exhibited sedation, compared with 1 of 27 patients (3.7%) in group R (P = 0.025). The mean sedation score in the recovery room was −0.32 ± 0.67 for group D versus −0.04 ± 0.19 for group R. No patients in either group exhibited sedation after the 6-hour postoperative mark.
The incidence of pruritus was statistically significantly higher in group R at 18 (25.9% vs. 0%, P = 0.004) and 30 hours postoperatively (22.2% vs. 0%, P = 0.008). The mean grade of pruritus was also higher in group R from 6 to 48 hours postoperatively, peaking at 18 and 30 hours (0.33 ± 0.68 and 0.22 ± 0.42), significantly exceeding those in group D (both P < 0.05).
Motor weakness was assessed using the Bromage scale. At 6 hours postoperatively, the incidence of motor weakness was higher in group D (78.6%) than in group R (63.0%). However, at subsequent time points, the incidence was higher in group R, but the differences were not significant. The mean motor block grade in the recovery room was higher in group D (2.46 ± 0.58) than in group R (1.96 ± 0.84, P = 0.028). Table 3 summarizes the incidence of side effects.
Incidence of side effects in the two groups.

Data expressed as numbers and percentages. *P < 0.05.
Group R, bupivacaine + fentanyl 4 µg/mL; group D, 0.1% bupivacaine + fentanyl 2 µg/mL with an epidural injection of dexmedetomidine 1 µg/kg.
Secondary outcomes
Hemodynamic parameters
Systolic and diastolic blood pressure, as well as heart rate, was measured at various time points. Systolic blood pressure in the recovery room was significantly higher in group R (P = 0.006). Diastolic blood pressure was significantly lower in group R at 30 minutes and 30 hours (P = 0.037 and P = 0.02, respectively), whereas it was higher in group R in the recovery room (P = 0.037). The heart rate was significantly lower in group D at 5 and 10 minutes (P = 0.032 and P = 0.026, respectively), with the opposite trend observed at 30 hours (P = 0.035; Figure 2).

SBP and DBP changes over time. Data are presented as the mean. Statistically significant differences are marked with asterisks (P < 0.05). Group R, bupivacaine + fentanyl 4 µg/mL; group D, 0.1% bupivacaine + fentanyl 2 µg/mL with an epidural injection of dexmedetomidine 1 µg/kg.
Sensory block duration and analgesia duration
The durations of sensory block and analgesia were longer in group D, albeit without significance (P = 0.859 and P = 0.616, respectively). Rescue analgesic usage was higher in group D for tramadol, whereas the rates of diclofenac and pethidine use were higher in group R. However, none of the differences was significant. The infusion rate and total amount of ephedrine administered intraoperatively were also not significantly different between the groups (Table 4).
Supplementary intravenous analgesia and intraoperative hemodynamic management.

Group R, bupivacaine + fentanyl 4 µg/mL; group D, 0.1% bupivacaine + fentanyl 2 µg/mL with an epidural injection of dexmedetomidine 1 µg/kg.
Discussion
This is the first study to investigate the synergistic effect and side effects of low-concentration PCEA with epidural dexmedetomidine on postoperative pain. The findings demonstrate that this combination provides equivalent analgesia as high-concentration PCEA alone with fewer side effects, particularly urinary retention and pruritus, after TKA.
Numerous studies have evaluated pain control methods following TKA, with CFB and CEB being widely used. Barrington et al. and a meta-analysis by Fowler et al. both demonstrated equivalent analgesia between CFB and CEB.9,11 However, CFB often requires a sciatic nerve block, and it has been associated with postoperative nerve palsy.30,31 Conversely, CEB has a higher incidence of adverse effects, including urinary retention, nausea, vomiting, pruritus, and motor weakness, as reported by Wang et al. and Vercauteren et al.9,11,13,24,29
Peripheral nerve blocks, such as iPACK block and ACB, provide effective motor-preserving analgesia after TKA. Studies revealed that combining iPACK with ACB improves ambulation pain control, reduces opioid consumption, and enhances functional outcomes, including range of motion and rehabilitation speed. 10 However, in this study, we selected epidural analgesia because of its ability to provide more comprehensive pain relief for both anterior and posterior regions of the knee, areas that might not be fully addressed by peripheral blocks alone. Furthermore, using dexmedetomidine in the epidural space extended analgesia and minimized side effects, making it a suitable choice in our context.
Studies on maintaining analgesia and reducing adverse effects at CEB have been conducted, and studies using clonidine as an adjuvant were recently reported. 32 Clonidine is an α-2 adrenoreceptor agonist with analgesic and sedative effects, and it has been used as a neuraxial adjuvant for regional anesthesia. 33 Recently, dexmedetomidine has been commercialized, and many studies on epidural dexmedetomidine, which has 9-fold higher affinity for α-2 adrenoreceptors than clonidine, have been conducted. Bajwa et al. concluded that dexmedetomidine is a better adjuvant than clonidine, providing stable cardio-respiratory changes and effective analgesia. 34 The side effects of neuraxial dexmedetomidine include hypotension, bradycardia, sedation, nausea, and vomiting. A meta-analysis by Wu et al. confirmed that neuraxial dexmedetomidine reduces the postoperative pain intensity and prolongs the duration of analgesia. 35 However, other studies investigated the intraoperative use of ephedrine or atropine consumption, and no difference was detected between the neuraxial dexmedetomidine and placebo groups, suggesting an overall stable hemodynamic and that these changes were easily reversed. 36 In this study, the durations of sedation and analgesia were longer in group D, likely because of to the combined effect of bupivacaine, fentanyl, and epidural dexmedetomidine.
Sedation caused by dexmedetomidine is dose-dependent and similar to natural sleep. In this study, the incidence of sedation was higher in group D only in the recovery room, indicating that dexmedetomidine can be safely used without additional monitoring after the recovery period. The incidence of urinary retention and pruritus was significantly lower in group D, consistent with previous findings that dexmedetomidine reduces these side effects. Dexmedetomidine reduces pruritus by avoiding activation of µ-opioid receptors, which are primarily responsible for opioid-induced itching, while providing effective analgesia through its α-2 adrenergic receptor agonist activity. Motor power was higher in group D, suggesting that the prolongation of motor block by epidural dexmedetomidine was effective.
Several studies reported that neuroaxial dexmedetomidine prolongs the duration of motor block. 37 In this study, motor power was higher in group D, reflecting the prolongation of motor block by epidural dexmedetomidine. In this study, we used dexmedetomidine not necessarily because it is superior to other adjuvants. Instead, it was selected to explore its potential to reduce the side effects commonly associated with opioids and other agents. Although dexmedetomidine has demonstrated benefits such as stable hemodynamics and extended analgesia, the primary goal was to evaluate whether it could reduce adverse effects such as nausea, vomiting, and urinary retention. This approach allowed us to investigate the feasibility of dexmedetomidine as a valuable alternative for balancing effective pain control with fewer side effects rather than claiming its overall superiority compared with other adjuvants such as opioids or dexamethasone.
The onset of sensory and motor block was not measured in this study because of operational constraints. Additionally, fluoroscopy was not used, which may have affected the accuracy of epidural catheter placement. Future studies should include these measurements and use fluoroscopic guidance to improve reliability.
Based on these findings, we recommend the use of dexmedetomidine in epidural anesthesia for patients undergoing knee surgery as it ensures effective pain management while maintaining stable vital signs. Furthermore, its safety profile and hemodynamic stability make dexmedetomidine a suitable option for anesthesia in lower-limb surgeries, even for hemodynamically unstable patients.
Limitations
Some limitations of this study merit mention. First, the relatively small sample size and limited involvement of researchers in data collection might restrict the generalizability of the findings. Future studies would benefit from larger sample sizes and increased collaboration among researchers to enhance the robustness of the data. Additionally, although we did not measure the onset of sensory and motor block because of operational constraints, this could be an important parameter to include in future research to better understand the timing and effectiveness of analgesia. Despite these limitations, this study offers valuable insights into the role of dexmedetomidine as an adjuvant in epidural analgesia, and future work could expand on these findings with longer-term follow-up and more detailed assessments.
Conclusions
Low-concentration PCEA with a bolus of epidural dexmedetomidine provides equivalent analgesia and after TKA with fewer side effects, especially in urinary retention and pruritus, than high-concentration PCEA alone.
Future studies should investigate the long-term effects of dexmedetomidine in epidural anesthesia and evaluate its efficacy in larger and more diverse patient populations to further validate its benefits and broaden its clinical applicability.
Footnotes
Acknowledgements
We would like to express our gratitude to the Knee Surgery Team of the Department of Orthopedic Surgery at St. Vincent’s Hospital for their invaluable contributions and support to this study. Their expertise and assistance were instrumental in the completion of this work.
Author contributions
Research concept and design: Seong Min Han, So Young Kwon, and Jin Deok Joo
Data collection: Seong Min Han and Jae Hyuk Kang
Investigation and methodology: Seong Min Han and So Young Kwon
Validation: So Young Kwon and Jin Deok Joo
Drafting of the manuscript: Seong Min Han and Jaesuk Kim
Making important revisions to the paper: So Young Kwon and Jaesuk Kim
Approval of the final paper to be published: All authors
Data availability statement
The authors confirm that the data supporting the findings of this study are available within the article.
Declaration of conflicting interest
The authors declare no conflict of interest in preparing this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.